Article Text

Abstract
The International Liaison Committee on Resuscitation recommends starting positive pressure ventilation (PPV) in the delivery room when heart rate (HR) <100 beats per min (bpm) and giving cardiac compressions when HR <60 bpm.
Objective To describe the effect of PPV on HR in infants <30 weeks gestation with HR <100 bpm in the first minutes after birth.
Study design Retrospective observational study of infants, <30 weeks gestation, born between 14 February 2007 and 28 February 2009 with HR <100 bpm soon after birth.
Methods Infants with a HR <100 bpm receiving PPV at birth were eligible for the study. Video recordings and respiratory physiological data were obtained during delivery room resuscitation and analysed to determine if the rate of change in HR varied with measures of PPV, for example, expiratory tidal volume.
Results It took a median (IQR) 73 (24–165) seconds of PPV for infants' HR to rise above 100 bpm and a median (IQR) 243 (191–351) seconds to rise above 120 bpm. There were large fluctuations in HR after reaching 100 bpm and before reaching 120 bpm. In 18/27 (67%) of infants the HR did not remain stable until a threshold of approximately 150 bpm was reached. In 6/27 (20%) of the infants the rise in HR was almost instantaneous. In the remaining 21/27 (80%) HR rise was more gradual. There was a poor correlation between time of HR increase to 120 bpm and tidal volume (p=0.13).
Conclusion It takes more than a minute for newly born infants <30 weeks gestation with a HR <100 bpm to achieve a HR above 100 bpm. In these infants HR does not stabilise until it reaches 120 bpm.
Statistics from Altmetric.com
Background
The International Liaison Committee on Resuscitation (ILCOR)1 recommends a heart rate (HR) <100 beats per min (bpm) as an action point for the commencement of positive pressure ventilation (PPV) in the delivery room (DR). A HR <60 bpm is an action point for commencement of chest compressions.1
The 2005 guidelines1 are based on findings from fetal lamb and apnoeic dog models of Dawes2 and Angell-James3 respectively. These explored the reflex nature of HR rise during supportive ventilation. In asphyxiated term animal models and term infants4 HR has been shown to increase rapidly with effective ventilation.
In addition, we could find no evidence supporting the use of the current HR parameters as action points in the neonatal resuscitation algorithm. The aim of this study was to describe the relationship between HR and measures of tidal volume (VT) in the DR.
What is already known on this topic
▶ Heart rate (HR) is an important indicator in guiding management during neonatal resuscitation.
▶ Vagal reflexes can be responsible for bradycardia in newly born infants.
▶ Increasing HR is a good indicator of effective positive pressure ventilation (PPV).
What this study adds
▶ In newly born infants <30 weeks gestation with a HR less than 100 bpm it can take more than a minute of PPV to achieve a HR more than 100 bpm.
▶ In some infants <30 weeks gestation the HR may not stabilise until it reaches 120 bpm.
Patients and methods
The Royal Women's Hospital (RWH), Melbourne is a tertiary perinatal centre where approximately 6000 infants are born and more than 100 infants of <1000 g birth weight are admitted to the neonatal intensive care unit annually.
Infants <30 weeks gestation, born at the RWH, Melbourne between February 2007 and February 2009 were eligible for this study. This was a convenience sample with infants enrolled in one of two prospective randomised trials in the DR. The first study compared the T-piece (Neopuff; Fisher & Paykel, Auckland, New Zealand) with a self-inflating bag (SIB) (Laerdal 240 ml silicone infant resuscitator; Laerdal, Stavanger, Norway) for resuscitation of infants < 29 weeks gestation. The second study investigated the use of the Florian Respiratory Function Monitor (RFM) (Acutronic Medical Systems AG, Zug, Switzerland) during PPV enrolling infants <32 weeks gestation. Respiratory physiological recordings from infants enrolled in the two studies were reviewed and included in the current study if the infant's initial HR was <100 bpm for at least 30 s, and pulse oximeter (PO) measurement of HR and web cam images were available. Infants with a congenital abnormality, initial HR >100 bpm soon after birth or who did not receive PPV were excluded. Both DR trials were approved by the Royal Women's Hospital Research and Ethics Committees, written parental consent was obtained.
