Article Text

Abstract
Background Physical and cognitive impairments are important risk factors for falls in older people. However, no studies have been adequately powered to examine whether cognitive or cognitive-motor training can prevent falls in older people. This is despite good evidence of improvements in fall-related cognitive and physical functions following both intervention types. This manuscript describes the study protocol for a three-arm randomised controlled trial to evaluate the effectiveness of home-based cognitive and cognitive-motor training interventions, compared to a minimal-intervention control group, in preventing falls in older people. This trial was prospectively registered with the Australia New Zealand Clinical Trial Registry, number ACTRN12616001325493.
Methods and analysis Community-dwelling adults aged 65 years and over, residing in Sydney Australia, will be recruited. Participants (n=750) will be randomly allocated to (1) cognitive-only training, (2) cognitive-motor training or (3) control groups. Both training interventions involve the use of the smart±step home-based computerised game playing system for a recommended 120 min/week for 12 months. Cognitive training group participants will use a desktop electronic touch pad to play games with the smart±step system while seated and using both hands. The cognitive-motor training group participants will use a wireless electronic floor step mat that requires accurate stepping using both legs for playing the same smart±step games, hence incorporating balance exercises. All groups will receive an education booklet on fall prevention. The primary outcome will be rate of falls, reported by monthly diaries during the 12-month duration of the study and analysis will be by intention-to-treat. Secondary outcomes include the proportion of fallers, physical and cognitive performance in 300 participants, and brain structure and function in 105 participants who will undertake MRI scans at baseline and 6 months. Cost-effectiveness will be determined using intervention and health service costs.
Ethics and dissemination Ethical approval was obtained from UNSW Ethics Committee in September 2015 (ref number HC15203). Outcomes will be disseminated through publication in peer-reviewed journals and presentations at international conferences.
Trial registration number ACTRN12616001325493
- accidental falls
- randomised controlled trial
- fall prevention
- cognitive training
- balance training
- stepping
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- accidental falls
- randomised controlled trial
- fall prevention
- cognitive training
- balance training
- stepping
Strengths and limitations of this study
This pragmatic single-blind randomised controlled trial is powered to evaluate the effectiveness of two novel exergaming interventions that incorporate cognitive training on the rate of falls in older people.
The interventions will involve identical exergames, one group will play with their hands while seated (cognitive training), the other group will play by stepping on a step mat (cognitive-motor training), such that any differential effects of the interventions will provide valuable insights into intervention components required for fall prevention.
This design will provide understanding of the relative contributions of cognitive and motor training to fall prevention as well as physical, neural and cognitive secondary outcome measures.
Outcome assessors are blinded to group allocation, but participant blinding is not possible.
The minimal intervention control group will have a reduced amount of research staff contact compared to the intervention groups.
Introduction
Falls in older people are a significant public health issue. With an ageing population, the impact of falls is projected to grow, creating additional demands on the health system that will be difficult to meet.1 Furthermore, the personal and community burden from falls is substantial, including mobility-related disability and loss of independence.2 3 The rate of falling in people with only mild cognitive impairment is significantly elevated compared to the general older adult population, suggesting that falls are not just a motor problem.4
Several fall prevention strategies have been tested in randomised controlled trials (RCTs), with good evidence for the effectiveness of exercise.5 6 In fact, systematic review evidence from 88 trials indicates exercise has a moderate (21%) effect in preventing falls with greater effects for interventions that include moderate–high-intensity balance training.6 Yet, some interventions have low adherence, especially in the longer term, and few interventions explicitly address the crucial risk factor of impaired cognition.
Impaired executive function has been found to be the primary neuropsychological risk factor for falls, independent of processing speed and balance impairments.7–9 Computerised cognitive training can improve cognitive ability10 11 and there is emerging evidence indicating such training also improves motor function and reduces fall risk.9 For example, computerised cognitive training has been shown to improve performance in clinical tests of mobility and gait speed.12–14
Cognitive-motor training programmes are considered promising strategies for improving physical function in older people with the use of computer-based technology ideal for such interventions.15 16 Interactive computer gaming (exergames) are emerging as tools for improving balance ability in older adults,17 addressing the issue of low exercise adherence by providing an enjoyable and engaging method of training.18 Exergames are played by the user performing physical exercises and can readily incorporate various cognitive challenges.
