Article Text

Abstract
Objectives The aim of the current study is to quantify mental health-related emergency department (ED) presentations and hospitalisations, and associated child and family characteristics, in children recruited through four Aboriginal Community Controlled Health Organisations.
Setting Four Aboriginal Community Controlled Health Services that deliver primary care. All services were located in urban or large regional centres in New South Wales, Australia.
Participants 1476 Aboriginal children aged 0–17 years at recruitment to the Study of Environment on Aboriginal Resilience and Child Health.
Primary outcome measures ED presentations and hospital admissions with a primary mental health diagnosis obtained via linkage to population health datasets.
Results Over a median of 6-year follow-up, there were 96 ED presentations affecting 62 children (10.7/1000 person-years) and 49 hospitalisations affecting 34 children (5.5/1000 person-years) for mental health conditions. Presentations/admissions increased with age. ED presentation was increased with: living in foster versus parental care (adjusted rate ratio (RR)=3.97, 95% CrI 1.26 to 11.80); high versus low baseline child emotional/behavioural problems (adjusted RR=2.93, 95% CrI 1.50 to 6.10); and caregiver chronic health conditions versus none (adjusted RR=2.81, 95% CrI 1.31 to 6.63). Hospitalisations were significantly increased with caregiver unemployment versus home duties (adjusted RR=4.48, 95% CrI 1.26 to 17.94) and caregiver chronic health problems versus none (adjusted RR=3.83, 95% CrI 1.33 to 12.12).
Conclusions Tertiary care for mental health issues was relatively common among participating Aboriginal children, with risk elevated for those living in foster care, with prior mental health and behavioural problems and with carers with chronic illness and/or unemployment. While this study suggests high rates of serious mental health events among children from participating communities, the optimum means for reducing these rates, and the need for tertiary care, has not yet been determined. Such information is urgently required to inform policy and programmes to support Aboriginal child and adolescent mental health.
- mental health
- aboriginal
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The current study provides, for the first time, insights into mental health-related emergency department presentations and hospitalisations among Aboriginal children and adolescents and their association with child and family characteristics.
Study of Environment on Aboriginal Resilience and Child Health (SEARCH) is the largest cohort of Aboriginal children living in urban and large regional centres in Australia. Emergency department and hospitalisation data were ascertained via linkage to population health datasets.
Like many cohort studies, SEARCH is not a representative sample. Consequently, emphasis should be placed on the relative risk estimates, indicating associations between child and family characteristics and tertiary mental healthcare, rather than the absolute rates of tertiary care.
SEARCH has a small sample size and limited statistical power, which may have underidentified child and family characteristics related to the receipt of tertiary care for mental health.
Background
Mental health problems are the chief health issue experienced by Australian young people, accounting for more than half of the burden of disease among individuals aged 15–25 years.1 As is the case among Indigenous young people from other high-income countries,2–4 mental health challenges are more common among Australian Aboriginal children and adolescents than other Australian young people,5–7 and suicide rates are several times higher.5 Data from the Study of Environment on Aboriginal Resilience and Child Health (SEARCH) indicated that 28% of participants aged 4–17 years were at a high risk of clinically significant emotional or behavioural problems,8 compared with 7.6% of all children in New South Wales (NSW).9 The disproportionately high rates of mental health problems noted among Aboriginal young people reflect the cumulative impact of the trauma, loss, disempowerment, racism and disadvantage that have been the legacy of colonisation.10 11 Improving the mental health of Aboriginal young people should be an urgent priority given the acute and long-term consequences of poor mental health on social, academic and developmental outcomes12 13 and on health and well-being.14
Mental health funding in Australia is managed by several sources including the Commonwealth and the states and territories. A recent review of services suggested that lack of coordination between these funders has resulted in service gaps, duplication of services and inequalities in access.15 The most recent Closing the Gap report concluded that, despite good intentions, policy and service delivery in Aboriginal health has often been characterised by wasted opportunities and poorly targeted and evaluated initiatives.16 Likewise, the National Mental Health Commission has highlighted the inadequate response of the mental health service system to the needs of Aboriginal Australians.15 There is a fresh opportunity to more systematically improve mental health with the Australian government’s recent announcement of $85 million for Aboriginal social and emotional well-being services.17 If these funds are to result in real improvements, however, evidence on which to base decisions about policies, services and programmes is urgently required. Unfortunately, many evidence gaps remain in this area, including an understanding of which mental health interventions are and are not effective for Aboriginal young people and under what circumstances.18
To most effectively deploy limited healthcare resources with the aim of improving the mental health of Aboriginal children and adolescents, more must be known about their current mental health service use. Over-reliance on tertiary mental healthcare is regarded by the National Mental Health Commission of Australia15 and other bodies internationally19 as symptomatic of ‘system failure’, reflecting a lack of investment in effective prevention or early intervention services and programmes. In keeping with international experience, NSW has reported substantial recent increases in mental health-related emergency department (ED) presentations20–22 and hospitalisations23 24 among children and adolescents. To the best of our knowledge, however, there is no published data available about mental health-related tertiary care use among Aboriginal children and adolescents. To address this knowledge gap, we aimed to quantify mental health-related ED presentations and hospitalisations, and associated characteristics of the child and family, in a cohort of urban Aboriginal children.