Births were attended by the research team in addition to the clinical team, which usually included a neonatal consultant, fellow, registrar and neonatal nurse. The research team did not participate in the clinical care of the patient. Resuscitation followed a standardised protocol using either a T-piece device or an SIB. All infants received PPV via a 00 size round silicone facemask (Laerdal, Stavanger, Norway).
Initial settings for the T-piece were: gas flow of 8 l/min; peak inflating pressure (PIP) and positive end expiratory pressure (PEEP) of 30 and 5 cm H2O respectively. Infants managed with a T-piece could receive continuous positive airway pressure (CPAP) at any time if the infant was breathing regularly but had signs of respiratory distress, expiratory grunt or chest recession. The SIB was used with 8 l/min gas flow without a manometer or an expiratory PEEP valve. SIB infants could receive CPAP after 6 min if the infant was breathing regularly but had signs of respiratory distress, expiratory grunt or chest recession. Intubation was recommended if the infant remained apnoeic, or HR was <100 bpm or if HR did not improve with 60 s of PPV. The initial resuscitation for all infants was with air. Supplemental oxygen was commenced if HR was <100 bpm and not increasing after 60 s of PPV. When >21% oxygen was given the percentage was reduced in stages by 10% every 30 s once the oxygen saturation (SpO2) was >90%.
Data collection
Heart rate data
A pulse oximetry sensor (LNOP Neo-L; Masimo, California, USA) was placed on the infant's right hand/wrist before being connected to a Masimo PO (Radical7 V5; Masimo)5 immediately following birth. The oximeter was set at 2 s averaging and maximum sensitivity. After birth, data (time, HR, SpO2 and signal quality) were downloaded from the oximeter to a computer using the neO2M program (Girvan Malcolm, Royal Prince Alfred Hospital, Sydney, Australia). We only analysed HR measurements when the oximeter signal was of good quality, that is, no alarm messages (low signal quality indicator, low perfusion, sensor off, ambient light) were displayed.
Respiratory physiological measures
Airway pressures, gas flow and VT were measured with a Florian (RFM). Airway pressure was measured directly from the ventilation circuit and a hot-wire anemometer flow sensor was placed between the ventilation device and the facemask measuring gas flow. The inspired oxygen concentration was measured with an oxygen analyser (MX300-1 portable oxygen monitor; Teledyne Analytical Instruments, California, USA), which was inserted into the inspiratory limb of the T-piece or SIB circuit. A web-cam (QuickCam Pro for Notebooks; Logitech, Romanel-sur-Morges, Switzerland) recorded the resuscitation at five frames per second. Data measured with the RFM was recorded at 200Hz using a dedicated computer with Spectra software (Grove Medical, London, UK).
Data collection started soon after birth and stopped when HR exceeded 120 bpm for at least 30 s. The primary outcome was time to reach the target HR of 120 bpm after commencement of PPV. Secondary outcomes included the time taken for HR to rise above 120 bpm for at least 30 s, percentage leak between the mask and ventilation device, expiratory tidal volume (VTe) and the amount of pressure given during PPV.
Data management
All inflations given to an enrolled infant were examined. Pauses in PPV and incomplete inflations were defined a priori as occurring when the mask was removed to observe the infant's breathing efforts, for intubation, or when the infant was suctioned. We also excluded the period when infants were receiving CPAP. We used the webcam images to identify pauses in ventilation.
The amount of leak between the mask and ventilation device was calculated by expressing the volume of gas that did not return through the flow sensor during expiration as a percentage of the volume that passed through the flow sensor during inflation (leak (%)=((inspiratory tidal volume−expiratory tidal volume)/inspiratory tidal volume)×100).6 Facemask leak was retrospectively corrected for body temperature, pressure and water vapour saturation using a standardised equation.7
Respiratory physiological data including leak, VTe, PIP and PEEP were exported from Spectra to a Microsoft Excel spreadsheet where it was time matched and merged with HR data from the PO. The merged Excel file was imported into Stata Version 10 (College Station, Texas, USA) for analysis.
Statistical analysis
For each inflation leak, VTe, PIP and PEEP were recorded. Results are presented as mean (SD) for normally distributed continuous variables and median (IQR) for variables with a skewed distribution. Sub group analysis comparing the two ventilation devices, T-piece and SIB were performed with two sample t tests used to compare the mean time of HR rise, PIP and inflation rate.