Training programmes that target both cognitive and motor activity involving balance control may provide enhanced value for fall prevention.19 20 Accurate and appropriately timed stepping is crucial for avoiding falls,21 and our pilot studies have shown that step training while playing computer games significantly improves balance, choice stepping reaction time , dual-task ability22 and cognitive functions including processing speed, attention, visuospatial skills and executive functioning.23 We have developed the smart±step in-home computerised game playing system that involves either cognitive-only (seated) or cognitive-motor (stepping) training by playing custom-built and adapted versions of popular video games that require cognitive functions.
This pragmatic RCT aims to determine the effectiveness of home-based cognitive-only and cognitive-motor training in preventing falls in older people, compared to a minimal-intervention control group. We hypothesise that both training programmes will prevent falls in older people via improvements in physical, cognitive and neural functions. Any differential effects of the interventions will provide valuable insights into the intervention components required for effective fall prevention, and those required for neural, neuropsychological and physical benefits. We will also estimate the cost-effectiveness of these interventions compared to usual care. The completion of this trial is expected by the end of 2020.
Methods and analysis
Trial design
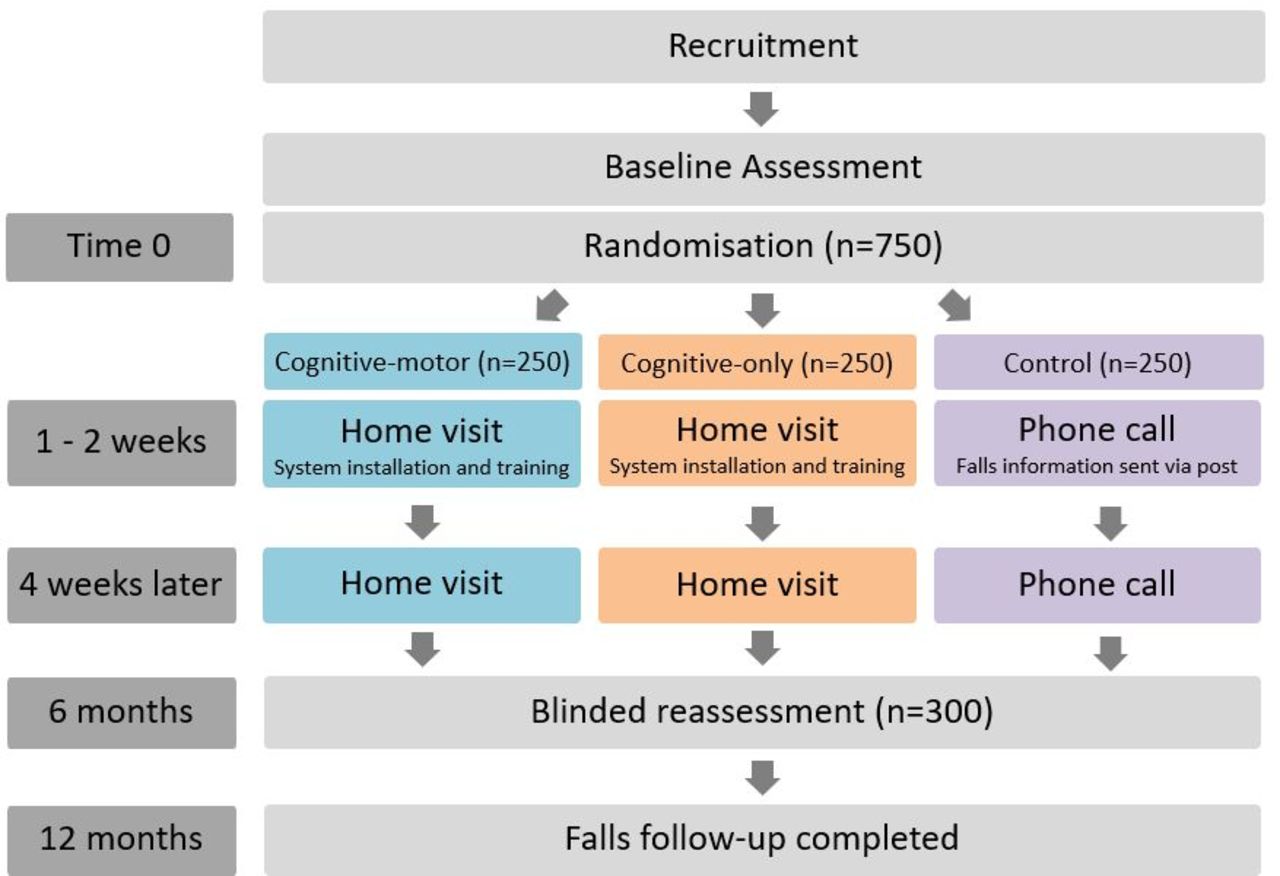
A single-blind three-arm parallel RCT with a 1:1:1 allocation ratio (figure 1) will be conducted to examine the effectiveness of two home-based interventions involving computerised game play, compared to a control group, on falls in older people. Falls will be monitored in all participants for 12 months. The protocol was registered prior to randomisation of the first participant on the Australian and New Zealand Clinical Trial Registry, see online supplementary appendix 1. Important protocol modifications will be recorded on the trial registry.
Supplementary file 1

Study flow diagram.
Participants and eligibility
Seven hundred and fifty people aged 65 years or older, living in the community, will be recruited via mailings to members of a private health insurance company, advertisements in circulars and flyers distributed to community groups. Eligibility criteria include age 65 years or older; English-speaking; living in the Sydney metropolitan area; independent in activities of daily living; able to walk 10 m without the use of a walking aid; willingness to