Methods
Study design
Prospective cohort study including linkage to population health data.
Study setting
Four Aboriginal Community Controlled Health Services (ACCHSs) that deliver primary care. All services were located in urban or large regional centres in NSW, Australia. An ACCHS is defined as ‘a primary health care service initiated and operated by the local Aboriginal community to deliver holistic, comprehensive and culturally appropriate health care to the community that controls it (through a locally elected board of management)’.25
Patient and public involvement
SEARCH is a decade-long partnership between four ACCHS, the Aboriginal Health and Medical Research Council of New South Wales, government and healthcare providers and a multidisciplinary team of researchers. SEARCH was developed in response to Aboriginal community concerns and addresses community priorities. Representatives from partner ACCHSs have played key roles in all aspects of the SEARCH programme from determining the research questions to the development of questionnaires to the interpretation and dissemination of results. The data produced as part of SEARCH is owned by the ACCHSs and they, and the Aboriginal Health and Medical Research Council of New South Wales, have given their written permission for this paper to be published.
Mental health and social and emotional well-being have been key community priorities since SEARCH began, and we have worked in partnership to complete a range of qualitative and quantitative work in this area.8 26–29 The current study arose due to concerns among participating services that many Aboriginal children and young people were unable to access primary mental healthcare28 and that this may be worsening outcomes, sometimes resulting in severe mental health events that require tertiary care. We have worked, and are continuing to work, in partnership with the SEARCH ACCHSs to engage with relevant policy makers and health service deliverers around the results of the current study, and our mental health work more broadly, and to advocate for a collaborative approach to improving mental healthcare for Aboriginal children and young people.
Study population
The protocol for SEARCH study has been published previously.30 The aim of SEARCH is to describe and investigate the causes of health and illness among Aboriginal children living in urban and large regional centres. It was aimed at Aboriginal children aged 0–17 years who attended a participating ACCHS and their parent/caregivers.
Baseline survey data were available for 1476 children, including 1465 children who linked to the routinely collected health data sets. Analyses are based on the total sample of 1476 children with the exception of two children hospitalised for a mental health problem more than 60 times each in a period of 5–9 months (accounting for 72% of all mental health-related admissions in the cohort) who were excluded from the hospitalisation analyses because these outliers were suggestive of hospital inpatient admission beyond generally accepted parameters (eg, akin to outpatient attendance) and skewed the results. Another child with two apparently overlapping hospital stays (implying a negative risk interval) was also excluded from the hospitalisation analyses.
Children in the target population were eligible to participate in the Phase One survey provided their parent/caregivers were aged 16 years or over and were willing to provide contact information for follow-up interviews. SEARCH is conducted in partnership with four ACCHSs. According to Australian Statistical Geography Standard Remoteness Structure criteria,31 three of our partner ACCHSs are located in major cities in NSW: Mount Druitt (Aboriginal Medical Service Western Sydney), Campbelltown (Tharawal Aboriginal Corporation) and Newcastle (Awabakal Aboriginal Cooperative). The fourth is located in Wagga Wagga (Riverina Medical and Dental Aboriginal Corporation), which is a large regional area.
Ethics and consent
Families meeting inclusion criteria were invited by an Aboriginal research assistant to participate in SEARCH while visiting a participating ACCHS. Parents/caregivers were provided with a Participant Information Sheet by an Aboriginal research assistant and talked through its contents. Willing parents/caregivers were provided written informed consent form to participate in the study and to be followed up through additional data collection and data linkage, on behalf of themselves and their children. Phase One data collection for SEARCH took place from 2006 to 2012. SEARCH is currently completing 5-year follow-up.
Outcomes
ED presentations and hospital admissions with a primary mental health diagnosis
The outcomes examined in our analyses were ED presentations and hospital admissions attributed to a mental health problem. International Statistical Classification of Diseases and Related Health Problems, 10th Edition, Australian Modification (ICD-10 AM) codes used to identify mental health-related presentations and admissions were those listed in table A4.2 of Mental health services in Australia 2007−08 32 and included all codes in the range F00−F99 and selected codes from chapters VI, XV, XVIII and XXI. We defined mental health-related ED presentations to include all presentations with a principal diagnosis code in this set of ICD-10-AM codes (for EDs using ICD-10-AM codes) or an ICD-9-CM or SNOMED CT principal diagnosis code that mapped to one of these ICD-10-AM codes. Diagnosis codes were mapped using the New Zealand Ministry of Health’s ICD-10-AM to International Statistical Classification of Diseases and Related Health Problems, Ninth Edition, Clinical Modification (ICD-9-CM) map33 and the SNOMED CT to ICD-10-CM map distributed by the U. S. National Library of Medicine.33 Mental health-related hospitalisations included all hospital stays with a mental health-related principal diagnosis code recorded for the initial episode of care. All sociodemographic and health-related explanatory variables used in the analyses were derived from the SEARCH baseline questionnaire data.
