Article Text

Abstract
Introduction Nasal high-flow (nHF) therapy is a popular mode of respiratory support for newborn infants. Evidence for nHF use is predominantly from neonatal intensive care units (NICUs). There are no randomised trials of nHF use in non-tertiary special care nurseries (SCNs). We hypothesise that nHF is non-inferior to nasal continuous positive airway pressure (CPAP) as primary support for newborn infants with respiratory distress, in the population cared for in non-tertiary SCNs.
Methods and analysis The HUNTER trial is an unblinded Australian multicentre, randomised, non-inferiority trial. Infants are eligible if born at a gestational age ≥31 weeks with birth weight ≥1200 g and admitted to a participating non-tertiary SCN, are <24 hours old at randomisation and require non-invasive respiratory support or supplemental oxygen for >1 hour. Infants are randomised to treatment with either nHF or CPAP. The primary outcome is treatment failure within 72 hours of randomisation, as determined by objective oxygenation, apnoea or blood gas criteria or by a clinical decision that urgent intubation and mechanical ventilation, or transfer to a tertiary NICU, is required. Secondary outcomes include incidence of pneumothorax requiring drainage, duration of respiratory support, supplemental oxygen and hospitalisation, costs associated with hospital care, cost-effectiveness, parental stress and satisfaction and nursing workload.
Ethics and dissemination Multisite ethical approval for the study has been granted by The Royal Children’s Hospital, Melbourne, Australia (Trial Reference No. 34222), and by each participating site. The trial is currently recruiting in eight centres in Victoria and New South Wales, Australia, with one previous site no longer recruiting. The trial results will be published in a peer-reviewed journal and will be presented at national and international conferences.
Trial registration number Australian and New Zealand Clinical Trials Registry (ANZCTR): ACTRN12614001203640; pre-results.
- neonatology
- paediatrics
- perinatology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study to compare nasal high-flow with nasal continuous positive airway pressure as respiratory support for newborn infants in non-tertiary settings.
The study is well-powered to detect non-inferiority of nasal high-flow with a non-inferiority margin of 10%; the use of a non-inferiority study design is appropriate given the advantages of nasal high-flow over nasal continuous positive airway pressure.
The study includes assessment of parental stress, nursing workload and financial costs.
Blinding of the allocated respiratory support modes is not possible, so objective criteria were specified for the primary outcome of treatment failure.
Some infants in the nasal high-flow group will have received a brief period of nasal continuous positive airway pressure prior to randomisation.
Introduction
Background
Preterm birth, at <37 weeks’ gestational age (GA), affecting about 15 million infants annually, is a major cause of morbidity and mortality worldwide. About one million infants die from complications of prematurity every year.1 In Australia, about 9% of all births are preterm.2 A major contributor to mortality and morbidity in preterm infants is respiratory distress syndrome (RDS) due to surfactant deficiency in the lungs, which leads to many preterm infants requiring respiratory support soon after birth; the proportion of infants who develop RDS increases with lower GA. However, about 80% of preterm infants are born moderate to late preterm (32–36 weeks’ GA),2 where RDS is less common. Respiratory symptoms in this more mature preterm population, and in term infants, may be due to conditions such as transient tachypnoea of the newborn or infection.
It is estimated that 2.5%–5% of all newborn infants have respiratory distress.3 In Australia, most of these infants are born in a non-tertiary hospital and cared for in a special care nursery (SCN), where (depending on the level of neonatal care available) they may be treated with supplemental oxygen and/or ‘non-invasive’ respiratory support from nasal continuous positive airway pressure (CPAP). However, if these treatments are not available such as in some smaller SCNs, or not successful, or if an infant is born very preterm (<32 weeks’ gestation) or very small (<1250 g), then the infant usually needs to be transferred to a tertiary-level neonatal intensive care unit (NICU). In Australia, neonatal intensive care is centralised in large metropolitan centres, and maternal and infant transfers from regional or rural centres involve large distances and significant costs.
