Article Text

Abstract
Objective To explore whether a preconsultation web-based intervention enables patients with diabetes to articulate their agenda in a consultation in the hospital outpatient clinic with their diabetologist.
Methods and design A qualitative study embedded in a pragmatic pilot randomised controlled trial.
Setting Two city outpatient departments in England.
Participants 25 patients attending a follow-up consultation and 6 diabetologists.
Intervention The PACE-D, a web-based tool adapted for patients with diabetes to use before their consultation to generate an agenda of topics to discuss with their diabetologist.
Data collection 25 participants had their consultation with their diabetologist audio-recorded: 12 in the control arm and 13 in the intervention arm; 12 of the latter also had their PACE-D intervention session and a consultation recorded. Semi-structured interviews with 6 diabetologists, and 12 patients (6 in the intervention group and 6 in the control group).
Analysis Thematic discourse analysis undertaken with patient representatives trained in qualitative data analysis techniques.
Results We identified four consultation types: diabetologist facilitated; patient identified; consultant facilitated and patient initiated and patient ignored. We also identified three critical aspects that explained the production and utilisation of the agenda form: existing consultative style; orientation to the use of the intervention and impact on the consultation. Where patients and diabetologists have a shared preference for a consultant-led or patient-led consultation, the intervention augments effective communication and shared decision making. However, where preferences diverge (eg, there is a mismatch in patients' and diabetologists' preferences and orientations), the intervention does not improve the potential for shared decision making.
Conclusion A simple web-based intervention facilitates the articulation of patients’ unvoiced agenda for a consultation with their diabetologist, but only when pre-existing consultation styles and orientations already favour shared decision making. More needs to be done to translate patient empowerment in the consultation setting into genuine self-efficacy.
Trial registration number ISRCTN75070242.
- health services research
- patient centred medicine
- qualitative research
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Patients were involved at all stages of the development of the intervention and its evaluation.
This qualitative study sampled patients and clinicians who had participated in both arms of a randomised controlled trial of an intervention conducted at two hospital sites.
A strength of the study is the use of multiple sources of qualitative data, collected from preconsultation intervention sessions, patient-diabetologist consultations, agenda forms and postconsultation interviews.
A limitation was the number of participants recruited to the trial, which limited the sampling available for the qualitative study.
Introduction
By 2045, 693 million people (aged 18–99 years) worldwide will have diabetes, with global healthcare expenditure for diabetes expected to increase by 7% from 2017 to US$958 billion.1 Diabetic complications are associated with substantial long-term healthcare costs, now rising steadily over time.2 Diabetes is largely monitored and managed by patients themselves.3 Self-management involves complex self-care tasks, which may place a burden on those with diabetes, which can inhibit effective self-care.4 Advice from professionals is vital to self-management, improving patients’ ability to cope with their illness.5 Effective consultations are associated with empowerment, positive behaviour change and improved diabetes outcomes.6–8 However, there is a lack of consensus among clinicians about the format of diabetes reviews9 and patients’ concerns are often overlooked.10 11 Thus, methods to improve the quality of consultations in terms of the ability of the patient to discuss their concerns, understand information and remember and follow advice are consistently sought.
