





Abstract
Right iliac fossa pain is a common acute general surgery presentation, and computer tomography (CT) is often used as an aid in determining the diagnosis. CT can play an important role in differentiating malignant and inflammatory causes of caecal wall thickening if certain key features are identified. Two patients with similar presentations of right iliac fossa pain had pre-operative CT, which showed inflammation and caecal thickening, the first was focal with homogenous enhancement, and the second eccentric with stratification. At operation, these were proven to be malignant and inflammatory caecal thickening. Although the clinical presentation of appendicitis and caecal carcinoma may be similar, and the correct recognition and interpretation of differentiating CT characteristics enables the patient for an appropriately tailored operation.
INTRODUCTION
Right iliac fossa pain is a common emergency surgical presentation. Computer tomography (CT) imaging is increasingly being used as an aid in determining the diagnosis and assessing for complications, especially in an atypical presentation such as in younger age groups. These two cases presented simultaneously to our hospital and highlight an important role that appropriate interpretation of CT findings can play in differentiating malignant from inflammatory causes of caecal wall thickening.
CASE REPORTS
A 49-year-old and a 55-year-old female each presented with 1 week of right iliac fossa abdominal pain with altered bowel habit. The first had iron deficiency anaemia, and was on non-steroidal anti-inflammatory medications. Neither had any other medical history, per rectal bleeding nor weight loss. Neither had any risk factors for colonic carcinoma or had a prior colonoscopy. On examination, both had normal vital signs, mild right-sided tenderness without guarding and no abdominal mass. The first patient had microcytic anaemia and normal serum CEA, and the second had an isolated mild white cell rise to 13.5 × 109/dl.

Axial view of patient with caecal carcinoma. Eccentric caecal wall thickening with homogenous contrast enhancement (arrow). Mild pericolic fat stranding is present.
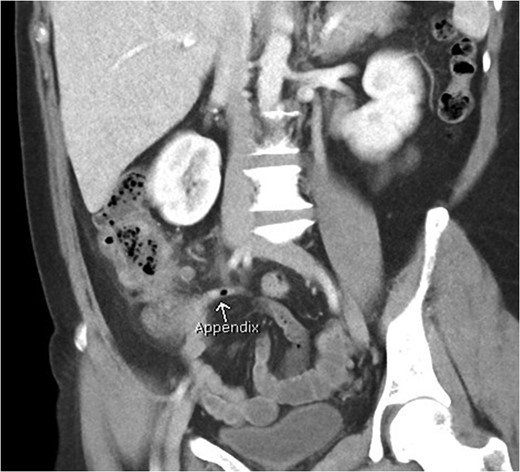
Coronal view of patient with caecal carcinoma. Normal (non-dilated) appendix (arrow).

Coronal view of patient with appendicitis. Dilated and thick walled appendix (arrow).

Axial view of patient with appendicitis. Eccentric caecal wall thickening (maximal surrounding the appendiceal orifice) with layered mural contrast enhancement secondary to prominent submucosal oedema (arrow) and prominent pericolic fat stranding represent the CT manifestation of the surgical phlegmon.
At laparoscopy, the first patient who had a normal appendix was identified with mild caecal fat stranding. Given the high index of suspicion for carcinoma on imaging, a right hemicolectomy was completed with en bloc resection of draining lymph nodes. She had an uncomplicated post-operative recovery and discharged on Day 3. Histopathology revealed a poorly differential adenocarcinoma extending into the pericolic adipose tissue with lymphovascular invasion and 3/29 lymph nodes contained metastatic adenocarcinoma (T3N1M0). She was referred for adjuvant chemotherapy and remains well after 3 months.
The second patient had a laproscopy, and appendicitis with serosal inflammatory changes of the caecum was noted. Due to a fragile appendiceal base, a laparoscopic ileo-colic resection was completed. She required a 5-day stay in hospital with intravenous antibiotics, and was well at her 2 week post-operative review. Histopathology confirmed acute appendicitis with transmural inflammation extending into the mesoappendix and no evidence of malignancy.
DISCUSSION
Caecal carcinoma is increasingly common in younger age groups [1], and is an important differential diagnosis in patients with right-sided abdominal pain. Clinical presentation may be similar to acute appendicitis due to local infiltration and micro-perforation resulting in secondary caecal inflammation. A pre-operative colonoscopy may not always be possible in the acute presentation. Bowel wall thickening is often seen on CT and is best appreciated if the bowel is distended (air, fluid or oral contrast). However, oral contrast limits the ability to differentiate malignant from inflammatory causes of bowel wall thickening (as well as detection of bowel wall infarction) and is therefore now typically not used in CT for evaluation of acute abdominal pain [2].
There are a number of CT features that help distinguish bowel wall thickening from malignant and benign causes [3]. A neoplastic cause is suggested if there is focal bowel wall thickening (less than 5 cm of extension) which is typically asymmetrical and eccentric. These may have homogeneous contrast enhancement due to infiltration of a tumour mass, or a heterogeneous areas of low attenuation from ischaemia and necrosis, findings with a sensitivity of up to 97% [4]. Malignancy may also have shouldered edges as opposed to tapering transition to normal bowel wall. Appendiceal dilatation, if present, may be thin walled and without inflammatory stranding due to a gradual obstructive process, although appendicitis can be a presenting symptom for carcinoma. Regional lymphadenopathy and distal metastases, when present, support the diagnosis.
Appendicitis features include a fluid-filled dilation (>6 mm) and thickening of the appendiceal wall with mild-to-moderate peri-appendiceal fat stranding [5]. Peri-caecal inflammation may occur, characterised by segmental eccentric bowel wall thickening centred over the appendiceal orifice. Importantly, the submucosa (expanded and low density), muscularis and serosa (both slightly thickened and enhancing more than normal) may be delineated in a stratified or layered pattern. Other complications may be present such as perforation or abscess formation, which are seen as rim enhancing collections. Rarely, hepatic abscesses may be present as a manifestation of portal pyaemia, characterised by diffuse liver lesions close to the portal vein tributaries.
The (often) subtle differences in CT findings between these two conditions are important to recognise as they can affect the surgical approach. Both may be managed laparoscopically, but the need to ensure appropriate margin and lymph node sampling for carcinoma requires more extensive surgery. Breach of the bowel wall and an R1 resection for colon carcinoma should also be avoided, given the poorer disease free and overall survival for such patients [6], hence the need for a high pre-operative index of suspicion. Alternatively, if an inflammatory phlegmon is suspected, an appendicectomy and control of sepsis is required, with caecal resection only if the base could not be adequately controlled. Extensive mobilisation of the ascending colon can be avoided and prevents damage to surrounding structures.
In summary, the clinical presentation of appendicitis and caecal carcinoma may be similar, and the correct recognition and interpretation of differentiating CT characteristics may be pivotal to the diagnosis. Both may have caecal wall thickening, the nature of which can usually be differentiated on CT imaging. With accurate interpretation, the patient may be prepared for a tailored operation and receive appropriate and definitive treatment.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}