Article Text

Abstract
Objectives In the 2010s, there has been an increase in sexually transmitted infections (STI) in men who have sex with men (MSM) in Australia, and since 2015 also in urban heterosexuals. Men who have sex with both men and women (MSMW) have characteristics that may differ from both men who have sex with men only (MSMO) and heterosexual men. We aimed to compare the sexual practices and the trends in HIV/STI positivity between MSMO and MSMW.
Design Repeated cross-sectional study.
Setting A sexual health centre in Melbourne, Australia.
Participants MSM aged 18 years and above who attended the Melbourne Sexual Health Centre for the first time between 2011 and 2018. This includes 12 795 MSMO and 1979 MSMW.
Primary outcome measures Demographic characterics, sexual practices and HIV/STI positivity.
Results Compared with MSMW, MSMO were more likely to practice anal sex and to have condomless receptive anal sex with casual male partners, and less likely to have a current regular relationship. Over the 8-year period, there was an increase in condomless receptive anal sex with casual male partners for both groups (MSMO: from 46.2% to 63.3%, ptrend <0.001; MSMW: from 41.3% to 57.9%, ptrend=0.011). Syphilis positivity increased in MSMO (from 5.5% to 7.9%, ptrend=0.012) and MSMW (from 0.9% to 6.4%, ptrend=0.004) and HIV remained stable. Gonorrhoea increased among MSMO from 2011 to 2014 (from 6.7% to 9.6%, ptrend=0.002), and remained stable from 2015 to 2018. MSMO had higher odds of testing positive for gonorrhoea (adjusted OR (aOR) 1.36, 95% CI 1.13 to 1.64), chlamydia (aOR 1.39, 95% CI 1.16 to 1.67), syphilis (aOR 1.74, 95% CI 1.37 to 2.22) and HIV (aOR 4.60, 95% CI 2.43 to 8.70) than MSMW.
Conclusions MSMW have overall lower condomless sex and lower HIV/STI positivity. In the last years, changes in sexual practices in MSM have affected both MSMW and MSMO leading to an increased STI risk.
- sexual medicine
- epidemiology
- public health
- HIV & AIDS
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
We compared sexual practices and HIV/sexually transmitted infections positivity in a high number of men who have sex with men only (N=12 795) and men who have sex with men and women (N=1979) over an 8-year period.
We provide a comprehensive description of sexual practices distinguishing between condom use with regular or casual sexual partners, and in receptive or insertive anal sex.
The study was conducted in one urban major sexual health clinic and it is possible that our findings may not be generalisable to other settings.
We were unable to analyse the statistical significance of the temporal trends during the whole study period for gonorrhoea and chlamydia due to a change in the diagnostic test in 2015.
Introduction
Despite considerable public health efforts and biomedical advances,1 the rate of sexually transmitted infections (STIs) is increasing at an alarming rate particularly among gay, bisexual and other men who have sex with men (MSM) worldwide.2 Among the Australian population, the notification rate, defined as the number of new cases reported to the national infectious diseases surveillance system, increased an 80% for gonorrhoea (from 65.5 to 118.0 per 100,000), a 14% for chlamydia (from 364.5 to 416.8 per 100,000) and has more than doubled for syphilis (from 7.8 to 18.3 per 100,000) between 2013 and 2017.3 In males, most of the early rises in gonorrhoea and syphilis were accounted for by rises in MSM. However, in the late 2010s, there has been a dramatic increase in both infections in the Australian heterosexual population to levels not seen since the 1980s.4 In stark contrast to the rise in the notification rate of gonorrhoea and syphilis, there has been an 11% decline in the HIV notification rate from 4.5 per 100 000 in 2013 to 4.0 in 2017 among MSM in Australia, with most of the reduction occurring between 2016 and 2017 after the introduction of pre-exposure prophylaxis (PrEP) in late 2016.3 5–7
Past studies have shown that sexual practices among MSM have changed over time (eg, an increase in condomless anal sex).8–12 However, there have been very limited studies examining whether there are any differences in sexual practices between men who have sex with men only (MSMO) and men who have sex with both men and women (MSMW or bisexual MSM).13 14 Therefore, this study aimed to compare the characteristics and sexual practices, and describe the trends in HIV/STI positivity in MSMO and MSMW attending a large sexual health clinic in Melbourne between 2011 and 2018. Additionally, we aimed to explore differences within MSMW depending on the most frequent gender of their sexual partners.
