Effectiveness of quadrivalent human papillomavirus vaccine for the prevention of cervical abnormalities: case-control study nested within a population based screening programme in Australia
BMJ 2014; 348 doi: https://doi.org/10.1136/bmj.g1458 (Published 04 March 2014) Cite this as: BMJ 2014;348:g1458
- Elizabeth Crowe, public health physician12,
- Nirmala Pandeya, biostatistician1,
- Julia M L Brotherton, public health physician and medical epidemiologist3,
- Annette J Dobson, biostatistician1,
- Stephen Kisely, public health physician4,
- Stephen B Lambert, public health physician56,
- David C Whiteman, cancer epidemiologist17
- 1The University of Queensland, School of Population Health, Brisbane, Australia
- 2NHS Borders, Department of Public Health, Melrose, Scotland, UK
- 3Victorian Cytology Service, Melbourne, Victoria, Australia
- 4The University of Queensland, Rural and Southern Clinical Schools, Wooloongabba, Australia
- 5Queensland Children’s Medical Research Institute, The University of Queensland and Children’s Health Queensland, Brisbane, Australia
- 6Queensland Health Immunisation Program, Brisbane, Australia
- 7QIMR Berghofer Medical Research Institute, Population Health Department, Brisbane, Australia
- Correspondence to: E Crowe NHS Borders, Department of Public Health, Melrose, Scotland, UK e.crowe1{at}uq.edu.au
- Accepted 31 January 2014
Abstract
Objective To measure the effectiveness of the quadrivalent human papillomavirus (HPV) vaccine against cervical abnormalities four years after implementation of a nationally funded vaccination programme in Queensland, Australia.
Design Case-control analysis of linked administrative health datasets.
Setting Queensland, Australia.
Participants Women eligible for free vaccination (aged 12-26 years in 2007) and attending for their first cervical smear test between April 2007 and March 2011. High grade cases were women with histologically confirmed high grade cervical abnormalities (n=1062) and “other cases” were women with any other abnormality at cytology or histology (n=10 887). Controls were women with normal cytology (n=96 404).
Main outcome measures Exposure odds ratio (ratio of odds of antecedent vaccination (one, two, or three vaccine doses compared with no doses) among cases compared with controls), vaccine effectiveness ((1−adjusted odds ratio)×100), and number needed to vaccinate to prevent one cervical abnormality at first screening round. We stratified by four age groups adjusted for follow-up time, year of birth, and measures of socioeconomic status and remoteness. The primary analysis concerned women whose first ever smear test defined their status as a case or a control.
Results The adjusted odds ratio for exposure to three doses of HPV vaccine compared with no vaccine was 0.54 (95% confidence interval 0.43 to 0.67) for high grade cases and 0.66 (0.62 to 0.70) for other cases compared with controls with normal cytology, equating to vaccine effectiveness of 46% and 34%, respectively. The adjusted numbers needed to vaccinate were 125 (95% confidence interval 97 to 174) and 22 (19 to 25), respectively. The adjusted exposure odds ratios for two vaccine doses were 0.79 (95% confidence interval 0.64 to 0.98) for high grade cases and 0.79 (0.74 to 0.85) for other cases, equating to vaccine effectiveness of 21%.
Conclusion The quadrivalent HPV vaccine conferred statistically significant protection against cervical abnormalities in young women who had not started screening before the implementation of the vaccination programme in Queensland, Australia.
Introduction
Two prophylactic human papillomavirus (HPV) vaccines are currently available worldwide. Phase III studies have shown that both the quadrivalent vaccine, targeted against HPV types 6, 11, 16, and 18, and the bivalent vaccine, targeted against types 16 and 18, prevent cervical lesions associated with the respective HPV types.1 2 3 4 Some cross protection against other HPV types has also been shown.5 6 7 The quadrivalent vaccine also prevents high grade vulval and vaginal lesions and genital warts in women, as well as genital warts and high grade anal disease in men.1 2 Efficacy against cervical abnormalities was greatest in the population of women who tested negative for the relevant vaccine HPV types at enrolment, as the vaccine does not seem to impact on the clinical course of existing infections. Although clinical trials conducted in controlled settings have shown the efficacy of the quadrivalent vaccine, less is known about the vaccine’s effectiveness when delivered to the broader population.