Results
There were 88 infants <30 weeks gestation enrolled in randomised trials of DR care during the study period. In all, 27/88 infants met the study criteria and formed the study group (figure 1). Tables 1 and 2 summarise the clinical characteristics of study infants and their DR interventions respectively. The data was rejected 37% of the time, when the PO measured poor signal quality/poor perfusion or there was a pause in PPV for assessment, readjusting the facemask or other interventions.
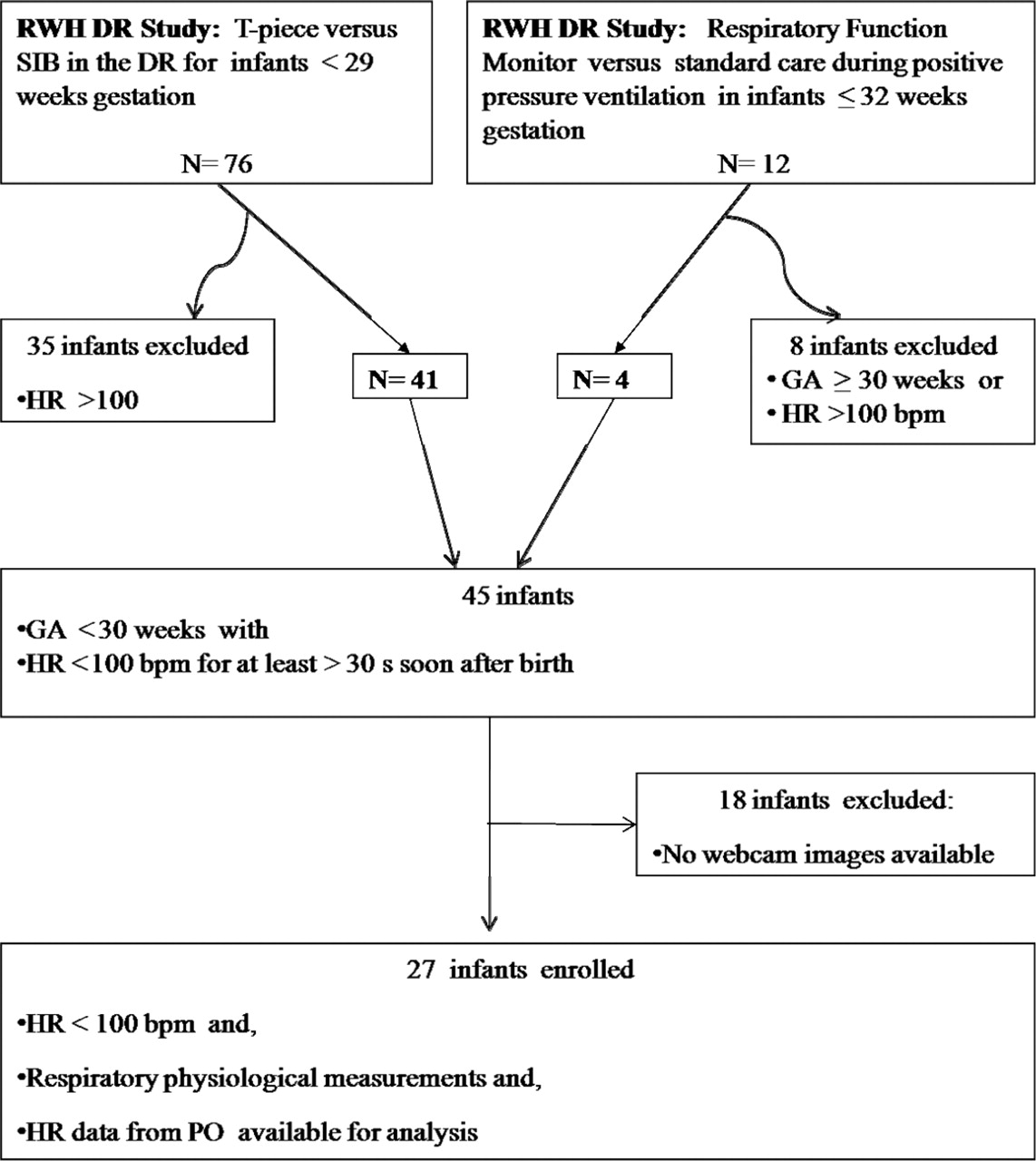
Flow diagram illustrating cohort entered into the study.
