Article Text

Statistics from Altmetric.com
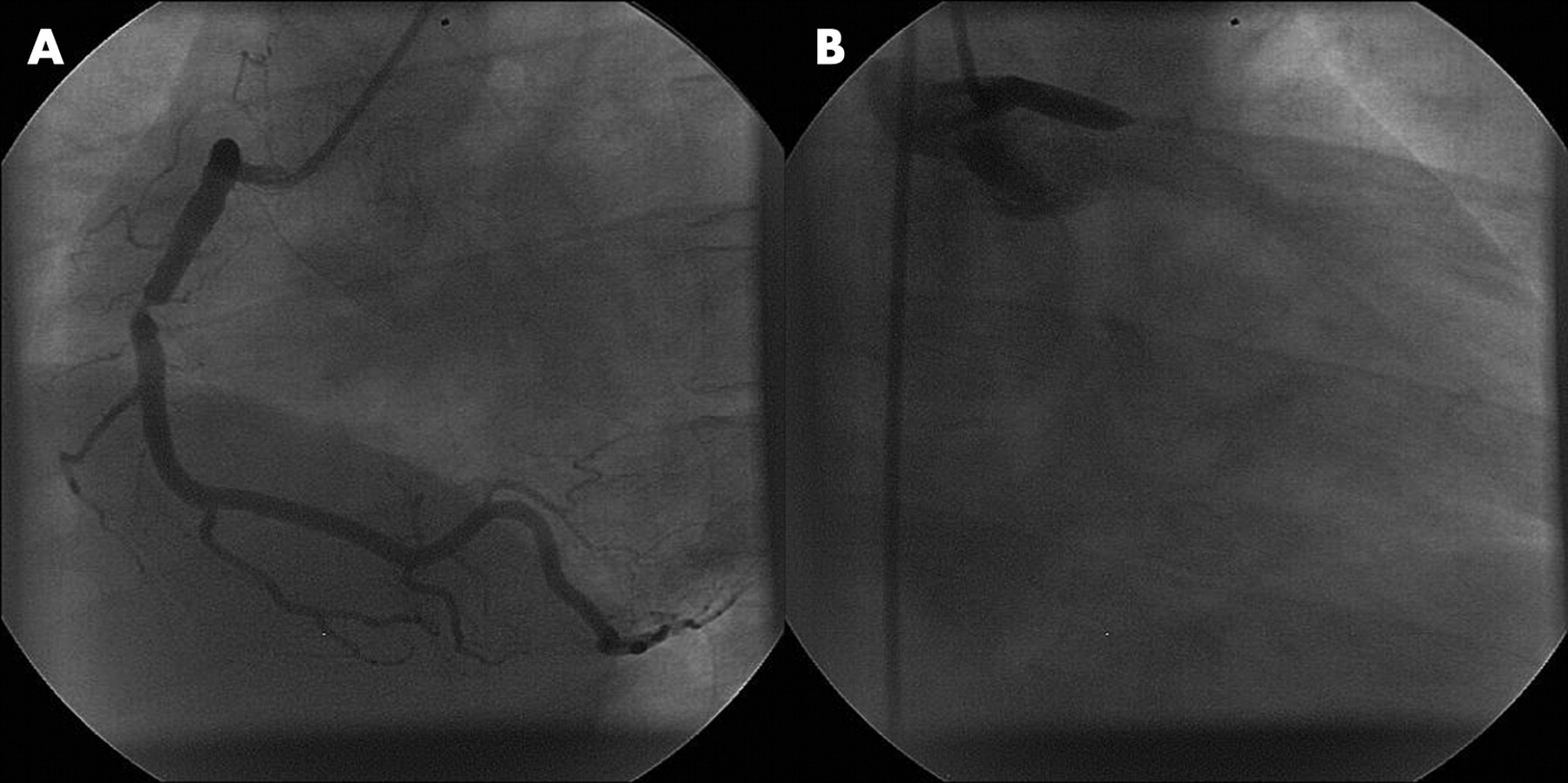
A 40-year-old man presented with severe chest pain. The electrocardiogram showed extensive anterolateral ST elevation. His blood pressure was 110/90 mm Hg. Emergency coronary angiography demonstrated a severe right coronary artery (RCA) stenosis and left main (LM) stem occlusion (panels A and B). After the first balloon inflation (59 minutes from pain onset), abciximab and intra-aortic balloon counterpulsation (IABP), a 4.0×16 mm Taxus stent was implanted in the LM stem. There was impaired antegrade flow despite a good angiographic result. IABP and inotropic support continued for 72 hours.

{kind=link}
{kind=link}
{kind=link}
Coronary angiography 1 week later demonstrated a good result of LM stenting. Using a FilterWire EZ, the RCA lesion was directly stented with a 4.5×16 mm Taxus stent (panels C and D). Left ventriculography showed mildly impaired left ventricular (LV) dysfunction with an LV ejection fraction (LVEF) of 39% and LV end diastolic pressure (LVEDP) of 16 mm Hg.