Covariates
Carers completed a comprehensive survey about their children aged 4–17 years describing their physical health, development, nutritional intake and physical activity. Carers also completed a self-report questionnaire that captured information on a range of demographic, social, lifestyle and health-related factors, quality and safety of housing. Questionnaire content was based on the Western Australian Aboriginal Child Health Survey [4] and the New South Wales Child Health Survey [11], where possible.
As part of the SEARCH baseline survey, the parents or carers of participating children aged 4–17 years completed the standard Australian Strengths and Difficulties Questionnaire (SDQ) in regard to their child by interview with an Aboriginal research assistant. The total difficulties score, ranging from 0 to 40, was calculated by summing all subscales excluding prosocial behaviours.34 These scores are considered to provide an indicator of level of risk for emotional or behavioural problems. The new four-band classification system for total difficulties scores for the parent report version of the SDQ used in the current study is as follows: 0–13: ‘close to average’, 14–16: ‘slightly raised’, 17–19: ‘high’ and above 19: ‘very high’.35 For the purposes of analysis, we considered that all children with a total difficulties score below the threshold for high risk of emotional or behavioural problems (less than 17) had ‘good’ mental health.36–38 The SDQ has previously been found to be acceptable,29 reliable and valid39 among the SEARCH cohort.
Statistical methods
Questionnaire data for participating children were linked probabilistically to the NSW ED Data Collection (EDDC), the NSW Admitted Patient Data Collection (APDC), the NSW Perinatal Data Collection and NSW Registry of Births, Deaths and Marriages deaths data by the Centre for Health Record Linkage (http://www.cherel.org.au). We used the linked EDDC and APDC data for this paper. The EDDC and APDC record attendances at larger public hospital EDs (approximately 160 EDs in 2015) and all separations following admitted patient care in public and private hospitals in NSW. EDDC and APDC data were available for the periods 1 January 2005–31 March 2016 and 1 July 2001–31 March 2016, respectively. Principal diagnoses are recorded in the EDDC using International Statistical Classification of Diseases (ICD-10-AM or ICD-9-CM) or Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT) codes.40 41 Principal diagnoses and up to 50 additional diagnoses are recorded in the APDC using ICD-10-AM codes.
Children were followed from the date of recruitment until 31 March 2016. Person-years (py) of follow-up was calculated as the time (in years) from the date of recruitment to 31 March 2016 (ie, the latest date for which ED presentation and hospitalisation data were available). Age-specific and sex-specific mental health-related ED presentation and hospitalisation rates were estimated using parametric multilevel frailty models.42 We assumed a Weibull hazard function, which permits rates to increase or decrease monotonically with time (years since birth in our analyses), and lognormal frailties for both children and families (allowing for multiple presentations or hospitalisations of the same child and correlated responses within families, respectively). Separate hazard function shape parameters were specified for females and males, so the models did not rely on the proportional hazards assumption. Shape parameter estimates smaller than 1 indicate that ED presentation or hospital admission rates decrease with increasing age; values greater than 1 indicate increasing presentation or hospitalisation rates. Children were considered to be at risk of a mental health-related ED presentation or hospitalisation when they were not in hospital for a mental health problem. Adjusted rate ratios (RRs) for sociodemographic and child and carer health factors were also estimated using multilevel frailty models. A single hazard function shape parameter, applied to all levels of each explanatory variable, was specified in these models (ie, we applied the proportional hazards assumption in estimating effects for all exposures and covariates). Analyses in which separate shape parameters were estimated for females and males yielded RRs very similar to those presented here (results not shown). All models were fitted using the Markov Chain Monte Carlo (MCMC) procedure in SAS V.9.3.43 More information about the statistical methods used is noted in online supplementary file 1.
Supplemental material
Results
Study population
The mean age at recruitment into the study was 6.73 years; the median age was 5.86 years. There were no deaths recorded during the follow-up period.