Prophylactic HPV vaccination programmes have been implemented in over 40 countries.8 Australia was the first country to implement a publicly funded national vaccination programme with the quadrivalent HPV vaccine in April 2007. As well as initiating an ongoing programme for 12 and 13 year old girls, an extensive catch-up programme was implemented and ran until December 2009. The school based catch-up programme targeted 12-17 year olds, whereas the community catch-up phase offered vaccination to women aged 18 to 26 years in general practice and community settings. The school based programme achieved vaccination rates of 84%, 79%, and 70% for one, two, and three doses, respectively, while the corresponding rates for the community programme were 64%, 53%, and 33%.9 We estimated the effectiveness of full and partial courses of quadrivalent HPV vaccine against high grade and other cervical abnormalities in the population of Queensland women targeted by both the school and the community based catch-up vaccination programmes in the first four years after their introduction.
Methods
Study overview and population
We performed a case-control analysis using linked, anonymised data obtained from population registers in Queensland, Australia, for a four year period after the introduction of the HPV vaccination programme in April 2007. The study population comprised all female Queensland residents who attended for their first ever cervical smear test between 1 April 2007 and 31 March 2011 and who had been eligible for HPV vaccination during the nationally funded catch-up programme—that is, those born between July 1980 and July 1997.
Our primary objective was to estimate the effectiveness of the quadrivalent vaccine in the population of sexually naïve young women with no previous infection. Information on sexual history was not available from study participants. The Australian national cervical screening programme recommends that cervical screening should start between the ages of 18 and 20 in women who have ever been sexually active, or one or two years after first having sexual intercourse, whichever is later.10 To best realise our objective using the data available, we restricted our study to women who presented for their first smear test.
Sampling frame
We determined case-control status from cytology and histology test results as recorded on the Queensland Health Pap Smear Register. This depository is an “opt off” register, which has stored results since 199911 and is estimated to contain data for 98.5-99.5% of all Queensland women participating in the cervical screening programme.12 Cervical cytology results are coded by reporting laboratories according to the Australian standard modified Bethesda coding schedule and electronically forwarded to the register.
Case-control definitions
We defined two case groups (table 1⇓) based on the first abnormal test result returned by a woman during the study period. High grade cases were those women who had a high grade cervical abnormality (cervical intraepithelial neoplasia 2 or adenocarcinoma in situ, or worse) confirmed by histology during the study period. We took the index date to be the date of the abnormal cytology test result immediately preceding the histology test result satisfying the high grade case definition, because from that point women entered a phase of diagnostic testing. “Other cases” were those women who did not meet the high grade case definition but had any other abnormality (either a low grade abnormality at histology or an abnormal cytology result that was not confirmed by histology). Thus, other cases included women with high grade cytological abnormalities who did not have subsequent histological testing during the study period, as well as women whose subsequent histology identified only a low grade abnormality or a negative finding. We classified cases with simultaneous squamous and endocervical abnormalities according to the endocervical abnormality. Endocervical abnormalities were judged to be more important because they are rare, always an indication for diagnostic testing, and of particular interest because cervical screening is not sensitive in detecting and preventing adenocarcinoma. The index date for other cases was the date of the first cytological abnormality to occur in the study period.
Frequency of cytological and histological diagnoses for cases, 1 April 2007 to 31 March 2011, primary analysis
We assigned control status to the remaining women. By definition all controls had only negative cytology results during the study period. A negative cytology test result consisted of a negative result for the squamous component and negative or unsatisfactory result for the endocervical component. A woman provided control data only once.