Characteristics of infants
Delivery room interventions during study period (commencement of PPV to attainment of a stable HR ≥120 bpm for at least 30 s)
It took a median (IQR) 73 (24–165) seconds of PPV for infants' HR to rise above 100 bpm and a median (IQR) 243 (191–351) seconds to rise above 120 bpm. There were large fluctuations in HR after reaching 100 bpm and before reaching 120 bpm.
At the commencement of PPV 7/27 (26%) infants had a HR less than 60 bpm. These seven infants required a median (IQR) of 8 (2–24) seconds PPV for the HR to rise above 60 bpm. The remaining 20/27 (74%) infants with a HR between 60 and 100 bpm required a median (IQR) of 73 (25–166) seconds PPV to rise above 100 bpm and 120 (69–195) seconds of PPV to reach HR ≥120 bpm. The median HR after 30 and 60 s of PPV in infants with an initial HR <60 bpm or HR 60 to 100 bpm were 82 and 87 bpm respectively. In 18/27 (67%) infants the HR did not remain stable until a threshold of approximately 150 bpm was reached.
Six of the 27 infants (20%) demonstrated a rapid increase in HR, defined as a rise of at least 75 bpm over 5 s (figure 2A). The remaining 21/27 (80%) infants experienced a slower HR rise, with some infants requiring up to 60 s for their HR to reach 100 bpm (figure 2B). In 18/27 (67%) infants the HR did not remain stable until a threshold of approximately 150 bpm was reached.
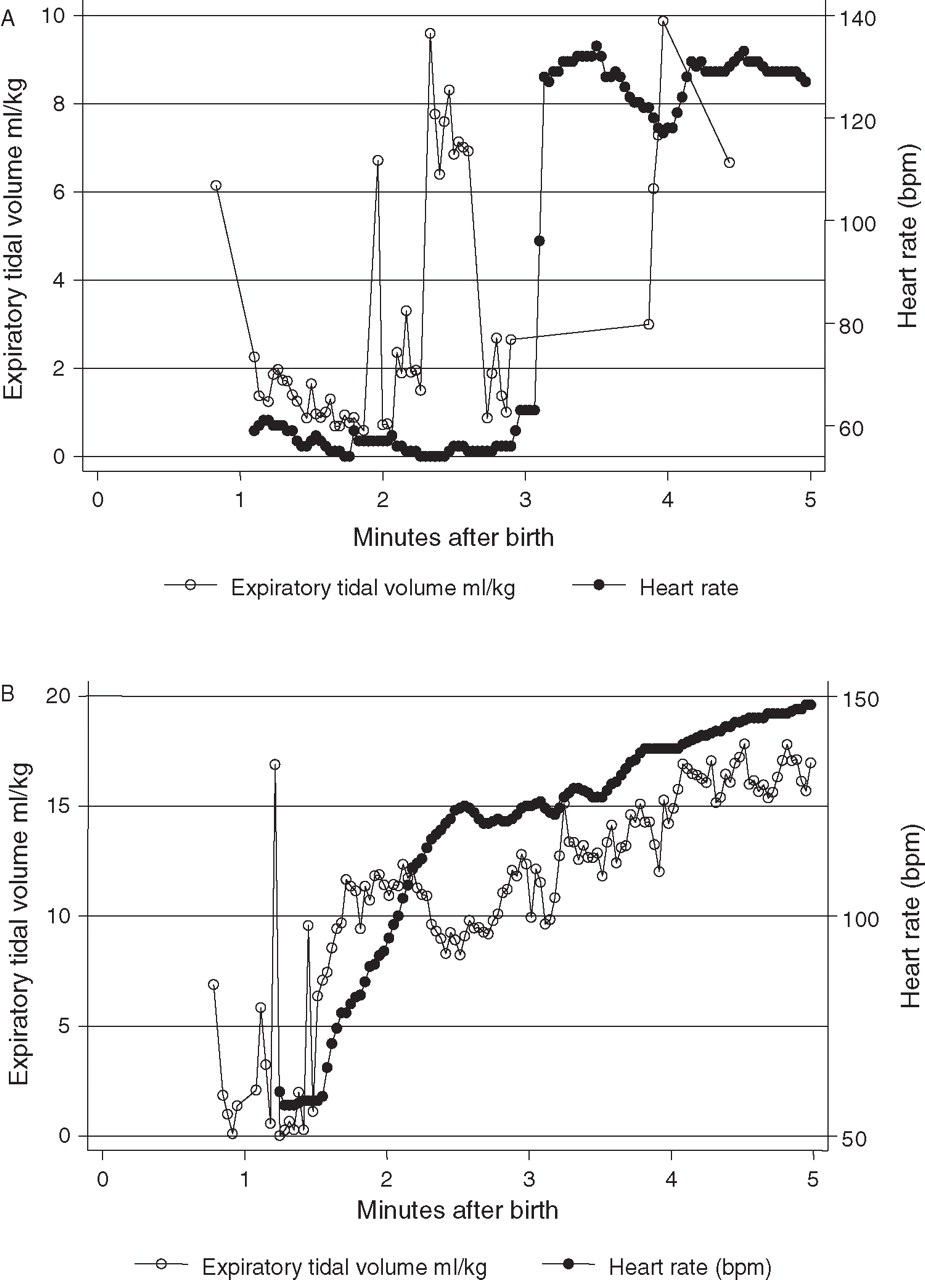
(A) Illustrates an example of a rapid rise in heart rate (HR) in a 27 week 990 g infant. In this example there is an ‘instant’ rise in HR from 57 to 122 bpm over 5 s. (B) Illustrates an example of a gradual rise in HR in a 26 week 575 g infant. In this example it takes nearly 60 s for the HR to rise from 50 to 125 bpm.