The standard non-invasive respiratory support: CPAP
CPAP uses large prongs in the nose, or a mask over the nose, fitted firmly to the infant’s face. The prongs or mask deliver heated and humidified air and oxygen under pressure. CPAP can be used effectively as the primary mode of respiratory support (the first mode of respiratory support applied after admission to the neonatal unit soon after birth) in infants with respiratory distress, even those born at 25–30 weeks’ gestation.4 5 When used in Australian non-tertiary SCNs to treat late preterm and term infants with respiratory distress, CPAP reduces the need for transfer to a tertiary NICU, and it reduces costs in comparison to the use of supplemental oxygen alone.6 However, CPAP has been associated with an increased risk of pneumothorax compared with supplemental oxygen alone.6 7
CPAP is a widely used method of respiratory support in larger Australian SCNs,8 9 but it has some disadvantages. CPAP fixation devices are bulky and cover much of the infant’s face, interfering with parental interaction and feeding; trauma to the nasal skin or septum is a commonly reported complication.10 Nursing vigilance is required to ensure that an adequate seal (and hence pressure) is maintained without causing nasal injury. For these reasons, and others including limits on staff and equipment, CPAP is not currently a feasible therapy in smaller Australian SCNs (with birth rates mostly <1500/year) that infrequently care for infants who require respiratory support.
The new therapy: nasal high-flow
In recent years, nasal high-flow (nHF) therapy, a newer form of non-invasive respiratory support, has become popular as an alternative to CPAP around the world, including in Australasian SCNs.9 11–15 nHF therapy delivers heated, humidified, blended oxygen and air via small binasal prongs, using gas flows of at least 1 L/min.16 While nHF therapy has been adopted by many NICUs around the world, there has until recently been relatively little evidence to support this practice. The increasing popularity of nHF seems to be due to its reported advantages over CPAP: it is easier to apply and maintain, more comfortable for infants, associated with less nasal trauma and preferred by parents and nursing staff.17–20 If nHF was demonstrated to be an effective mode of respiratory support in non-tertiary SCNs, these factors would make it the preferred interface in this setting.
Clinical trials of nHF in newborn infants
Preventing extubation failure in NICUs
The majority of published randomised controlled trials (RCTs) of nHF have evaluated its use as an alternative to CPAP, as postextubation respiratory support. An updated Cochrane Review20 of these trials, published in 2016, found no difference in rates of treatment failure or reintubation in infants treated with postextubation nHF, compared with those treated with CPAP. The nHF infants were noted to have lower rates of nasal trauma and a small reduction in the risk of pneumothorax.
Primary respiratory support for newborn infants
Prior to the HUNTER trial commencing, there was little evidence from RCTs to support the use of nHF as primary support for newborn infants. Yoder et al 21 conducted an RCT in 432 infants, of whom about one-third were included in an ‘early support’ arm. There was no difference between the nHF and CPAP groups in need for intubation or in other neonatal morbidities. Studies by Iranpour et al 22 and Kugelman et al,23 each including approximately 70 infants, compared nHF with CPAP and nasal intermittent positive airway pressure, respectively, as early respiratory support for preterm infants; they found no difference between groups in rates of treatment failure or other important outcomes.
Within the past year, two larger RCTs evaluating nHF as primary respiratory support in NICUs have been published. The HIPSTER trial24 included 564 preterm infants of mean 32 weeks’ GA and 1.7 kg in birth weight, not previously treated with surfactant, in nine NICUs in Australia and Norway; nHF use resulted in a higher rate of treatment failure (based on objective clinical criteria) than CPAP (25.5% vs 13.3%, p<0.01), but no greater risk of intubation, likely due to the use of ‘rescue’ CPAP in infants with nHF failure. Lavizzari et al 25 studied 316 infants of mean 33 weeks’ GA and 1.9 kg in birth weight in an Italian NICU. They found no difference in rates of treatment failure (mechanical ventilation within 72 hours) between infants treated with nHF and those treated with CPAP and/or biphasic positive airway pressure (10.8% vs 9.5%, p=0.71). However, it is notable that infants in this study could be intubated, treated with surfactant and extubated (‘INSURE’ treatment), without being classed as having treatment failure. Surfactant use was common, occurring in >40% of infants in both treatment groups.
While providing important guidance on the use of primary nHF in NICUs, it is important to recognise that the results of these studies cannot be directly applied to use in non-tertiary SCNs, where there is currently no high-quality evidence to guide practice. Staffing in SCNs is different to that in tertiary NICUs, and infants in SCNs have different antenatal exposures, GAs and pathologies.
Summary and rationale
The reported advantages of nHF—easier nursing care, improved feeding and parental interaction, reduced nasal trauma and greater infant comfort—have led to widespread adoption of this new therapy. While there are now a number of studies assessing nHF use in the NICU, there are no published trials that study the efficacy and safety of nHF compared with CPAP as early respiratory support for newborn infants in SCNs. The reference treatment against which non-inferiority is being assessed, CPAP, has been shown to be effective in SCNs in a study with similar inclusion criteria and CPAP treatment protocols.6 If proven to be effective and safe, the ease of use of nHF would mean that it could be widely applied to infants with respiratory distress in non-tertiary SCNs, both in Australia and around the world, potentially reducing the need for transfer to a tertiary NICU—reducing costs and keeping mothers and their babies together. Conversely, if nHF is shown to be unsafe or significantly less effective than CPAP, this will guide clinicians to avoid nHF treatment of newborn infants outside NICUs. The above considerations led to the adoption of a non-inferiority trial design.