Source of exposure information and exposure definitions
Our exposure of interest was receipt of the HPV vaccine before the index date, as recorded on the Queensland Health Vaccination Information Vaccination Administration System. The register includes several mandatory fields: name, date of birth, address, practitioner and clinic details, date of vaccination, type of vaccine, and dose number. Dose dates are recorded against the relevant dose number, as reported by the healthcare provider. A complete vaccination course consists of three doses over a 4-6 month period. We considered a vaccine dose to be valid if administered in line with national guidelines for minimum intervals, and a woman to be fully vaccinated if no more doses were clinically indicated.13 We also excluded individual doses that were subject to a cold chain breach (that is, the vaccine stored outside of the recommended temperature range) or were duplicate vaccine doses (where the same dose date was recorded more than once per woman). We defined women as unvaccinated (no doses), partially vaccinated (one or two doses), or fully vaccinated (≥3 doses) where receipt of vaccine doses occurred at any point before the index date.
Data linkage
Extracts from the Queensland cervical smear register and Queensland vaccination administration system were sent for linkage to Queensland Health Data Linkage Unit. The unit used the LinkageWiz software package to probabilistically identify potentially matching records for each woman. Weighting scores were assigned to matching variables, including full name, sex, date of birth, and address. The linkage generated a total of 287 224 potential matches (pairs) with weighting scores between 12 and 35. Of these, 249 885 pairs (87.0%) were automatically accepted because of a weighting score of more than 19 or an exact match on full name and address or full name and date of birth. The remaining 37 339 pairs were reviewed; 27 257 (73.0%, 9.5% overall) were accepted as true pairs and 10 082 (27.0%, 3.5% overall) were rejected. We received an anonymised linked dataset.
Ineligibility and exclusions
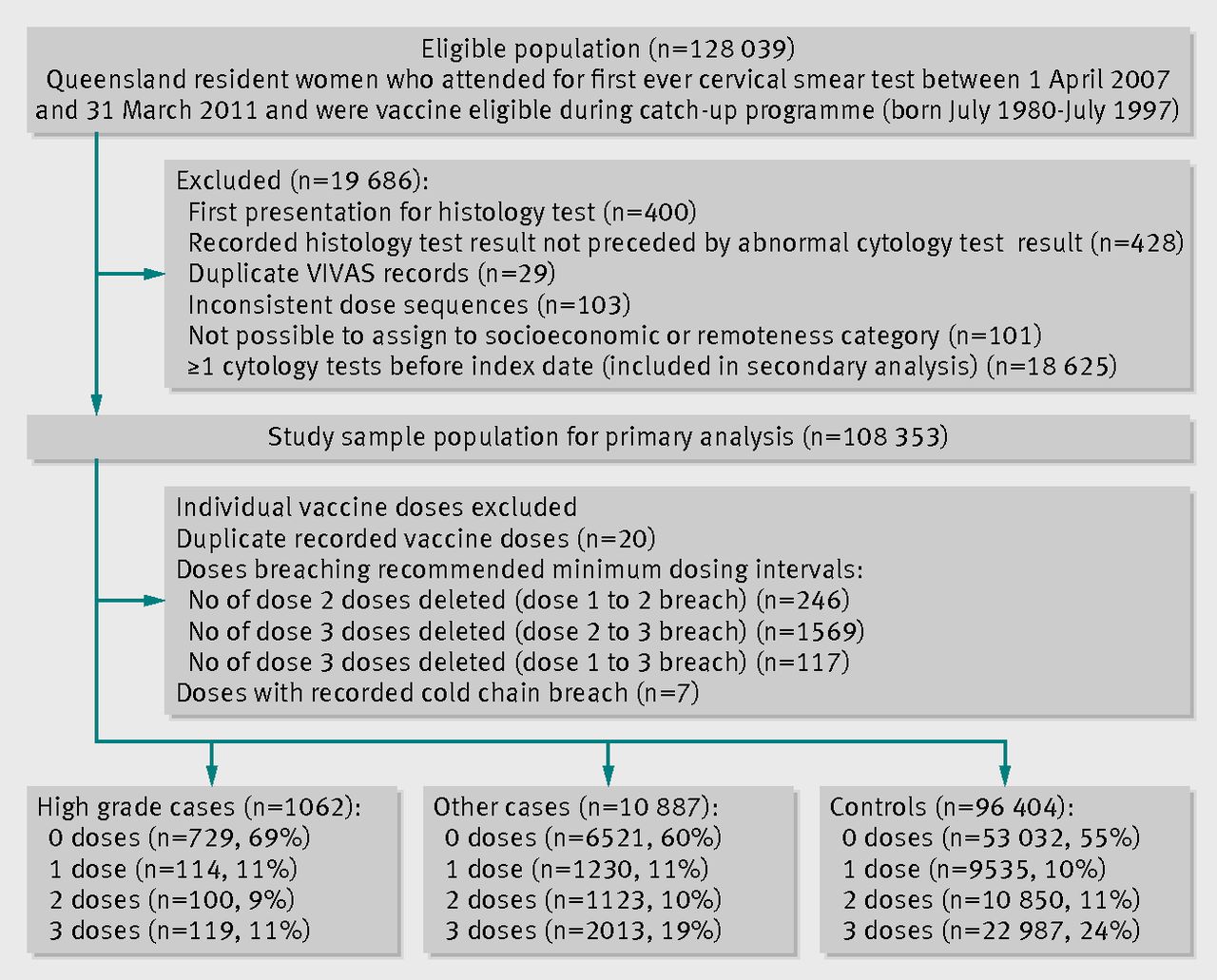
We excluded women whose first record in the cervical smear register was for a histology test result, and women who had any of the following characteristics: a recorded histology test during the study period that was not preceded by a record of an abnormal cytology test, duplicate records in the vaccination administration system that could not be combined into one record, inconsistent vaccination records (for example, an unreliable sequence of vaccination dose dates), or a postcode that was not possible to assign to a socioeconomic or remoteness category. We excluded cytology and histology tests that were reported as unsatisfactory for clinical reporting purposes. The figure⇓ and supplementary figure 1 on bmj.com show the numbers of women in each of these exclusion categories.