provide informed consent and comply with the study protocol. Exclusion criteria include an acute psychiatric condition with psychosis; an unstable medical condition that would preclude safe participation; a progressive neurological condition (such as Parkinson’s disease, multiple sclerosis, Meniere’s disease); cognitive impairment defined as a Pfeiffer Short Portable Mental Status Questionnaire (SPMSQ) score <824; residing in residential aged care, currently participating in a fall prevention trial.
Potential participants undertake initial eligibility screening in a telephone interview. This includes the SPMSQ.24 Trained research personnel will provide detailed study information, obtain verbal consent and arrange an appointment for a baseline assessment. Study information will also be posted to potential participants at this time.
Immediately before a scheduled baseline assessment, participants will view a video showing the main aspects of the two interventions to ascertain their intention to adhere to the protocol. If participants indicate that they are not willing to adhere with the intervention protocol they will not undergo baseline assessment or take part in the study. Written consent will be obtained from those who are willing to participate in the study.
Randomisation
Following baseline assessment, participants will be randomly allocated to the intervention or control groups using a web-based randomisation service. Permuted block randomisation using computer-generated random numbers will be applied to form three groups of similar size (allocation ratio 1:1:1). People living in the same household are treated as one unit and randomised into their own blocks to ensure that equal numbers of couples are allocated to intervention and control groups. Allocation concealment will be ensured as the randomisation code will only be released to non-blinded research staff after all baseline assessments have been completed.
Interventions
All participants will receive an evidence-based education booklet on healthy ageing and fall prevention. The booklet includes information on healthy eating, medications, bone health, eyesight, foot care, depression, cognitive impairment and physical activity. It also includes information on risk factors for falls, evidence-based prevention strategies and information on what to do in the event of a fall. The provision of education material involves a follow-up telephone call to control group participants; this additional contact with the study team partially matches the staff contact received by intervention group participants during their home visits.
