Article Text

Abstract
Women with past gestational diabetes mellitus (GDM) are at risk of subsequent type 2 diabetes and adverse cardiovascular events. Digital and telemedicine interventions targeting weight loss and reductions in body mass index (BMI) may help reduce risk for women with GDM. The aim was to compare the effectiveness of digital or telemedicine intervention with usual care. Randomized controlled trials (RCTs) were identified in Embase, Medline, CINAHL, PsycINFO and the Cochrane Library. Included trials recruited women with prior GDM but without pre-existing diabetes, and tested a digital or telemedicine intervention with or without an in-person component. Data extraction was carried out independently by two authors. The search yielded 898 citations. Eighteen articles reporting 15 trials were included, of which 8 tested digital interventions. Reported outcomes included weight, BMI, fasting plasma glucose and waist circumference. None of the included trials reported type 2 diabetes incidence or cardiovascular risk. Data were pooled using a random-effects model. The point estimate favored the intervention but was non-significant for both BMI (−0.90 kg/m2, 95% CI −1.89 to 0.09; p=0.08) and weight (−1.83 kg, 95% CI −4.08 to 0.42, p=0.11). Trials evaluating digital and telemedicine interventions identified clinically relevant, but non-significant improvements in BMI and weight compared with control. No trials assessed type 2 diabetes occurrence as an outcome. More well-designed RCTs with adequate power and long-term follow-up are needed to identify the impact of these interventions on type 2 diabetes occurrence.
- diabetes
- gestational
- telemedicine
- meta-analysis
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Gestational diabetes (GDM) is defined as hyperglycemia first identified in pregnancy, usually during the second or third trimester. Screening for GDM is offered to women with one or more risk factors (eg, body mass index (BMI) >30 kg/m2) and diagnoses typically made with abnormal values on an oral glucose tolerance test. GDM affects an estimated 5%–20% of pregnancies.1 Hyperglycemia generally resolves within weeks of delivery but it can predict subsequent diabetes mellitus.
Women living with GDM have a sevenfold increased risk for subsequent type 2 diabetes2 and they are twice as likely to develop hypertension and have increased risk for ischemic heart disease.3 During the 5 years following delivery, type 2 diabetes incidence can rise sharply before plateauing around a decade later.4 The temporal lag between GDM and type 2 diabetes may offer a therapeutic window of intervention and the National Institute for Health and Care Excellence (NICE) recommends dietician referral and lifestyle modification.5
In general, interventions promoting weight loss and exercise in people at risk of type 2 diabetes significantly reduce incidence of type 2 diabetes, and can reduce markers of cardiovascular health.6–8 However, women with GDM can find it difficult to make lifestyle changes.9 For instance, busy routines, low self-efficacy and poor social support have been identified as barriers to change.10 11 Women with and without GDM have similar weight retention and reduced physical activity in the postpartum period,12 but following GDM there are additional health risks.
The role of digital interventions in delivering healthcare have recently been examined by WHO.13 These interventions can be delivered in various ways including automated text messages, web-platforms and online consultations. They are used in several contexts and can provide multiple services including educational resources, goal-setting and remote self-monitoring. Intervening using digital interventions has been conducted in the areas of smoking cessation,14 hypertension and weight loss.15 In comparison, telemedicine refers to delivery of remote health, involving telephone consultations and videoconferences, particularly useful where distance can prevent face-to-face contact.
Both digital and telemedicine interventions can facilitate lifestyle change by supplementing or replacing face-to-face contact, potentially overcoming barriers. To date, prototype applications have been viewed positively by women with GDM.16 However, inconsistent findings mean it is unclear if they are genuinely superior to standard care.17 18 Previous systematic reviews focusing on GDM have either not addressed digital interventions or they have focused on management during pregnancy rather than after.2 19 20 Therefore, we addressed this gap in evidence by focusing on the impact of digital and telemedicine interventions (with or without in-person contact) on weight and BMI when used by women who have previously experienced GDM.