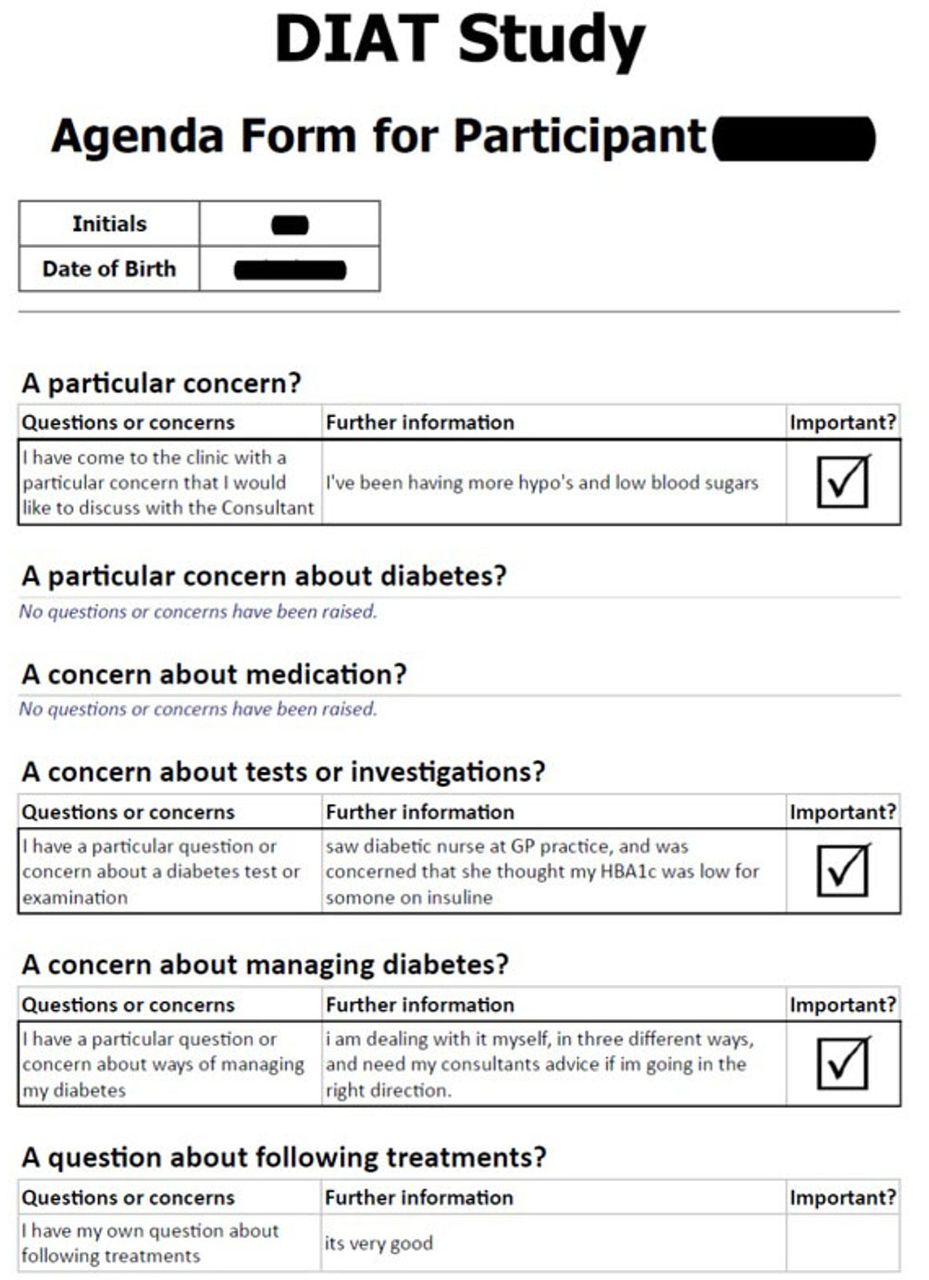
Methods used to improve consultations include question checklists and patient coaching delivered immediately before consultations. Information-seeking behaviour and patient satisfaction are most improved by combining coaching with written material.12 A systematic review of computer-based self-management interventions for adults with type 2 diabetes identified 16 randomised controlled trials, but was unable to discern the active ingredients or optimal ‘dose’ of the interventions.13 Previously, Greenfield et al used a medical record review, a treatment algorithm and a behaviour change strategy, to improve both patient participation in the consultation and glycaemic control.14 Subsequently, Cegala et al have suggested that communication skills training for patients can enhance their participation in the medical consultation.15 They have proposed the Presenting Asking Checking Expressing (PACE) system for patients to develop effective communication; this involves patients presenting detailed information about how they are feeling, asking questions if desired information is not provided, checking understanding of information that is given to them and expressing any concerns about the recommended treatment. We modified the PACE system specifically for diabetes to produce a web-based tool (PACE-diabetes or PACE-D), designed to be completed by a patient immediately before a clinic appointment with a diabetologist to identify the issues that they wish to discuss with them (ie, their ‘agenda’—figure 1 16 17 and online supplementary file).
Supplementary file 1

{kind=link}
Agenda form for Mrs Edwards.
The aim of this paper is to explore whether a preconsultation web-based intervention enables patients to articulate their agenda in a consultation with their diabetologist.
Methods
Design
A qualitative study embedded in a pragmatic pilot randomised controlled trial.16
Participants and study setting
For the trial, we aimed to recruit 120 patients attending diabetes clinics at two outpatient departments in England. Eligible patients were adults with type 1 or type 2 diabetes who were due to attend outpatient appointments with their diabetologist. Participants were aged 18 years or over with basic spoken or written English, necessary to complete the outcome measures. Pregnant women with diabetes and patients with diabetes receiving insulin pump therapy were excluded as they attended separate designated clinics for those conditions.