Methods
We conducted a repeated cross-sectional analysis of retrospective data of MSM attending the Melbourne Sexual Health Centre (MSHC), Australia, between 2011 and 2018. MSHC is a public clinic that offers a range of free clinical services regarding sexual health. MSHC is the largest sexual health clinic in Victoria and provided more than 50 000 clinical consultations in 2019, approximately 40% of clients are MSM.5 On arrival, all clients are invited to complete a questionnaire via computer-assisted self-interviewing (CASI), which collects client’s demographic characteristics (eg, age, country of birth, Aboriginal and Torres Strait Islander status), sexual practices (ie, gender of partners, type of partners (regular or casual), number of partners, condom use and anal sex practice (receptive anal sex (RAS) and insertive anal sex (IAS))), sex work status and injecting drug use practice. Data on sexual practices and injecting drug use were measured in the past 12 months, and sex work status was defined as clients who had ever worked in the sex industry during lifetime. Clients are allowed to decline to answer any questions they may wish to.
Clients who were male, aged 18 years and above, reported having sex with another man in the past 12 months, and attended MSHC for the first time between 2011 and 2018 were included in this analysis. We only included data from the client’s first visit to MSHC to avoid any bias including men with repeated visits as they might be at a higher risk of HIV/STI with different sexual practices. We categorised MSM into two main categories based on their self-reported sexual practices: (1) MSMO and (2) MSMW. We further categorised MSMW into two groups: (1) MSM who reported more female partners than male partners in the past 12 months (MSMW-W) and (2) MSM who reported more male partners than female partners in the past 12 months (MSMW-M). We compared the characteristics between the MSMW-M and MSMW-W. Men with an equal number of male and female partners in the past 12 months (N=336) were excluded in the comparisons among MSMW subgroups but they were included in the overall MSMW category.
We also extracted the HIV/STI testing results on the day. STI testing results included syphilis (serologically confirmed by rapid plasma regain test, Treponema pallidum enzyme immunoassay and Treponema pallidum particle agglutination assay and including all syphilis stages), gonorrhoea (stratified by anatomical site: anorectal, urethral and oropharyngeal) and chlamydia (stratified by anatomical site: anorectal and urethral). For HIV, we analysed separately incident cases (diagnosed on the day of the first visit using screening assay followed by a confirmatory Western Blot assay) and MSM with a previous HIV diagnosis visiting MSHC for the first time. There was a major change in gonorrhoea and chlamydia testing at our clinic.15 Prior to 2015, gonorrhoea was diagnosed by using culture and chlamydia was diagnosed by nucleic acid amplification test using the BD ProbeTec Strand Displacement Amplification Assay (Becton, Dickinson and Co, Sparks, Maryland, USA). From March 2015 onwards, testing for both gonorrhoea and chlamydia was performed using the Aptima Combo 2 Transcription-Mediated Amplification Assay (AC2) (Hologic Gen-Probe, San Diego, California, USA). HIV and syphilis testing methods did not change during the study period.
Before July 2015, screening for urethral gonorrhoea was only performed in MSM with urethral symptoms while screening for urethral chlamydia was performed in all MSM as per the Australian guidelines.16 However, since July 2015, all MSM were screened for both urethral gonorrhoea and chlamydia regardless of the presence of symptoms as per our clinic policy.17 Therefore, the positivity for urethral gonorrhoea was calculated as the number of men tested positive divided by the number of men who were tested for urethral chlamydia to avoid the bias of testing urethral gonorrhoea only among symptomatic MSM until July 2015, and this approach was also used elsewhere.18 In addition, routine screening for oropharyngeal chlamydia among all MSM at MSHC were introduced in April 2017; before then, only MSM who reported as a contact of infection were tested. Routine screening for HIV, syphilis, oropharyngeal and anorectal gonorrhoea, and anorectal chlamydia were conducted among all MSM and the screening guidelines did not change over the study period at MSHC.