Characteristics of ED presentations
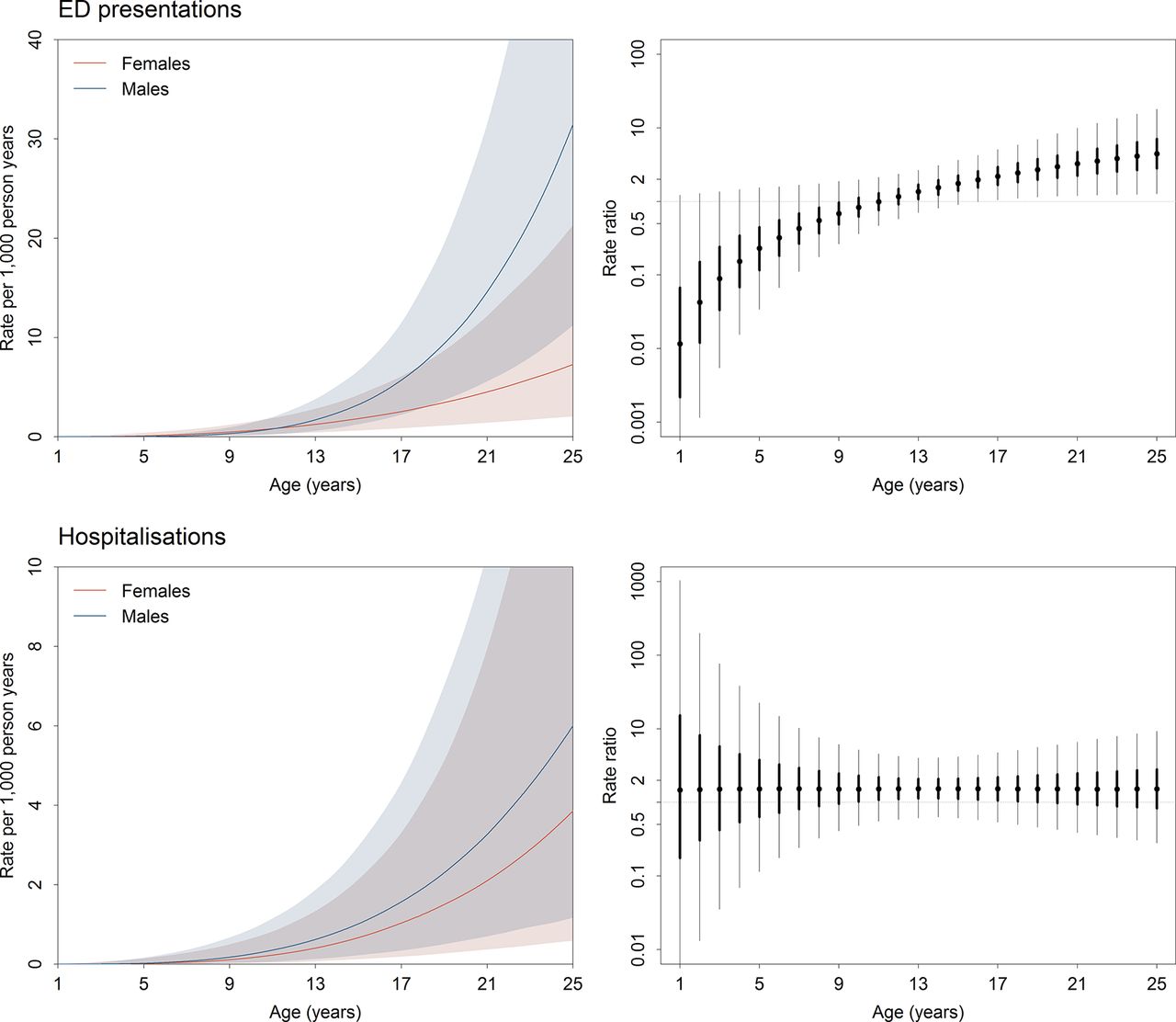
Over a median 6 years since recruitment, 96 ED presentations (10.7/1000 py) for mental health conditions occurred affecting 62 children; of these, the majority made one ED presentation (47/62, 76%) (figure 1). Mental health-related ED presentation rates increased with age (Weibull shape parameter estimates: females 3.64, 95% credible interval (CrI) 2.45 to 4.95; males 5.49, 95% CrI 4.22 to 7.00) and were significantly higher among young adult males (≥17 years) than females of the same age (figure 2). Fifty per cent of ED presentations were classified as urgent and 32% of children who presented to an ED for a mental health problem were subsequently admitted to hospital. The most common ED principal diagnoses were behavioural and emotional disorders (32/96, 33%), neurotic, stress-related and somatoform disorders (17/96, 18%) and unspecified mental disorders (17/96, 18%) (table 1).