Eligibility and exclusions, primary analysis. VIVAS=Queensland Health Vaccination Information Vaccination Administration System
{kind=link}
Covariates
For measures of remoteness and socioeconomic status, we assigned women to a category according to the 2006 Australian Bureau of Statistics (ABS) Remoteness Area (a measure of the remoteness of a location from the services provided by large towns or cities) and to a 2006 ABS Index of Relative Socioeconomic Disadvantage quintile based on current residential postcode on the Queensland cervical smear register. We calculated the median follow-up time from study start date to index date for the study population overall and assigned women to follow-up time quartiles. We included year of birth as a covariate. No information was available on other potential confounders, such as lifestyle factors, from the administrative datasets.
Statistical analysis
Analyses were conducted for all women and within strata of four age groups (at 2007): 11-14 years, 15-18 years, 19-22 years, and 23-27 years. We restricted our primary analysis to those women who had no cytology tests before their index date (women whose first ever smear test result defined their status as a case or control). This was because the number of previous cytology tests differed between cases and controls. Our secondary analysis comprised cases and controls with one or more cytology tests before their index date. For the secondary analysis, we randomly selected an index date for controls from all negative test results to minimise any opportunity for exposure bias. Such a bias might otherwise have occurred had we used the last test result available, allowing control women to be in the study longer and therefore have more opportunity to become vaccinated than cases.
Our measure of association was the exposure odds ratio—that is, the ratio of exposure odds among cases to the exposure odds among controls. We estimated the exposure odds ratio for each vaccination dose compared with no vaccination using multinomial logistic regression models for each of the two mutually exclusive case categories (high grade cases, other cases) compared with controls. We adjusted for potential confounding by socioeconomic status, remoteness, age, and follow-up time. We estimated vaccine effectiveness and associated 95% confidence intervals using the formula (1−adjusted odds ratio)×100. We calculated approximate point and interval estimates of the number needed to be vaccinated to prevent one cervical abnormality at first screening round using multiple logistic regression with adjustment for confounding variables, according to the method of Bender and Blettner.14 We used SAS statistical software (version 9.4) for all data cleaning and analyses.