Methods and analysis
Study design
HUNTER is a multicentre, randomised, non-inferiority trial, including newborn infants cared for in Australian non-tertiary SCNs, who require early non-invasive respiratory support in the first 24 hours of life. A schedule of enrolment, interventions and assessments is shown in the figure.

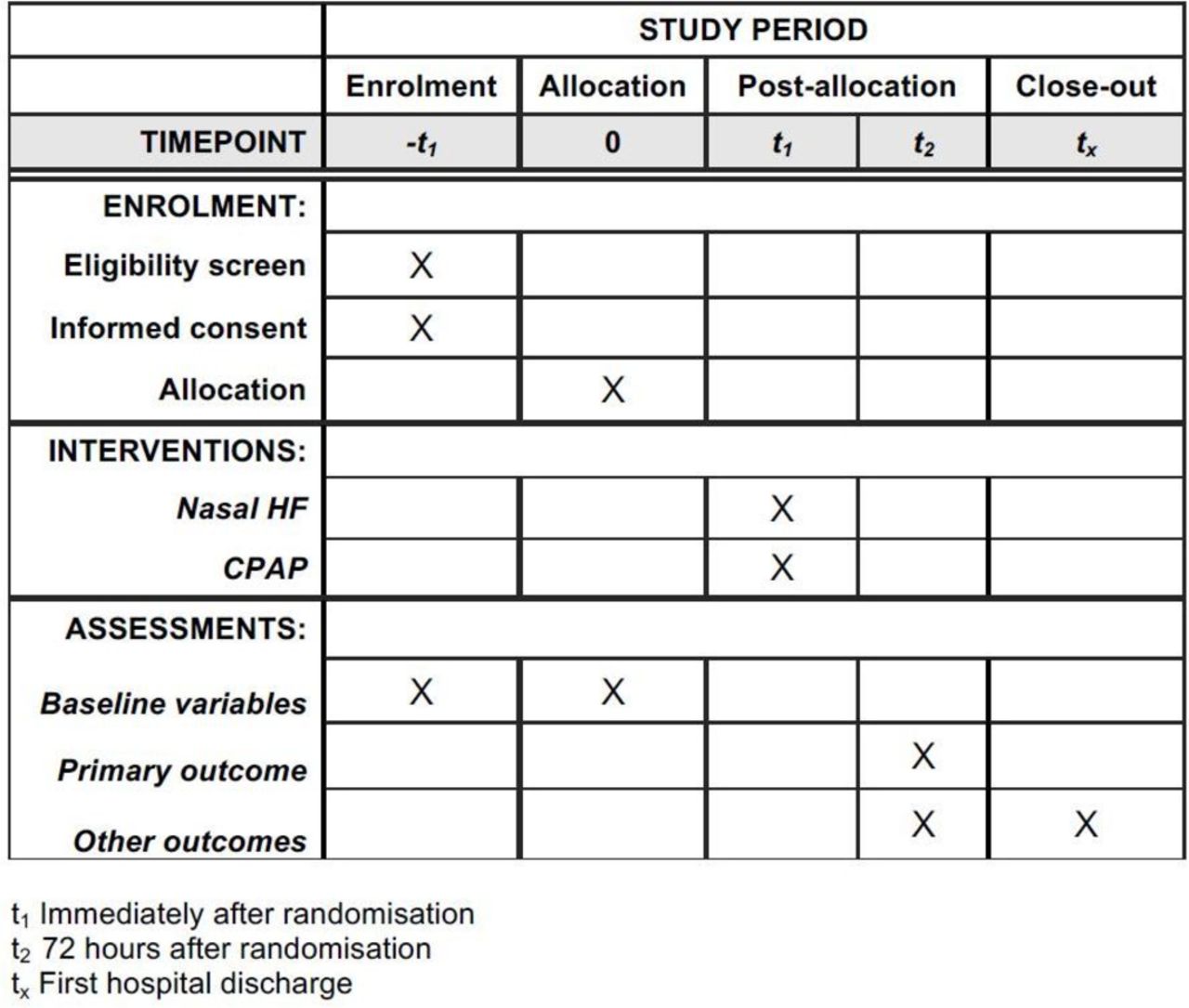{kind=link}
Schedule of enrolment, interventions and assessments: the HUNTER trial. HF, high flow; CPAP, continuous positive airway pressure.
