Article Text

Abstract
Objectives Children exposed to social adversity—hardship as a result of social circumstances such as poverty or intergenerational trauma—are at increased risk of poor outcomes across the life course. Understanding what promotes resilient outcomes is essential for the development of evidence informed intervention strategies. We conducted a systematic review to identify how child resilience is measured and what factors are associated with resilient outcomes.
Design Systematic search conducted in CINAHL, MEDLINE and PsychInfo from January 2004 to October 2018 using the keywords ‘resilien* and child* in the title or abstract. Eligible studies: (1) described children aged 5–12 years; (2) identified exposure to social adversity; (3) identified resilience; and (4) investigated factors associated with resilience.
Outcome measures (1) approaches to identifying resilience and (2) factors associated with resilient outcomes.
Results From 1979 studies retrieved, 30 studies met the inclusion criteria. Most studies were moderate to high quality, with low cultural competency. Social adversity exposures included poverty, parent loss, maltreatment and war. Only two studies used a measure of child resilience; neither was psychometrically validated. Remaining studies classified children as resilient if they showed positive outcomes (eg, mental health or academic achievement) despite adversity. A range of child, family, school and community factors were associated with resilient outcomes, with individual factors most commonly investigated. The best available evidence was for cognitive skills, emotion regulation, relationships with caregivers and academic engagement.
Conclusions While there is huge variation in the type and severity of adversity that children experience, there is some evidence that specific individual, relational and school factors are associated with resilient outcomes across a range of contexts. Such factors provide an important starting point for effective public health interventions to promote resilience and to prevent or ameliorate the immediate and long-term impacts of social adversity on children.
- community child health
- mental health
- preventive medicine
- public health
- resilience
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first systematic review summarising research about the individual, family, school, social and community factors associated with resilient outcomes in children across a broad range of social adversities including child maltreatment, war and poverty.
The synthesis was limited to a descriptive review of the studies due to the significant heterogeneity in the measurement approaches, categorisation of resilience and the resilience factors investigated.
The studies reviewed were limited to those published in English.
Background
Why is it important to understand resilience in children?
Social adversity can be defined as exposure to hardship as a result of social circumstances, for example, poverty, racial discrimination, maltreatment, intergenerational trauma or community violence. Significant numbers of children are exposed to social adversity in childhood. One in eight adults report childhood sexual abuse, one in four report physical abuse1 2 and more than one in four children are exposed to intimate partner violence.3 4 Globally, 28 million children are uprooted by war and conflict with attendant trauma, hardship and disadvantage.5 One in 10 Australians live below the internationally accepted poverty line, with almost one quarter of these being dependent children,6 and Indigenous families experience a far greater cumulative load of early life stress and social adversity, including intergenerational trauma.7 8
Experiences of social adversity have multiple direct and indirect effects on the social, mental and physical health of individuals and families.9 10 Children exposed to social adversity are more likely to experience emotional and behavioural problems, mental health disorders, speech and language problems, learning difficulties and physical disorders.4 11–15 Furthermore, childhood experiences of adversity are associated with lifelong negative impacts on health and well-being.16–20 There is also clear evidence of a clustering of social adversity, including trauma, in families and communities.1 6 10 21–23 In summary, child exposure to social adversity is common, and there is clear evidence of negative impacts for many children. At the same time, there is also evidence that some children show positive outcomes.
What is resilience?
Resilience has been defined as positive developmental outcomes in the face of adversity or stress,24 being relatively resistant to psychosocial risk experiences25 and the development of competence despite chronic stress.26 While differing in terminology, these descriptions encompass the two common factors necessary for defining resilience: first, the experience of adversity or stress, and second, the achievement of positive outcomes during or following the exposure to adversity. Current research predominantly views resilience as the process by which individuals draw on personal characteristics and resources in their environment to withstand and negotiate adversity—a dynamic process across contexts and over the life course.27 28
Resilience can be considered within an ecological framework, with risk and protective factors present within an individual; in their proximal environments of family, school or work; and at the more distal community and societal levels. A range of factors has been identified as supporting resilient outcomes in adolescence and adulthood. Individual factors such as coping style, cognition, optimism and self-esteem,29–31 positive family relationships or social connectedness30–32 and community factors such as school engagement,33 church or support groups.32 34 Most of the resilience research to date has focused on adult or adolescent resilience to trauma or other types of adversity (although the trauma may occur in childhood). There is limited research available on factors that support resilience in middle childhood (5–12 years).
