Restrictive versus liberal transfusion strategy for red blood cell transfusion: systematic review of randomised trials with meta-analysis and trial sequential analysis
BMJ 2015; 350 doi: https://doi.org/10.1136/bmj.h1354 (Published 24 March 2015) Cite this as: BMJ 2015;350:h1354
- Lars B Holst, medical doctor1,
- Marie W Petersen, medical student1,
- Nicolai Haase, medical doctor1,
- Anders Perner, professor1,
- Jørn Wetterslev, chief medical doctor2
- 1Department of Intensive Care 4131, Copenhagen University Hospital, Rigshospitalet, Blegdamsvej 9, DK-2100 Copenhagen, Denmark
- 2Copenhagen Trial Unit, Centre for Clinical Intervention Research 7812, Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark
- Correspondence to: L B Holst lars.broksoe.holst{at}regionh.dk
- Accepted 10 February 2015
Abstract
Objective To compare the benefit and harm of restrictive versus liberal transfusion strategies to guide red blood cell transfusions.
Design Systematic review with meta-analyses and trial sequential analyses of randomised clinical trials.
Data sources Cochrane central register of controlled trials, SilverPlatter Medline (1950 to date), SilverPlatter Embase (1980 to date), and Science Citation Index Expanded (1900 to present). Reference lists of identified trials and other systematic reviews were assessed, and authors and experts in transfusion were contacted to identify additional trials.
Trial selection Published and unpublished randomised clinical trials that evaluated a restrictive compared with a liberal transfusion strategy in adults or children, irrespective of language, blinding procedure, publication status, or sample size.
Data extraction Two authors independently screened titles and abstracts of trials identified, and relevant trials were evaluated in full text for eligibility. Two reviewers then independently extracted data on methods, interventions, outcomes, and risk of bias from included trials. random effects models were used to estimate risk ratios and mean differences with 95% confidence intervals.
Results 31 trials totalling 9813 randomised patients were included. The proportion of patients receiving red blood cells (relative risk 0.54, 95% confidence interval 0.47 to 0.63, 8923 patients, 24 trials) and the number of red blood cell units transfused (mean difference −1.43, 95% confidence interval −2.01 to −0.86) were lower with the restrictive compared with liberal transfusion strategies. Restrictive compared with liberal transfusion strategies were not associated with risk of death (0.86, 0.74 to 1.01, 5707 patients, nine lower risk of bias trials), overall morbidity (0.98, 0.85 to 1.12, 4517 patients, six lower risk of bias trials), or fatal or non-fatal myocardial infarction (1.28, 0.66 to 2.49, 4730 patients, seven lower risk of bias trials). Results were not affected by the inclusion of trials with unclear or high risk of bias. Using trial sequential analyses on mortality and myocardial infarction, the required information size was not reached, but a 15% relative risk reduction or increase in overall morbidity with restrictive transfusion strategies could be excluded.
Conclusions Compared with liberal strategies, restrictive transfusion strategies were associated with a reduction in the number of red blood cell units transfused and number of patients being transfused, but mortality, overall morbidity, and myocardial infarction seemed to be unaltered. Restrictive transfusion strategies are safe in most clinical settings. Liberal transfusion strategies have not been shown to convey any benefit to patients.
Trial registration PROSPERO CRD42013004272.
Introduction
Transfusion of red blood cells are often used to treat anaemia or bleeding in a variety of patient groups.1 2 3 Recent results of randomised clinical trials4 5 6 7 8 have favoured restrictive transfusion strategies and elucidated potential harm with liberal transfusion strategies. Data from several newly published randomised controlled trials9 10 11 12 13 warrant an up to date review of the available evidence comparing the effects of different transfusion thresholds to inform on the benefits and harms of transfusion strategies guiding red blood cell transfusion. A Cochrane review identified 19 randomised controlled trials including 6264 patients.14 Most of the data on mortality were from the Transfusion Requirements in Critical Care (TRICC) trial4 (52%) and Transfusion Trigger Trial for Functional Outcomes in Cardiovascular Patients Undergoing Surgical Hip Fracture Repair (FOCUS) trial (23%),15 underlining the somewhat limited evidence base for guiding the use of red blood cells.16
We carried out a systematic review including data from the latest published randomised controlled trials and used conventional meta-analysis to compare the effects of different transfusion strategies on important outcomes in various patient groups. We were particularly interested to examine whether the evidence supported a restrictive strategy without harm to patients.
Methods
Our systematic review was conducted according to the protocol previously published in the PROSPERO register (www.crd.york.ac.uk/PROSPERO). The methodology and reporting were based on recommendations from the Cochrane Collaboration17 and the preferred reporting items for systematic reviews and meta-analyses statement,18 and evaluated according to the GRADE (grading of recommendations assessment, development, and evaluation) guidelines.19
Eligibility criteria
We considered prospective randomised controlled trials to be eligible for inclusion if red blood cell transfusions were administered on the basis of a clear transfusion “trigger” or “threshold,” defined as a specific haemoglobin or haematocrit level. Comparator group patients were required to be either transfused at higher haemoglobin or haematocrit levels than the intervention group or transfused in accordance with current transfusion practices. We considered for inclusion trials that included surgical or medical patients and adults or children, but excluded trials conducted on neonates and children with low birth weight.