Numbers of mental health-related emergency department presentations and hospital admissions and numbers of children presenting or admitted to hospital for a mental health problem by principal diagnosis
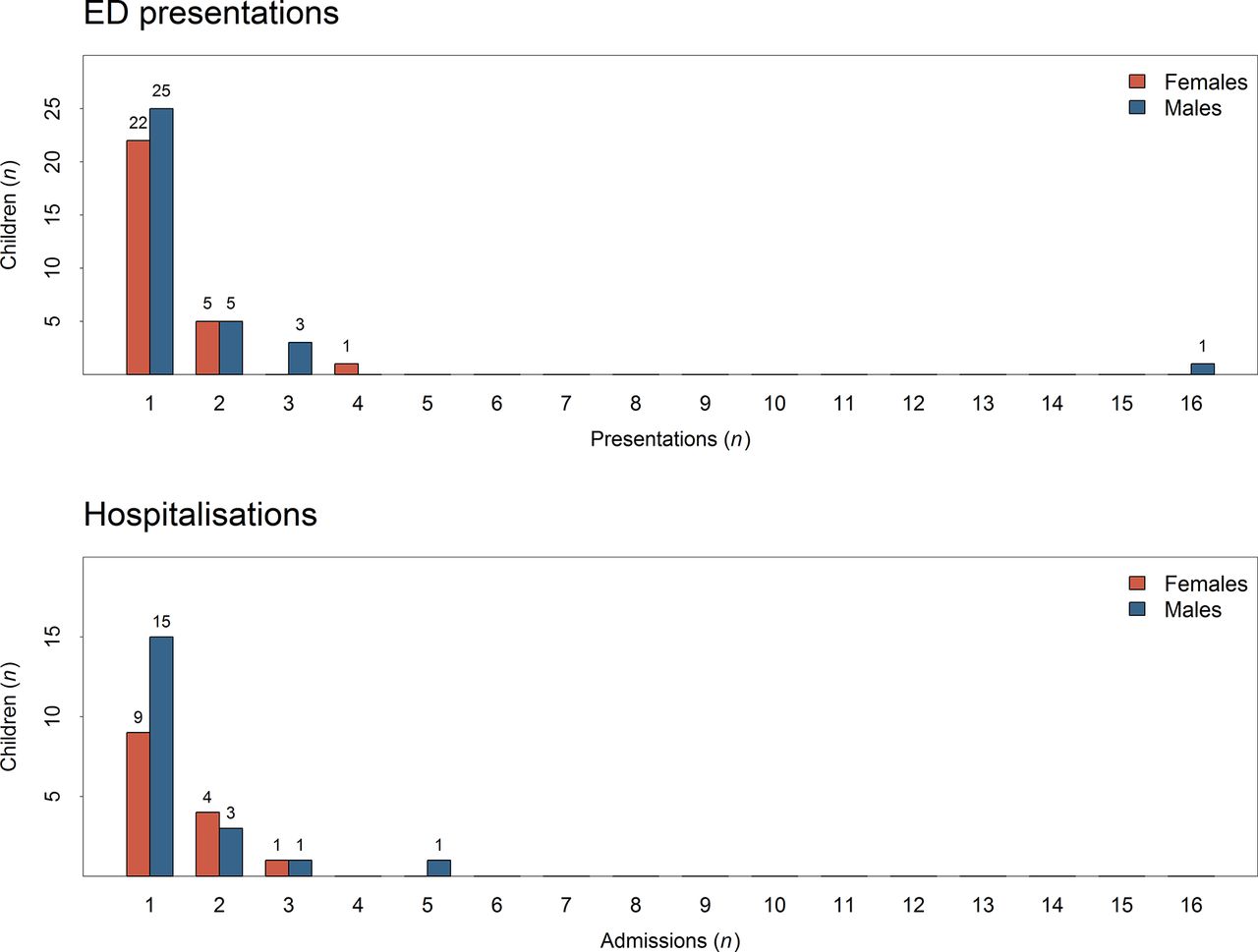
Upper panel: numbers of children presenting to an emergency department (ED) for a mental health problem. Lower panel: numbers of children hospitalised for a mental health problem.

(A): Cumulative numbers of mental health-related emergency department (ED) visits (solid lines) and numbers (divided by 10) of children under follow-up (shaded bars). (B): Cumulative numbers of mental health-related hospitalisations (solid lines) and numbers (divided by 10) of children under follow-up (shaded bars). (C): Age-specific and sex-specific rates (per 1000 person-years) of mental health-related ED presentation.
Characteristics of hospitalisations
Over a median of 6-year follow-up, there were 49 hospitalisations (5.5/1000 py) for mental health conditions among 34 children in the cohort. Among admitted children, the majority had one hospitalisation (24/34, 71%) (figure 1). Mental health-related hospitalisation rates for females and males increased with age (Weibull shape parameter estimates: females: 4.42, 95% CrI 2.66 to 6.53; males: 4.42, 95% CrI 2.98 to 6.24) and did not differ significantly between the sexes (figure 2). The median length of stay was 1 day (mean 3.1 days). The most common principal diagnoses for hospitalisation were behavioural and emotional disorders (12/49, 24%) and neurotic, stress-related and somatoform disorders (19/49, 39%) (table 1).
Factors associated with ED presentations
After adjusting for age, sex, family and recruiting health service, the following factors were associated with higher risk of ED presentation for mental health during follow-up: living in foster care versus with a parent (RR 3.97; 95% CrI 1.26 to 11.80), high risk versus low risk of emotional or behavioural problems based on baseline SDQ data (RR 2.93, 95% CrI 1.50 to 6.10) and having a carer with a self-reported a chronic medical condition versus not (RR 2.81, 95% CrI 1.31 to 6.63) (figure 3). Children whose carer reported previous treatment for mental health had double the risk of an ED presentation compared with other cohort members (RR 2.00, 95% CrI 0.93 to 4.47), although this result was not statistically significant.

Mental health-related emergency department (ED) attendance rate ratios for sociodemographic and child and carer health factors. Adjusted rate ratios are plotted with 95% and 50% credible intervals, indicated by thin and heavy error bars, respectively. Open circles indicate the reference categoy for each factor. ACCHS, Aboriginal Community Controlled Health Services; SDQ, Strengths and Difficulties Questionnaire.