Why focus on childhood?
While there have been recent systematic reviews of adult resilience factors,35 36 there is only one systematic review on child resilience and this focuses on interventions to build resilience.37 As the key developmental tasks in adolescence or adulthood differ greatly from those in childhood, there may be key differences in the factors that support resilience in children. For example, while adolescents are developing independence from family and focusing on relationships with peers, a key developmental task for children is building a close supportive bond with a caregiver. Resilience factors identified as important for adults or adolescents, such as optimism, positive family relationships and school engagement30 31 33 have obvious relevance for children, while others such as employment, church and community support may be less important. There may also be factors that are key in childhood that have not been identified in the adult literature. Exploring the factors that are associated with resilient outcomes in children is essential to improve outcomes for the millions of children experiencing poverty, violence and other social adversities.
While the data are complex, economic evaluations suggest that investment in evidence-based interventions in childhood can have significantly greater and longer lasting impacts per dollar spent, compared with intervening in adulthood.38 39 Additionally, early intervention has the potential to interrupt the intergenerational transmission of trauma and disadvantage.40 While there is huge variation in the challenges children may experience, ranging from societal factors, such as poverty, to individual exposures, such as sexual abuse, there are likely to be resilience factors that are important across different contexts and adversities. Better evidence as to what promotes resilient outcomes in children exposed to trauma or adversity is essential for effective interventions to prevent or ameliorate the immediate and lifelong impacts.41 42
Aims
The purpose of this systematic review was to identify studies that have examined resilience in children exposed to social adversity. Specifically, the objectives were to identify: (1) how resilience was assessed in research studies; and (2) the individual, family, social, school, community/neighbourhood and societal factors associated with positive outcomes or resilience in children who have experienced social adversity.
Methods
Titles and abstracts of papers identified by the search terms described below were screened by three reviewers (DG, EB and SM) against the inclusion and exclusion criteria. Papers remaining after this initial screening were imported into EndNote, and full-text articles were obtained. A more in-depth examination of the Methods section of each paper was conducted to ensure studies matched the inclusion criteria. Disagreements as to inclusion/exclusion were discussed with a fourth reviewer (ER) where necessary, with final decisions agreed by consensus.
Patient and public involvement
Patients were not involved in this study.
Inclusion criteria
Table 1 shows the study inclusion and exclusion criteria. Eligible studies were limited to research studies describing original research and written in English. Reviews, case reports, commentaries, government reports and non-peer-reviewed papers were excluded. The population of primary interest was children aged 5–12 years who had been exposed to ‘social adversity’. Social adversity was defined as exposure to trauma or hardship as a result of social circumstances, for example, poverty, racial discrimination, violence, war or maltreatment. Studies in which participants were exposed to hardship as a result of physical rather than social factors, such as natural disasters, cancer, genetic conditions or physical disability were not included. Studies that included some children outside the age range were included if enough detail was provided to ascertain that the majority of participants were aged 5–12 years. While much research has been conducted over the previous 50 years on factors associated with positive child outcomes, for example, success in school or positive coping skills, given that our focus was on child resilience, studies were required to identify or name ‘resilience’ as a focus of the investigation.
Review inclusion and exclusion criteria
The objectives of this review were twofold: (1) to identify how child resilience is identified/measured and (2) the factors associated with resilient outcomes in children. Factors were considered within the socioecological domains of individual, family, social, school and neighbourhood or community.
Search strategy
The search strategy was developed in consultation with a librarian. We searched published literature from January 2004 to October 2018. We limited the search to the previous 10 years (at the time of developing the protocol) to focus on the more recent approach to resilience research, where resilience is seen as a dynamic process rather than a static individual characteristic. Selection of electronic databases was based on the topic of our systematic review and included two general databases (MEDLINE and CINAHL) and a databases more specific to the topic area (PsychInfo). Databases were searched for articles in English with resilien* and child* in the title or abstract. Papers with genetic or only adolesce* (without child) in the title or abstract were excluded as per criteria described above. This simple approach was adopted in preference to a more complex search strategy as the significant heterogeneity in adversity exposures, child outcomes and resilience factors described in the literature meant that more complex searches missed papers we were already aware of.