All randomised controlled trials were eligible irrespective of language, blinding, publication status or date, or sample size. We excluded quasirandomised trials for assessment of benefit but considered them for inclusion for assessment of harm.
Search strategy
We identified relevant randomised controlled trials through an up to date systematic search strategy used in a published Cochrane review14; in the Cochrane central register of controlled trials, SilverPlatter Medline (1950 to October 2014), SilverPlatter Embase (1980 to October 2014), and Science Citation Index Expanded (1900 to October 2014). To identify any planned, unreported, or ongoing trials we contacted the main authors of included trials and experts in this discipline. We reviewed the references of included trials to identify additional trials. Moreover, we identified ongoing clinical trials and unpublished trials through Current Controlled Trials, ClinicalTrials.gov, and www.centerwatch.com (see supplementary appendix 1 for detailed information on the search strategy).
Trial selection
Authors (LB, MWP, and NH) independently reviewed all titles and abstracts identified through the systematic search. They excluded trials that did not fulfil the eligibility criteria and evaluated the remaining trials in full text. Disagreements were resolved with JW.
Data extraction
The researchers were not masked to the author, institution, and publication source of trials at any time. Using preprepared extraction forms the researchers (LBH, NH, or MWP) independently extracted the characteristics of the trials (single or multicentre, country), baseline characteristics of the patients (age, sex, disease severity), inclusion and exclusion criteria, the description of intervention (thresholds, duration), and outcomes. When information was unclear or missing we contacted the corresponding authors of the relevant trials.
Predefined primary outcomes were mortality and overall morbidity, defined by authors as one or more complications, overall complications, or any adverse event (if not reported, we included the most common complication). Secondary outcomes were adverse events (transfusion reactions, cardiac events—for example, myocardial infarction, cardiac arrest, acute arrhythmia, angina), renal failure, thromboembolic events, infections, haemorrhagic events, stroke, or transitory cerebral ischaemia. We also registered the proportion of patients transfused with allogeneic or autologous red blood cells, and the number of allogeneic and autologous blood units transfused. Haemoglobin or haematocrit levels during intervention and length of hospital stay were regarded as process variables and thus reported as trial characteristics.
Risk of bias assessment
According to recommendations from the Cochrane Collaboration17 we reviewed the major domains of bias (random sequence generation, allocation concealment, blinding of participants and staff, blinding of outcome assessors, incomplete outcome data, selective outcome reporting, baseline imbalance, sponsor bias (bias related to funding source), and academic (whether authors had published other trials in the same field of research) in all trials. We categorised trials with low risk of bias as those with a lower risk of bias in all domains except blinding because blinding of trigger guided transfusion is generally not feasible. All other trials were categorised as unclear or at high risk of bias.
Grading quality of evidence
We assessed the quality of evidence for mortality, overall morbidity, and fatal and non-fatal myocardial infarction according to GRADE methodology19 for risk of bias, inconsistency, indirectness, imprecision, and publication bias; classified as very low, low, moderate, or high.
Statistical analysis
All statistical analyses were performed using Review Manager (RevMan) version 5.3.3 (Nordic Cochrane Centre, Cochrane Collaboration) and trial sequential analysis program version 0.9 beta (www.ctu.dk/tsa).20 For all included trials we report relative risks (95% confidence intervals) for dichotomous outcomes and mean differences (95% confidence intervals) for continuous outcomes. We pooled these measures in meta-analyses.
If data from two or more trials were included in analysis of an outcome, we used random effects20 and fixed effect models21 for meta-analyses. We report the results from both models if there was discrepancy between the two; otherwise we report results from the random effects model. Heterogeneity among trials was quantified with inconsistency factor (I2) or (D2) statistics22 and by χ2 test, with significance set at a P value of 0.10. We did sensitivity analyses by applying continuity adjustment in trials with zero events.17
For risk of bias we performed predefined subgroup analyses (lower versus high or unclear risk) and we emphasise the results from the trials with lower risk of bias,17 patient populations (adults versus children; surgical versus medical), length of follow-up (≤90 days versus >90 days), and transfusion product (leucocyte reduced versus non-leucocyte reduced red blood cell suspensions). Only subgroup analyses showing a statistically significant test of interaction (P<0.05) were considered to provide evidence of an intervention effect. We preplanned exploration of moderate to high heterogeneity using metaregression, including mean age and fraction of men as covariates if possible. However this was not feasible owing to missing values of the covariates in the included trials, but we performed a post hoc subgroup analysis, stratifying trials according to clinical setting. There were no data to support the predefined subgroup analysis of randomised trials of patients with sepsis compared with patients without sepsis.
Meta-analyses may result in type I errors owing to an increased risk of random error when sparse data are analysed23 and due to repeated significance testing when a cumulative meta-analysis is updated with new trials.20 24 To assess the risk of type I errors we applied trial sequential analysis to cumulative meta-analysis. Trial sequential analysis combines an estimation of information size (cumulated sample size of included trials) with an adjusted threshold for statistical significance20 25 in the cumulative meta-analyses.26 The latter, termed trial sequential monitoring boundaries, adjusts the confidence intervals and reduces type I errors. When the cumulative z curve crosses the trial sequential monitoring boundary, a sufficient level of evidence for the anticipated intervention effect may have been reached and no further trials are needed. If the z curve does not cross any of the boundaries and the required information size has not been reached, evidence to reach a conclusion is insufficient. We calculated information size as a diversity adjusted required information size,27 suggested by the diversity of the intervention effect estimates among the included trials.