Recruitment
Potential participants were identified from clinic lists of participating consultant diabetologists by a research nurse at each location. Those who expressed an interest were sent a Patient Information Sheet, and telephoned a week later by a research nurse who established their willingness to participate, and sent them a Consent Form and baseline questionnaires. On receipt of these documents, participants were randomised to either the intervention or usual care. Because patients were added to the clinic list later than anticipated, with ethical approval this process was condensed to facilitate recruitment.17
Intervention
In a 20 min session immediately preceding the clinic appointment, a trained healthcare assistant (HCA) assisted the patient to complete the web-based form (figure 1).
The patients in the intervention arm proceeded to the clinical consultation with the printout of their intervention form which they handed to the diabetologist, and which then acted as an agenda for their consultation. Due to the nature of the intervention and the production of an agenda, it was impossible to blind health professionals or patients to trial allocation.
Control
This comprised usual clinical care provided by the same diabetologists in outpatient clinics.
Data collection
We planned to audio-record 10 intervention sessions, to explore how patients used the web-based intervention and the amount of assistance that they required from the HCA. We also planned to audio-record 30 clinical consultations across both trial arms and study sites, to understand the mechanisms that underlie the impact of the production of an agenda on the clinical consultation, and its subsequent utilisation in practice, when compared with usual care.18 19 As patients, rather than diabetologists were randomised, we sought to explore the impact on diabetologists’ conduct, by comparing ‘naturally occurring’ data for consultations with patients in the control arm (to establish the natural ecology of conversations), and research generated data (from use of the agenda form in the intervention arm) for each diabetologist.20 21
We also aimed to conduct semi-structured interviews with a purposive sample of 5 clinical staff and 10 patients in each trial arm to explore wider organisational factors. All data were transcribed and anonymised, and managed using Nvivo software.
Analysis
Data analysis began with a preliminary charting exercise (JF, CA), first of consultations from the control arm and subsequently for those in the intervention arm, which allowed us to typify usual care and subsequently to identify any relationships between the process of agenda identification and agenda use.22 From the charting exercise, we identified a preliminary typology of consultations (patient ignored, consultant led, patient led, consultant and patient led). AG, NB and JF then trained a group of four patient and public involvement (PPI) representatives, including the two PPI co-applicants (see below), in qualitative data analysis techniques.23 The PPI group developed the preliminary typology—identifying the terms ‘patient identified’ (rather than ‘patient led’) and ‘diabetologist facilitated’ (rather than ‘consultant led’) as more nuanced. For example, a consultation was defined as patient initiated and diabetologist facilitated, when the doctor brought his agenda into play but he interweaved it into the patient’s agenda. These discussions were incorporated into a coding manual that defined each of the four categories, and which was used to further analyse the data and develop display matrices for each category (JF, LM).24 Both coders independently coded the dataset on the basis of those categories, and the small number of disagreements were resolved by discussion (eg, revisiting the discussions with the PPI group). By applying this typology to the whole dataset, including the agenda forms, field notes and interviews with patients and physicians, we sought to identify explanatory factors which mediated the production and utilisation of an agenda form. Completed matrices for the whole dataset were then discussed again with the PPI group, who confirmed the analyses.
Patient and public involvement
Patients identified the research question and were involved in the design and conduct of the research and dissemination of findings.16 With patient input, a project team was convened and a scoping exercise undertaken to assess what is known about the problem. Two patient representatives who have diabetes joined the research team as co-applicants on this proposal. Supported by a designated PPI research fellow (AG), these patient co-applicants were members of the project management team, who co-wrote the study documentation (including Patient Information Sheets and interview guides), assisted with training the HCAs, and participated in the data analysis.25 A further group of eight people with diabetes provided feedback on a prototype of the intervention.