Data extraction
Data were extracted using a structured data abstraction form, with the first 10% of papers independently abstracted by two reviewers, and the results were compared to ensure adherence to the protocol, check the quality of the data and check consistency in data abstraction. Data extracted included study design, country, sample size, participant characteristics (eg, age and gender), informant (eg, parent, social worker and/ or child), social adversity exposure, resilience definition/criteria, resilience measure (if included), resilience factors measured and factors associated with resilience. The quality of the included studies was appraised by one author using the Health Evidence Bulletin Wales critical appraisal tool adapted from the Critical Appraisal Skills Programme.43 This tool assesses key domains of study quality, including clarity of aims, appropriateness and rigour of design and analysis, risk of bias and relevance of results. To appraise the studies in terms of culturally safe and participatory methods, a cultural competency appraisal tool was also used.44
Results
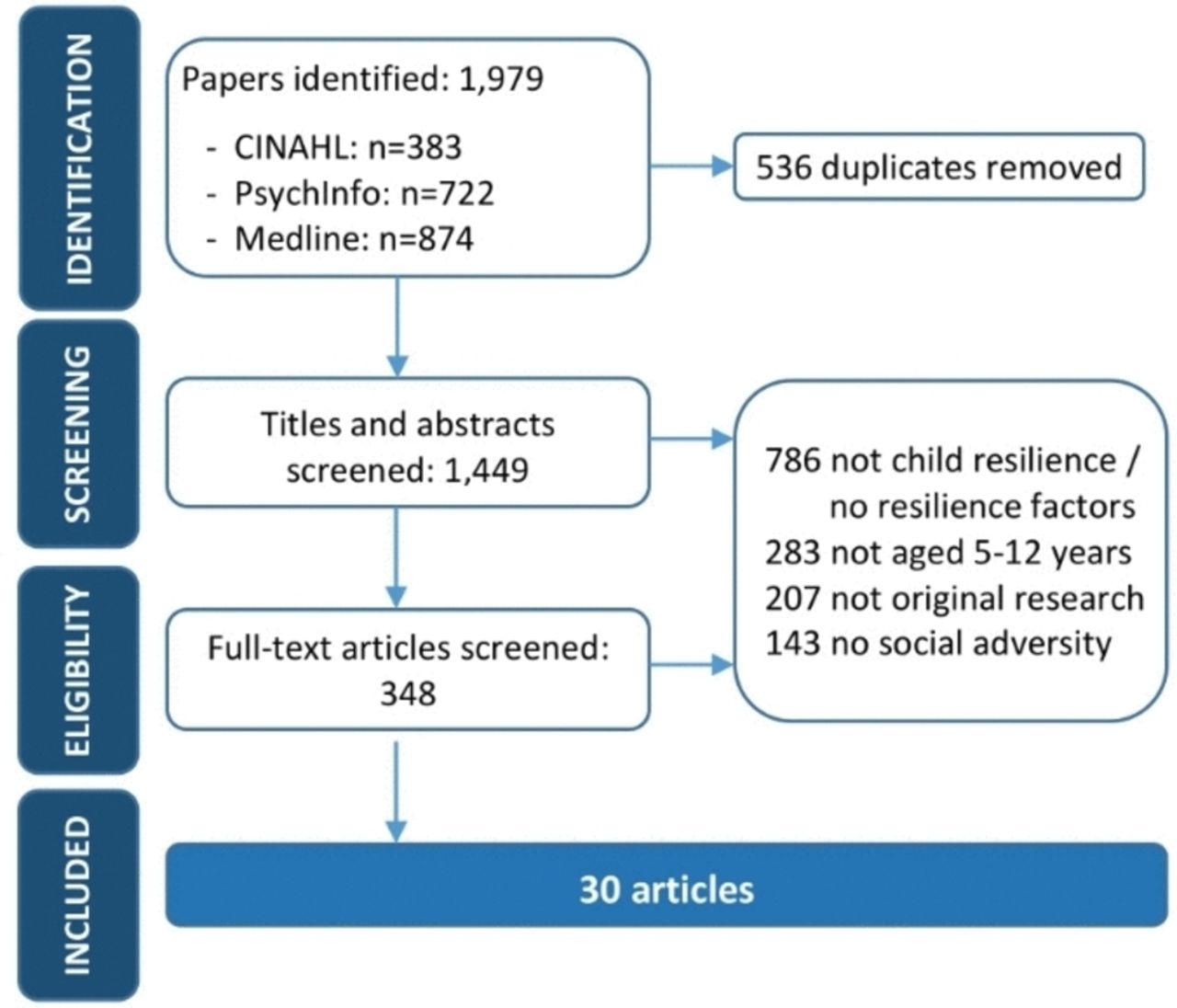
The initial search identified 1979 papers, which was reduced to 348 after initial screening of titles and abstracts (see figure 1). A further 318 studies were excluded after obtaining the full papers and examining study methods in greater detail. Papers were excluded due to: not investigating child resilience and/or factors associated with resilience (n=786); participants outside the age range or age not specified (n=283); and not an original research report. Thirty papers describing 30 studies met the inclusion criteria.