χ2 test was used to compare the demographic characteristics and sexual practices between risk groups. We examined the annual trends of sexual practices and HIV/STI positivity for MSMO and MSMW using χ2 trend test. Annual trends for condomless IAS and RAS with causal male partners were examined separately. We reported any condomless sex (ie, IAS and/or RAS) with regular male partners for the trend analysis due to the small number of participants who reported having regular male partners. For chlamydia and gonorrhoea positivity, we calculated the annual trends for 2011–2014 and 2015–2018 separately due to the change of the diagnostic assays.15 Univariable and multivariable logistic regression was used to examine the association between sexual practice (MSMW or MSMO) and HIV/STI positivity. We assessed HIV and each STI separately, and this included (1) gonorrhoea at any anatomical site, (2) chlamydia at any anatomical site, (3) syphilis, (4) new HIV diagnosis on the day of the first visit and (5) previous HIV diagnosis, as the dependent variables. Therefore, five different logistic regression models were conducted, and the independent variables included sexual practice (being MSMW or MSMO and using MSMW as reference), the year of the visit and all potential confounding factors (ie, variables with p<0.20 in the univariable analyses) in the multivariable analysis. Missing data were presented as ‘no information’. We repeated the same procedure using sexual practice categorised in MSMO, MSMW-M and MSMW-W as the independent variable with MSMW-W as the reference group. We reported the crude odds ratio (OR) and adjusted OR, and their respective 95% confidence interval (CI). The 0.05 level was used for statistical significance in all the analysis. All statistical analyses were conducted using SPSS V.25.
Patient and public involvement
Patients were not directly involved in this study; only data gathered retrospectively and coming from electronic health records was used.
Results
Demographic characteristics
There were 18 851 MSM attending MSHC for the first time between 2011 and 2018. We excluded 1909 MSM (10.1%) who had had sexual contact with another man but declined to report the number of male sexual partners, 1630 MSM (8.6%) who reported no male sexual partner in the past 12 months at the current visit but had reported male partners at subsequent visit at the clinic and 538 (2.9%) duplicate records from the same individual on the same day. The remaining 14 774 men were included in this data analysis, and the number of men increased from 1215 in 2011 to 2468 in 2018 but the proportion of MSMO and MSMW remained stable over the period (table 1). Overall, there were 12 795 MSMO (86.6%) and 1979 MSMW (13.4%). Among 1979 MSMW, 804 (40.6%) were MSMW-W, 839 (42.4%) MSMW-M and 336 (17.0%) had an equal number of male and female partners in the past 12 months.
Number of men who have sex with men attending the Melbourne Sexual Health Centre between 2011 and 2018, stratified by men who have sex with men only (MSMO) and men who have sex with men and women (MSMW)
Among the 14 774 MSM, the median age was 27 years (interquartile range [IQR]: 23–33) and MSMW were slightly older than MSMO (median age: 29 vs 27; p<0.001) (table 2). The proportion of men born in Australia was higher in MSMW than in MSMO (55.3% vs 48.5%, p<0.001). The proportion of injecting drug use in the past 12 months was higher in MSMW than MSMO (2.0% vs 1.6%, p=0.032; table 2); but injecting drug use was similar between MSMW-W and MSMW-M (2.5% vs 2.1%, p=0.777; online supplemental table S1).
Supplemental material
Demographic characteristics and sexual practices among men who have sex with men attending a sexual health centre in Melbourne, 2011–2018, stratified by men who have sex with men only (MSMO) and men who have sex with men and women (MSMW)
Sexual practices
The proportion of men who reported sex overseas in the past 12 months was comparable between MSMW and MSMO (37.1% vs 34.5%; p=0.060); and more MSMW-W (43.0%) reported sex overseas than MSMW-M (34.6%; p=0.002) (online supplemental table S1). Less than half (40.1%) of MSMO had a male regular partner. Among MSMW, 8.5% had a regular male partner, 33.5% a regular female partner, and 4.6% had regular male and female partners (table 2).
The median number sexual partners (regardless gender of the partners) in the past 12 months, was higher among MSMW (7, IQR: 5–12 in MSMW-M; and 6, IQR: 4–11 in MSMW-W) than MSMO (5, IQR: 3–10; p<0.001) (online supplemental table S1). The proportion of men with ≥5 sexual partners increased significantly in MSMW (from 63.1% in 2011 to 70.2% in 2018, ptrend=0.014), as well as in MSMO (from 50.8% to 56.4%; ptrend=0.002) (online supplemental tables S2 and S3). In addition, the proportion of MSMW with ≥5 female sexual partners increased significantly from 23.2% in 2011 to 29.5% in 2018 (ptrend=0.039) (online supplemental table S3).