Aim
The aim of the HUNTER trial is to determine whether nHF is non-inferior to CPAP in avoiding treatment failure when used as early non-invasive respiratory support for newborn infants cared for in Australian non-tertiary SCNs.
Blinding
Blinding of the allocated treatment is not feasible, as the mode of respiratory support is clearly apparent to medical and nursing staff and parents/guardians. We have therefore defined objective criteria for the primary outcome to minimise potential bias, and have provided guidance to clinicians considering the need to escalate respiratory support and/or arrange transfer to a tertiary NICU.
Outcomes
The primary outcome will be assessed on a hypothesis of non-inferiority. Outcomes, eligibility criteria and the CPAP treatment protocol are similar to those of a study in Australian SCNs that demonstrated the efficacy of CPAP in comparison to passive oxygen for preventing treatment failure.6 The major change from that study is a reduction in the fraction of inspired oxygen (FiO2) threshold for treatment failure from 0.50 to 0.40, in line with current international practice to reduce neonatal oxygen exposure.
Primary outcome
The primary outcome is treatment failure within 72 hours of randomisation. Treatment failure occurs when an infant has reached maximal therapy for their allocated treatment (nHF 8 L/min or CPAP 8 cm H2O) and one or more of the following criteria are satisfied:
Sustained increase in oxygen requirement: fraction of inspired oxygen (FiO2) ≥0.40 for more than 1 hour to maintain peripheral oxygen saturation (SpO2) 91%–95%.
Respiratory acidosis: both pH <7.20 and pCO2 >60 millimetres of mercury (mm Hg) on two blood gas samples (which can be capillary, venous or arterial), with the first sample collected at least 1 hour after initiation of the assigned treatment and the second sample taken at least 1 hour after the first.
Frequent or severe apnoea: more than one apnoea receiving positive pressure ventilation within any 24 hours period, or six or more apnoeas in any 6-hour period receiving intervention (stimulation or increased oxygen).
The treating paediatrician determines that urgent intubation and mechanical ventilation is required.
The treating paediatrician determines that the infant requires transfer to a tertiary NICU, through consultation with the local neonatal transport service.
Secondary outcomes
The secondary outcomes are as follows:
Cost: estimated differences between the interventions based on the costs of equipment, care in SCNs and NICUs, costs associated with hospital stay, costs to the family and the costs of transfer (both infant and maternal).
Mortality (specified as a significant adverse event).
Pneumothorax requiring drainage via needle thoracocentesis or intercostal catheter insertion (specified as a significant adverse event).
Duration of supplemental oxygen (hours).
Oxygen supplementation at 28 days of age, or at 36 weeks’ corrected GA for infants born <32 weeks’ gestation.
Mechanical ventilation via an endotracheal tube in the first 72 hours after randomisation and at any time prior to discharge home.
Duration of respiratory support (hours): including hours of nHF, CPAP and mechanical ventilation.
Duration of hospital admission and duration of admission to a tertiary NICU (days).
Incidence of nasal trauma.
Weight gain and feeding performance, including weight gain from birth to hospital discharge, proportion of infants fully breastfed at discharge, number of days receiving any intravenous fluids and number of days to reach full suck feeds (defined as tolerating suck feeds without any requirement for intravenous fluids or nasogastric/orogastric feeds for >24 hours).
Parental stress and satisfaction, measured using a modified version of the validated Parental Stressor Scale: NICU,26 assessed as soon as possible after treatment has ceased, or prior to transfer to a NICU.
Nursing workload and treatment preference, measured using the Professional Assessment of Optimal Nursing Care Intensity Scale tool,27 and by questionnaire.
Setting
The trial has been enrolling infants in nine non-tertiary SCNs in Victoria and New South Wales, Australia. All participating SCNs routinely care for newborn infants with respiratory distress, using CPAP as the standard non-invasive support mode; participating centres did not previously use nHF to treat newborn infants. No Australian SCNs provide ongoing mechanical ventilation; this is only provided while awaiting transfer of the infant to a tertiary NICU. All participating centres administer exogenous surfactant if the infant requires intubation for RDS prior to retrieval by the neonatal transport team; the standard of care is that all these infants are transferred to a tertiary NICU. Two participating centres have some experience using the ‘INSURE’ (Intubate, Surfactant, Extubate) procedure28 in select infants with the support of the neonatal transport service (after which NICU transfer could potentially be avoided), but this is an infrequent practice that is staff dependent. The participating SCNs have 24 hour on-site junior paediatric staff and a designated on-call consultant paediatrician available to advise management and/or attend as required. Some participating centres have one or two consultant staff with specialist neonatal training, but most Australian SCNs do not.