The training interventions will consist of computerised game play (exergame) using the smart±step system delivered with either a desktop touch pad (cognitive only) or a floor step mat (cognitive-motor) installed in the participant’s home. To play the games, the cognitive-only training is performed while seated and using the hands to press sensor targets on the desktop touch pad. The cognitive-motor training is performed while standing and stepping onto step targets on a wireless electronic floor mat (step mat). The step mat is designed so that game play by stepping in different directions on the mat challenges stepping speed, accuracy and balance control. With the exception of the game play response method (hands vs feet) the training is identical for both interventions with respect to dose, game type and progression. The smart±step system consists of eight games that are designed to target specific cognitive functions including working memory, visuospatial skills, dual tasking, inhibition and attention. These games were newly developed and/or adapted from popular video games by Neuroscience Research Australia (NeuRA) software engineers (see figure 2 and online supplementary appendix 2).
Supplementary file 2

Smart±step games. (A) StepMania, (B) Brick Stacker, (C) La Cucaracha, (D) Greek Village, (E) Alien Invasion, (F) Anaconda, (G) Toad Runner and (H) Dot Muncher.
Within 2 weeks from randomisation (figure 1, time 0), intervention participants will receive an initial home visit from an exercise physiologist, who will instal the equipment in an appropriate location in the home and provide training instructions. The cognitive-only training group will receive the smart±step system (personal computer, software and instruction/safety booklet), a touch pad and a desktop computer monitor and will be instructed to play the training games while seated and using the hands (figure 3a). The cognitive-motor training group will receive the smart±step system and step mat to interface with their television screen (or provided a monitor) and will be asked to play the games while standing and taking quick and appropriate steps on the mat (figure 3b). The exercise trainer will discuss goal setting and barriers to training with participants to encourage adherence to the training dose and exercise progression. Participants will be instructed to start on an easy level and when confident, progress to more challenging levels and try to beat their highest score.

{kind=link}
{kind=link}
{kind=link}
The smart±step system used for (A) motor-cognitive training and (B) cognitive training interventions. This participant has provided written consent for photography.
The exercise trainer will conduct a follow-up home visit 4 weeks after the initial visit to ensure safe use and progression of training and discuss any issues. To facilitate training progression, the exercise trainer will explain that obtaining high scores is best achieved by playing the exergames at the higher difficulty levels. Exergame difficulty levels are subsequently chosen by participants for the remainder of the trial. Additional home visits during the intervention will be offered only as needed/requested. At the completion of the 12-month trial, a research staff member will collect the training equipment from participants’ homes. Due to the nature of the intervention, participants and exercise trainers will not be blinded to group allocation.
Training dose
Intervention participants will be encouraged to undertake at least 120 min of smart±step training per week for 12 months, to maintain the effects of exercise over the period of collection of the primary outcome. Weekly game play will be capped at 150 min to help ensure equal doses of training between the cognitive-only and cognitive-motor training groups. To ensure a variety of games are played, participants will be required to play two core games on each day they train (Stepmania and Brickstacker), after which the other games will become available to play. To encourage adherence, medals will be awarded based on the number of minutes played each week (bronze for >80 min, silver for >100 min, gold for >120 min) and collected over the 12-month intervention. To encourage progression, participants will receive feedback after each game; that is, the score for the game just completed and their highest score for that game to date.
Monitoring
Adherence will be monitored following daily data transfer from participants’ smart±step personal computers to a server at NeuRA. Participants engaging in <80 min of training per week for two consecutive weeks will be contacted by telephone to encourage improved adherence, assist with goal setting and address barriers to training.
Outcomes
Assessments, including questionnaires and physical and cognitive performance tests (table 1) will be conducted by trained staff in clinic rooms at NeuRA (figure 1). The order of these assessments will be standardised and take ~2 hours to complete. At baseline, demographic data will be collected, including age, gender, living arrangements, education, computer use, health, lifestyle, function, disability and medical history (presence of medical conditions, medication use and fall history), will be collected.25–28 Falls will be monitored in all participants for 13 months from their baseline assessment according to recommended methods using falls calendars,29 as described below. Research staff collecting falls data and conducting the reassessments will be blind to group allocation.