Post hoc analysis
There were two infants who took more than 5 min to achieve the target HR. Both had received two intubation attempts within 90 s. Both were delivered by caesarean section under epidural anaesthesia for maternal hypertension. The first infant (27 week 820 g male) was randomised to the T-piece; HR rose rapidly to 100 bpm within 10 s but remained between 100 and 115 bpm until a second successful intubation, thus taking a total of 478 s from commencement of PPV to reach HR ≥ 120 bpm. The second infant (28 week 980 g male) received PPV via a SIB and had a persistently low HR of <100 bpm. HR rose rapidly following the second successful intubation to 155 bpm, after 386 s of PPV. Both infants were included in analysis as they were typical of scenarios which occur in the DR and there were no demographic factors distinguishing them from the rest of the cohort.
Figure 3 illustrates the HR, VTe and leak from a 1080 g 29 week infant receiving PPV from a T-piece. In this infant the HR did not rise until VTe was above 4 ml/kg and leak was reduced. However, for the cohort there was no statistically significant relationship between leak and time to reach HR ≥120 bpm (correlation coefficient=−0.14, r2=0.08, p=0.91).

{kind=link}
{kind=link}
{kind=link}
Illustrates the heart rate, expired tidal volume and mask leak in a 29 week 1080 g week infant receiving positive pressure ventilation from a T-piece.
In the 13 intubated infants there was no difference in HR, SPO2 or FiO2 in the 30 s before and the first 30 s after intubation. (Median (IQR) HR (bpm) 154 (126–163) versus 158 (127–170) (p=0.51) pre versus post-intubation respectively; median (IQR) SPO2 72 (50–85) versus 72 (41–91) (p=0.71)) pre versus post-intubation respectively). Median (IQR) oxygen concentration (%) was 100 (90–1.00) versus 96 (46–100) pre versus post-intubation (p=0.51). Following intubation infants received inflations with a lower median (IQR) VTe ml/kg when compared with inflations given prior to intubation. (Preintubation vs postintubation inflations median (IQR) VTe ml/kg 7.8 (1.6–16.5) and 6.1 (4.6–7.6) p=0.03)
Discussion
A small number of newly born infants require assistance to breathe after birth8. ILCOR recommends that infants with bradycardia (HR <100 bpm) should be given PPV.1 Clinical assessment of effectiveness of PPV includes an improving HR, adequate chest excursion, auscultation of bilateral breath sounds and improving muscle tone. HR is considered an important clinical sign indicating the need for and efficacy of neonatal resuscitation.6 However, we could find little evidence describing the relationship between HR and efficacy of PPV during resuscitation of infants <30 weeks gestation.9 In our study of preterm infants with a HR <100 bpm we measured the time taken for HR to reach >120 bpm. The HR targets in our study were based on the knowledge that HR varies between 110 and 160 bpm in healthy term infants10 and that HR is relatively lower in preterm infants.11 We defined a HR remaining above 120 bpm as indicating cardiorespiratory stability.
