Article Text

Abstract
Background A clinical decision support system (CDSS) covers a broad spectrum of applications, for example, screening reminders, can reduce malpractice, improve preventive services and enable better management of chronic conditions. CDSSs have traditionally been used successfully in large hospitals. The availability (ie, whether the function is provided by the software) and usage (ie, actual use) of a CDSS in office-based primary care settings, however, are less well studied.
Objective To establish a benchmark of CDSS availability and usage in office-based primary care settings, particularly given the large volume of visits in such settings.
Methods We used the 2015 Centers for Disease Control and Prevention’s National Ambulatory Medical Care Survey to conduct secondary data analysis. We selected preventive services reminders and drug interaction alerts, along with several other variables as examples of a CDSS.
Results CDSS usage rates ranged from 68.5% to 100% among solo or non-solo primary care practices owned by physicians or physician groups that have electronic medical records (EMRs)/electronic health records (EHRs) and 44.7% to 96.1%, regardless of EMR/EHR status. According to proportion tests, solo practices had significantly lower CDSS usage and availability rates on several measures if the practice is entirely EMR/EHR based and significantly lower (16.3%–28.9%) CDSS usage rates than did non-solo practices on each measure, regardless of EMR/EHR status.
Conclusion In the USA, a CDSS, especially under the categories of basic preventive reminders and drug interaction alerts, is used routinely between 68% and 100% in primary care if a practice is entirely EMR/EHR based. More work is needed, however, to determine the reasons for large usage gaps between solo and non-solo practices and to reduce such gaps.
- BMJ Health Informatics
- medical informatics
- BCS Health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known?
Clinical decision support systems (CDSSs) are used successfully in large medical centres and hospitals.
CDSSs are used to reduce malpractice and to improve preventive services and enable better management of chronic conditions.
The usage of CDSSs in office-based primary care settings in the USA is unknown at a national level.
What the new findings are:
The CDSS usage rates, especially under the categories of basic preventive reminders and drug interaction alerts, ranged from 68.5% to 100% in office-based primary care practices in the USA that are entirely electronic medical record (EMR)/electronic health record (EHR) based.
Solo practices had significantly lower CDSS usage and availability rates than did non-solo practices on several measures when practices are entirely EMR/EHR based.
Solo practices have significantly lower CDSS usage rates than do non-solo practices on every measure regardless of a practice’s EMR/EHR status.
How this might have an impact on clinical practice in the foreseeable future:
CDSS usage and availability data can be used as a benchmark on a national level, which may help health information technology-related policymakers to estimate the scale of CDSS usage in primary care settings more accurately.
Solo practices may need additional assistance (eg, more investment in the entire life cycle of CDSS, longer time of investment and more user-friendly technologies) to achieve a level of CDSS usage similar to that of non-solo practices.
Introduction
A clinical decision support system (CDSS) refers to a computerised system or application that can be used within an electronic health record (EHR) or electronic medical record (EMR).1 Meta-analysis has provided strong evidence that a CDSS is effective in increasing preventive care services ordered and completed and in improving treatment ordering and completion.2 In addition, there is moderately strong evidence that a CDSS can reduce patients’ morbidity, decrease costs, and increase providers’ job satisfaction and is effective in providing appropriate clinical study orders.2
In the last decade in the USA, EHR has been increasingly adopted, especially as a result of the Health Information Technology for Economic and Clinical Health Act and Meaningful Use. The EHR adoption rate was 20.8% in 2004 and 86.9% in 2015 in office-based settings.3 EHRs have become the main platform for office-based practices. Although a CDSS is typically a component of an EHR, CDSS availability (ie, whether the function is provided by the software) and usage (ie, actual use) may not be equal to the EHR adoption rate. In the USA, EHR adoption data and usage data, in general, are very well documented (via https://dashboard.healthit.gov and Meaningful Use programme); however, if we attempt to seek more granular data about usage of different components (such as CDSS) within an EHR, no such data points are immediately available yet.