List of measures collected at BA, 6M and 12M assessments
A subsample of 300 consecutive consenting participants will return for physical and cognitive performance reassessments 6 months’ postrandomisation. MRI will be conducted in a subset of participants (n=105) who consent to a 1 hour scanning session and experimental memory paradigm at the University of Sydney within 2 weeks of the baseline and 6-month physical and cognitive assessments.
Measures
Outcome measures and their measurement time points are outlined in table 1. The primary outcome measure is the rate of falling at 12 months and additional fall metrics are secondary outcomes. A fall is defined as ‘unintentionally coming to the ground or some lower level and other than as a consequence of sustaining a violent blow, loss of consciousness, sudden onset of paralysis as in stroke or an epileptic seizure’.30 Falls frequency will be monitored with monthly falls calendars, according to recommended protocols.29 Calendars are designed for daily recording and monthly return to research staff via email or postal mail. Participants who report falling will be telephoned to seek more information about the circumstances and consequences of the fall, including medical interventions and hospitalisations. If a diary is not returned within 2 weeks of the end of each month, participants will be contacted by telephone to obtain the falls data required. These data will be collected regardless of deviation or discontinuation of the intervention.
Secondary outcomes include physical performance, neuropsychological (cognitive) performance and neural function measures to (1) elucidate mechanisms underlying any fall reduction observed in the trial and (2) determine to what extent the training transfers to other important outcomes such as balance, mobility, quality of life, cognitive functioning and neural plasticity (brain structure and function changes).
Standing balance will be assessed using a swaymeter to measure postural sway while standing on a foam rubber mat for 30 s.31 Leaning balance will be assessed with the coordinated stability test, which requires participants to adjust their body position in a steady and coordinated manner when near the limits of stability32.32 Spatial and temporal parameters of gait (velocity, step length, cadence, double support time, support width and gait variability) will be measured while walking at usual speed over a GAITRite system (CIR Systems, Clifton, New Jersey, USA),33 a 6 m long mat embedded with active sensors to measure footfall time and position, under single-task and dual-task conditions (counting backwards by 3 s) for three trials each. Balance and mobility will be further assessed with the short physical performance battery and the timed up and go test. The short physical performance battery contains three timed tasks: static balance in three foot positions, gait speed over 4 m and sit-to-stand five times.34 The timed up and go test, which measures the time taken to stand, walk 3 m at usual pace, turn around, walk back to the chair and sit down, will be used to determine posited training effects on mobility performance.35 Simple had reaction time will be measured in milliseconds with participants seated using a light as the stimulus and a finger press as the response.31
Stepping performance will be assessed with a series of stepping reaction time tests providing composite measures of balance, executive function and reaction time.21 For choice stepping reaction time, participants are required to step as fast as possible onto one of six target panels on an electronic step mat (two forwards and backwards and one left and one right) as presented on a display screen in random order. The choice stepping reaction timetest will be conducted with and without a go/no-go task, requiring participants to select between response activation and inhibition36 and conflict resolution (Stroop) task, requiring participants to step on the panel according to a word written within the arrow, rather than the arrow direction.37
Neuropsychological measures of executive functions will be undertaken, including working memory, processing, inhibition, attention and set-shifting. These include the Trail Making Tests (parts A and B) of selective attention and processing speed,38 the Victoria Stroop test of attention and response inhibition,39 the controlled oral Word association test38 of verbal fluency, the digit span test of working memory,40 and the Wisconsin card sorting test of problem solving and set-shifting.41 The Addenbrooke’s Cognitive Examination Revised42 will be used to assess global cognition.