Eligibility criteria
Infants are eligible for inclusion in the trial if:
They are born at ≥31 weeks’ GA by best obstetric estimate and have birth weight ≥1200 g; and
They are admitted to the SCN of a participating centre and are <24 hours old at the time of randomisation; and
They require non-invasive respiratory support after admission to the SCN (at clinician discretion) or require any supplemental oxygen to maintain SpO2 91%–95% for more than 1 hour.
Infants are excluded from the trial if:
They have received more than 2 hours of CPAP prior to randomisation; or
They have previously been intubated (including intubation for suctioning below the cords in the delivery room), or immediately need intubation, as determined by the attending paediatrician; or
They have a known major congenital abnormality that may impact on the infant’s condition after birth (eg, complex congenital cardiac disease, upper airway obstruction, gastrointestinal malformation); or
They are judged by their paediatrician to require transfer to another hospital for ongoing care (the reason for this decision will be clearly documented).
Randomisation
Randomisation will be prestratified by centre and according to GA at birth: <34 weeks’ GA and ≥34 weeks’ GA. Within each stratum, a 1:1 allocation ratio and block randomisation with variable block sizes (4, 6 or 8) will be used. Multiple births with more than one eligible infant will be randomised individually. Each participating centre will be provided with consecutively numbered, sealed opaque randomisation envelopes containing the assigned treatment allocation. The appropriate envelope will be opened after written consent has been obtained and the infant has become eligible for the trial; the assigned treatment will then immediately be applied to the infant. Random sequences were generated in SAS v9.4 by author Arnolda.
Clinical management
Eligible and consented infants will be randomised to treatment with either nHF or CPAP; allocated treatment will be applied immediately after randomisation. Infants in both groups will receive standard supportive care as per local policies, for example, blood tests, antibiotics, intravenous fluids/nutrition and enteral feeds. In both groups, supplemental oxygen will be adjusted to maintain SpO2 91%–95%. Chest X-rays and blood gas analyses are not mandated prior to randomisation, and the timing of these investigations will be a physician discretion in keeping with the pragmatic trial design; however, it is expected that most enrolled infants will have these investigations performed as per local guidelines.
Interventions
nHF therapy is defined as heated, humidified gas (blended air/oxygen) delivered at gas flows of 5–8 L/min via the Fisher & Paykel ‘Optiflow Junior’ circuit and prongs (Fisher & Paykel Healthcare, Auckland, New Zealand).
CPAP is defined as the use of short binasal prongs or nasal mask to deliver heated, humidified gas (blended air/oxygen) using a ‘bubble’ CPAP device (any brand may be used) with set pressures of 5–8 cm H2O.
Intervention group: nHF
A nasal cannula size should be selected that maintains a leak at the nares.
The starting flow will be 6 L/min for all infants.
Increasing nHF support: Gas flow may be increased to a maximum of 8 L/min.
If treatment failure criteria are satisfied, infants should receive CPAP 8 cm H2O and then be managed as per the CPAP group protocol:
If treatment failure criteria are again satisfied when the infant is receiving CPAP 8 cm H2O, it is recommended that the treating paediatrician consider referral to the local neonatal transport service for advice and/or transfer of the infant to a tertiary NICU, and surfactant may be administered at the paediatrician’s discretion according to the unit’s individual policy.
If the infant’s condition is improving, the CPAP pressure should be weaned, and nHF may be reinstituted at the paediatrician’s discretion.
Decreasing and ceasing nHF support.
Gas flow may be decreased (in decrements of 1 L/min) or ceased if there is no supplemental oxygen requirement (infant is receiving air), or if the infant has required FiO2 <0.25 for >24 hours.
nHF should be ceased when the gas flow is 5 L/min, and there is no supplemental oxygen requirement, or the infant has required FiO2 <0.25 for >24 hours:
If nHF is ceased, infants may receive ongoing oxygen supplementation via ‘low-flow’ nasal cannulae, cot oxygen or head-box oxygen.
After ceasing nHF, if non-invasive breathing support is again required, nHF should be recommenced at ≥5 L/min and managed as above.
Infants randomised to nHF will not receive CPAP after randomisation, unless treatment failure criteria are met.
Standard care group: CPAP
The starting set pressure will be 6 cm H2O for all infants.
Increasing CPAP support: the set CPAP pressure may be increased to a maximum of 8 cm H2O.