CDSS has been routinely and successfully used in large academic institutions for decades in the form of infobuttons, preventive service reminders or drug–drug interaction alerts, among others, to facilitate healthcare professionals to make more informed decisions.1 4 In the USA, small practices provide healthcare services to a majority of the population, with the volume of physician office visits at about 7.4 times that of hospital visits, according to the Centers for Disease Control and Prevention (CDC).5 Therefore, a CDSS can be a critical tool to provide safer and more consistent care and better preventive services to the majority of the population, as served by office-based practices. CDSS availability and usage data in office-based primary care settings are a critical yet understudied benchmark. How broadly CDSS is used in office-based primary care settings is unknown. Such data may facilitate our understanding of the full potential of using a CDSS in primary care settings and may provide key evidence about the scale of CDSS use for health information technology (IT) policymaking at a national level.
Methods
Data sources and variables selection
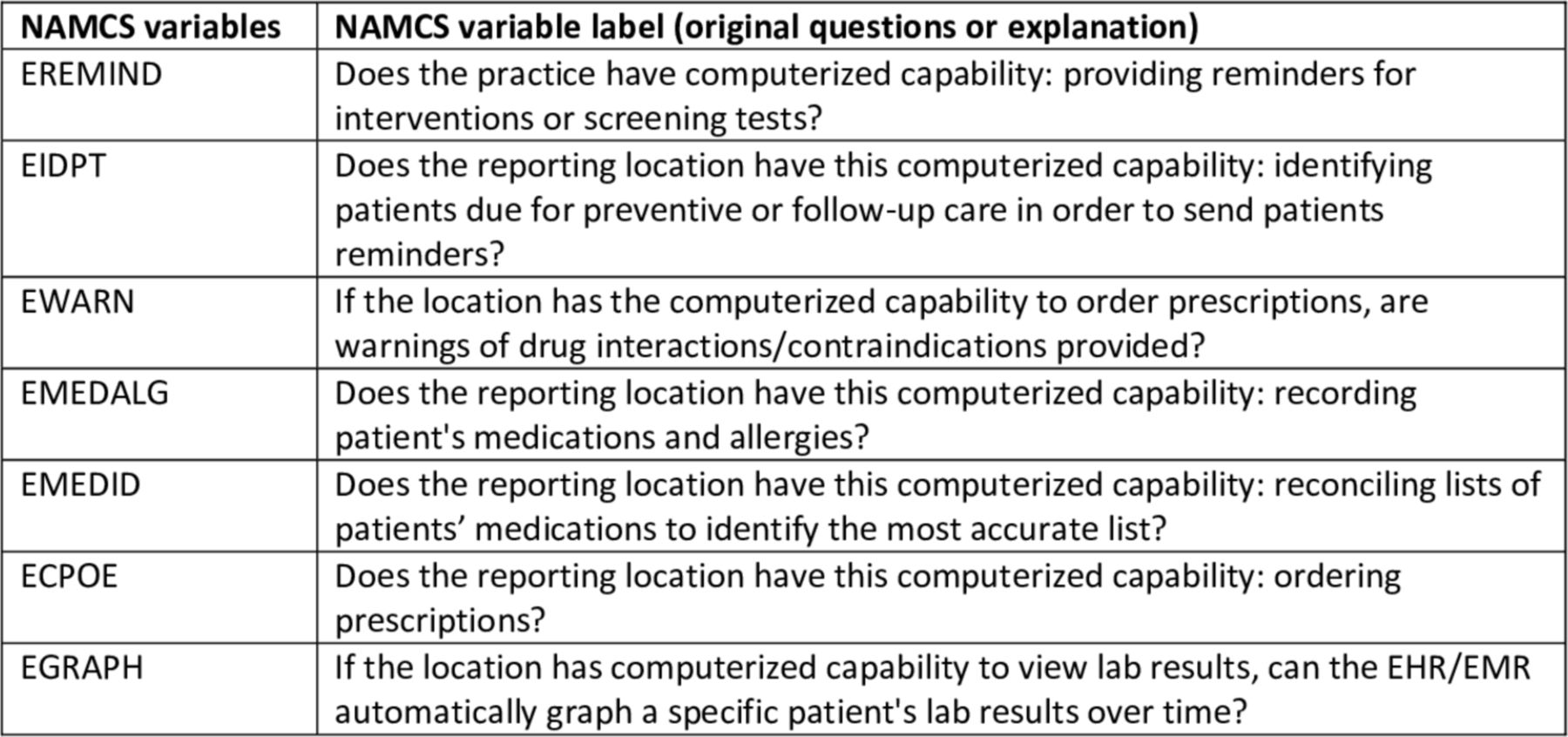
We used data from the CDC’s National Ambulatory Medical Care Survey (NAMCS) 20156 and the Office of the National Coordinator (ONC) for the Health IT Dashboard to conduct secondary data analysis of the availability and use of CDSS in primary care settings. NAMCS focuses on ambulatory medical care provision and usage data in the USA,6 including EHR usage data. The data were collected from physicians based on a sample of visits.6 Hospital visit data and community health centre visit data were collected separately.6 As noted, a CDSS has a number of definitions and a broad spectrum of uses, including knowledge support, for example, infobutton,7 preventive service reminders and drug interaction alerts, among others.8 9 In this paper, we use drug interaction alerts and preventive screening reminders, along with several other variables, detailed in figure 1, as examples of a CDSS.