Quality of life will be assessed using the utility-based quality of life measure EuroQol EQ-5D.43 An Australian scoring algorithm for the EQ-5D44 will be used to estimate quality-adjusted life years (QALY) for the economic evaluation. Concern about falling will be assessed with the Iconographical Falls Efficacy Scale mobile application.45 Detailed self-report information on weekly frequency and duration of physical activity over the last 3 months will be assessed using the Incidental and Planned Exercise Questionnaire.46
The average weekly training duration and total training duration will be used to assess adherence at 6 and 12 months. The Attitudes to Falls-Related Interventions Scale47 and the Exercise Self-Efficacy Scale48 will assess the acceptability of the interventions. The System Usability Scale49 and Physical Activity Enjoyment Scale50 will be used to assess usability and enjoyment of the smart±step system within each intervention group.
Neuroplasticity substudy
The first consecutive 105 participants who consent to the MRI component of the study and are eligible for this procedure will attend the Brain and Mind Centre, University of Sydney to undergo scanning at baseline and 6 months on a 3-Tesla 750 Discovery GE scanner (Milwaukie, USA) and 8-channel receive head coil. Multimodal MRI scanning (total scan duration=60 min) will provide measures of brain structural plasticity, white matter plasticity, functional network plasticity and neurometabolic plasticity and will be processed, as previously reported.51 In brief, brain structural plasticity will be assessed via structural MRI (3D whole-brain T1-weighted spoiled gradient sequence with 1 mm isotropic resolution, TR=6.40, TE=2.35, TI(=450 ms), using a combination of whole-brain analyses (Voxel-Based Morphometry and FreeSurfer-based cortical thickness and subcortical volumetric processing streams).51 Hippocampal subfield plasticity will be determined from a dedicated, high-resolution T2-weighted spin echo, coronally obliqued sequence (in-plane resolution 0.4×0.4 mm, slice thickness=2 mm, TR/TE=6000/105 ms), using the FreeSurfer-based and automated segmentation of hippocampal subfields-based hippocampal subfield processing streams. White matter plasticity will be determined with Diffusion Tractography Imaging (64-direction, blip-up, TR/TE=8250/66 ms, 60 slices, 2 mm3 isotropic, with an additional blip-down B0 for postprocessing, echo-planar imaging (EPI) distortion correction), using a combination of whole-brain analyses of fractional anistropy as well as fibre-tracking analyses focused on the planned regions of interest, using our published techniques.51 Functional network plasticity will be assessed using resting state functional magnetic resonance imaging (T2*-weighted, EPI-based blood oxygenation level dependent acquisition with 200 whole-brain volumes acquired eyes closed TR/TE=3000/36 ms, slice thickness=4 mm, in-plane resolution=4×4 mm) to examine change in hippocampal and prefrontal cortical networks as determined by seed-based correlational analyses using the Data Processing Assistant for Resting-State Functional MRI processing stream.51 Neurometabolic plasticity will be assessed with 1H-magnetic resonance spectroscopy (Point-RESolved Spectroscopy, TE 30, TR 2000) from regions of interest placed in the posterior cingulate (voxel size=20×20×20 mm, averages=128) and left hippocampus (voxel size=10×15×30 mm, averages=256). Absolute concentrations of N-acetylaspartate, myoinositol, phosphocreatine + creatine and glutamate/glutamine will be estimated using our published techniques.51 The same MRI subsample also undergo an experimental pattern separation memory paradigm to assess for links to individual variation and plasticity of hippocampal subfields.
Safety and data quality
Participants enrolled in the study will be assigned a unique identification (ID) code. All data collected will be identified with this ID to maintain participant confidentiality. Records that contain names such as consent forms will be stored separately from study records that include IDs.
Data will be collected using a combination of paper-based and web-based data forms. Electronic study data will be managed using Research Electronic Data Capture tools hosted securely at NeuRA.52 Data integrity will be enforced via valid values and range checks. Trial data integrity will be monitored by regularly checking data files for omissions and errors. A subset of data will be re-entered later for quality control.
Original paper-based versions of data collected will be stored securely at the study site and participant information will be stored in locked cabinets in areas with limited access, in accordance with procedures approved by the ethics committee. Participant files will be maintained in storage for at least 7 years after completion of the study.