{kind=link}
Flow chart of paper selection.
Table 1 provides details of the 30 included studies conducted from 2004 to 2017. The majority of studies was conducted in North America (n=20, 67%). The remaining studies were conducted in Africa (2), Asia (3), Australia (1) and Europe (4). Participants ranged in age from 2 years to 16 years (n=26 studies), with the mean age ranging from 4.5 years to 11.9 years (n=19 studies). Twelve studies (40%) were prospective longitudinal cohort studies and 18 were cross-sectional studies (60%). Two studies (7%) included qualitative methods.
The most common social adversity described was poverty (n=14, 47%) (see Table 2). Belonging to a minority population group, such as an ethnic minority, is associated with a higher risk of social disadvantage and adversity across the life course.9 40 45 46 Seven studies reported that participants belonged to an ethnic minority (23%), with six of these seven studies also identifying poverty as an adversity exposure. The seventh study was an examination of cross-ethnic friendships in South Asian British children in the context of perceived ethnic discrimination.47 None of the included studies separately identified Indigenous or refugee children, although Cortina et al48 examined refugee status as a risk factor for children living in rural Southern Africa.
Summary of reviewed papers (n=30)
Seven studies described children who had been abused or neglected (23%) and four (13%) described children exposed to violence (including intimate partner violence, community or school violence). Eight studies described children with interruptions in the caregiving relationship: five (17%) were about parental loss or illness (HIV, mental illness, incarceration or death) and three reported on children in out-of-home care (10%). One study described children living in a war-affected zone (3%).
Critical appraisal of the included studies using the Health Evidence Bulletin Wales critical appraisal tool determined that the majority of the studies were of high quality (see online supplementary table 1a). In terms of culturally safe and participatory study methods,44 most of the included studies were of low quality, with only one study—investigating resilience in South African children48—classified as high quality (see online supplementary table 1b).
Supplementary file 1
Measuring resilience in middle childhood
Two studies (7%) used a resilience measure. Bagci et al47 used a brief resilience scale developed by Bartko and Eccles49 to assess resilience in 247 South Asian British children. The scale was originally developed for American adolescents and asks respondents ‘How often are you very good at’ on four items related to problem solving, planning, bouncing back from bad experiences and learning from mistakes. Bagci et al47 report a relatively low scale reliability of 0.6. No other psychometric properties were reported.
Somchit and Sriyapor50 report using a resilience framework developed by Grotberg to develop a resilience measure to examine perceptions of adversity and academic achievement in 267 Thai children. The paper provides no information about the properties of the newly developed measure, and it is unclear how Grotberg’s resilience framework was operationalised. There is no information included in the paper about the items, scales or psychometric properties of the measure.
The remaining 28 studies classified children as resilient by specifying positive outcomes on one or more measures of mental health (eg, internalising problems or life satisfaction) or functioning (eg, cognitive outcomes, academic achievement or social behaviours) in the context of exposure to adversity or trauma. Of the 12 longitudinal cohort studies, all studies used positive functioning in a single domain to define resilience. Six studies used a measure of positive mental health to classify children as resilient (see table 2), four identified an aspect of child behaviour (eg, low levels of antisocial behaviour) and two used an academic measure (eg, positive classroom behaviour and academic performance). Lagasse et al51 used positive outcomes across both social and mental health domains but investigated each separately (ie, resilience was not having a mental illness diagnosis or lower levels of delinquent behaviour rather than a composite of a positive outcome in both areas).
There was considerable variation in the approaches used to define resilience. For example, Halevi et al52 classified Israeli war-exposed children as resilient if they exhibited a lack of psychopathology on the Development and Well-Being Assessment. Brown et al53 used latent growth curve analysis of poor black American students’ internalising symptoms over time and classified students who exhibited stable low level internalising symptoms as resilient. While both studies used mental health to identify children as resilient, they employed very different measures and approaches. Across all 30 studies, the measures used and the methodological approach to identifying children as resilient or non-resilient/vulnerable varied greatly.