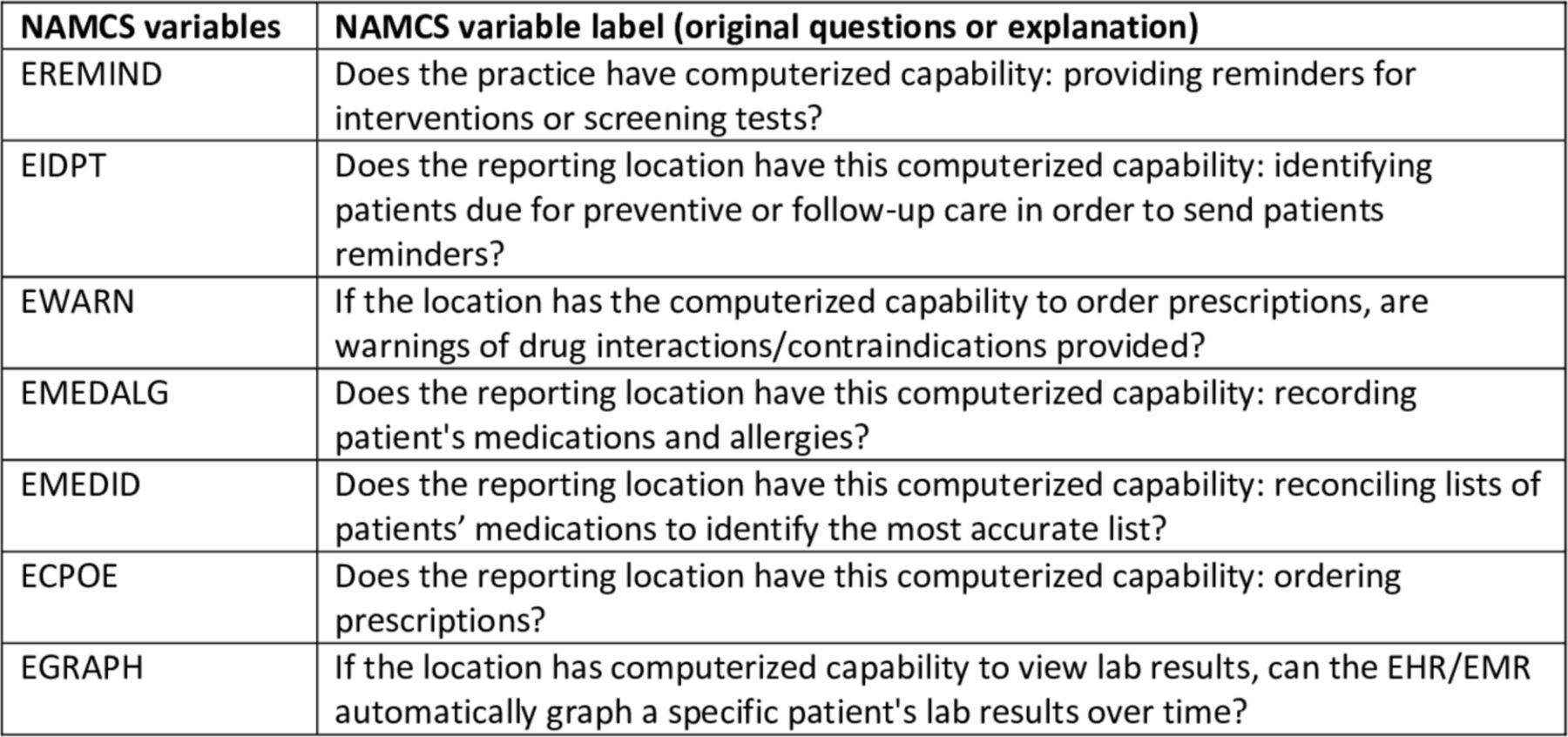
Variables selected from NAMCS 2015 to measure clinical decision support system availability and usage in primary care settings. NAMCS, National Ambulatory Medical Care Survey.