Sensitivity analyses
We tested the impact of excluding cases and controls in whom the time interval (latent period) between date of last vaccination and index date was shorter than nominated latent periods. We assumed putative latent periods of 30, 180, and 365 days based on uncertainties about the timing of immune responses to HPV vaccination and the interval between infection and neoplasia.15 16 Because the date of origin of a cervical lesion cannot be known with certainty, it is possible that our decision to define the event date as the cytology test result immediately preceding the abnormal histology result may have introduced bias. We therefore repeated our secondary analyses using the date of the first abnormal cytology test result as the index date for high grade cases.
It was possible for a woman to have no record of a first or second vaccine dose but records for subsequent doses. In our initial analysis, we assigned exposure status using the actual number of doses that had dates recorded against them, ignoring provider assigned dose numbers. We repeated all analyses after reassigning exposure status based on the last dose number for which there was a valid dose date occurring before the index date, analogous to the “third dose assumption” used to estimate coverage of primary course vaccines in children.17
Results
Participants
In total, 108 353 women were eligible for inclusion in the primary analysis: 1062 (1.0%) high grade cases, 10 887 (10.0%) other cases, and 96 404 (89.0%) controls (figure). See supplementary figure 1 on bmj.com for the numbers included in the secondary analysis. The median follow-up time from study start date to index date for women in the primary analysis was 808 days (interquartile range 456-1131 days) for controls, 654 (313-1038) days for other cases, and 766 (381-1087) days for high grade cases. Cases were older, more disadvantaged, and less likely to live in major cities than controls (table 2⇓). These differences were more pronounced for high grade cases. Supplementary table 1 on bmj.com presents the characteristics for women in the secondary analysis. Table 1 presents the histological and cytological diagnoses for cases (see supplementary table 2 on bmj.com for secondary analysis). For the primary analysis 11.2% of high grade cases (n=119), 18.5% of other cases (n=2013), and 23.8% of controls (n=22 987) were fully vaccinated (≥3 doses) before their index date (figure). Fully vaccinated women were younger at first vaccine dose (median age 17.0 years (interquartile range 16.0-19.4 years) than partially vaccinated women (19.6 (18.0-22.4) years for two doses; 21.0 (19.1-23.7) years for one dose).
Comparison of characteristics of cases and controls, 1 April 2007 to 31 March 2011, primary analysis. Values are numbers (percentages) unless stated otherwise
Vaccine effectiveness estimates
The largest difference between crude and adjusted estimates was made by adjusting for year of birth. Effect estimates were essentially unchanged after adjustment for remoteness and socioeconomic status in both the primary and secondary analysis.
The primary analysis was of women who had no cytology tests before their index date. In this analysis, the adjusted odds ratios for exposure to three doses of HPV vaccine compared with no vaccine were 0.54 (95% confidence interval 0.43 to 0.67) for high grade cases and 0.66 (0.62 to 0.70) for other cases compared with controls with normal cytology (table 3⇓), equating to vaccine effectiveness of 46% (95% confidence interval 33% to 57%) and 34% (30% to 38%), respectively. The adjusted numbers needed to vaccinate (three doses) to prevent one cervical abnormality at first screening round were 125 (95% confidence interval 97 to 174) and 22 (19 to 25), respectively. We observed variation in estimates across age strata, with significantly reduced odds of full vaccination in high grade cases aged 15 to 18 years and 19 to 22 years, and little evidence of any vaccine effect among vaccinated women in the oldest age stratum (exposure odds ratio 0.95, 95% confidence interval 0.63 to 1.45). The adjusted odds ratios for exposure to two vaccine doses were 0.79 (0.64 to 0.98) for high grade cases and 0.79 (0.74 to 0.85) for other cases, equating to vaccine effectiveness of 21% (table 3). We found no statistically significant effectiveness of one dose for high grade or other cases. Adjusted effectiveness of one or more vaccine doses against a high grade cervical abnormality was 26% (15% to 36%) and against any other abnormality was 22% (18% to 25%).