Factors associated with hospitalisations
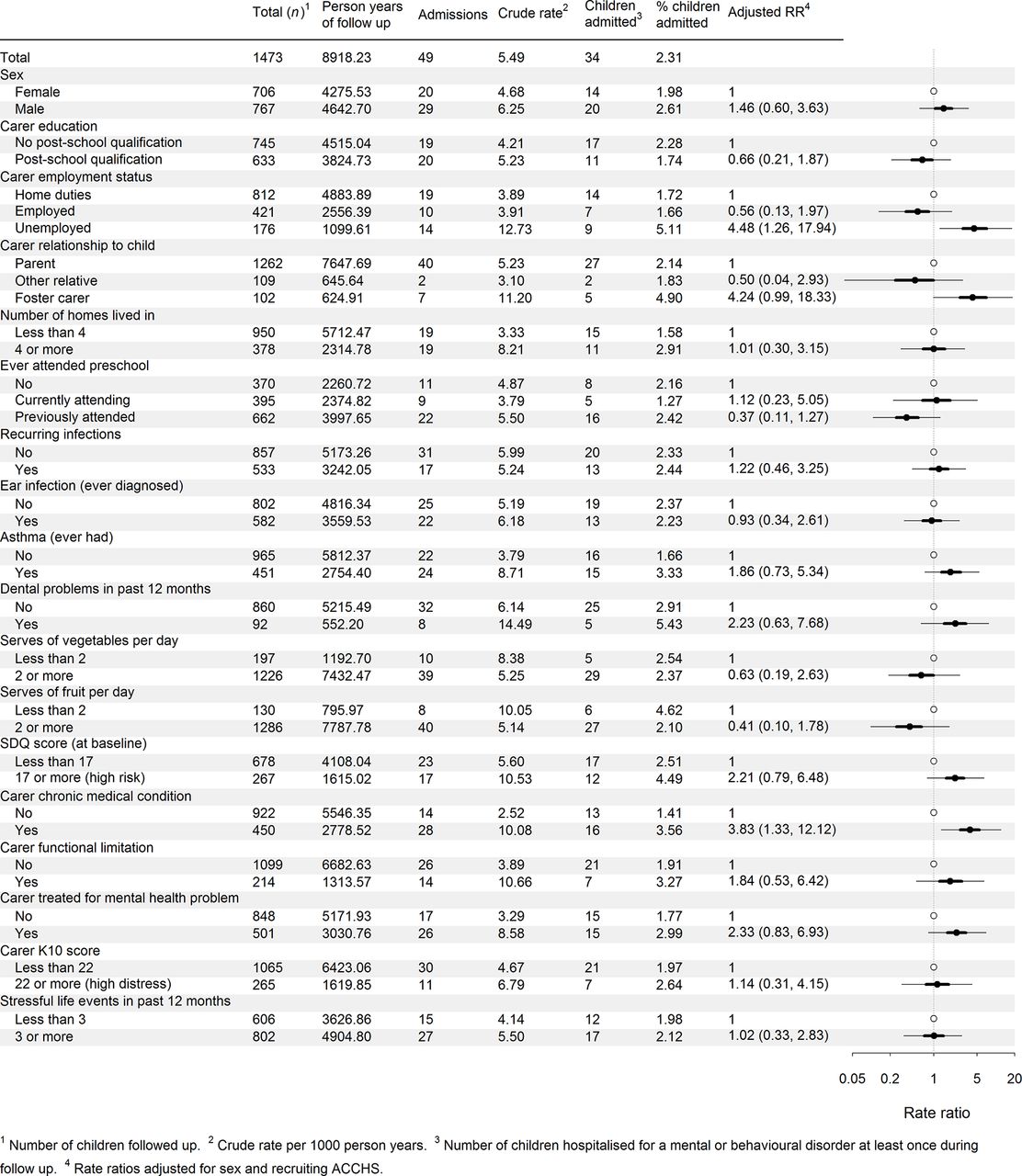
After adjusting for age, sex, family and recruiting ACCHO, the risk of mental health-related hospitalisation was significantly higher among children whose carers reported that they were unemployed at baseline versus doing home duties (stay-at-home parenting) (RR 4.48, 95% CrI 1.26 to 17.94) and whose carer self-reported a chronic medical condition compared with those who did not (RR 3.83, 95% CrI 1.33 to 12.12) (figure 4). Children living in foster care at baseline versus with a parent had a higher rate of mental health-related hospitalisation although this did not reach significance (RR 4.24, 95% CrI 0.99 to 18.33).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mental health-related hospitalisation rate ratios for sociodemographic and child and carer health factors. Adjusted rate ratios are plotted with 95% and 50% credible intervals, indicated by thin and heavy error bars, respectively. Open circles indicate the reference categoy for each factor. ACCHSs, Aboriginal Community Controlled Health Services; SDQ, Strengths and Difficulties Questionnaire.