The required information size was calculated based on a relative risk reduction of 15% in mortality and overall morbidity and a relative risk reduction of 50% in myocardial infarction. We appropriately adjusted all trial sequential analyses for heterogeneity (diversity adjustment) according to an overall type I error of 5% and a power of 80%, considering early and repetitive testing.
Results
Trial selection
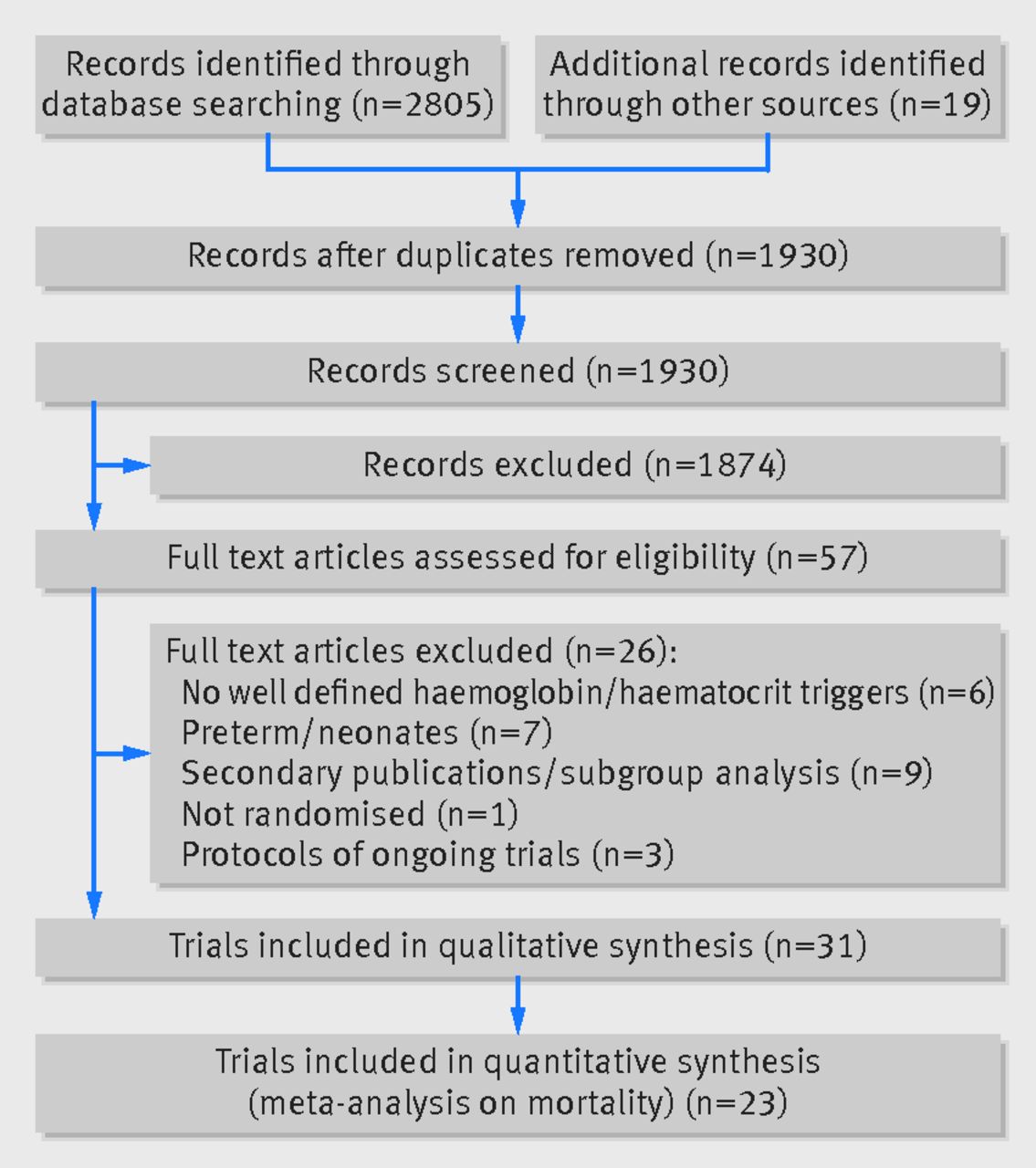
In the updated systematic search strategy we identified an additional 1930 records, of which 38 were assessed in full text for eligibility to supplement the former 19 published randomised controlled trials. In total we found 33 eligible records published, all in English, between October 1986 and October 2014, describing 31 trials of 9813 patients.4 5 6 7 8 9 10 11 12 13 15 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 72 73 Three identified records provided data from the same trial.45 46 47 We excluded a total of 26 records,46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 the primary reasons being a lack of well defined haemoglobin or haematocrit levels guiding the intervention (six records),48 49 50 51 52 53 the inclusion of preterm or very low birth weight neonates (seven records),54 55 56 57 58 59 60 71 and secondary publications or subgroup analyses (nine records).46 47 60 61 62 63 64 65 66 Three records related to ongoing trials.67 68 69 Figure 1⇓ summarises the results of the search strategy.