Any adverse events associated with the intervention will be monitored, recorded and reported to the study Safety and Data Quality Committee, as well as the research institute’s (NeuRA) Safety Monitoring Committee. Adverse events will be reported to the responsible Institutional Ethics Committee.
Sample size
A sample size calculation (5% significance level, 80% power, 33% effect, 20% dropout rate) was performed using the nbpower command in STATA version 16 and indicated a sample size of 750 will be necessary for this study. Our previous study of 500 older adults was used to calculate alpha (a measure of over-dispersion in the negative binomial regression model), found to be 1.2.53 The control group rate of falls was assumed to be 0.8 fall/person-year and the incident rate ratio of 0.67 was based on meta-regression results from 41 RCTs investigating the effect of balance challenging exercise on falls rates.54 Our pilot trials22 23 indicate that a subsample of 300 participants will be sufficient to detect between-group differences in secondary outcome measures. For example, we have 95% power to detect differences in postural sway (effect size f=0.38, correlation ρ=0.76, repeated measures analysis of variance (RM ANOVA), α 5%, 20% dropout). The sample size for the MRI substudy is based on previous study findings showing significant beneficial effects on posterior cingulate cortical thickness following resistance training and hippocampal resting-state functional networks following cognitive training.55
Statistical analysis
Primary outcome
Primary outcome analyses (rate of falls over 12 months between groups) will be conducted using an intention-to-treat approach and data will be coded to maintain group allocation blinding. Analyses will be conducted by an independent statistician using Statistical Package for Social Sciences and Stata v16 software packages and will be separately replicated by a study investigator. The number of falls per person-year will be analysed using negative binomial regression to estimate the difference in fall rates between comparison groups (cognitive-only vs control and cognitive-motor vs control).
Secondary outcomes
The rate of falls, proportion of fallers and rate of falls per weekly hours of physical activity among the comparison groups will be compared using negative binomial regression and the relative risk statistic respectively using an intention-to-treat approach. In addition, complier average causal effect analysis will be used to explore intervention effects in people with greater adherence.56 The effect of group allocation on the continuously scored secondary outcome measures will be examined with mixed-effects models. Predictors of uptake, acceptability and adherence will be established using multivariate modelling techniques including multiple linear and logistic regression analyses. As the outcomes are categorised by degree of importance (primary and secondary), p values will not be adjusted for multiplicity.
Economic analysis
An economic evaluation will be conducted from the perspective of the health system according to current guidelines.57 The outcome measure for the cost-effectiveness analysis will be the cost per fall prevented over the 12-month study duration. Benefits will also be measured in terms of QALY gained in the intervention groups compared to the control group, based on utility weights derived from the EQ-5D at baseline, 6 and 12 months. Data will be collected prospectively regarding costs of programme delivery (including staff, training, equipment, consumables, and administration and overhead costs), fall-related healthcare resource use and the total cost of healthcare resource use. Using the mean costs in each trial arm and the mean health outcomes in each arm, the incremental cost per QALY of the intervention groups compared to the control group will be calculated. Results will be plotted on a cost-effectiveness plane.
Bootstrapping will be used to estimate a distribution around costs and health outcomes, and to estimate the confidence intervals around the incremental cost-effectiveness ratio. One-way sensitivity analysis will be conducted around key variables, and a probabilistic sensitivity analysis will be conducted to estimate the joint uncertainty in all parameters and a cost-effectiveness acceptability curve will be plotted. This curve provides information about the probability that an intervention is cost-effective, given a decision maker’s willingness to pay for each additional QALY.
Patient and public involvement
Following a pilot study of our earlier cognitive-motor step training system,23 24 intervention group participants, aged 70–97 years, were interviewed regarding their experience using the training programme, to identify usability issues, to explore factors influencing programme uptake and adherence and to guide the current trial design.58 These results were used to refine the smartstep system, including the development of new games and feedback elements. None of the study participants or public were involved in the development of the research question, design, recruitment or conduct of the study.