Effectiveness of quadrivalent human papillomavirus (HPV) vaccine by number of doses, stratified by age in 2007, primary analysis
The secondary analysis was of women who had one or more cytology tests before their index date. For this analysis the adjusted odds ratios for exposure to three doses of HPV vaccine compared with no vaccine were 0.77 (0.64 to 0.92) for high grade cases and 0.81 (0.72 to 0.91) for other cases (see supplementary table 3 on bmj.com). The adjusted numbers needed to vaccinate were 38 (23 to 104) and 24 (16 to 50), respectively. Effectiveness of two doses did not reach statistical significance. Adjusted effectiveness of one or more vaccine doses against a high grade cervical abnormality was 18% (4% to 30%) and against any other abnormality was 15% (6% to 23%).
Sensitivity analyses
Vaccine effectiveness estimates for three doses were essentially unchanged when we assumed latent periods of 30, 180, and 365 days (see supplementary tables 4-6 on bmj.com); however, the effectiveness of two doses seemed to increase with assumed latent periods of 180 and 365 days.
Vaccine effectiveness remained essentially unchanged in sensitivity analyses in which we used last dose number to assign exposure status rather than number of doses recorded on the register (see supplementary table 7 on bmj.com). Finally, in the secondary analysis, vaccine effectiveness was also unchanged when we defined the index date for high grade cases as the date of their first ever abnormal cytology test result in the study period rather than the cytology test result immediately preceding the abnormal histology test result (data not shown).
Discussion
Key findings and comparison with other studies
Four years after the introduction of a routine and catch-up vaccination programme against human papillomavirus (HPV), we estimated that the quadrivalent vaccine provided 46% protection against histologically confirmed high grade cervical abnormalities and 34% protection against other cervical abnormalities in women who had not started screening before vaccination. The numbers needed to vaccinate to prevent one cervical abnormality at first screening round were 125 for a histologically confirmed high grade abnormality and 22 for other abnormalities. We found that partial vaccination with two doses provided 21% protection against both high grade and other cervical abnormalities.
These findings are in accord with recent studies indicating that approximately 52% of high grade cervical abnormalities are due to HPV 16 and HPV 18.18 This attributable fraction is the theoretical upper limit of vaccine efficacy, unless cross protection against other HPV types provides additional protection. Vaccine effectiveness in the population setting would therefore be expected to be lower than this ideal, owing to imperfect implementation, previous exposure, and other factors.19
Our vaccine effectiveness estimates for one or more vaccine doses (primary analysis: 26% against high grade abnormality, 22% against any other abnormality; secondary analysis: 18% against high grade abnormality, 15% against any other abnormality) are most comparable, and are similar, to phase III trial intention to treat analyses, which reported efficacy of one or more vaccine doses against all HPV related disease (including disease cases due to non-vaccine type) in the population that included women already infected with vaccine type HPV but without disease at recruitment. In women vaccinated with one or more doses the proportion of histologically confirmed high grade lesions decreased by 19% (95% confidence interval 7.7% to 28.9%) and all categories of cervical smear abnormalities decreased by 11.3% (6.5% to 15.9%).20 Both the slightly longer follow-up time and the differences between our population and the trial populations could account for the higher effectiveness estimates in our primary analysis. Our population may contain a higher proportion of HPV naïve women than the trial populations because we excluded women who had attended screening before their index date. Women new to screening may be closer to sexual debut than women who have been regularly screened and for longer, despite having a history of only negative cytology results. Both relative and absolute estimates of vaccine effectiveness are encouraging after a short duration following the introduction of the national programme.
Data on the effectiveness of partial vaccination against cervical abnormalities are limited as such efficacy was not assessed in clinical trials. Although this analysis indicates that three vaccine doses are required for optimal protection, our data suggest reasonable effectiveness with fewer doses. Partially vaccinated women were older than fully vaccinated women and therefore more likely to have been infected with HPV before vaccination. We may therefore have underestimated the effectiveness of partial vaccination. Further research is needed to establish whether optimised two dose schedules are adequate.