Discussion
The current study is the first to examine the use of tertiary mental healthcare among Australian Aboriginal children and adolescents. We found that risk of using mental health-related tertiary care increased as children grew older and that early signs of emotional or behavioural problems, living in foster care and having a carer who was unemployed or had chronic health problems were also associated with increased risk of mental health-related tertiary care. Behavioural and emotional disorders, and neurotic, stress-related and somatoform disorders, were the most common reasons for mental health-related ED presentations and hospitalisations in this cohort, as in all children aged less than 18 years in NSW.24
While no precisely comparable data are available, tertiary mental healthcare appears to have been relatively common among the SEARCH cohort compared with Australian young people in general. While noting that the age range considered does not precisely align with that of SEARCH participants, the 2014–2015 rate of mental health-related admissions including specialised care was 0.5/1000 for Australians aged 0–15 years, and the rate without specialised care was 1.4 per 1000.44 Higher rates of mental health-related hospitalisations have also been noted among Indigenous compared with non-Indigenous children and young people in Canada45 and among Maori youth (15–24 years) but not children in New Zealand46 (we were unable to locate national data for Native American children and youth). Several surveys have indicated that Australian Aboriginal children are at increased risk of emotional or behavioural problems6 8 47; however, this is the first study to demonstrate that for a noteworthy proportion, these problems are severe enough to warrant tertiary mental healthcare during childhood and adolescence. Of note, baseline SDQ Total Difficulties scores were associated with risk of subsequent tertiary mental healthcare, indicating that childhood emotional and behavioural difficulties may be predictive of later mental health problems and early intervention and support may be warranted. It is also adds support to growing evidence of the validity of the SDQ instrument for Aboriginal children.27 29
It should be noted that the help-seeking process that precedes the receipt of mental health-related tertiary care for Australian Aboriginal or other Indigenous young people has not been comprehensively described and nor has perceived need for mental healthcare or the nature of unmet mental healthcare need.48 While much more information is needed, the higher rates of mental health-related tertiary care noted among Aboriginal children and adolescents may reflect a higher prevalence of mental health challenges as well as a relative lack of access to culturally appropriate primary mental healthcare.49 It is likely that there are differences in access to community-based mental health assessment and support for Aboriginal children and adolescents for each of the four participating communities, particularly between the communities based in major cities and those in inner regional areas. This has not yet been comprehensively assessed.
The majority of SEARCH children who received tertiary mental healthcare were admitted once during the median 6 years of observation. The mean length of hospital stay among those admitted to hospital was 3.1 days, substantially less than the NSW average for <18 year olds in 2002–2013 of 7.0–19.0 days, depending on the admitting unit.24 Further research is required to determine whether this shorter length of stay is consistent with patterns of inpatient mental healthcare for Aboriginal children and adolescents more broadly and, if so, what the factors driving this relatively short length of stay may be. Previous research has highlighted the inadequacies of the biomedical approach to inpatient mental healthcare for Aboriginal people50 and the discomfort many Aboriginal people report in hospital settings due to racism and a lack of cultural safety.51 52 Indeed, Aboriginal patients in NSW have been found to report lower levels of satisfaction with several aspects of hospital care.53 As is generally the case,23 24 54 rates of tertiary mental healthcare in the SEARCH cohort increased with age, reflecting a concomitant increase in the prevalence of severe mental disorders as children move through adolescence.55
While the underlying reasons for the relatively high rates of mental health related tertiary care in Aboriginal children are not known, this study indicates several potential contributors. Around 16% of SEARCH children were in non-parental care at baseline compared with 0.01% of children in Australia overall and 0.06% of Aboriginal children nationally. Children living in foster versus parental care were at greater risk of ED presentation for mental health problems; findings for hospitalisation were consistent with this but were not statistically significant. The relationship between foster care and mental health risk, using the SDQ,34 was previously demonstrated in our analysis of baseline survey data from SEARCH8 and has been noted in numerous other studies,47 56–58 as has higher use of mental health-related tertiary care among children living in foster care.59 Despite this, research suggests that many children in foster care with mental health concerns do not receive any treatment.58 60 The Royal Australian and New Zealand College of Psychiatrists has highlighted the need to ensure children in out of home care have ‘priority access to comprehensive health and developmental assessments and multidisciplinary mental health care that can address their complex health, psychosocial and developmental needs within the context of their placement and the care system’.61
Consistent with SEARCH baseline findings,8 we found that children from families with additional stressors, such as an unemployed carer or a carer with chronic physical health problems, were more likely to receive tertiary care for mental health in this longitudinal study. Previously, there has been mixed evidence of a relationship between carer employment and child mental health service use62; however, the relationship between socioeconomic disadvantage and receipt of tertiary mental healthcare54 and ED attendance and hospital admission in general63 is well established. Chronic health problems among parents have been associated with a range of additional family stressors, including financial disadvantage and reduced family cohesion,64 which are, in turn, likely to impact child mental health. Taken together, our findings suggest children in families facing additional stressors are likely to require additional services and support. While this support may include mental healthcare, it appears likely that other social and health services will also often be required. These findings accord with the views of leading Indigenous voices in this space who have underlined the importance of increasing access to the social determinants of health for Aboriginal young people and their families in order to support mental health and social and emotional well-being.10 65 66