The participants of the current study will be provided with a summary of their baseline and 6-month assessments and will be emailed or postal mailed a brief report outlining the main results of the study in layman’s terms.
Discussion
Due to current population ageing trends, a sharp rise in fall-related healthcare costs is expected,1 indicating the urgency for effective fall prevention strategies to be identified and implemented. Exercise can prevent falls in older people but compliance with exercise protocols is often suboptimal. Exergaming is a promising approach to deliver falls prevention exercises and increase adherence in older people.59 In addition, exergaming enables integration of cognitive training, from which additional benefits might be gained for fall prevention.60
This RCT will evaluate the effects of both cognitive and cognitive-motor training for preventing falls in older people. These results will be representative of relatively healthy and motivated people aged 65 years and over, living independently in the community. In addition, changes in fall-related neural, physical and neuropsychological functions will be examined. This study has the potential to significantly reduce fall-related injury and enhance cognition, physical functioning and quality of life in older people. Any differential effects of the interventions will provide valuable insights into the intervention components required for effective fall prevention and those required for neural, neuropsychological and physical benefits. An economic analysis will determine cost-effectiveness, important for future implementation. Recruitment for the study commenced in November 2016, and we expect final results to be available in mid-2020.
Dissemination
The results of this trial will be disseminated in a peer-reviewed scientific journal and presented at national and international conferences. Authors will have provided substantive contributions to the design, conduct, interpretation and reporting of a data within a publication.
References
Footnotes
Contributors DLS, SRL, KD, JM and MV conceived and designed the trial. Additional advice regarding design and statistical analyses was given by CS and RDH and technological aspects by DS. Funding was obtained by DLS, JM, KD and MV with significant input by SRL. MV, AL and KB designed the MRI substudy, including study protocols and oversaw data collection. JT established databases, study manuals, contributed to data collection and processing and assisted in producing the first draft of the manuscript. DLS is project manager. All authors contributed intellectual input into and approved the manuscript. The authors agree to be accountable for the work.
Funding This work is supported by the National Health and Medical Research Council of Australia Project Grant (ID: 1086804) and Programme Grant (ID: 1055084). Authors MV, KD, CS, RDH and SRL also receive salary funding from the National Health and Medical Research Council of Australia Fellowships. DLS is supported by a Bushell Foundation Rising Star Fellowship.
Competing interests None declared.
Ethics approval The study protocol has been approved by The University of New South Wales Human Research Ethics Committee (reference HC15203).
Provenance and peer review Not commissioned; externally peer reviewed.
Collaborators Organisational structure and responsibilities: principal investigator: Daina Sturnieks is responsible for the design and conduct of the trial, staff management, participant recruitment, data collection, adherence to study protocol, organising steering committee meetings and completion of reports. Steering committee (SC): Daina Sturnieks, Jasmine Menant, Michael Valenzuela, Kim Delbaere, Stephen Lord, Catherine Sherrington, Rob Herbert, Jessica Turner, Cameron Hicks, Mayna Ratanapongleka,Natassia Smith, Carly Chaplin, Bethany Halmy, Angeliki Stivactas, Ashley Woodbury, Dinaz Parekh, Matthew Hand, Kathryn Broadhouse, Isabella Hoi Kei Leung and Polly Barr. Trial Management Committee (TMC): Daina Sturnieks, Jasmine Menant, Michael Valenzuela, Kim Delbaere, Stephen Lord and Jennifer Davis. Safety and data quality: The Data Safety and Monitoring Committee comprises Professor Jacqueline Close and Ms Barbara Toson, who will review the progress of the trial and provide advice on the conduct of the trial to the Investigators Group and UNSW Ethics Committee. Data manager: Daina Sturnieks. Lead Investigators: Daina Sturnieks, Jasmine Menant, Michael Valenzuela, Kim Delbaere, Stephen Lord, Catherine Sherrington and Rob Herbert. All principal investigators will be given access to the cleaned datasets.
Patient consent for publication Obtained.