If treatment failure criteria are satisfied, it is recommended that the treating paediatrician consider referral to the local neonatal transport service for advice and/or transfer of the infant to a tertiary NICU, and surfactant may be administered at the paediatrician’s discretion according to the unit’s individual policy.
Decreasing and ceasing CPAP support:
The set pressure may be decreased (in decrements of 1 cm H2O) or ceased if there is no supplemental oxygen requirement (infant is receiving air), or if the infant has required FiO2 <0.25 for >24 hours.
CPAP should be ceased when the set pressure is 5 cm H2O, and there is no supplemental oxygen requirement, or the infant has required FiO2 <0.25 for >24 hours.
If CPAP is ceased, infants may receive ongoing oxygen supplementation via ‘low-flow’ nasal cannulae, cot oxygen or head-box oxygen.
After ceasing CPAP, if non-invasive breathing support is again required, CPAP should be recommenced at ≥5 cm H2O and managed as above.
Infants randomised to CPAP will not receive nHF at any stage of their admission.
Sample size calculation
Non-inferiority of nHF will be determined using the absolute risk difference (RD) and 95% CI for the primary outcome of treatment failure within 72 hours of randomisation. We have set the margin of non-inferiority at 10%. Thus, for nHF to be non-inferior to CPAP, the upper limit of the two-sided 95% CI of the RD must be <10%. This margin was adopted after agreement between the site investigators and our parent representative; it is equivalent to the smallest margin chosen in previously published non-inferiority trials of neonatal respiratory support,25 29 and it is narrower than in most non-inferiority trials published in the adult medical literature.
Based on pretrial data from six non-tertiary SCNs, we estimate the rate of the primary outcome in the CPAP group will be 17%. A sample size of 750 infants (375 infants in each group) is required to demonstrate non-inferiority of nHF with 90% power: that is, to be 90% sure that the upper limit of a two-sided 95% CI will exclude a difference in favour of CPAP of more than 10% (www.sealedenvelope.com/power/binary-noninferior).
Statistical analysis and economic evaluation plan
Statistical analysis will be performed by authors Manley and Arnolda with assistance from the Trial Steering Committee. Data will be exported from an electronic database to an electronic statistical package for analysis. The primary analysis will be by intention to treat. A secondary per protocol analysis will also be performed for the primary outcome and any important differences reported, as is recommended for non-inferiority trials.30
The difference between the groups in the incidence of the primary outcome will be reported using RD with two-sided 95% CI. Subgroup analysis by GA at birth will be performed for the primary outcome and selected secondary outcomes. Dichotomous secondary outcomes will be compared with an RD (two-sided 95% CI) and a Χ2 test. Continuous secondary outcomes will be compared by the appropriate parametric (t-test) or non-parametric (Mann-Whitney U) test. The primary outcome will be assessed on a hypothesis of non-inferiority; all secondary outcomes will be assessed against a hypothesis of superiority.
Cost-effectiveness analysis will be conducted from the healthcare system perspective, incorporating the costs of inpatient stay including the associated device and patient transfer costs. Routinely available costs of inpatient stay will be sourced from the hospital costing units. To inform whether it is cost-effective to incorporate nHF or CPAP into the existing health system, decision analysis will be constructed based on the primary outcome and associated hospital costs. Univariate and probabilistic sensitivity analyses will be conducted to test the impact of uncertainty in data.
Nursing workload measures will be analysed using longitudinal methods, as these are provided by the nurse primarily responsible for the infant at the hospital of birth, for each shift in the first 72 hours of care after randomisation.
Ethics and dissemination
Research ethics approval
Multisite ethical approval for the study has been granted by The Royal Children’s Hospital, Melbourne, Australia (No. 34222, current approved protocol version 6, 15 May 2017). Site-specific governance approval has been granted by the following human research ethics committees: Victoria, Australia: Western Health, Northern Health, Eastern Health, Barwon Health and Monash Health; New South Wales, Australia: Central Coast Local Health District and Illawarra Shoalhaven Local Health District.
Recruitment and consent
In all cases, prospective, written consent will be obtained from a parent or guardian. Consent may be either antenatal or postnatal.
For postnatal consent, eligible infants will be identified after birth and their parents or guardians approached as soon as possible for prospective consent. Parents or guardians of infants who are not yet eligible but are likely to become eligible (eg, infants requiring supplemental oxygen who are likely to continue on this treatment) may also be approached. In some cases, antenatal consent may be obtained (eg, when a preterm birth is planned). Written consent will be recorded on the trial patient information and consent form.
Consent will be obtained by a doctor or nurse who has been trained in obtaining consent for the trial and who has received education regarding the trial protocol. Wherever possible, consent will be obtained by someone not directly involved in the clinical care of the infant at the time.