Figure 1 presents all of the variables that we selected from the CDC NAMCS survey, and these are used to measure the availability and usage of a CDSS in office-based primary care settings. Notably, NAMCS is a comprehensive survey that includes over 1000 different variables. The variables and questions that we selected for this paper are only a small fraction of the entire NAMCS 2015. We believe that our selected variables are representative of CDSS use in such settings. The answers to the questions for all of the variables listed in figure 1 include one of the following: 1=yes, used routinely; 2=yes, but not used routinely; and 3=yes, but turned off/not used. We used the sum of 1 and 2 as usage measurements and the sum of 1, 2 and 3 as availability measurements.
Data analytical methods and tools
Initially, we queried the dataset based on the following criteria: the respondents’ selected primary care as the specialty, the reported practices owned by physicians or physician groups, and the reported location as either a solo or non-solo practice that is entirely EMR/EHR based. Among those selected cases, we queried the variables listed in figure 1, one by one, in the survey, via IBM SPSS V.25. For example, for EREMIND, we obtained the frequency of 1, 2 or 3 as answers in the dataset. We then calculated the percentage of the frequency for each answer (ie, 1, 2 and 3) against the total respondents who met the initial criteria, that is, solo and non-solo primary care practices owned by physicians or physician groups that are entirely EMR/EHR based. For comparison purposes, we also reported the percentages for each variable against the solo and non-solo primary care practices owned by physicians or physician groups regardless of their EMR/EHR status.
We present analytical results in percentages, which were calculated via weighted frequencies by physician weight (PHYSWT, weight used for physician-level estimates based on responding in-scope physicians who see patients) to ensure correct calculations, as suggested by the NAMCS 2015 documentation.6 As noted earlier, NAMCS is collected from physicians via a sample of medical visits. To reflect the objective information about the provision and usage of ambulatory medical care, it is critical to use physician weighted frequencies during analysis. This can be implemented via SPSS V.25 by the following steps: selecting data→weight cases→selecting PHYSWT to weight cases before obtaining any frequencies.
We compared two groups: (1) non-solo primary care practices owned by physicians or a physician group and (2) solo primary care practices owned by physicians or a physician group. The majority of the results are presented and compared between the two groups that are entirely EMR/EHR based. We also present the results for each variable between the two groups, regardless of their EMR/EHR status.
Proportion tests via R V.3.4.1 were used to detect the differences among the percentages of routine usage and availability in the two groups for each variable. The main rationale behind this comparison is that solo primary care practices may need more assistance to provide a level of service via a CDSS similar to that of non-solo practices.
This is a secondary data analysis study that uses a publicly available CDC data resource. Therefore, no institutional review board is involved in this study. If no result is reported for any item in the NAMCS 2015 dataset during analysis, it is listed as no value reported in the results.
Results
The NAMCS 2015 results identified 46.45% of survey respondents as those with a primary care specialty. Among the primary care providers, 53.2% were physician owners or physician group owners who practised in non-solo settings, and 46.8% were in solo primary care practices. Among those primary care providers who were either physician owners or physician group owners, 59.3% of solo practices are entirely EMR/EHR based, and in non-solo settings, 86.4% of practices have all EMRs/EHRs. The non-solo settings have a significantly higher EMR/EHR rate. Table 1 lists detailed answers about whether the reported location is entirely EMR/EHR based, a mix of electronic and paper records or paper records only.