We found that relative vaccine effectiveness was lower in the secondary analysis in the population of women with one or more cytology test results before their index date (that is, who met the case definition on subsequent screening rounds) compared with women in the primary analysis with no previous tests. High grade cases in particular were statistically significantly more likely to have had one or more previous tests. Australian guidelines recommend that women who have a low grade abnormality on cervical smear testing should undergo repeat testing to assess clearance (usually at 12 months) before proceeding to colposcopy and biopsy. Because of these screening recommendations, and given the clinical course of HPV infection, it is not surprising that women with high grade abnormalities are more likely than other women to have had preceding cytology tests. We found that the number needed to vaccinate to prevent one high grade cervical abnormality was lower among women with a screening history than among women with no previous screening history (38 v 125). This is likely to be because the incidence of high grade abnormalities is higher in this group of women and reflects the fact that unlike the exposure odds ratio, the number needed to vaccinate is a measure that is influenced by both effect size and outcome incidence. Our finding also accords with a subanalysis from the trials indicating a benefit of vaccination even in women already treated for cervical disease.21 The number needed to vaccinate to prevent one other cervical abnormality, however, was similar in women both with and without a history of smear tests (24 v 22).
Strengths and limitations of this study
Our study used administrative databases, which avoid some of the reporting and selection biases that can occur in interview based studies. Inclusion of both the school and the community based catch-up programmes enabled a comprehensive evaluation of the effect of the vaccination with adequate power to assess outcomes for those women who only received one or two doses. Consistent with known risk factors for cervical abnormalities, cases were older, more disadvantaged, and less likely to live in major cities than controls. Because age, socioeconomic status, and remoteness were associated with case status and are likely to be associated with cervical screening, we stratified our analyses by age group and included terms for year of birth, measures of socioeconomic status and remoteness, and index date. We used cumulative incidence sampling in which controls were defined by having no abnormal cytology test results throughout the study period. We were concerned about possible exposure opportunity bias, whereby control participants may have had systematically greater opportunity for vaccination owing to longer duration in the cohort overall. We controlled for this in two ways. Firstly, we included a term for follow-up time in the analysis. Including this term in the primary analysis attenuated estimates of vaccine effectiveness by up to 20% for other cases, but had a negligible impact on estimates for high grade cases. Secondly, in our secondary analysis, among control women (defined as having persistently negative smear test results), the index date was randomly selected from among their negative screens using a computer algorithm.
Our study has some limitations. Misclassification of exposure status in some women is likely to have occurred owing to inaccuracies in vaccine register data and those arising from data linkage. One quarter of women aged 19-26 years and 12% of women aged 12-18 years recorded on the vaccine register had no record of a first dose but had records of subsequent doses. This suggests either inaccuracy in reporting of dose numbers or under-reporting of vaccine doses by providers to the vaccine register. Proportions of women classed as vaccinated in our study are lower than national coverage statistics because our study included screening events that occurred during the delivery phase of the vaccination programme, and we counted only vaccine doses delivered before a woman’s index date. Some degree of under-linkage (failure to correctly assign a woman’s vaccination record to her smear test record) may have occurred during probabilistic linkage between registers owing to possible address or name changes as a result of marriage in this particular population. Over-linkage (that is, assigning a vaccination history to a woman erroneously) should, however, occur infrequently.22 We believe that under-linkage is likely to have occurred infrequently and to have been non-differential for cases and controls. Non-differential under-linkage or under-reporting could lead to underestimation of vaccine effectiveness. However it is possible that under-reporting occurred differentially because cases were older and therefore more likely to have been vaccinated as part of the community based programme (where under-reporting was higher). The potential impact of this would be to over-estimate vaccine effectiveness. We tested the impact of under-reporting of doses in sensitivity analyses, where possible, and found no statistically significant differences in our results (see supplementary table 7 on bmj.com).
We were able to control for a limited number of covariates in this analysis. It is possible that residual confounding by other factors may have occurred (for example, smoking or sexual activity); however, we consider it unlikely that any such confounding would be of sufficient magnitude and in the direction observed to explain these findings. Finally, generalisability of our findings to other population settings may be limited. Vaccine effectiveness will predominantly depend on the extent of previous infection and type specific HPV prevalence in the population cohort vaccinated. This will relate to age of sexual debut in relation to age at vaccination and vaccine coverage. Indeed, while we conclude that estimates of vaccine effectiveness in our youngest age group (11 to 14 years) are likely to be generalisable to the cohort of 12 year old girls targeted by the ongoing vaccination programme, it might be anticipated that effectiveness in this cohort of girls will be higher.