Anal sex practices with casual male partners varied between MSMO and MSMW. The proportion of MSMO having RAS only with casual male partners was higher (9.9%) than in MSMW (6.6%); however, the proportion of MSMO having IAS only with casual male partners was lower (10.5%) than in MSMW (14.2%; p<0.001). Condomless anal sex with casual male partners in the past 12 months was more common in MSMO than in MSMW for RAS (53.8% vs 49.9%; p=0.012) but there was no significant difference in IAS. Two-thirds (67.5%) of MSMW had condomless vaginal and/or anal sex with female casual partners in the past 12 months (table 2). Among MSMO, condomless RAS with casual male partners in the past 12 months increased from 46.2% to 63.3% (ptrend <0.001) and IAS from 45.8% to 64.2% (ptrend <0.001) from 2011 to 2018 (figure 1 and online supplemental table S2). Similarly, among MSMW, there was an increase from 41.3% to 57.9% in condomless RAS (ptrend=0.011), the proportion of condomless IAS with casual male partners did not change during the study period (ptrend=0.087), and the proportion of condomless sex with casual female partners remained high and only increased marginally from 65.4% to 71.0% (ptrend=0.056) (figure 1 and online supplemental table S3). MSMW-M compared with MSMW-W showed higher condomless sex with casual male partners (55.0% vs 46.1% for RAS; p=0.004 and 57.0% versus 47.1% for IAS; p=0.001) and lower condomless sex with casual female partners (60.9% vs 75.6%; p<0.001) (online supplemental table S1).
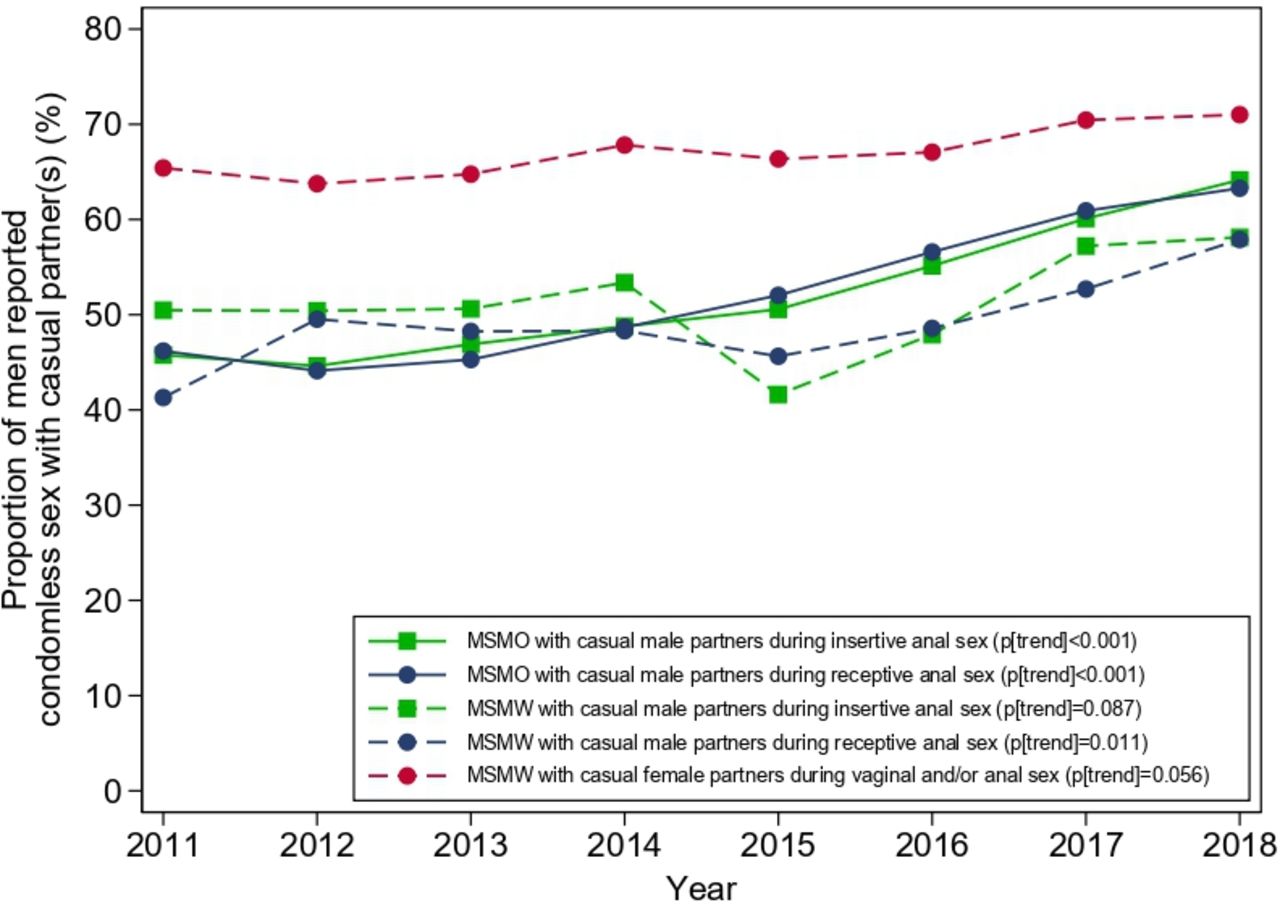
Proportion of condomless anal and/or vaginal sex in the past 12 months with casual partners between 2011 and 2018, stratified by men who have sex with men only (MSMO) and men who have sex with men and women (MSMW). MSM reporting condomless anal and/or vaginal sex includes MSM who sometimes, usually or never used a condom with their sexual partners in the past 12 months.