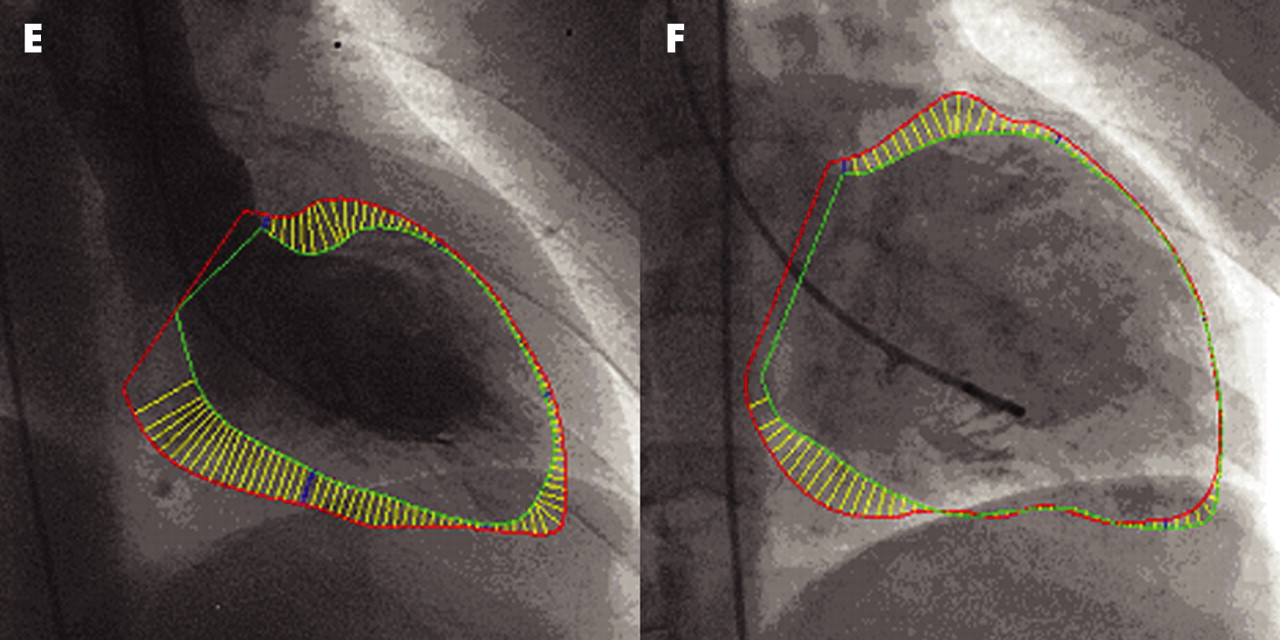
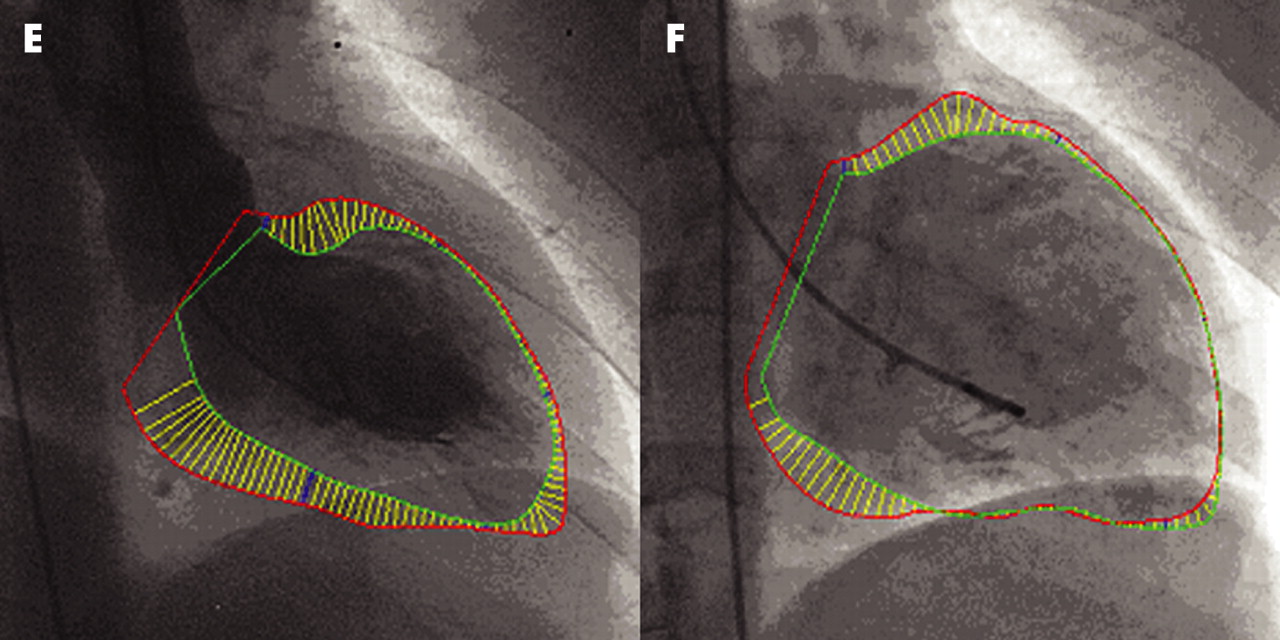
The patient had repeated admissions with breathlessness; however, hypotension limited treatment to rampril 2.5 mg and bisoprolol 2.5 mg. Nine months later the patient continued to complain of exertional dyspnoea. Repeat angiography demonstrated severe LV dysfunction with an LVEF of 19% and LVEDP of 38 mm Hg (panels E and F). Referral for heart transplantation was made.
Emergency restoration of coronary flow probably saved this patient’s life. However, the consequence of such extensive global ischaemia was severe LV hypotension, restricting prescription of ACE inhibitors and β blockers. Subsequent adverse LV remodelling resulted in further deterioration of LV performance. This case illustrates a potential future role for catheter implantable LV assistance devices which might facilitate early revascularisation and maintain circulation in the weeks after major myocardial infarction.
Acknowledgments
This article has been adapted from van Gaal W J, Jennings B R, Banning A P. Late adverse ventricular remodelling as a consequence of acute left main coronary artery occlusion Heart 2007;93:1019