While SEARCH is the largest cohort of urban Aboriginal children in Australia and has independent, virtually complete data on hospitalisations, like many cohort studies, it is not a representative sample. This does not lessen its appropriateness for research based on internal comparisons within the cohort or longitudinal analyses.67 In this context, greater emphasis should be placed on the relative risk estimates, indicating associations between child and family characteristics and tertiary mental healthcare, rather than the absolute rates of tertiary care. Another limitation is the small sample size and limited statistical power, which may have underidentified child and family characteristics related to the receipt of tertiary care for mental health. Any mental health condition resulting in a primary diagnosis of self-harm was not identified in these analyses as we chose to use a comparable set of mental health codes to the Australian Institute of Health and Welfare report. ED and admitted patient data are based on clinician report. We are unaware of any thorough examinations of the accuracy of these codes in regard to mental health in Australia22; however, we note that inaccuracies have been noted in other similar data sets.68 In addition, the codes applied may be influenced by both clinician and funding-related factors, particularly within the current climate of activity-based funding.68–70 Challenges related to cross-cultural assessment should also be borne in mind.29 71 72 Furthermore, we acknowledge the limitations inherent in the fact that the clinical codes reported reflect the Western biomedical model, rather than the Aboriginal concept of social and emotional well-being (which extends far beyond mental health to include connection to family and community, culture and the land).10 73 This study focuses on tertiary mental health service use in response to the concerns of our partner Aboriginal communities. Due caution regarding the accuracy and completeness of linked routinely collected data should be applied.
The National Mental Health Commission has asserted that the mental health system as it currently stands is failing Aboriginal people.15 Qualitative work suggests that while Aboriginal parents and ACCHSs staff highly value the role of family and community in supporting child and adolescent mental health, they also see a clear need for more culturally appropriate, specialist services in this area, preferably housed within trusted and culturally appropriate service providers, such as ACCHSs.28 At last count, however, 87% of Aboriginal Medical Services did not have funding for social and emotional well-being services.74 The challenges surrounding accessing primary mental health services for Aboriginal Australians are likely to be particularly acute for children and adolescents given the shortage of mental health professionals who specialise in working with young people. Unpublished data from NSW Health suggest that Child and Adolescent Mental Health Services in NSW have less than half of the recommended staff required to meet the needs of the population.75
In conclusion, Aboriginal children from four communities in urban and large regional centres in NSW appear to be accessing tertiary care for mental health at high rates. Risk of tertiary mental healthcare use was higher for those living in foster care, with prior mental health and behavioural problems and with carers with chronic illness and/or unemployment. While this study suggests high rates of serious mental health events among children from participating communities, it is unclear how generalisable these results are to other communities. Furthermore, the optimum means for reducing these rates, and the need for tertiary care, has not yet been determined. The SEARCH team is currently undertaking further research, including qualitative work, to learn more about which aspects of the local mental health service ‘system’ are working well for Aboriginal children and young people and where there are key opportunities for improvement. Such information is urgently required to inform policy and programmes to support Aboriginal child and adolescent mental health.
References
Footnotes
Contributors AW conceived of the study, contributed to its design and the interpretation of results and drafted the initial manuscript. AS was involved in study design, conducted the data analyses and was involved in drafting the manuscript. KF was involved in the data analyses and interpretation of results and in drafting the manuscript. KC was involved in the conception and design of the study and participated in the interpretation of results and in drafting the manuscript. SJE was involved in the conception and design of the study and the interpretation of results. EB was involved in the conception and design of the study, the analysis and interpretation of results and in drafting the manuscript. All authors were involved in revising the manuscript critically for important intellectual content and have given final approval of the final version of the manuscript.
Funding Study of Environment on Aboriginal Resilience and Child Health (SEARCH) is funded through the Australian National Health and Medical Research Council (grant numbers 358457, APP1035378, APP1023998 and APP1135721), an Australian Primary Health Care Research Institute Centre for Research Excellence Grant, the Rio Tinto Aboriginal Foundation and the Centre for Aboriginal Health within the NSW Department of Health. The current study is funded by a Financial Markets Foundation for Children (Australia) grant (2016-341).
Competing interests None declared.
Patient consent None declared.
Ethics approval Ethics clearance for this project has been provided by the Aboriginal Health and Medical Research Council of New South Wales (729/10), the NSW Population and Health Services Research Ethics Committee AU RED Reference: HREC/10/CIPHS/42 and the Cancer Institute NSW reference number: 2010/06/243. This paper has been approved for publication by the Board of all Aboriginal Community Controlled Health Services which are partners in SEARCH and by the Aboriginal Health and Medical Research Council of New South Wales.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All SEARCH data are owned by partner Aboriginal Community Controlled Health Services. No data are available for release without their written permission.