The availability of an electronic version of patients’ records in solo and non-solo primary care settings with physician owners or physician group owners (weighted by physician weight of National Ambulatory Medical Care Survey 2015)
The CDSS usage and availability results are presented in table 2 (non-solo practices with physician owners or physician group owners that are entirely EMR/EHR based) and table 3 (solo). table 4 and figure 2 present the comparison of CDSS use in solo and non-solo practices with physician owners or physician group owners regardless of their EMR/EHR status. Both weighted total respondents and the percentages for each variable and each answer are presented in tables 1–4.
CDSS availability (in yellow) and usage (in green) in non-solo primary care settings with physician owners or physician group owners when the reporting location is entirely electronic records based (n=52 807 providers weighted by physician weight of National Ambulatory Medical Care Survey 2015)
CDSS availability (in yellow) and usage (in green) in solo primary care practices with physician owners or physician group owners when the reporting location is entirely electronic records based (n=31 833 providers weighted by physician weight of National Ambulatory Medical Care Survey 2015)
CDSS usage in solo and non-solo primary care practices with physician owners or physician group owners regardless of the EMR/EHR status at the reporting location (providers weighted by physician weight of National Ambulatory Medical Care Survey 2015))

{kind=link}
{kind=link}
Clinical decision support system availability and usage in solo and non-solo office-based primary care settings, regardless of electronic medical record/electronic health record status at the reporting location (practices owned by physicians or physician groups).
Among all of the primary care practices owned by physicians or physician groups that are entirely EMR/EHR based, (1) CDSS usage rates and availability rates are very similar in both solo practices (between 68.5% and 100%) and non-solo practices (between 77.3% and 99.4%); (2) solo practices have significantly higher usage of reminders for intervention and screening tests (ie, EREMIND) than do non-solo practices (93.7% vs 91%, p<0.001); and (3) solo practices have significantly lower usage rates for the following two variables: identifying patients who need preventive services or follow-up reminders (ie, EIDPT, 76.9% vs 89.5%, p<0.001), and drug interaction alerts (ie, EWARN, 91.9% vs 94.3%, p<0.001).
Among all of the primary care practices owned by physicians or physician groups regardless of their EMR/EHR status, CDSS usage rates are significantly lower (p<0.001) in solo practices (between 44.7% and 79.8%) than in non-solo practices (between 73.6% and 96.1%) on every measure. The differences ranged from 16.3% (EMEDALG) to 28.9% (EGRAPH).
The data presented in tables 1 and 2 indicate that 89.5% of non-solo primary care practices owned by physicians or physician groups had used reminders to identify patients who need preventive or follow-up care routinely (ie, EIDPT=1 or 2), compared with 76.9% among solo primary care practices when they both are entirely EMR/EHR based. Further, 77.3% of non-solo primary care practices owned by physicians or physician groups had generated graphs automatically (ie, EGRAPH=1 or 2), and among solo primary care practices, 68.5% had used the same services when they are entirely EMR/EHR based.
Among the primary care practices when they are entirely EMR/EHR based, the availability and usage of EREMIND (p<0.001) in non-solo practices are lower than in solo practices, whereas the availability and usage of EIDPT (p<0.001), EWARN (p<0.001) and EGRAPH (p<0.001) are lower in solo practices than in non-solo practices.
Discussion
We have focused our analysis on office-based primary care practices rather than on larger hospital networks or academic medical centres. The reasons for this are twofold. First, office-based practices serve a greater proportion of the population. Specifically, CDC data from 2012 showed that the volume of office-based visits is about 7.4 times that of hospital visits.5 Second, we anticipate that office-based practices may need additional or different support to become self-sustainable in the use of CDSS, as many of them are under-resourced.
Interpretation of the study results
This paper presents the results of secondary data analysis from a CDC nationwide survey on ambulatory medical care visits, NAMCS. We notice that the survey does not contain a single question regarding CDSS availability and usage. Further, CDSS availability and usage data in primary care settings also are not readily available in the ONC Health IT Dashboard, despite the rich data reported for Meaningful Use. CDSS availability and usage data are critical benchmarks to further identify the true impacts of CDSS in primary care settings. Such data can provide key evidence to estimate the scale of CDSS use and impacts for health IT-related policymaking as well.