Results
Fifteen diabetologists working at the two centres were approached. Nine consented to participate and were formally inducted to the study in terms of the use of the agenda form, ethical practice and trial procedures. Patients were screened for eligibility (n=395). Of those who were eligible for the trial (n=380), 71 were recruited to the study, with 38 participants randomised to the intervention arm and 33 to the control arm (table 1). Participants were similar to eligible non-participants with respect to mean (SD) age at registration (56.5 (12.4) vs 51.3 (16.1)), type 1 (as opposed to type 2) diabetes status (66.2% vs 60.5%) and whether attending for a new appointment (4.2% vs 8.1%). With consent, 25 participants had their consultation with their diabetologist audio-recorded: 12 in the control arm and 13 in the intervention arm. Twelve of the latter had both their intervention session and consultation recorded. JF, an experienced qualitative researcher, then conducted semi-structured interviews with a purposive sample of 6 diabetologists, and 12 patients (6 in each trial arm) to contextualise our understanding. Patient interviews were conducted at their homes while all diabetologists except one were interviewed in the clinic. Interviews lasted between 20 and 60 min, and JF made field notes afterwards. All participants and clinics were given pseudonyms in line with in line with the principles of the Declaration of Helsinki,26 and the International Conference on Harmonisation-Good Clinical Practice.27
Patient characteristics
Applying the PPI groups’ typology to the wider dataset enabled us to identify the key aspects that explained the production and utilisation of an agenda form: existing consultative style; orientation to the use of an agenda form and, ultimately, the impact on the consultation.
Existing consultative style
In the control group we were able to identify each diabetologists’ usual style for eliciting information. For some this involved checking each medication and whether routine screening has been undertaken rather than asking patients about their concerns, while for others an open question was sufficient to set the tone of the consultation:
So can I start by double checking some stuff with you, is that all right? And we’ll get on to what you want. (Mrs Brown, 49 years/Dr Smith, Parkview, control group consultation)
How do you think things are? I mean, have you had any particular problems over the last month or two, or do you think it’s fairly stable and under reasonable control? (Mr Wilson, 79 years/Dr Jones, Parkview, control group consultation)
Unsurprisingly, this continuum is evident in the intervention group, with some diabetologists using their existing script prior to facilitating use of the agenda form, while others use the agenda form instead of their usual open questioning:
So you very kindly agreed to take part in the study…Fantastic. And you’ve gone through that (Agenda) before, and we’re going to be using this as the basis for the consult today… (Miss Roberts, 52 years/Dr Smith, Parkview intervention group consultation)
We found no evidence of contamination between consultations in the intervention arm and the control arm (ie, there were no examples of physicians changing what they did in usual practice as a result of participating in the trial). Rather, we identified that the diabetologists’ consultative style endured despite the use of an agenda form, with the agenda form acting as a magnifier of existing consultative style rather than as a mediator.
Patient experiences of participating in a diabetes consultation varied considerably. In some consultations, we were able to discern much that is literally unsaid or shorthand, where both parties knew the broader context, due to their ongoing relationship:
I’ve known her now for well over twenty years, and she has been nothing but nice, and stern if I’ve been naughty, you know, which is fair enough…And what it does, it makes me more enthusiastic to look after my diabetes. I go away feeling better and saying ‘Well, I must improve on that and must do this’. Be nice if she could do it every fortnight that would be even better! (Mrs Johnson, 70 years, Moorland, control group interview)
In other consultations, agenda items were discussed at length, with the diabetologist using this as an opportunity to educate, inform or reassure their patients. Where people with diabetes and their diabetologist have a positive pre-existing relationship and share the same orientation to decision making (eg, both have a preference for either the diabetologist or the patient leading the consultation), the agenda form augments existing relationships and mutual information sharing styles:
She’s always interested in my view and respects my view, um, ‘cause we both know that I’ve been told that I can’t be cured and it’s just prophylactic care….And she’s said to me ‘If you think I’m trying to ask you to do things that is too much for you, you just say, and that. Um, due to the fact that she’s also very, very interested in my illness. (Miss Clarke, 50 years, Parkview intervention group interview)
Where relationships are weaker and there is dissonance in information exchange (due to lack of an existing relationship or lack of agreed orientation), the agenda form amplifies existing tensions:
I saw (diabetologist). At the end of the consultation he said to me, erm, you have 10 s is there anything else you would like to ask me which I thought was, you know, ha ha ha…couldn’t believe it, I was so gob smacked… I just walked out you know….Well he seemed very arrogant to me. (Mr Martin, 74 years, Moorland, intervention session)
Orientation to the use of the intervention
Consultative styles were not distributed equally across our typology. Most consultations had some examples of shared decision making (ie, patient led or diabetologist facilitated), with fewer examples of interactions that were either explicitly consultant led, or where the patients’ agenda remained unvoiced or was ignored.