Data collection, storage and access
Data will be sourced from the infant’s bedside observation chart, medical and nursing notes, pathology results, electronic monitors, the mother’s medical chart and verbally and by questionnaire from parents/guardians and nursing staff. Data will be de-identified and entered onto a paper case record form and subsequently will be entered into a secure, web-based electronic database. Only the members of the Trial Steering Committee will have access to the final dataset.
Monitoring and safety
An independent data safety and monitoring committee (DSMC) has been convened, consisting of two neonatologists, a paediatric emergency specialist and a statistician. An early safety review was undertaken after 150 infants were recruited to the trial, and further safety reviews are planned approximately 6 monthly. A single review of the primary outcome and its components was planned, after the primary outcome was known for 375 participants.
Defined serious adverse events (SAEs) for the study are:
Air leak from the lung (pneumothorax) requiring drainage via needle thoracocentesis or intercostal catheter insertion.
Death before discharge from hospital.
All incidences of these SAEs are reported to the lead Human Research Ethics Committee and to committees at the relevant site.
The DSMC may make a recommendation to the Steering Committee to temporarily or permanently stop the trial. Although no formal stopping rule will be used, such a decision may be based on:
A difference in the primary outcome such that the committee considers the trial should no longer continue.
An increase in the rate of SAEs in the nHF group.
Equipment failure or unforeseen complications pertaining to the equipment or its manufacture.
New information such as other trial results which make it ethically impossible to continue the trial.
The primary outcome review was completed in December 2016, and on the basis of this, and on safety reviews conducted to date, the DSMC has recommended that the trial continue without modification.
Dissemination of results
The results of the trial will be published in a peer-reviewed journal and will be presented at national and international conferences.
Current status and study duration
The trial began recruiting in April 2015, with additional sites joining subsequently. It is currently recruiting in eight centres, with one previous site ceasing recruitment due to a change in its level of care classification, meaning that it could no longer care for infants requiring prolonged non-invasive respiratory support. To the end of March 2017, over 500 infants have been enrolled in the trial. It is expected that recruitment for the study will be completed in 2018.
Discussion
nHF therapy has been widely adopted in neonatal practice due to its desirable qualities such as ease of use, reduced nasal trauma and parental and nursing preference.17–20 Recently, the HIPSTER trial demonstrated that in NICUs, rates of treatment failure with nHF are higher than with CPAP in preterm infants born ≥28 weeks’ GA, although with ‘rescue’ CPAP available there is no difference in rates of intubation.24 The HIPSTER results suggest that CPAP should be favoured over nHF if only one treatment is available; however, these findings cannot be directly applied to environments other than the NICU. The other recently published trial of primary nHF was also performed in a NICU and it included a high rate of surfactant administration by the INSURE technique, an intervention which is not currently practised routinely in Australian SCNs, and that has not been well-studied in the SCN setting or in the infant population relevant to SCNs (infants ≥31 weeks’ GA).28
There has traditionally been a lack of clinical research in newborn infants cared for in non-tertiary SCNs and only one previous RCT of respiratory support in this setting.6 Research in SCNs is important because care of infants in these units incorporates a number of factors distinct from tertiary NICUs. Non-tertiary SCNs do not care for large numbers of very preterm or very low birth weight infants and often need to treat term infants with respiratory distress. The resources and staffing available in non-tertiary SCNs are different from those in NICUs, and while capable of intubation and mechanical ventilation as a stabilisation measure, SCNs are not equipped to provide this level of treatment for longer periods. The implications for failure of non-invasive support are therefore greater in SCNs: transfer of the infant to a NICU and separation from his or her parents. Furthermore, there are potentially important financial implications of treatment failure: retrieval by specialist neonatal transport services, particularly when over long distances, as would apply in many areas of Australia, bears a significant cost. Transfers from SCNs also have an impact on staffing and resource allocation in receiving tertiary NICUs.
There has never been a randomised trial of nHF in non-tertiary SCNs; nHF may be an effective mode of support in this setting and, due to its ease of use, would be preferable to CPAP if shown to be non-inferior. However, it is equally important to determine if nHF is unsafe or significantly inferior to CPAP, so that clinicians may be guided to avoid nHF use in non-tertiary SCNs. If nHF use was associated with a reduction in nursing workload, it may prove to be more cost-effective than CPAP or may result in a greater capacity to manage infants requiring non-invasive support in SCNs. CPAP is associated with an increased risk of pneumothorax in comparison with oxygen treatment.6 A Cochrane Review noted nHF treatment to be associated with a small reduction in pneumothorax rate compared with CPAP.20 If a lower rate of this complication was seen in our trial with nHF, in conjunction with non-inferiority in treatment efficacy, nHF could be the preferred mode of treatment.