In the 18 cross-sectional studies, three studies identified resilience using a composite of positive child outcomes across more than one domain, for example, mental health and social competence.54–56 Lin et al57 used a composite of three outcome measures but all were within the domain of mental health (below clinical cut-off for depression, anxiety and internalising/externalising problems). The remaining studies used a positive child outcome in a single domain of mental, behavioural or academic outcomes to identify resilience in children exposed to adversity (see table 2). Overall, no two papers employed the same method to identify children as resilient.
What factors are associated with resilient outcomes?
In addition to examining the way in which studies identified resilience in children, we also abstracted information on factors associated with resilient outcomes. Table 3 summarises the included studies according to a single primary social adversity to avoid artificially inflating results and the factors that were identified as significantly associated with child resilience. The factors investigated in each study have been grouped into the domains of individual, family, social, school and neighbourhood/community. Each domain will be described in turn.
Individual factors
Individual characteristics were identified as significantly associated with resilient outcomes in all social adversity contexts. Most studies included individual characteristics (n=24, 80%). A wide range of factors was investigated including gender, temperament, emotion regulation, cognitive skills, social skills, self-efficacy and self-esteem (see table 3). Five longitudinal studies identified a significant association between an aspect of cognition and resilient outcomes in the different adversity exposures. For example, in a large study of child emotional and behavioural resilience in the context of persistent poverty, verbal cognitive ability was found to be significantly associated with low levels of child internalising problems.58 Brown et al53 found moderate support for an association between cognitive abilities and stable low internalising problems over time in a large longitudinal cohort of 1603 boys living in poverty (and belonging to an ethnic minority). Jaffee et al59 reported that maltreated boys with above average intelligence had a significantly higher likelihood of being in the resilient group; however this association was not evident for girls (resilience was defined as antisocial behaviour scores at or below the median of the non-maltreated group).
Significant resilience factors (grouped into themes) in the individual, family, social, school and community domains by primary adversity exposure*
Eight studies identified associations between self-regulation and resilience: three longitudinal cohort studies, four cross-sectional and one qualitative study. Self-regulation refers to purposeful modulation of thoughts, emotions or behaviour or ‘effortful regulation of the self by the self’.58 Although Flouri et al58 found that self-regulation benefited both poor and non-poor children, there was an increasing gap in outcomes over time between the poor children with high and low regulation, particularly in terms of internalising problems. The trajectories of internalising and externalising problems of poor and non-poor children with high self-regulation were similar, particularly as they got older.58 Borman and Overman60 in a cross-sectional study of 925 low SES third grade students purposively selected from a longitudinal cohort found a higher internal locus of control to be associated with resilient outcomes (as defined by performing better than expected in maths), irrespective of minority status. Emotion regulation also predicted group membership of low rather than high bullying in 61 children attending a summer camp for children of incarcerated mothers.61
Two papers reported aspects of self-esteem to be significantly associated with resilient outcomes. Anthony62 identified four distinct clusters among 157 ethnically diverse children living in public housing in the USA. High levels of self-esteem and coping skills (among other factors) were found among children in the first cluster, who were found to be resilient in terms of low drug use and delinquency and better academic grades. A large longitudinal study of ethnically diverse children living in rural Texas similarly found that children with a self-perception of competence were less likely to engage in health risk behaviours (ie, smoking cigarettes, using marijuana, drinking alcohol or carrying a weapon).63
As shown in table 2, a range of other child characteristics was associated with resilient outcomes in one or two studies including prosocial skills,64 coping skills,57 65 hope,66 daily living skills,67 help seeking68 and empathy.69
Family and social support factors
Sixteen studies examined aspects of caregiver relationships, family environment and/or parenting skills across all the social adversity contexts, with significant factors identified in all contexts. For example, support from family was associated with significantly lower engagement in health risk behaviours in a sample of almost 2000 ethnically diverse children living in poverty in rural Texas.63 In a mixed methods study, feeling loved, cared for and supported by their caregivers was significantly associated with emotional health for 20 children who were in the full time care of their grandparents.65 For 219 children who had been exposed to intimate partner violence in the previous year, parenting warmth was one of the factors that significantly differentiated resilient children from those with severe problems.56