Despite participating in the study, two diabetologists did not embrace the philosophy of the project:
I discuss the issues but I tend to find that I don’t get answers that I, that I want…Yeah, maybe the doctor’s got a different opinion about it, but I would like to see results and I don’t see the results… there’s always a different answer coming back to me from the um, the diabetic doctor… maybe I’ve got one way of thinking and he’s got a different way, you know. And when I said to him, you know, ‘What about an insulin pump, would that help?’ ‘Oh well, yeah, but you wouldn’t, it wouldn’t be any good for you’ and that’s it, you know, nothing’s tried. (Mr Wright, 52 years, Parkview, control group interview)
Two patients in the intervention arm were prevented from using the agenda as intended. Dr Smith wrongly believed that the intervention was making the clinic run over, and Miss Taylor was prevented from completing the intervention, to ensure that the clinic was not affected. Another patient, Mr Davies, reported that he was told by Dr Green to ‘put the agenda form in his backpack’ because it was not needed. Although both instances may be due to misperceptions about the impact of the study on clinic waiting times,17 evidence from the consultations suggests that both of these diabetologists typically favour a more consultant-led style of consultation:
I don’t think the agenda improved it at all, it may have been slightly useful for her but from my perspective we discussed two things that weren’t relevant to diabetes. So I was doing a general practitioner role and we over ran by about 10 min as a result so I have considered that a negative experience on my behalf, but she may have liked it. (Dr Smith, Moorland, message left for researchers on audio-recorder).
Some patients did not produce their own agenda (eg, Mr White), and took blank forms to consultations, suggesting to the HCA that they did not have any concerns or that they were satisfied with how the diabetologist conducted the consultation.
In contrast, there were more diabetologists with a more facilitative predisposition, who embraced the ethos of the agenda form, and permitted patients to set the agenda for the consultation, even if this led to patients discussing unrelated issues:
I seem to remember one of the questions that they asked … it was really off the wall, as in it was really not really at all relevant in terms of their care… it introduced new topics that I wouldn’t have brought up myself and they might not have otherwise done…And they say this all the time ‘Is this something I can discuss here or is this something I should discuss with the GP?’ (Dr Williams, Moorland, interview)
Well, I thought it was, one of the reasons I was interested in the study was ‘cause I am concerned, so—my background to this is I watch my friends who’ve all become GPs, get trained in consultation skills and how to set up consultations …And since some of the principles of the study involved sort of setting up a patient agenda and maybe an alternative way of tackling a consultation that improved patients well-being, might potentially improve patient engagement with that process … (Dr Thomas, Parkview, interview)
Patients who engaged with the intervention highlighted presuggested issues and/or used the form to write their own list of questions or concerns —with only some highlighting the three most important issues as instructed. The most common agenda item was medication and insulin management specifically.
I think (the agenda form) was good idea… ‘cause I must admit I go down to the doctors’ and you go on to one thing and then suddenly summat’ll be said and then they go off in a direction and then you’ve got to try and get back on to what you want to talk about….we just went through the agenda, basically, you know, we’d talk about this, what are you doing, where’s your weight, you know, what’s your sugar levels and everything else… (Mr Hughes, 55 years, Parkview, intervention group interview)
Impact on the consultation
Having identified the significance of existing consultative styles and orientations, we then explored how they related to the PPI identified typology and the use of an agenda form:
Patients were ignored when, despite completing an agenda form, the diabetologist stuck to their regular script and conducted business as usual. These diabetologists often declined to have their consultations recorded, despite the patient consenting, and information was thus gathered from observations and conversations in the clinic, or by interview with the patient at home. For example, this patient had three questions on her agenda form but perceived that she has still not been able to discuss them (figure 1):
Well, what I mean is probably I don’t talk. I can’t talk about the impact on my life, like you’ve asked me today (in the qualitative interview) mostly it’s all internalised in my head, my experiences of diabetes. (Mrs Edwards, 76 years, Moorland, intervention group interview)
Consultations were consultant facilitated when the diabetologist stuck to their pre-existing script or maintained business as usual despite the participant writing a list of concerns. In this example, the diabetologist focused on the patients’ perceived lack of understanding rather than their agenda:
D: Since the exenatide hasn’t worked I don’t have another treatment that will help your diabetes and also cause weight loss or isn’t any other treatment we have. So insulin is what we have to go with, okay and your blood sugar levels have been very high, and I can see from that blood test they have been worryingly high so I would say to you that we do need to increase the insulin dose and in fact get your blood sugars down.