Methods
Protocol and registration
The protocol for this systematic review was prospectively registered (PROSPERO registration number: CRD42019145051). This review is reported according to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement.21
Eligibility criteria
Participants: trials included women aged ≥18 years with a prior GDM diagnosis, but those recruiting women with pre-existing diabetes were ineligible. Trials recruiting women during the GDM affected pregnancy were eligible for inclusion. Interventions: digital interventions included websites and text messages. Telemedicine interventions not including any digital component, such as interventions only involving telephone calls, were treated as distinct from digital interventions. Trials without any digital or telemedicine component were excluded. For the purposes of this review, trials reporting interventions including both in-person and digital or telemedicine components were eligible for inclusion. Comparisons: trials comparing digital or telemedicine interventions with a usual care comparator were included. Outcomes: trials with BMI or weight reported in a 3–6 months time frame post partum were included in the meta-analysis. Trials that reported these outcomes outside this time frame or other secondary outcomes of interest for lifestyle interventions were retained for the systematic review qualitative summary. Outcomes must have been measured at least 6 weeks post partum. Study design: only randomized controlled trials (RCTs) were eligible for inclusion.
Information sources
The search strategy was applied to Embase, MEDLINE, CINAHL, PsycINFO and The Cochrane Library from the inception of each database to February 17, 2020. The full, electronic search strategy used to identify trials from the Embase database is listed in online supplemental table S1. No language or date restriction was applied. The coverage and date of search is presented in online supplemental table S2.
Supplemental material
Study selection
Titles and abstracts of all citations identified by the search were screened by JH and MEW independently using Rayyan, a web and mobile application for systematic reviews.22 Disagreements were discussed and escalated for resolution to a third reviewer (AJF). Full-text articles were screened for eligibility with any discrepancies resolved through discussion. References cited in the manuscripts of the included trials were also checked for additional RCTs not identified in the database search.
Data collection process
JH and MEW extracted data independently using a custom Cochrane Collaboration data extraction form. The form was initially piloted for two trials to check it collected all of the appropriate fields. Any disagreements were discussed and resolved with AF. In the event missing data were recorded, we did not contact study authors.
Data items
Data were extracted for title, authors, publication date, setting (country and context), study design, study duration, GDM diagnostic criteria, participant characteristics (including age and ethnicity) and sample size, as well as details of the intervention and comparator conditions. The primary outcome of interest was weight and BMI at least 6 weeks post partum. Secondary outcomes included type 2 diabetes incidence, cardiovascular risk, waist circumference, fasting plasma glucose (FPG), oral glucose tolerance test (OGTT), physical activity and dietary behaviors.
Risk of bias in individual studies
Risk of bias was assessed by the first and second author using the Cochrane Collaboration’s risk of bias tool. The included trials were judged as being either at low risk, high risk or with an unclear level of risk. Disagreements were resolved with AF. Cluster RCTs were reported separately.
Synthesis of results
If more than two trials reported both baseline and follow-up values, findings were pooled using a random-effects model using RevMan V.5.3 software. Missing SD values for mean change were derived using equations recommended by Cochrane (Cochrane Handbook: Chapter 16.1.3.2). Where possible, SD values were derived from 95% CI. When trials reported data at multiple follow-up timepoints, the earliest timepoint was chosen for pooling to align with the other trials. Summary measures were reported along with 95% CI. Heterogeneity of trials were reported using the I2 statistic; 0%–40% was considered not significantly important, while ≥75% deemed to have significant heterogeneity.