The analysis indicates that CDSSs in primary care settings are highly available (71.8% to 100%) and are used routinely (68.5%–100%) when EMR/EHR are used in both solo and non-solo practices. The rates are slightly lower in solo practices when they are entirely EMR/EHR based. Solo practices, however, have a significantly lower overall EMR/EHR rate (59.3% vs 86.4%, p<0.001). Therefore, CDSS usage rates are significantly lower (the differences range from 16.3% to 28.9%) for every measure in solo primary care practices than in non-solo settings without considering their EMR/EHR status. Without a carefully planned investigation, we can only speculate on the reasons (eg, lack of in-house technical support, physicians’ experience and types of EHR systems) for such large differences. The lower availability and usage rates in solo primary care practices suggest that greater investment in the entire life cycle of CDSS, longer time of investment or more user-friendly technology may be necessary to improve CDSS use by this group of practitioners.
Noticeably, about 40% of solo practices do not use EMR/EHR completely, and 23.7% (table 1) of solo practices do not have EMR/EHR at all. Meanwhile, the office-based practices’ general EMR/EHR adoption rate reached 86.9% in 2015. The data show a clear inequity in EMR/EHR adoption in solo practices, even under the US government incentive programme ‘Meaningful Use’. The data also support our hypothesis that small practices, especially solo practices, may need additional support on top of the initial incentives to adopt EMR/EHR, but also support on the use of EMR/EHR continuously and, further, CDSS use on a consistent basis.
When the practices are entirely EMR/EHR based, EREMIND, which provides reminders for interventions or screening tests, is the only variable that solo practices used significantly higher than did non-solo practices. This result shows the true potential of basic CDSS functions in primary care operations, such as reminders. If the CDSS function is useful and the application is straightforward, it will be used frequently at the point of care.
The capability to automatically generate graphs for lab results (ie, EGRAPH) has the lowest availability in non-solo practices and solo practices (78.1% and 71.8%, respectively) and lowest usage rates (77.3% and 68.5%, respectively) when they are entirely EMR/EHR based. The general use rates of automatic graph generation for lab results (ie, EGRAPH) are 73.6% (non-solo) and 44.7% (solo), without considering their EMR/EHR status. The second-lowest availability and usage rates are seen in the capability to identify patients for preventive or follow-up care (ie, EIDPT) in both groups. Although the value of prevention is well recognised, only 12.7%–82.9% of the population receives recommended prevention services.10 A CDSS in primary care settings has the potential to facilitate preventive services2 for the majority of the population. Although we do not have evidence to explain exactly why the use of the EGRAPH and EIDPT is significantly lower in solo practices, we feel that the reason may relate to the following factors: whether the configuration of using EGRAPH and EIDPT is difficult, whether it takes more cognitive power to interpret the generated graphs, or whether the results generated by EGRAPH and EIDPT can be used by primary care providers directly in clinical encounters.
Our original research interest is CDSS usage by primary care physicians in small practices (practices with less than five physicians), for whom both EHR and CDSS are relatively new. According to a 2018 physician survey in the USA, 36.9% (2018 data) of physicians are in primary care.11 About 16.5% of physicians work in a solo practice (2017 data) and 22.3% of physicians work in a two-to-four physician practice (2016 data).11 12 Thus, about 40% of primary care physicians work in small practices, and about 15% of the physicians work as primary care providers in small practices. Considering the possible resource restraints in small practices versus large academic centres or large healthcare systems, these relatively new EHR and CDSS adopters and users may need some health IT support, as it is unlikely there is in-house IT support within these practices. To determine the CDSS usage rate baseline is the first concern that we would like to address, which will set the benchmark for further studies. In the NAMCS dataset, however, only solo and non-solo practice types are collected; therefore, we compared solo and non-solo practices. In addition to the types of practices and the ownership of practices that we used in our analysis, there are other characteristics that may be used to stratify the dataset, for example, payment type (eg, Medicare and Medicaid) and patients’ characteristics.
Significance of using CDSS in clinical practice
CDSS has been used to deliver safer care13 and consistent preventive services as well as to improve chronic condition management.1 2 Using a CDSS in office-based primary care practices can be a critical factor to improve population health, increase preventive services and control ever-growing healthcare expenses.
