





Most invasive coronary imaging modalities only provide anatomical information from which physiologic significance is inferred. Fractional flow reserve (FFR) and other physiologic indices of lesion severity are more reliable methods to identify physiologically significant lesions. Currently, accomplishing both anatomic and physiologic interrogation of an intermediate coronary stenosis requires the use of multiple devices within the coronary artery.
Coronary angiography, optical coherence tomography (OCT), and FFR were performed in a left anterior descending artery harbouring an intermediate lesion. Quantitative coronary angiography (QAngio XA 7.3, Medis, the Netherlands) and OCT analysis were performed (QIvus 3.0, Medis, the Netherlands). Angiography and OCT were fused to reconstruct the vessel. Pulsatile non-Newtonian coronary flow was performed using computational fluid dynamics (CFD) to virtually derive FFR (vFFR). Computed arterial pressures were time averaged, and vFFR was calculated as P Dmean/P Amean (Figure).
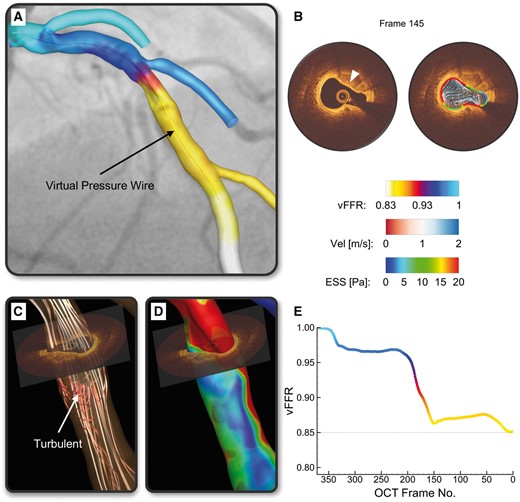
By quantitative angiography the lesion had a diameter stenosis of 52%, and by OCT the minimal lumen area was 3.20 mm2. Optical coherence tomography imaging demonstrated a highly eccentric, asymmetric fibro-calcific lesion (Panel B). Computational fluid dynamics showed turbulent flow (Panel C) and low endothelial shear stress (ESS) distal to lesion (Panel D) that results in vFFR = 0.85 (Panel B) vs. invasively determined FFR of 0.83. However, vFFR was also able to be determined along the OCT pullback segment (Panels A and B, Supplementary material online, Video S1) providing an instantaneous snapshot of the vFFR that was directly correlated with useful characterization of the plaque burden.
The hypothetical advantage of this method is gaining physiologic information along with high-resolution anatomic imaging through the marriage of OCT and vFFR without having to rely on the limitations of angiography alone.
Supplementary material is available at European Heart Journal online.


{kind=link}