Results
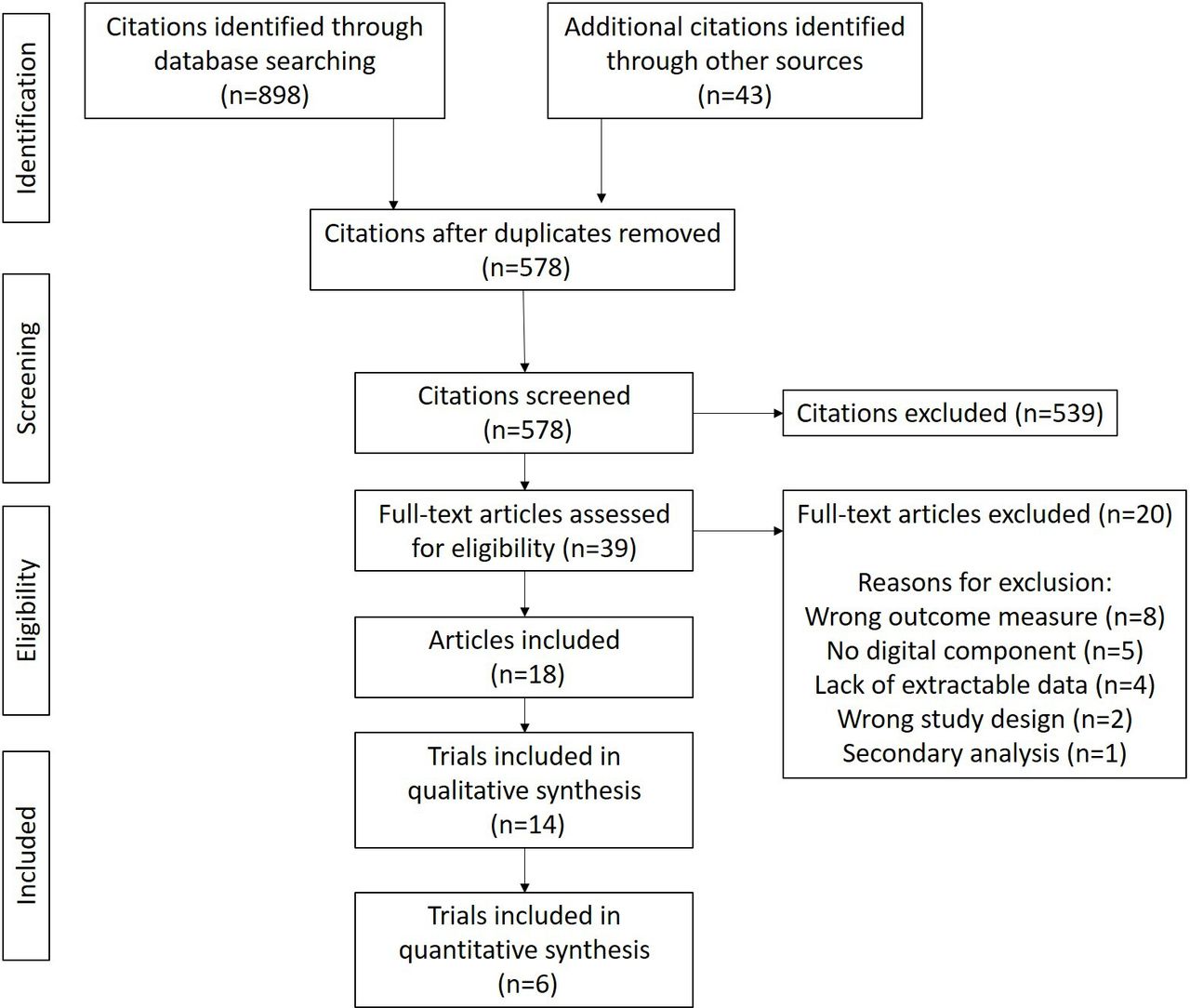
A total of 941 citations were identified from the database searches and from checking the reference lists of included papers (figure 1 and online supplemental table S2). Thirty-nine full-text articles were retrieved. Eighteen citations were eligible for inclusion, reporting results of 15 studies (3 citations were conference proceeding reports of subsequently published work and 2 citations reported results from the same study).