Characteristics of trials
We included both single (17 trials)6 7 11 12 28 29 30 31 33 34 35 38 39 41 42 43 72 and multicentre (14 trials)4 5 8 9 10 13 15 32 36 37 40 44 45 73 randomised controlled trials. Population sizes ranged from 2534 to 2016,15 and eight trials included more than 500 patients.4 5 6 7 9 13 15 45 The clinical settings of most of the randomised controlled trials were perioperative and acute blood loss (20 trials),6 7 11 12 13 15 30 31 32 33 34 35 36 38 39 41 42 45 72 critical care (eight trials),4 5 8 9 10 37 40 73 and trauma (two trials),29 43 and one trial included patients with leukaemia undergoing stem cell transplantation.44 Table 1⇓ summarises the characteristics of the included trials.
Characteristics of included trials
Intervention
In 24 trials,4 5 [8-7] 9 10 12 13 28 30 31 32 33 34 35 36 37 40 41 43 44 45 73 patients received allogeneic red blood cells, and among these two trials also allowed the use of autologous transfusion.38 39 For the remaining five trials there was no information on the type of red blood cells used.11 12 40 42 72 Leucocyte reduced red blood cells were transfused in 12 trials,5 6 9 10 28 33 35 36 40 45 46 73 and partially leucocyte reduced red blood cells were administered in two trials.8 15 Non-leucocyte reduced red blood cells were used in five trials,4 7 37 38 39 and information was not provided for the remaining 12 trials.11 12 13 29 30 31 32 34 42 43 72
The intervention trigger value varied between trials. The triggers for restrictive transfusion ranged from haemoglobin 7.0 to 9.7 g/dL, haematocrit 24% to 30%, or symptoms of anaemia as defined by the authors. The triggers for liberal transfusion ranged from haemoglobin 9 to 13 g/dL and haematocrit 30% to 40%.
Risk of bias assessment
Table 2⇓ provides detailed information on blinding. Overall, 12 randomised controlled trials were categorised as at lower risk of bias,4 5 6 9 10 13 14 15 28 32 35 73 14 as unclear,8 11 12 29 33 34 37 38 39 40 41 42 43 72 and five as at high risk of bias.7 30 31 36 45 Figures 2⇓ and 3⇓ summarise the risks of bias.
Summary of reported blinding procedure in included trials to supplement ROB table (figure 2.) on blinding procedure, not assessed in overall evaluation of trial bias domains owing to feasibility issues

Fig 2 Risk of bias summary for all included records

{kind=link}
{kind=link}
{kind=link}
Clinical outcomes
Mortality
Data on mortality were provided in 23 trials (8321 patients),4 5 6 7 8 9 10 11 12 15 28 29 30 32 33 36 37 40 41 42 43 73 but few trials followed the patients for 90 days or more.8 9 10 12 37 40
A total of nine trials with 5707 randomised patients were included in the analysis of mortality in trials with lower risk of bias (fig 4⇓),4 5 6 9 10 15 28 32 73 showing a relative risk of 0.86 (95% confidence interval 0.74 to 1.01; P=0.07; I2=27%) for restrictive versus liberal transfusion; the GRADE quality was judged to be low (table 3⇓). The trial sequential analysis adjusted 95% confidence interval was 0.67 to 1.12 (fig 5⇓).