P: By how much, you know?
D: I don’t know, so be clear just try that, bear with me sir, please bear with me. I don’t know now how much insulin you will need, so some people need…
P: How is that you can be so certain that exenatide is not doing me any good… yet you failed to tell me what dose I should be taking of insulin.
D: I think you should just listen and I will answer that question for you… With insulin different people have hugely different requirements so some people take 20 units a day, some people might take several hundred units in a day, okay. So if I look at you and you say to me, how much insulin do I need? The answer is I do not know how much insulin but we have a way of finding out, so the answer is we increase the dose, until your blood sugars come down, so otherwise this case would increase, an increase until we get the dose right, okay.
P: But by how much?
D: That is something I can’t tell you, I am just explaining.
(Mr Martin, 74 years/Dr Smith, Moorland, intervention group consultation)
Mr Martin and Dr Smith had an established relationship, and we found no evidence that having an enduring relationship in itself was a guarantee of agenda facilitation. Nor did we find evidence that the age of the patient determined either their desire or experience of shared decision making, although we acknowledge that due to recruitment challenges our sample was small.
Consultations were consultant facilitated and patient initiated when pre-existing relationships were positive and/or the ethos of shared decision making was embraced. In this example, the participant had recently been diagnosed with dementia and attended the clinic with his wife who was his carer. They identified 12 concerns, and the diabetologist focused on his primary concern, which was tiredness:
D: Good to have (your) concerns. Right, OK. Right, nice to see you again.
P: Yes.
D: It’s been a little while hasn’t it… Since I saw you last time. … Yeah, how are you anyway, bring me up to date
P: Going down really, aren’t I?… I was getting so tired, very tired, you know, got no energy at all. I don’t know that’s the diabetes or the, um…
D: So that’s still the main concern, really, from your end of the line, this fatigue, we just haven’t really got on top of that….
P: … Oh yes, just been diagnosed with dementia as well, the start of dementia…
D: You have?
P: Vascular dementia…
D: How did that come about?
P: Um, it’s just my GP, we were talking to the GP and I was saying I was beginning to forget a lot of things and she did a few tests and um, said ‘Yeah, it looks as though you are’ and she sent me off to see a specialist in (place)…
D: Have you stopped any treatment that you were on, or are you basically finding you still need all the same?
P: I still need all the same stuff…
D: Right. Um, there’s a few things I suspect we need to chat about today. Were there any other specific concerns that you had at this point?
P: Not really, no…
D: That’s the general issue. (Mr Lewis, 74 years/Dr Smith, Parkview, intervention group consultation)
Few consultations were patient identified. This tended to occur when patients had greater material advantage, for example, they were a health professional with a similar repertoire of knowledge, long-standing patients who were competent at self-management, or a new patient already versed in shared decision making. In this example, a new patient, who had recently returned to the UK from living overseas, was able to articulate a range of concerns for the diabetologist to address:
D: Can I ask you, you’ve gone through an agenda before you came in this morning, what were the areas of concern that, um, you wanted to discuss today?
P: Well, I think now that I’ve basically on the insulin and getting my diabetes organised is the neuropathy that’s of most concern right now.
D: So there’s …
P: It’s affecting my lifestyle to such an extent, I’m not sleeping. Because I walk every day, I mean, you have to walk, but it’s just um, I mean, I like to do all the travelling and walking and I’m concerned about it, how it’s going to affect my lifestyle.
D: How is it affecting you currently? So what symptoms does your neuropathy give you currently?
P: Er, a lot of pain, aching, deep ache….
D: OK. Apart from pain, does it affect you any other way? Is pain the main feature at the moment, is it that when you’re walking you’re unsteady at all, or…?
P: Yeah, my balance has been affected, yes.
D: OK. So there’s your neuropathy, concern number one. Were you saying that your diabetes, just levelling out your glucose levels, your glucose values, was also a concern to you, getting those optimised, is that part of your…?
P: Oh obviously, it’s going to, yeah, that’s a major concern, yeah, just getting those level, get it right, diet organised, those levelled out and just the feeling of being, I feel like I’ve got the ‘flu' all the time, just tired.
D: You’re tired, OK.