Trial characteristics
General study characteristics are presented in table 1. Sample size ranged from 2823 to 248024 people and five trials were reported as pilot studies.25–29 Trial durations ranged from 12 weeks25 30 to 12 months.23 Of the trials that reported the country in which the research was done, Australia and New Zealand (n=6), the USA (n=4), Canada (n=1) and Europe (n=2) were listed. The majority of trials were in the hospital setting with eight trials recruiting during pregnancy, six recruiting post partum and one recruiting women in late pregnancy or shortly after birth.31 A variety of criteria were also used to determine eligibility for including women with GDM (online supplemental table S3).
Trial characteristics; values are mean (SD) unless otherwise stated
Intervention characteristics
Nine trials reported digital interventions and seven reported telemedicine interventions, using telephone calls. A full description of the various trials is provided in online supplemental table S4. One trial assigned controls to a waiting list to the nutritional program.30 Usual care included a clinic-based educational class,32 an educational DVD33 and printed materials being most frequent (n=8) (table 1).
Risk of bias
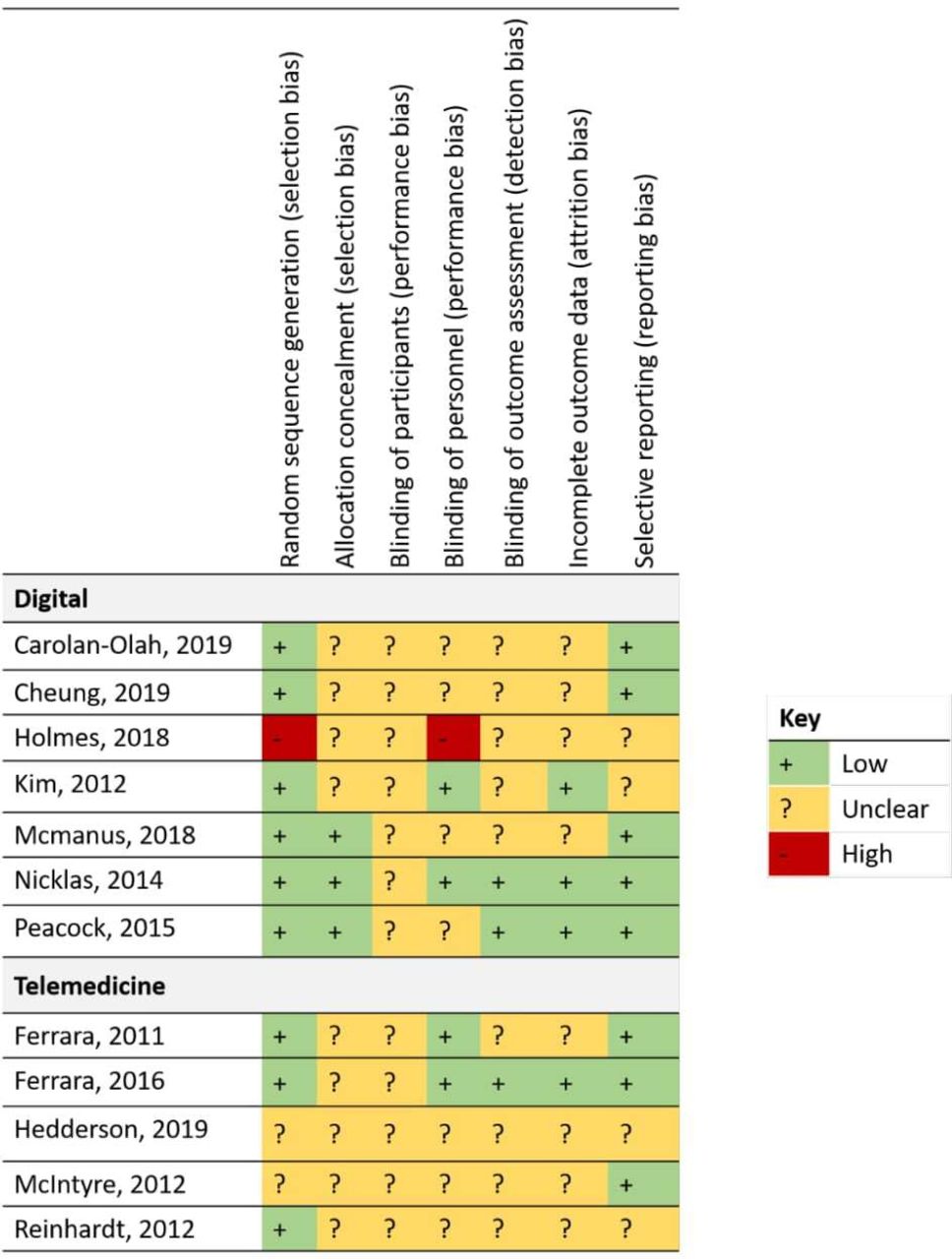
Results of the risk of bias assessment for all included studies are presented in figure 2. One trial was judged to have high risk of bias for random sequence generation because randomization was assigned by week of attendance at postpartum OGTT, rather at the level of the individual.33 Four trials either blinded personnel carrying out outcome assessment or analysts undertaking statistical analyses.