Fewer studies (n=11) investigated social factors associated with resilient outcomes across the different adversity contexts. Broader social support from friends or adults outside the family was identified as significant in the face of poverty, child abuse, violence and parental absence/loss. For example, in a longitudinal cohort of 517 children aged 11 years who had been exposed to violence (child abuse, family violence, violent friends and/or community violence), the authors reported that children who had positive ‘relatedness to others’ scores (a composite of positive relationships and prosocial behaviour with teachers, parents, friends and peers) were more resilient in terms of experiencing less school-specific delinquency (truancy or suspension), depression, oppositional defiance disorder and conduct disorder.51 Furthermore, in a cross-sectional study, the ability to form a positive relationship with an adult figure outside of the immediate family predicted resilience in maltreated Latino children.55 Finally, investigation of the benefits of cross-ethnic friendships in 247 South Asian British children identified that friendship quality, but not the number of friends, was associated with psychological well-being and resilient outcomes.47
School factors
School factors were investigated in two contexts only: five studies in the context of poverty and one study in the context of parental loss/illness. School factors included both student characteristics, such as academic engagement, and school environment factors. Student academic engagement was reported to mediate the association between risk experiences (a count that included child maltreatment, low maternal education at birth, homeless shelter stay, poor prenatal care, preterm birth/low birth weight and lead exposure) and both reading and mathematics outcomes in a cross-sectional study involving almost 4000 third grade African-American boys.33 For ethnically diverse children living in public housing developments in the USA, school commitment was significantly associated with resilient outcomes in terms of lower delinquency and drug use and better school grades.62 A single study investigated parental loss and reported that academic performance was not significantly associated with resilient outcomes (lower levels of emotional and/or behavioural problems) in a sample of 531 children living in out-of-home care.70
In relation to aspects of the school environment, a large cross-sectional study of 925 students living in poverty examined the school characteristics for resilient (above expected mathematics achievement) versus non-resilient students (below expected mathematics achievement).60 The authors reported few differences for school resources (eg, class sizes) or effective school environment (eg, strong principal leadership) but did find significant differences with respect to supportive school community. Resilient students were significantly more likely to come from schools with positive student–teacher relationships, a safe and orderly environment and that were supportive of family involvement.
Community factors
Eight studies explored community factors associated with resilient outcomes, seven of which identified significant associations between diverse aspects of community or culture. For example, in a large longitudinal cohort study of children living in relatively high crime neighbourhoods, those children who lived in communities with high social cohesion and informal social control were more likely to be resilient to maltreatment.59 Perceived community support was associated with life satisfaction in a sample of 75 children living in poverty in Hong Kong.66 Finally, spirituality was associated with resilience in a qualitative study involving institutionalised African children and African-American children living in a high crime, high poverty area in Texas.68 71 However, in one longitudinal prospective cohort study, family religiosity was associated with higher levels of internalising symptoms for Puerto Rican children.72
Discussion
While there is a growing body of resilience research, to date, there has been a limited focus on child resilience in the context of social adversity and disadvantage, especially among children aged 5–12 years. Of the 30 studies included in this systematic review, only two employed a structured measure of resilience and neither of these measures was validated. Most studies relied on categorisation to identify resilience (exposure to adversity+positive achievement in a particular outcome=resilience). Across the 28 studies using this approach, there was significant variation in outcome measurement and how children were classified as resilient/non-resilient. These findings are consistent with a recent systematic review of the operationalisation of resilience in longitudinal studies by Cosco et al.35 The authors comment that the considerable ‘heterogeneity in adversity/adaptation dyads and operationalisation methods’ (p. 5) meant they were unable to meaningfully review the actual protective factors investigated in the studies they reviewed. This existing variation in the identification of resilience makes comparisons across studies, populations and contexts problematic. The adoption of a more consistent approach to defining and measuring child resilience would enhance our understanding of resilience across different contexts and improve our ability to examine the effectiveness of interventions.26 35 41 73 74
Most of the included studies identified child resilience by measuring positive outcomes in a single domain, such as mental health. Resilience is a multidimensional construct that may vary across domains.26 73–75 Positive outcomes in a single domain may mask negative outcomes in other areas, and conversely, while adversity and trauma will impact the mental health of all exposed children to some degree, they may exhibit resilience in other domains such as academic or behavioural. Therefore, the identification of factors associated with resilience based on a single domain may not be generalisable to other domains or settings.