Fig 4 Forest plot of mortality in lower risk of bias trials. Size of squares for risk ratio reflects weight of trial in pooled analysis. Horizontal bars represent 95% confidence intervals
{kind=link}
Summary of findings including GRADE quality assessment of evidence trials with lower risk of bias

Fig 5 Trial sequential analysis of nine trials with lower risk of bias reporting all cause mortality, control event proportion of 17.4%, diversity of 56%, α of 5%, power of 80%, and relative risk reduction of 15%. The required information size of 14 217 has not been reached and none of the boundaries for benefit, harm, or futility has been crossed, leaving the meta-analysis inconclusive of a 15% relative risk reduction. The trial sequential analysis adjusted 95% confidence interval for a relative risk of 0.86 is 0.67 to 1.12
{kind=link}
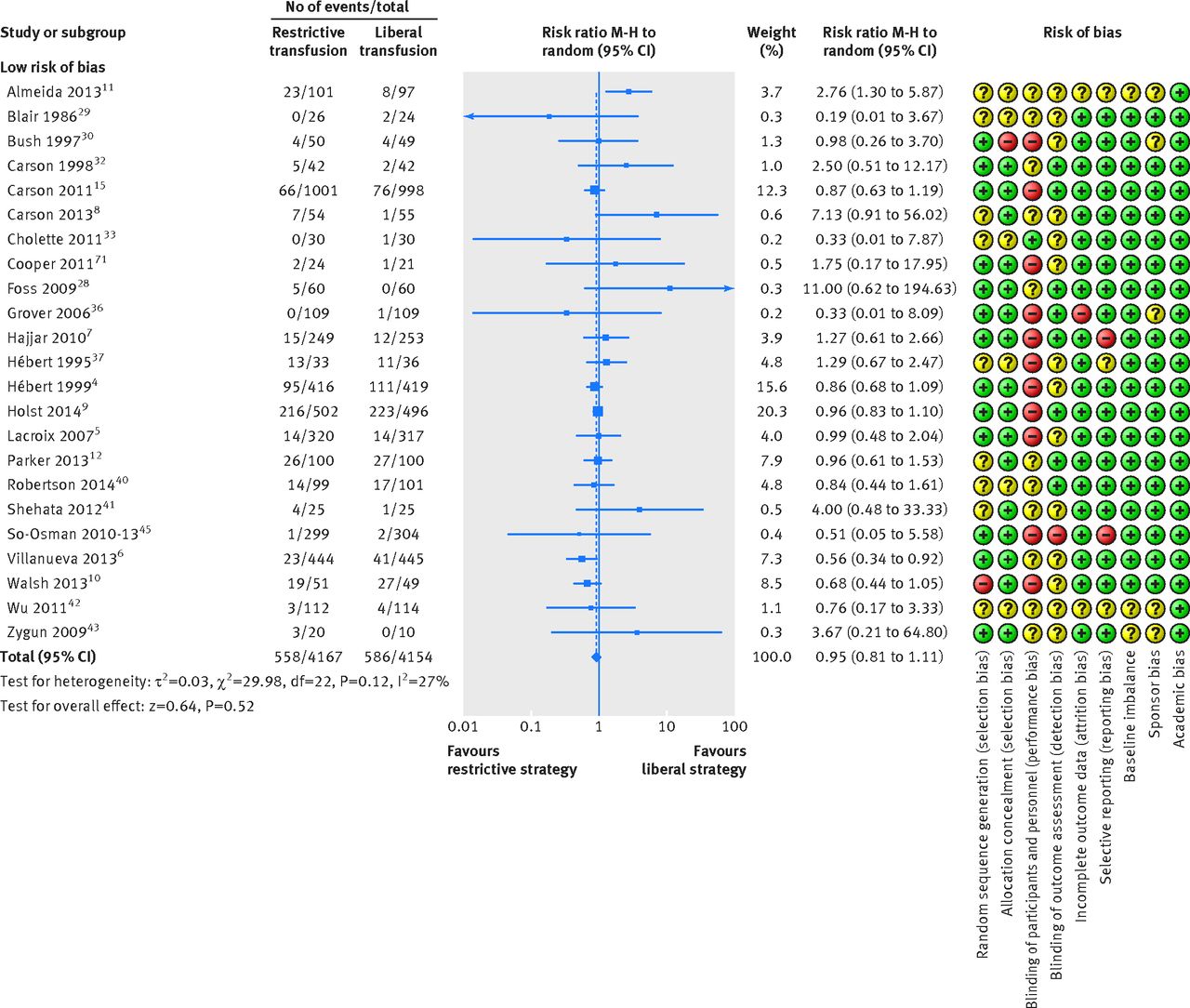
Restrictive versus liberal transfusion strategies did not affect the relative risk of death (0.95, 95% confidence interval 0.81 to 1.11; P=0.52; I2=27%), including all trials despite risk of bias (fig 6⇓); the GRADE quality was judged to be low (table 4⇓). The trial sequential analysis adjusted 95% confidence interval was 0.74 to 1.21 (fig 7⇓). Figure 8⇓ shows the results of meta-analysis on mortality in trials stratified by clinical setting.

Fig 6 Forest plot of mortality despite risk of bias. Size of squares for risk ratio reflects weight of trial in pooled analysis. Horizontal bars represent 95% confidence intervals
{kind=link}
Summary of findings including GRADE quality assessment of evidence, all trials

Fig 7 Trial sequential analysis of 23 trials (despite risk of bias) reporting mortality, with control event proportion of 13.7%, diversity of 62%, α of 5%, power of 80%, and relative risk reduction of 15%. The required information size of 20 799 is far from reached and none of the boundaries for benefit, harm, or futility has been crossed, leaving the meta-analysis inconclusive of a 15% relative risk reduction. The trial sequential analysis adjusted 95% confidence interval for a relative risk of 0.95 is 0.74 to 1.21
{kind=link}

Fig 8 Forest plot of mortality in trials stratified by clinical setting. Size of squares for risk ratio reflects weight of trial in pooled analysis. Horizontal bars represent 95% confidence intervals
{kind=link}
Overall morbidity
A total of six trials with lower risk of bias including 4517 patients were included in the meta-analysis of overall morbidity (fig 9⇓).4 5 6 8 15 73 Overall morbidity did not differ between the restrictive and liberal transfusion strategies (relative risk 0.98, 95% confidence interval 0.85 to 1.12; P=0.75; I2=60%) and the trial sequential analysis adjusted 95% confidence interval was 0.81 to 1.19. Future trials are unlikely to show a 15% relative risk reduction in favour of restrictive or liberal strategies as the boundary for futility was crossed (fig 10⇓). The GRADE quality of evidence was judged to be very low (table 3).