Preferred Reporting Items for Systematic Review and Meta-Analysis flow of the selection process.

Risk of bias assessment.
Primary outcome
Reported outcomes of each trial are listed in online supplemental table S5.
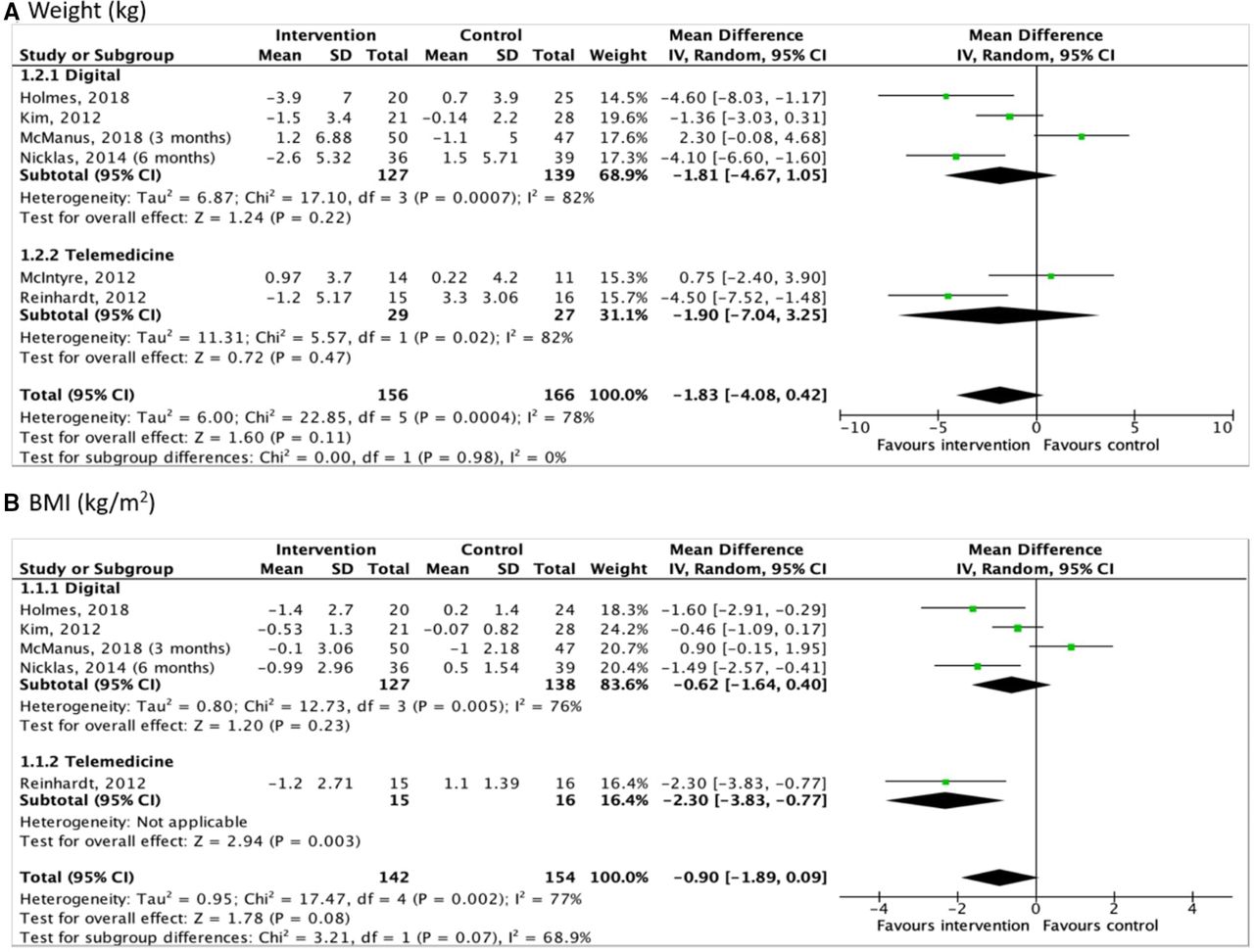
Of the 13 trials reporting weight as an outcome, 5 revealed significant differences.23 26 30 32 33 One trial reported a significant difference favoring the intervention (p=0.002), but was excluded from the meta-analysis by reporting median and IQR.30 A mixture of self-report and clinic-measured weight were reported. Data from six trials were pooled where the data were available and where outcomes were reported at 3–6 months (figure 3A).23 25 26 29 31 33 The point estimate favored intervention but overall was non-significant (−1.83 kg; 95% CI −4.08 to 0.42; p=0.11), nor within either subgroup analyses. The I2 statistic was 78%, indicative of high heterogeneity.
{kind=link}
{kind=link}
{kind=link}
Forest plots for (A) weight and (B) body mass index (BMI).
Seven trials reported a change in BMI. Four trials found significant differences between intervention and control.23 26 29 31 33 A mixture of self-report and clinic-measured BMI was calculated. Available data from five trials were pooled for meta-analysis where outcomes were reported across 3–6 months (figure 3B).23 26 29 31 33 Four of the trials included a digital element, with both subgroup analyses remaining significant. Overall, the point estimate favored the intervention but overall was non-significant (−0.90 kg/m2; 95% CI −1.89 to 0.09; p=0.08) and the I2 statistic was 77%.
Secondary outcomes
Key outcomes are reported in online supplemental table S6. Several trials did not report prespecified outcomes of interest in this review. One trial reported psychological determinants of behavior change,34 and one trial reported weight change in a form that could not be quantitatively extracted.35 One trial36 did not