Regarding regular male partners, both condomless RAS and condomless IAS were more commonly reported in MSMO (RAS: 71.5%; IAS: 71.4%) than in MSMW (RAS 62.9%; IAS: 63.5%; p=0.005; p=0.010) (table 1) and condomless anal sex regardless of IAS or RAS, increased from 69.2% to 78.4% in MSMO (ptrend <0.001) but not in MSMW (ptrend=0.435) (figure 1 and online supplemental tables S2, S3).
HIV/STI positivity
Overall, MSMO had a higher HIV, syphilis, gonorrhoea and chlamydia positivity than MSMW. MSMO had higher extragenital gonorrhoea and chlamydia positivity than MSMW; however, the positivity for urethral gonorrhoea and urethral chlamydia did not differ between the two groups (table 3). In the period 2011–2014, there was an increase in oropharyngeal and anorectal and oropharyngeal gonorrhoea among MSMO, while chlamydia remained stable. There was no increase in gonorrhoea and chlamydia positivity in the period 2015–2018 in either group (online supplemental tables S4 and S5). Among MSMW, MSMW-M had higher extragenital gonorrhoea and chlamydia positivity but similar urethral gonorrhoea and chlamydia, HIV and syphilis compared with MSMW-W (online supplemental table S6).
Positivity for gonorrhoea, Chlamydia, syphilis and HIV among men who have sex with men attending a sexual health centre in Melbourne, 2011–2018, stratified by men who have sex with men only (MSMO) and men who have sex with men and women (MSMW)
There was a 43.5% increase in syphilis positivity from 5.5% (43/778) in 2011 to 7.9% (152/1917) in 2018 (ptrend=0.012) in MSMO (online supplemental table S4) and more than a sixfold increase in syphilis positivity from 0.9% (1/112) in 2011 to 6.4% (19/299) in 2018 (ptrend=0.004) in MSMW, although the number of infections remained low in this group (figure 2 and online supplemental table S5). HIV positivity did not change in either group between 2011 and 2018 (figure 2 and online supplemental tables S4,S5).

{kind=link}
{kind=link}
Positivity for syphilis and HIV between 2011 and 2018, stratified by men who have sex with men only (MSMO) and men who have sex with men and women (MSMW).