A total of 12 trials with 5975 randomised patients were included in the meta-analysis of overall morbidity regardless of risk of bias (relative risk 1.06, 95% confidence interval 0.93 to 1.21; P=0.36; I2=58%).4 5 6 7 8 15 35 37 39 41 46 73
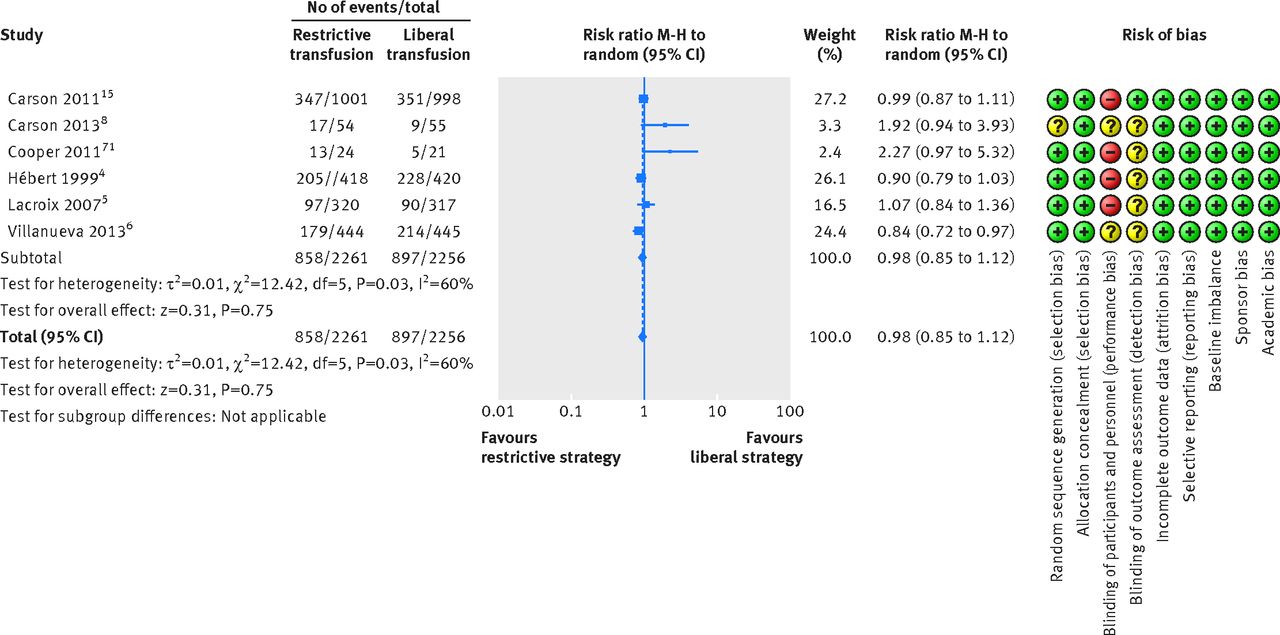
Fig 9 Forest plot of overall morbidity in low risk of bias trials. Size of squares for risk ratio reflects weight of trial in pooled analysis. Horizontal bars represent 95% confidence intervals
{kind=link}

Fig 10 Trial sequential analysis of six trials reporting overall morbidity, a control event proportion of 40%, diversity of 75%, α of 5%, power of 80%, and relative risk reduction of 15%. The required information size of 7188 has not been reached, but the boundaries for futility are crossed, leaving out the possibility of a 15% relative risk reduction. The trial sequential analysis adjusted 95% confidence interval for a relative risk of 0.98 is 0.81 to 1.19
{kind=link}
Fatal or non-fatal myocardial infarction
Seven trials assessing fatal or non-fatal myocardial infarction including 4730 patients were defined as trials with lower risk of bias.4 5 9 10 15 28 73 Restrictive transfusion strategies were not associated with a relative risk reduction or relative risk increase in fatal or non-fatal myocardial infarction (relative risk 1.28, 95% confidence interval 0.66 to 2.49; P=0.46; I2=34%) (fig 11⇓) and the trial sequential analysis adjusted 95% confidence interval was 0.40 to 4.31 (fig 12⇓). The GRADE quality of evidence was judged to be very low (table 3). A total of 16 trials with 6501 randomised patients were included in the meta-analysis of fatal or non-fatal myocardial infarction regardless of risk of bias (1.05, 0.82 to 1.36; P=0.70; I2=6%); the GRADE quality of evidence was judged to be low (table 4).4 5 7 8 9 10 15 28 30 31 36 38 39 40 41 73

Fig 11 Forest plot of myocardial infarctions in low risk of bias trials. Size of squares for risk ratio reflects weight of trial in pooled analysis. Horizontal bars represent 95% confidence intervals
{kind=link}

Fig 12 Trial sequential analysis of seven trials reporting myocardial infarction, with a control event proportion of 1.8%, diversity of 62.3%, α of 5%, power of 80%, and relative risk reduction of 50%. The diversity adjusted required information size of 13 686 is far from reached and none of the boundaries for benefit, harm, or futility has been crossed, leaving the meta-analysis inconclusive of even a 50% relative risk reduction. The trial sequential analysis adjusted 95% confidence interval for a relative risk of 1.28 is 0.40 to 4.13
{kind=link}
Other adverse events
A total of eight trials defined as lower risk of bias with 5107 patients were included in the meta-analysis on infectious complications. Our analysis showed an association in favour of using a restrictive transfusion strategy (relative risk 0.73, 95% confidence interval 0.55 to 0.98, P=0.03, I2=53%) (see supplementary appendix 2).4 5 6 13 15 28 32 35 The inclusion of all 15 trials (7217 patients) regardless of risk of bias did not alter the result (0.79, 0.64 to 0.97, P=0.03, I2=40%).4 5 6 7 8 13 15 28 31 32 35 36 40 41 46 Our analysis showed no association of restrictive versus liberal transfusion with other adverse events (cardiac complications, renal failure, thromboembolic stroke or transitory ischaemic insult, or haemorrhage) (see supplementary appendices 3 and 4).