report FPG and instead only reported post partum 2 hours OGTT. Findings revealed no significant difference between 3 months postpartum results between the two groups (p=0.25). One trial32 reported blood pressure, a marker of adverse cardiovascular risk when raised, but found no significant difference between groups at follow-up. No included trials reported occurrence of type 2 diabetes or cardiovascular events. No trials reported economic analysis of the interventions.
Fasting plasma glucose
Only one trial reported a significant effect, but favoring control.30 Inconsistency in reporting was noted with one trial32 reporting baseline and follow-up data for the intervention group only, and another trial omitting baseline values.28 Three other trials reporting FPG revealed non-significant differences.25 29 33
Waist circumference
Two digital trials reported significant improvements in favor of the intervention.30 33 Two trials reported non-significant effects favoring intervention,26 29 whereas two trials reported greater reduction for controls.25 31
Physical activity
Eight trials measured levels of physical activity24–30 35 and only one of these trials used activity monitors to measure device-based physical activity.25 Insufficient reporting prevented data pooling. No significant differences were reported.
Diet
Ten trials reported dietary behaviors.23 24 26–28 30 31 33–35 Four of these trials23 26 27 35 reported significant effects favoring the intervention; notably reductions in calorie intake,23 dietary fat intake,27 daily total intake35 and carbohydrate intake.26 One study identified barriers to healthy eating and reported a significant reduction in barriers in response to the intervention.34 Only one trial28 explicitly reported interview-led measurement (ie, dietician-led, rather than self-report) to assist with outcome measurement at baseline. Inconsistent use of dietary behavior outcomes prevented data pooling.