Conclusions and implications for policy
These population data suggest a risk reduction of 46% for histologically confirmed high grade cervical abnormalities and 34% for other cervical abnormalities among young women who were fully vaccinated with the quadrivalent HPV vaccine before starting screening. The adjusted numbers needed to vaccinate (three doses) to prevent one cervical abnormality at first screening round were 125 and 22, respectively.
At present, cervical screening will remain necessary in vaccinated populations owing to the relative type specificity of current vaccines. Falling population prevalence of cervical abnormalities will reduce the sensitivity and positive predictive value of cytological testing,23 and screening programmes will need to adapt to maintain their effectiveness. Our data suggest that this task is now becoming more urgent given the relatively rapid impact of the vaccine on disease in the real world setting. To tackle this, Australia is currently conducting a comprehensive review of cervical screening.24 Continued observation of this population is necessary to assess the implications for cervical screening recommendations in the coming era of mass vaccination.
What is already known on this topic
Vaccination programmes against human papillomavirus (HPV) have been implemented in over 40 countries
Although results from phase III trials show 98% efficacy of the quadrivalent vaccine against vaccine type related high grade cervical abnormalities, less is known about vaccine effectiveness against cervical abnormalities in population settings
What this study adds
The quadrivalent HPV vaccine was 46% effective against high grade cervical abnormalities and 34% effective against any other cervical abnormality in young women attending their first cervical screening after they were fully vaccinated at school or up to 27 years of age
Receipt of two vaccine doses provided some, although lesser, protection
The vaccine seemed more effective for preventing high grade abnormalities than other abnormalities and more effective in younger than older women
Notes
Cite this as: BMJ 2014;348:g1458
Footnotes
We thank the following units within Queensland Health for providing the data and conducting the linkage for this study: Communicable Diseases Branch, Cancer Screening Services Branch, Health Statistics Centre. We thank Claire DeBats, Nathan Dunn, Belinda Eagle, and Vicki Bryant for the data extraction. The provision of linked data was made possible through HealthLinQ, the Queensland node of the Population Health Research Network, funded by the Australian Government’s National Collaborative Research Infrastructure Strategy. This project was overseen by a steering group and we thank the following members for their contributions: Christine Selvey, Jennifer Muller, and Leane Christie. We thank Paddy Farrington for discussions on study design and analysis and Tim Patterson for his comments on earlier drafts. EC thanks the South East of Scotland Postgraduate Deanery and NHS Borders for support to undertake this research during postgraduate training.
Contributors: EC, AJD, SK, and DCW designed the study. EC is guarantor. EC and NP analysed the data. EC, JMLB, AJD, SK, SBL, NP, and DCW interpreted the data. EC wrote the first draft. JMLB, AJD, SK, SBL, NP, and DCW made substantial contributions to drafts of the manuscript and critically revised the report. All authors saw and approved the final version of the report.
Funding: No specific project funding was received but EC was supported by a salary from the University of Queensland and NHS Borders. DCW was supported by a Future Fellowship from the Australian Research Council (FT0990987). NP was supported by an early career fellowship from the National Health and Medical Research Council (631691). SK and AJD were supported by salaries from the University of Queensland. JMLB was supported by salary from the Victorian Cytology Service. SBL was supported by an early career fellowship from the National Health and Medical Research Council (GNT1036231) and is a Queensland Children’s Medical Research Institute senior research fellow supported by the Children’s Health Foundation Queensland (50025).
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: no support from any organisation for the submitted work. SBL has received research grants, travel funds, and payments from Merck, GSK, and BioCSL. JMLB has been a co-investigator on Australian HPV epidemiology grants that have received partial unrestricted funding from BioCSL and Merck. The University of Queensland receives royalties from the sale of Gardasil (Merck). There are no other relationships or activities that could appear to have influenced the submitted work.
Ethical approval: This study was approved by the University of Queensland medical research ethics committee (2010001247) and Queensland Health human research ethics committee (HREC/10/QHC/48).
Data sharing: No additional data available.
Transparency: EC affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/.