Number of patients and units transfused
A total of 24 trials with 8923 patients were included in the meta-analysis of the proportion of patients receiving red blood cells (relative risk 0.54, 95% confidence interval 0.47 to 0.63; P<0.001; I2=95%), and a total of 12 trials with 4022 patients were included in the meta-analysis of the number of units transfused (mean difference −1.43, 95% confidence interval −2.01 to −0.86; P<0.001; I2=96%) both showing lower numbers associated with restrictive versus liberal transfusion strategies (see supplementary appendices 5 and 6).
Discussion
We did not find any association with mortality, overall morbidity, or myocardial infarction when comparing restrictive transfusion strategies with liberal transfusion strategies; however, the overall quality of evidence was low. We performed trial sequential analysis to account for sparse data and repetitive testing on accumulating data and found that the 95% confidence intervals of the point estimates widened and the results supported those obtained in the conventional meta-analyses. In our analysis of all cause mortality, the cumulative z curve did not cross any boundaries, with only 40% of the required information size being reached (5707 of 14 217 patients), indicating that further trials are needed to establish firm evidence. In our analysis of all trials, the trial sequential analysis indicated that it is unlikely that future trials will show overall harm with restrictive transfusion strategies. Regarding overall morbidity, we found no association with benefit or harm between groups, but the trial sequential analysis indicated it would be futile to obtain more trial data on this outcome. We found that the trial sequential analysis of pooled risk of fatal or non-fatal myocardial infarction was inconclusive, because only 26% of the required information size was obtained. Regarding infectious complications, our analysis indicated a possible association between a restrictive transfusion strategy and reduced rates of infection across the different clinical settings.
Relation to other reviews
Well conducted systematic reviews with meta-analysis on red blood cell transfusion have been published. A Cochrane review indicated that restrictive transfusion strategies were not associated with the rate of adverse events (that is, mortality, cardiac events, stroke, pneumonia, and thromboembolism) compared with liberal transfusion strategies. Restrictive transfusion strategies were associated with a reduction in hospital mortality (relative risk 0.77, 95% confidence interval 0.62 to 0.95) but not in 30 day mortality (0.85, 0.70 to 1.03).14
A review was published in 2014 including 6936 patients from 19 trials assessing the impact of red blood cell transfusion.74 Pooled data from three trials (2364 patients) using restrictive haemoglobin transfusion triggers of 7 g/dL showed reductions in in-hospital mortality (relative risk 0.74, 95% confidence interval 0.60 to 0.92), total mortality (0.80, 0.65 to 0.98), rebleeding (0.64, 0.45 to 0.90), acute coronary syndrome (0.44, 0.22 to 0.89), pulmonary oedema (0.48, 0.33 to 0.72), and bacterial infections (0.86, 0.73 to 1.00) compared with liberal transfusion. In contrast, pooled data including trials with less restrictive transfusion thresholds did not show associations with any of the predefined outcomes.
A recent systematic review with meta-analysis included 18 randomised controlled trials reporting data on in-hospital infections.75 Restrictive transfusion strategies were associated with a reduced risk of infections among patients admitted to hospital compared with liberal transfusion strategies (0.88, 0.78 to 0.99). Our analysis showed comparable results, with a possibility of lowering the rate of infections using restrictive transfusion strategies. We also included data on non-healthcare associated infections, but our results may be influenced by multiple testing and sparse data.
We included data from the recent Transfusion Requirements In Septic Shock (TRISS) trial, which randomised 1005 patients with septic shock in the intensive care unit, in which there was no difference in mortality or morbidity with the use of pre-stored leucocyte reduced red blood cells at a transfusion trigger of 7 versus 9 g/dL.9 In accordance with the Cochrane review we did not find evidence of harm with the use of restrictive transfusion strategies compared with liberal transfusion strategies. However, our trial sequential analyses were inconclusive for the assessment of mortality and myocardial infarction owing to insufficient information sizes.
Strengths and limitations of this review
Applying Cochrane methodology is a major strength of this systematic review, comprising a prepublished protocol, a non-restricted up to date literature search, independent data extraction by at least two authors, and risk of bias assessment leading to GRADE evaluations of important outcomes. Trial sequential analysis was performed to explore the risk of random error as a result of sparse data and repetitive testing in order to increase the robustness of the meta-analyses and distinguish the current information size from the required information size.
Our systematic review also has limitations. The randomised controlled trials included in the primary analysis dealt with different indications for transfusion by randomising a variety of patient groups (for example, children and adults) in different clinical settings (for example, elective surgery and critical illness). Thus, the risk of introducing potentially important heterogeneity is imminent. To get a clinical applicable result, we excluded trials of neonates and infants with very low birth weight. None of the included trials was blinded, as this is not feasible. This may introduce both performance and detection bias. However, the primary outcome of all cause mortality is less prone to be influenced by lack of blinding.76 Transfusion triggers varied between trials, with some using a liberal transfusion threshold equal to the restrictive one in other trials, introducing clinical heterogeneity. Both clinical heterogeneity and inadequate follow-up increase the risk of type II error. Bias in the included trials, losses to follow-up, and incomplete reporting of outcome measures are additional limitations in this review. The definitions of overall morbidity and adverse events were heterogeneous and should be taken into account when interpreting these data. Finally, for some of the predefined outcomes, limited trial data could be included in the meta-analyses resulting in wide confidence intervals and less certain point estimates.