Cluster RCT
One trial used a cluster design.24 In this trial, significantly more women achieved postpartum weight goals in the intervention group over 12 months (OR 1.28, 95% CI 1.10 to 1.47) compared with the usual care group.24 Mean weight change between groups was significant at 6 months (p=0.01) but not at 12 months (p=0.12). Mean change in vigorous physical activity was significant at 6 months (15.4 min/week, 95% CI 4.9 to 25.8) but moderate or total activity/week was not.
Dropout from studies
The rate of dropout from the included trials is reported in table 2. Withdrawal ranged from 6.7% to 52.5% and averaged 24.8% in the intervention group. Control group dropout, in comparison, ranged from 7.7% to 60% and averaged 23.5% across reporting trials. Studies investigating a digital intervention averaged a higher dropout rate than the telemedicine trials (30.7% vs 14.6%, respectively). Two trials26 32 did not report rates of dropout by group, however did report a rate of 5.2% (n=6/116) and 5.3% (n=2/38), respectively, across the sample. Two trials did not report trial drop-out rates.35 When trials did report reasons for dropout, they ranged from being too busy, work-related reasons, subsequent diagnoses of diabetes, subsequent pregnancy, spontaneous abortion or being lost to follow-up. Eight of the trials reported using the intention-to-treat principle in handling participant dropout.
Rates of dropout across the included studies reported by group allocation (where available)
Discussion
Key findings
We aimed to investigate the effect of digital and telemedicine interventions on weight and BMI following GDM. Our meta-analysis identified a statistically non-significant reduction in BMI and weight and the CIs of the impact of the interventions on weight included a clinically important impact. Reducing weight lowers type 2 diabetes incidence,37 with every 1 kg lost reducing risk of diabetes by 16%.38 Interventions could potentially be cost-effective, but no economic analyses were reported beyond unit costs.
There is international recognition of digital platforms as being potentially helpful in the management and treatment of disease and risk.13 National guidelines are currently being developed by NICE on the use of digital and mobile health interventions to support behavior change.39 The fast pace of development of emerging technologies requires that assessments of impact are updated regularly to remain relevant. These novel digital interventions may modify current clinical practice, potentially reducing the reliance on face-to-face consultation.40
In the review, we grouped interventions into either digital or telemedicine. While both may help supplement or reduce sole reliance on face-to-face consultation, which can be overwhelming for new mothers,41 the mode of their delivery differs. Telephone conversation, while not replicating face-to-face interactions, can be more convenient. In contrast, the delivery of a digital intervention may be different from that of a face-to-face consultation, for example, an interactive website or multiple platforms with data collection can reduce physical contact with health professionals and provide educational information with websites accessible at any time and from any location.23 30–32 Many of the trials identified in this review used multiple methods of delivery (including a combination of in-person and digital or telemedicine) leading to heterogenous interventions and ‘key ingredients’ not being easily identified. In addition, we report that the dropout rates from the interventions comprising a telemedicine component averaging a slightly lower dropout rate (14.6%) compared with the studies exploring an intervention with a digital component (30.7%). Future studies should direct careful consideration toward minimizing dropout and ensure clear reporting on drop out by group allocation with reasons when collected.