After adjusting for other potential confounding factors, MSMO had higher odds of testing positive for gonorrhoea at any anatomical site (aOR 1.36, 95% CI 1.13 to 1.64), chlamydia at any anatomical site (aOR 1.39; 95% CI 1.16 to 1.67), syphilis (aOR 1.74, 95% CI 1.37 to 2.22) and HIV (aOR 4.60, 95% CI 2.43 to 8.70) compared with MSMW (table 4). Additionally, MSMO had higher odds of testing positive for gonorrhoea at any anatomical site (aOR 1.58; 95% CI 1.15 to 2.18), chlamydia at any anatomical site (aOR 1.47; 95% CI 1.09 to 1.99), syphilis (aOR 2.11, 95% CI 1.36 to 3.27) and HIV (aOR 5.49, 95% CI 1.74 to 17.30) compared with MSMW-W in the adjusted analysis; however, there was no significant difference in HIV/STI positivity between MSMW-M and MSMW-W nor MSMW-M and MSMO (table 5).
Association between sexual practice and gonorrhoea, Chlamydia, syphilis and HIV positivity among men who have sex with men only (MSMO) and men who have sex with men and women (MSMW) attending a sexual health centre in Melbourne, 2011–2018
Association between sexual practice and gonorrhoea, Chlamydia, syphilis and HIV positivity among men who have sex with men only (MSMO) and men who have sex with men and women (MSMW) attending a sexual health centre in Melbourne, 2011–2018
Discussion
In this study of 12 795 MSM only (MSMO) and 1979 MSMW in Melbourne, Australia, we found significant changes in sexual practices among MSMW between 2011 and 2018, a period in which rates of STIs had been increasing in both MSM and the heterosexual population. Specifically, we found that condom use with casual female partners remained low during the study period and that condomless anal sex with casual male partners had increased in MSMW, and these results echo the rise in syphilis positivity over the same period. While some sexual risk practices and STI positivity were generally lower in MSMW than in MSMO, their rising rates could indicate more transmission from MSMW to their female partners than had occurred previously. Clarifying this issue and what factors are causing the rising rates of STIs is likely to contribute significantly to the design of STI control programmes.
Several studies have assessed HIV and sexual practices in MSMW, but their results are conflicting. A meta-analysis published in 2014 concluded that MSMW had a lower HIV prevalence (16.9%) compared with MSMO (33.3%) but the prevalence is higher than men who have sex with women only (3.5%), and this is consistent with our findings.19 The authors also found that MSMW (15.9%) were less likely to engage in condomless RAS compared with MSMO (35.0%).19 Other factors such as drug and alcohol use, other risky practices (eg, group sex, paying for sex), frequent HIV testing and the use of biomedical interventions (eg, pre-exposure prophylaxis and post-exposure prophylaxis) are also associated with HIV acquisition,20–22 and very limited studies examining these factors between MSMO and MSMW. However, some other studies conducted in different settings, such as China, India and the USA, have shown the risk of HIV among MSMW is similar or even at a higher risk compared with MSMO.13 23–25
Our data suggest that MSMO have a higher positivity for syphilis, chlamydia and gonorrhoea than MSMW; however, the comparison of STI positivity between MSMO and MSMW varies across published studies. For example, Davis et al conducted a study among Chinese MSM showing no differences between MSMW and MSMO in the lifetime prevalence of syphilis, gonorrhoea, chlamydia and genital warts but a higher prevalence of genital herpes in MSMW (6.6%) compared with MSMO (0.4%).25 In the USA, MSMW had a 57% increased odds of having an STI compared with heterosexuals, but no differences were found between MSMO and heterosexuals or MSMO and MSMW.24 Similarly, an Indian study has shown that there were no differences in any STI positivity (ie, either syphilis, gonorrhoea or chlamydia) between MSMO and MSMW.23 Furthermore, MSMW are also less likely to ever have an HIV/STI test compared with MSMO,23 26 27 which is consistent with an Australian qualitative study suggesting MSMW have a poor sexual health knowledge compared with MSMO.28 Furthermore, the rise in antimicrobial resistance in STI,29 particularly gonorrhoea, is of particular concern. Transmission of antimicrobial resistance across risk populations (eg, between MSMW and female) may have occurred.30 31
Our data also show that MSMW are less likely to have RAS with male partners and less likely to have condomless RAS. These findings may explain the reasons why MSMW have a lower positivity for anorectal gonorrhoea and chlamydia than MSMO in our study. Importantly, we did not find any significant differences in urethral gonorrhoea and chlamydia between MSMO and MSMW despite differences in anal sex and condom use. This may be because some urethral chlamydial infections in MSMW are acquired from women and urethral gonorrhoea is commonly acquired from no anal sexual activity such as oral sex.32 33 The disparities of HIV and syphilis positivity between MSMO and MSMW were more pronounced compared with gonorrhoea and chlamydia, and there was a striking increase in syphilis positivity in both groups.