These limitations aside, there appears to be a range of factors that may contribute to resilience in children across different social ecological domains. At an individual level, factors such as emotion regulation, cognitive skills, empathy or a positive outlook have been associated with resilient outcomes. In the family and social domains, good relationships with caregivers and positive parenting approaches appear key, but this is also the case for social support from friends or other adults. There was less evidence available for school factors associated with resilient outcomes for children. A safe and orderly school environment, positive relationships with teachers and student academic engagement appear to be associated with resilient outcomes in the context of poverty. Few studies addressed community factors, but community cohesion and links with cultural identity, including spiritual beliefs, also appear to be associated with resilience in children.
As noted above, there was significant heterogeneity in the measurement approaches, categorisation of resilience and the resilience factors investigated in the reviewed literature. This meant we were not able to summarise the papers quantitatively to compare effect sizes for variables associated with resilient outcomes using meta-analyses. Limitations of this review include the breadth of resilience research, which required the exclusion of a large number of papers after a brief review. In hindsight, some relevant papers may have been missed due to the databases chosen—a recent paper by Bramer et al76 suggests that a combination of Embase, MEDLINE, Web of Science Core Collection and Google Scholar performs best for systematic reviews. We did not have sufficient funding to include papers published in languages other than English. The studies on the whole were moderate to high quality; however, many scored poorly in terms of employing culturally safe and participatory study methods. This may introduce bias in our understanding of the resilience factors that are important for children from migrant or minority backgrounds. None of the included studies reported data for Indigenous or refugee children. This may be because these children did not participate or were not identified separately in the included studies. Given the greater burden of childhood trauma and social adversity experienced by Indigenous77 78 and refugee children,79 this is a major gap in the literature.
The review findings provide a starting point for focusing research efforts on a broader conceptualisation of resilience that includes individual factors and factors in the socioecological context surrounding the child. Developmentally, this broader understanding of resilience is particularly important for children, who have a limited capacity to shape their world compared with adolescents and adults. It also highlights aspects of resilience that will be important to consider when attempting to improve child resilience in clinical or educational settings. Two recent systematic reviews conducting meta analyses of resilience interventions, one focused on adults and one on school-based interventions, concluded that resilience interventions, particularly those including cognitive behavioural therapy, appeared to be beneficial, at least in the short term.37 80 However, considerable heterogeneity across studies, weak methodologies, lack of longitudinal data and small sample sizes were among the limitations noted. Given the breadth of factors identified as contributing to child resilience in the current review, it appears likely that resilience interventions will be most effective where both individual and broader relevant socioecological aspects are addressed and multilevel approaches are taken.37 41 81 82
It is imperative to investigate resilience and develop interventions to build child resilience in a way that embraces more vulnerable, harder-to-reach populations, often not captured using standard research methods. It is also vital that all the relevant domains of resilience including self, family, school, social and neighbourhood/community strengths are incorporated. The development of a measure of child resilience factors that is relevant and appropriate for children who are more vulnerable to disadvantage and social adversity will have several advantages. It will support consistency across studies and contexts and the development and evaluation of intervention programmes, and it will improve assessment of child outcomes in clinical, research and educational settings for families.
While there is huge variation in the type and severity of adversity that children may experience, there are a number of resilience factors associated with positive child outcomes across different contexts and exposures. Such factors provide an important starting point for effective public health interventions to promote resilience and to prevent or ameliorate the immediate and long-term impacts of social adversity on children.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.
- 84.
Footnotes
Contributors DG, ER, SM, RG and SJB devised the search protocol; EB, DG, ER and SM executed the protocol; SM and ER completed the critical appraisal; DG conducted the analysis and wrote the paper with input from RG, TOA, HM, HH and SJB. All authors have contributed to and approved the final manuscript.
Funding Funding for this study was provided by the Australian National Health and Medical Research Council Project Grant (#1064061) and Myer Family Foundation philanthropic funding. Murdoch Children’s Research institute is supported by the Victorian Government’s Operational Infrastructure programme. HM is supported by the Chedoke Health Chair in Psychiatry. TOA is supported by a Canadian Institutes of Health Research (CIHR) New Investigator Award and a CIHR Foundations Grant. SJB is supported by a NHMRC Research Fellowship. RG is supported by a NHMRC Career Development Fellowship.
Disclaimer The funding bodies had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript or the decision to submit the paper for publication.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The full results of the quality appraisal are available upon request.
Patient consent for publication Not required.