No trials reported on the long-term outcomes of GDM, which are challenging to measure, particularly in the context of device trials. A systematic review led by Goveia et al42 identified that lifestyle interventions can significantly reduce diabetes incidence by 25% using data from eight trials, with trials offering the intervention within 6 months post partum most effective. In our review, we focused on proxy indicators of health status including BMI and weight, which can provide evidence for intermediate outcomes known to predict long-term adverse consequences. Goveia et al demonstrated moderate reductions in weight (−1.07 kg), BMI (−0.94 kg/m2) and waist circumference (−0.98 cm) following participation in a lifestyle intervention, but did not distinguish between trials using digital/non-digital delivery.42 Other reviews in the area of GDM have looked at reducing diabetes risk showing low recruitment rates and possible contributions to postpartum weight loss and improved dietary behaviors.43 Reviews specifically focusing on telemedicine-based interventions have shown that monitoring glucose levels can result in significant reductions in HbA1c19 and GDM services can be streamlined using telemedicine without compromising maternal or fetal outcomes.20 Our review adds to the literature that digital/telemedicine interventions have not shown significant improvements in weight or BMI 3–6 months post partum. However, it does not rule out clinically meaningful changes in weight loss from participation in a digital/telemedicine intervention compared with usual care.
The effect size observed for weight loss and change in BMI was not substantially different. Although the CIs for weight loss did not provide evidence of a statistically significant effect, this does not exclude a clinically important benefit. The trials included in the pooled estimates of impact on weight and BMI only differed by the additional inclusion of McIntyre et al in the BMI quantitative analysis. The extent of heterogeneity suggests a need for more consistent selection of outcome measures in trials. One additional trial noted during our systematic review but not included due to ineligibility revealed that outcomes can also focus on breastfeeding duration.44 Several of the studies were deemed to have an unclear level of risk of bias with one study33 deemed to be at high risk. This is a notable finding and suggests that future research studies should implement explicit transparent reporting on risk attribution to selection bias, performance bias, detection bias and attrition bias.
Challenges and limitations
Reporting of both planned intervention fidelity and actual delivery of intervention was limited across all trials. Many trials commented on whether participants used the system, but details such as call duration were often missing. The search strategy was comprehensive and inclusive, which identified some studies that did not include outcomes of interest. This review reported outcomes according to PRISMA, but findings were limited by reporting and design of included trials. While findings on behavior change are encouraging, there are challenges in interpreting self-report behavior. For example, in the instance where physical activity was reported, it was self-reported rather than device-based which raises concerns around social desirability bias. The methods used to collect weight and BMI were largely through clinical measurement; however, a few trials did use self-report methods or a combination of self-report and clinical measurement.26 In one trial the method of collection was unclear.33 The digital and telemedicine field is rapidly advancing, meaning backward-looking review is required to evaluate possible beneficial impact from these interventions. However, lack of standardized reporting and timepoint of assessment presented a barrier to direct comparison between trials, and the search strategy did not identify any relevant trials addressing theories of behavior change. This suggests a need for promoting long-term behavior change with digital and telemedicine interventions with long-term follow-up of clinical outcomes.
Summary
In summary, this systematic review demonstrated the point estimate of the effect of the intervention on weight and BMI has potential to be clinically relevant but was not statistically significant. Previous systematic reviews suggest telemedicine interventions can aid management of GDM during pregnancy, but do not conclude these interventions were superior to standard care.19 20 Findings from the present review provide evidence that these interventions can positively impact important short-term outcomes following pregnancy. Large, adequately powered, multicentre trials of longer duration are needed to determine their impact on long-term outcomes (such as type 2 diabetes incidence). Economic evaluations should also be incorporated to establish whether the implementation of digital and telemedicine intervention are cost-effective.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
Acknowledgments
AJF is an NIHR Senior Investigator and supported by NIHR Oxford Biomedical Research Centre.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JH made substantial contributions to the conception of the work, acquisition, analysis and interpretation of data for the work, drafted the work, approved the final version to be published and agreed to be accountable for all aspects of the work. MEW made substantial contributions to the acquisition, analysis and interpretation of data for the work as well as revised the work critically for important intellectual content, approved the final version to be published and agreed to be accountable for all aspects of the work. NR made substantial contributions to the acquisition of data for the work as well as revised the work critically for important intellectual content, approved the final version to be published and agreed to be accountable for all aspects of the work. AJF made substantial contributions to the conception of the work and interpretation of data, revised the work critically for important intellectual content, approved the final version to be published and agreed to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.