For example, one of the most commonly reported medical errors made by family medicine physicians in the USA and in other countries concerns prescription medications,14–16 which can be reduced by incorporating and using drug–drug and drug–allergy interaction CDSSs. The ability of a CDSS to capture patients’ medications and allergies is a critical foundation for identifying potential drug–drug and drug–allergy interactions. These features have the highest usage rates in both non-solo primary care practices (about 100%) and solo primary care practices (about 99.4%), if they are entirely EMR/EHR based, suggesting that further implementation of such a CDSS on a larger scale is feasible and likely warranted.
The rules of a CDSS, human and machine-readable, decide a CDSS’s performance within clinical contexts. CDSS rules must be maintained continuously to ensure the full potential of a CDSS over time. Outdated rules can lead to missing alerts about preventive services or follow-up appointments or even to a patient’s death due to outdated drug interaction alerts. Considering the relatively high CDSS usage rates, we envision that CDSS rule management and maintenance will be vital to ensuring that CDSS perform continuously as expected.
CDSS rule management and maintenance have been recognised as challenging in large institutions,4 17–19 which usually have in-house technical support and adequate resources. Thus, we anticipate that CDSS rule management and maintenance will be one of the greatest challenges to increased use in office-based settings, especially in solo practices. Data on the current state of CDSS in these settings will help to estimate the scale of CDSS rule management and maintenance that such settings will need.
Limitations of the study
One limitation of our analysis is that usage data answer only the question of whether the CDSS functionality was used, but do not tell whether the CDSS is used to validate or facilitate the development of, or change physicians’ clinical decisions. Another limitation is that the reported CDSS use focuses on traditional definitions of a CDSS. It is possible that providers also may be using clinical guidelines or proprietary or publicly accessible online resources as a CDSS within their EHR systems. Therefore, the actual use of a CDSS may be much higher than what is reflected in this paper.
Another limitation of this study is that we selected available measures as representatives of CDSS from NAMCS 2015, which is a small portion of CDSS, not comprehensive coverage of CDSS. In addition, preventive alerts are on the administrative side of medical care delivery, not as sophisticated as a true medical decision. We do recognise that CDSS can include a large range of functionalities, from basic preventive reminders, such as those we used in this paper, to the advanced decision support tools, such as those facilitated by deep learning algorithms. Therefore, any further interpretation of our results should be within the context.
Implications of the study and future work
Our results provide strong evidence that CDSS, especially under the categories of basic preventive reminders and drug interaction alerts, is used routinely in primary care practices if the practices are entirely EMR/EHR based, with rates of routine usage that range from 68.5% to 100%. When classified according to practice type, solo practices have significantly lower usage rates on several measures if practices are entirely EMR/EHR based. Solo practices have significantly lower usage rates on every measure without considering practices’ EMR/EHR status. Investment in more user-friendly technologies may be necessary to bring solo practices up to speed in exploring the full potential of a CDSS in clinical care.
Although our data were collected in the USA, we do feel such results can be used as an important reference point and benchmark for international peers to compare the CDSS usage across different countries, especially considering that although USA is a high-income county, its health system is fundamentally different from those of most other high-income countries. Whether such difference plays a role in CDSS usage behaviours, our analysis results provide baseline data for further investigations.
One future research direction is to explore the possibilities to enable primary care providers, especially the ones who work in office-based settings, to manage and maintain CDSS rules independently. Many such practices, especially solo ones, are under-resourced, which is indicated by the lower EMR/EHR adoption rates and lower CDSS usage rates in solo primary care practices. Under-resourced practices are unlikely to allocate additional resources for maintenance of CDSS rules, even though it is necessary to keep CDSS rules updated regularly. Therefore, development of straightforward and user-friendly tools to enable primary care providers to maintain the CDSS rules independently can be a promising solution.
Acknowledgments
The authors thank Ms Kelly Nottingham for her very helpful editing and great suggestions to this paper.
Footnotes
Contributors XJ designed, conducted the analysis and drafted the manuscript; LH verified the analysis and participated in study design and manuscript revision; TL participated in study design and manuscript revision actively.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.