We identified two distinct patterns in HR rise, a rapid rise and a gradual rise. A rapid rise was defined as an increase in HR from <100 bpm to >120 bpm within 5 s. Infants experiencing a gradual HR rise took at least 60 s for their HR to reach >100 bpm. Both patterns have previously been reported by Palme-Kilander9 12 in infants receiving respiratory support.
The rapid rise in HR rise is consistent with observations of a vagal reflex seen in earlier studies of asphyxiated animal models by Dawes.13 Several authors including, Anrep14 and Angell-James3 described the pulmonary vagal inflation reflex in their animal models. This reflex may be modulated by extrinsic (effectiveness of PPV) or intrinsic (secondary apnoea and depressed reflexes) factors. In particular, infants with primary apnoea are more responsive to stimulation, as opposed to infants with secondary apnoea who are more likely to experience a more gradual rise in HR. The latter group are more severely compromised and hence reliant on assisted ventilation to recover.6 These factors collectively may explain why the increase in HR occurred at variable lengths of time after the commencement of PPV.
Animal models generally describe the effect of asphyxia on term animals. The median (IQR) cord pH for infants in our study was 7.29 (7.22–7.34). Therefore, very few of our infants were asphyxiated however they were all very preterm with disease process (stiff lungs, reduced surfactant, compliant chest wall and poor respiratory effort) related to prematurity that may contribute to a delay in developing adequate pulmonary gas exchange.
All preterm infants in our study received PPV, initially by facemask and some infants via endotracheal tube. It is possible that PPV stimulated Head's paradoxical reflex promoting an increase in spontaneous breathing efforts. We observed high VT being delivered just prior to and during the sudden HR rise in some infants. We hypothesise that these large volumes may be responsible for eliciting this vagal reflex, which is consistent with observations by Anrep in 1936.14 We observed pauses in PPV due to interventions and clinical assessments, for example, removing the facemask to observe an infant's spontaneous breathing, oropharyngeal suction and auscultation of the heart and/or lungs. After each pause it may take several inflations to overcome dead space in the facemask, reducing the development of a functional residual capacity.
We found that the median time taken for the cohort to reach HR of 120 bpm is much longer than the time taken to reach 100 bpm. We observed infants whose HR did not stabilise until it ≥120 bpm. In 18/27 (67%) infants the HR did not remain stable until a threshold of approximately 150 bpm was reached. This suggests that the critical threshold for stabilisation of HR in the newborn should be greater than the 100 bpm currently recommended.1
The lack of correlation between time of HR rise and delivered VT was an unexpected finding and is contrary to the suggestion that VT between 4 and 8 ml/kg15 and minimising mask leak during PPV16 might improve ventilation and thus HR. During mask ventilation in the DR, resuscitators are unable to accurately assess mask leak or delivered VT.17 Following intubation preterm infants in our current study received more inflations within the 4 to 8 ml/kg range.
In this study we relied on the PO to measure HR. PO is gaining acceptance as a tool in the DR.18,–,21 The accuracy of the PO in detecting HR <60 bpm is unknown. However, Kamlin22 has shown that HR measured by PO has a sensitivity of 89% and specificity of 99% when compared to an ECG in detecting a HRECG <100 bpm in the DR setting.
An additional tool to assess effectiveness of ventilation is continuous measurement of exhaled carbon dioxide. This technique might have provided additional information about pulmonary gas exchange. However, we did not record this in the current study.
The relatively small number of subjects may have exaggerated any inherent variations in the data collected in the cohort.
In summary, it takes more than a minute for newly born bradycardic infants <30 weeks gestation to achieve a HR more than 100 bpm. We found that HR did not stabilise until it reached 120 bpm. Our findings suggest that current recommendations regarding the use of HR as a parameter to monitor effectiveness of PPV may need revision. This study builds on previous animal studies, providing a foundation upon which the interventions required to reverse bradycardia in newly born infants can be further explored. Further studies including term infants and recruiting a larger sample size are required to better understand these complex relationships.
References
Footnotes
-
Funding JAD and GMS are past recipients of RWH Postgraduate Scholarships. GMS is a recipient of a Monash University International Postgraduate Research Scholarship. PGD has an NHMRC Practitioner Fellowship. PGD and CJM hold an NHMRC Program Grant No. 384100 which partially funded this work.
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the The Royal Women's Hospital Research and Ethics Committees.
-
Provenance and peer review Not commissioned; externally peer reviewed