The differential sexual practices and HIV/STI positivity among MSMW34 35 may also be due to other health issues such as mental health and substance use, that also place them as an especially vulnerable population.36 37 Bisexual men may face unique stressors, such as specific prejudices against them, pressures or negative attitudes from both heterosexual and lesbian, gay, bisexual, and transgender (LGBT) individuals, which can have a negative impact on their health.37 38 This factors may also render bisexual men less likely to discuss their sexual health and disclose their sexual orientation with their general practitioners14 and, hence not receive the appropriate sexual healthcare and management. An LGBT-friendly and non-judgemental approach is essential to build up the trust between clinicians and patients. Furthermore, the current health promotion and prevention programmes mainly targeting the MSM population as a whole. It is possible that some MSMW may not be engaged in the LGBT community and hence they may not targeted with the current programmes. Future public health campaigns and prevention programmes should also tailor for MSMW via different channels.
Our study, including a high number of MSM over an 8-year period, provides relevant and updated information to understand changes in sexual practices and STI epidemiology occurring in Australia and across the world. We also provide detailed information regarding condom use, differencing between both casual or regular partners and RAS or IAS. Nevertheless, there are several limitations in the study that must be considered. First, data were self-reported by MSHC clients which may influence the results regarding sexual practices, including the number and gender of the sexual partners due to social desirability or recall bias. However, the use of a CASI to collect sexual history at the clinic has shown to improve the accuracy and reduce biased information. Besides that, data on sexual orientation were not collected and the categorisation of MSMO and MSMW was based on self-reported sexual practice rather than sexual identity. This means that MSMW in this study might not define themselves as bisexual men. Second, this study was conducted in one urban major sexual health clinic. It is possible that MSM attending a sexual health clinic are more likely to be at increased sexual risk and hence our findings may not be generalisable to the whole MSM population in Australia or in other settings. Third, other sexual practices that may increase the risk of HIV/STI (eg, chemsex, group sex, rimming or saliva use as a lubricant)39–42 were not routinely collected in the clinic and hence not included in the study. Fourth, we only included individuals who attended the clinic for the first time. Sexual practices might change with age and further longitudinal cohort studies examining the changes in sexual practices among individuals would be required. Lastly, we were unable to examine the temporal trends for gonorrhoea and chlamydia over the 8-year period because we changed the diagnostic test for gonorrhoea and chlamydia at our clinic in 2015.
Conclusion
In our study population, MSMW were a heterogeneous group in which sexual practices and STI positivity varied between MSMW with mainly female partners and MSMW with mainly male partners. Compared with MSMO, MSMW were less likely to engage in condomless sex and had a lower HIV/STI positivity. From 2011 to 2018, changes in the sexual practices in MSM have affected both MSMW and MSMO leading to an increased risk of STI in both subgroups. Further studies also including heterosexual men and women are needed to better understand the recent changes in the STI epidemiology.
Acknowledgments
The authors would like to acknowledge Afrizal Afrizal for his assistance with data extraction at the Melbourne Sexual Health Centre.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @mmsanchz
Contributors EPFC and CF planned, conceived and designed the study. RC conducted some preliminary analyses. MM-S performed the literature review, conducted the statistical analysis and wrote the first draft of the manuscript. EPFC provided statistical advice and oversaw the study. RC, CF, JSH, CB, JO, MYC and EPFC assisted with data interpretation. MM-S, RC, CF, JSH, CB, JO, MYC and EPFC critically revised it for important intellectual content and approved the final version of the manuscript.
Funding EPFC is supported by an Australian National Health and Medical Research Council (NHMRC) Emerging Leadership Investigator Grant (GNT1172873). CKF is supported by an Australian NHMRC Leadership Investigator Grants (GNT1172900).
Disclaimer The funder had no role in the study design, collection of data, writing, or decision to submit the paper for publication.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the Alfred Hospital Ethics Committee, Melbourne, Australia (project number 83/18).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as online supplemental information.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.