The HUNTER trial is a well-powered, carefully designed randomised clinical trial, which will determine whether nHF is an appropriate mode of early respiratory support for newborn infants in the non-tertiary setting. The non-inferiority design used in the HUNTER trial was until recently quite rare but has been used recently in similar trials by our group.24 31 The choice of non-inferiority margin of 10% was made in view of the fact that the primary outcome was treatment failure and not a more critical outcome, such as death, and that infants who have treatment failure on nHF will be offered CPAP, which may ‘rescue’ them from intubation and/or transfer to a NICU, as seen in previous NICU trials of nHF.24 31 32
A potential limitation to this trial is that blinding of treatment allocation is not possible. We have attempted to minimise this by setting objective treatment failure criteria, which were agreed on by all participating centres. Some infants allocated to nHF will receive a brief period of CPAP before randomisation, which conceivably could affect interpretation of the results. However, we have aimed to restrict the impact of this by excluding infants who have received two or more hours of CPAP from the trial, which we felt to be the shortest window in which seeking parental consent would be feasible. The HUNTER trial is a pragmatic trial, designed to assess whether nHF is non-inferior to CPAP in real-world practice. We have not mandated the need or timing of investigations such as chest X-rays or blood gas analysis nor have we protocolised the decision to treat infants with non-invasive support, which remains at clinician discretion. We acknowledge that some randomised infants may have recovered from respiratory distress without the use of non-invasive support or may have an unrecognised pneumothorax if randomised prior to a chest X-ray being performed.
The use of nHF in NICU practice is well-established and supported by evidence from multiple RCTs. However, nHF use is also being adopted in non-tertiary SCNs,9 13–15 a setting in which there is little evidence of its efficacy and safety. If this trial demonstrates that nHF is non-inferior to CPAP as primary support for newborn infants in non-tertiary SCNs, then many units worldwide are likely to incorporate nHF into their routine practice. However, if nHF is inferior to CPAP, the results of this study will ensure that this treatment is not applied inappropriately, and infants in non-tertiary SCNs with respiratory distress will continue to receive evidence-based care.
Acknowledgments
The HUNTER Trial Investigators: Amy Brett and Bernice Mills (Victorian trial coordinators), The Royal Women’s Hospital, Victoria, Australia; Jane Wardle (New South Wales trial coordinator), Gosford Hospital, New South Wales, Australia; Wei Qi Fan, Northern Hospital, Victoria, Australia; Isaac Marshall, Geelong Hospital, Victoria, Australia; Rosalynn Pszczola, Sunshine Hospital, Victoria, Australia; Alice Fang, Box Hill Hospital (Eastern Health), Victoria, Australia; Tracey Clark, Dandenong Hospital (Monash Health), Victoria, Australia; Alex Aldis, NICU parent and Life’s Little Treasures Foundation, Victoria, Australia. Data Monitoring and Safety Committee: David Cartwright (Chair), Royal Brisbane and Women’s Hospital, Queensland, Australia; Chris McKinlay, Liggins Institute, University of Auckland, New Zealand; Stuart Dalziel, Starship Children’s Hospital, Auckland, New Zealand; Susan Donath, Murdoch Childrens Research Institute, Victoria, Australia. Health Economics: Li Huang, The University of Melbourne.
References
Footnotes
Contributors BJM conceived and designed the trial protocol, co-wrote the first draft and revised the manuscript for intellectual content. CTR co-wrote the first draft and revised the manuscript for intellectual content. GRBA, AGB, IMW, LSO, JPF and PGD conceived and designed the trial protocol and revised the manuscript for important intellectual content. GRBA designed the statistical analysis. KMD designed the cost-effectiveness analysis and revised the manuscript for important intellectual content. All the authors have read and approved the final manuscript, and all are accountable for its accuracy.
Funding The trial is funded by the National Health and Medical Research Council (NHMRC), Australia (Project grant 1098790). Brett Manley is the recipient of an NHMRC Early Career Fellowship (1088279).
Competing interests None declared.
Ethics approval Human Research and Ethics Committee, The Royal Children's Hospital, Melbourne, Australia.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Only the members of the Trial Steering Committee will have access to the final dataset.
Correction notice This paper has been amended since it was published Online First. Owing to a scripting error, some of the publisher names in the references were replaced with 'BMJ Publishing Group'. This only affected the full text version, not the PDF. We have since corrected these errors and the correct publishers have been inserted into the references.