P: Just tired all the time. So, I mean, I don’t know whether there’s any health things, I haven’t had a complete health check-up for years, so, I mean, it’s just really difficult.
D: OK, but those are the … are there any other areas you want to bring up today, or are those the three?
P: No, those are the three, yeah. (Mrs Harris, 65 years/Dr Thomas, Parkview, intervention group consultation)
In the wider transcript of the consultation, Mrs Harris suggests that her motivation for asking questions was the differing experiences of diabetes provision that she experienced in both North America and Australia, and her recent diagnosis of neuropathy, which she interpreted as a sign of deterioration.
Discussion
The principal finding is that where patients and diabetologists have a shared preference for a consultant-led or patient-led consultation the PACE-D augments effective communication and shared decision making. However, where preferences diverge PACE-D does not improve the potential for shared decision making (ie, concerns could remain unvoiced or ignored). The trial design allowed us to compare individual consultative styles across arms, outpatient settings and between cases. The majority of patients who completed the PACE-D found the intervention acceptable, and suggested that it helped them to think about issues related to their care.17 Our qualitative findings provide insights into how an agenda form may (or may not) function in medical consultations where patient concerns are often discounted.28 29
Our findings support those of previous research that used a single exposure intervention for prioritising diabetes-related treatment goals30: PACE-D did not universally improve patient empowerment, but acted as a magnifier for pre-existing consultative styles and orientations. Our findings are similar to those of Rhodes et al who identified that at worst, patients can experience ‘industrialisation’ of diabetes care whereby their concerns are diminished by the demands of the clinic, while at best the clinician can use the introduction of an intervention as an opportunity to practise patient-centred care.31 Key challenges that we identified include: lack of resources in the outpatient setting (including lack of time and space for an intervention) and lack of buy-in from clinicians despite consenting to participate. Any future research would need to give these contextual factors greater consideration in the designing and planning stages.
A limitation of this study is that although we planned recruitment of 120 participants, only 71 participants were randomised during the 7-month recruitment period, and only half agreed to participate in this qualitative study. We have previously identified that a randomised controlled trial of the preconsultation web-based intervention as set out in our current protocol is not feasible without significant modification to improve recruitment and follow-up of participants.17 However, triangulating data from interventions sessions, consultations, agenda forms and interviews allowed us to identify the extent to which individual patient concerns were addressed in a given consultation.23 As a recent systematic review of interventions to improve health outcomes arising from patient-clinician encounters failed to include trials that sought to explicitly empower patients,31 our findings suggest that more now needs to be done to explore which interventions patients consider to be most effective at addressing their concerns.
A strength of this study is the participation of patient representatives at all stages of the study enabled them to make a valuable contribution to our understanding of intervention development and implementation. We concluded that it would not be appropriate to run a definitive randomised controlled trial without amending our intervention in order to optimise the elicitation and utilisation of the patients’ agenda.
Conclusion
A simple web-based intervention can facilitate the articulation of patients’ unvoiced agenda for a consultation with their diabetologist, but only when pre-existing consultation styles and orientations already favour shared decision making. More needs to be done to translate patient empowerment in the consultation setting into genuine self-efficacy.
Acknowledgments
The authors would like to thank the study sponsor Royal Devon and Exeter NHS Foundation Trust. The authors would like to thank Donald Cegala (Emeritus Professor of Communication and Family Medicine, Ohio State University) for supporting their use and modification of the PACE intervention. Catherine Argyle (CA) assisted in the preliminary charting exercise. Faith Harris-Golesworthy, Jim Harris and the wider group of PPI representatives undertook the qualitative data analysis, transforming our understanding of doctor-patient consultations. Lucy Moore (LM) independently second coded the qualitative data.
References
Footnotes
Contributors NB, AG, OU, BV, JF conceived the original study and developed the protocol. JF led the writing of the first draft of the manuscript, with contributions from AG, OU, BV and NB. All authors contributed to the editing and redrafting.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Ethics approval The original protocol for this study and subsequent minor amendments were approved by the NHS Research Ethics Committee North West—Preston (13/NW/0123). ISRCTN5070242.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Transcripts will not be shared in their entirety to protect the anonymity of patients and diabetologists delivering the intervention. However, requests for excerpts of the data will be considered on an individual basis. Please contact the corresponding author.
Collaborators Faith Harris-Golesworthy; Jim Harris.
Patient consent for publication Obtained.