Unanswered questions
Whether the overall use of red blood cells should be guided by a restrictive or a liberal transfusion strategy is still debatable. Patients with coronary artery disease, and in particular patients with ongoing cardiac ischaemia, might require a higher haemoglobin level to sustain oxygen delivery to the myocardial cells and to reduce the sympathetically mediated compensatory mechanisms of anaemia and reduce myocardial oxygen demand. However, red blood cell transfusion could worsen patient outcome as a result of an increased risk of circulatory overload and increased thrombogenicity with higher haematocrit levels. Results from the FOCUS trial showed no association with the primary composite outcome of morbidity and mortality 60 days postoperatively or the incidence of coronary syndrome when comparing two transfusion strategies (8 g/dL (or symptoms of anaemia) versus 10 g/dL).15 Two small randomised controlled trials evaluating a restrictive transfusion trigger of haemoglobin <8 g/dL in patients with symptomatic coronary artery disease have been published8 73; pooled data from these two trials randomising a total of 155 patients did not show an association between a restrictive transfusion strategy and cardiac events or mortality compared with a liberal transfusion strategy. A meta-analysis including observational studies on transfusion in patients with myocardial infarction indicates that the rates of subsequent myocardial infarction and all cause mortality may be associated with blood transfusions compared with standard supportive interventions, after adjustment for possible confounding variables.77 Large randomised controlled trials of restrictive compared with liberal transfusion are warranted in patients with myocardial infarction.
Patients with traumatic brain injury may require more liberal transfusion strategies to prevent secondary cerebral ischaemic insults because the injured brain may not compensate for decreased oxygen delivery associated with anaemia.78 One randomised controlled trial using a factorial design compared the effects of erythropoietin and two different haemoglobin thresholds for red blood cell transfusion (7 versus 10 g/dL) in 200 patients with a closed head injury and showed no difference in neurological outcome at six months.40 Also in patients with acute brain injury data from high quality randomised controlled trials are needed to guide transfusion practice.
Conclusions
In conventional meta-analyses restrictive transfusion strategies compared with liberal transfusion strategies were associated with a reduction in the number of red blood cells used and the number of patients being transfused but were not associated with benefit or harm regarding mortality, overall morbidity, and fatal or non-fatal myocardial infarction in various clinical settings. However, the required information sizes were not reached except for overall morbidity, where a 15% relative risk reduction or increase with restrictive transfusion strategies may be refuted. Analyses of all trials, regardless of risk of bias, showed similar findings. We found possible associations between restrictive transfusion strategies and a reduced number of infectious complications.
Restrictive transfusion strategies are safe in most clinical settings. Liberal transfusion strategies have not been shown to confer any benefit to patients but have the potential for harm.
What is already known on this topic
Red blood cells are commonly used in the treatment of haemorrhage and anaemia, but recent trials have shown potential harm with this intervention
Recent meta-analysis indicates no harm with the use of a restrictive transfusion strategy
What this study adds
This review includes new data from five recently published randomised trials of restrictive versus liberal transfusion strategies and includes data from more than 9000 patients
Pooled analyses did not show harm with restrictive transfusion strategies (no increased risk of mortality, overall morbidity, or acute myocardial infarction) but the number of units and number of patients transfused were reduced compared with liberal strategies
Liberal strategies have possible associations with harm (risk of infectious complications)
Further large trials with lower risk of bias are needed to establish firm evidence to guide transfusion in subgroups of patients
Notes
Cite this as: BMJ 2015;350:h1354
Footnotes
We thank Sarah Klingenberg, search coordinator for the Cochrane Hepato-Biliary Group, for performing the literature search.
Contributors: LBH developed the protocol, was responsible for the searches, selected trials, extracted data, assessed the risk of bias of trials, did the data analysis, and developed the final review. MWP developed the protocol, selected trials, extracted data, assessed the risk of bias of trials, and developed the final review. NH developed the protocol, selected trials, extracted data, assessed the risk of bias of trials, and developed the final review. AP developed the protocol, analysed data, and developed the final review. JW developed the initial idea for the review, developed the protocol, selected trials, advised on statistical methods, analysed data and resolved any disagreements during data extraction and bias assessment, and developed the final review. All authors read and approved the final manuscript. LBH and JW are the guarantors and affirm that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained.
Funding: This review was funded by the Danish Strategic Research Council (09-066938), supported by Copenhagen University Hospital, Rigshospitalet. The funders had no influence on the protocol, data analyses, or reporting.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: AP was principal investigator for Transfusion Requirements In Septic Shock (TRISS) trial and LBH, NH, and JW were members of the steering committee. AP is head of research in his intensive care unit, which receives research grants from CSL Behring, Fresenius Kabi, and Cosmed.
Ethical approval: Not required.
Data sharing: No additional data available.
Transparency: The lead authors (LBH and JW) affirm that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.