Article Text

Abstract
Dandy-Walker syndrome (DWS) is a group of brain malformations which sometimes present with psychotic symptoms. We present the case of a patient diagnosed with Dandy-Walker variant who presented with schizophrenia-like psychosis. A man in his 30s was admitted to an acute psychiatric unit presenting with persecutory delusions, auditory hallucinations and violent behaviour. The MRI performed showed the typical alterations of Dandy-Walker variant: vermian hypoplasia and cystic dilatation of the fourth ventricle. He also suffered from mild intellectual disability. After being treated with olanzapine 10 mg/d for a month, his psychotic symptoms greatly improved and he was discharged. In conclusion, DWS may cause psychosis through a dysfunction in the circuit connecting prefrontal, thalamic and cerebellar areas. The association between these two conditions may contribute to the understanding of the aetiopathogenesis of schizophrenia.
- psychotic disorders
- schizophrenia
- schizophrenia spectrum and other psychotic disorders
- cerebellar vermis
- cerebral ventricles
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- psychotic disorders
- schizophrenia
- schizophrenia spectrum and other psychotic disorders
- cerebellar vermis
- cerebral ventricles
Introduction
Dandy-Walker syndrome (DWS) is a group of brain structural abnormalities that includes four subtypes: Dandy-Walker malformation, mega cisterna magna, posterior fossa arachnoid cyst and Dandy-Walker variant.1
Dandy-Walker variant is the mildest form and is characterised by vermian hypoplasia and cystic dilatation of the fourth ventricle. Its clinical presentation typically consists of intellectual disability and epileptic seizures, although some patients may remain asymptomatic. Diagnosis is based on neuroimaging tests, mainly MRI. There is currently no curative treatment and, consequently, therapeutic strategies focus on its symptoms and complications.2
Occasionally, psychotic symptoms and other psychiatric disorders have been reported to occur in patients with DWS.3–18 However, the prevalence and clinical features of this comorbidity have not been established yet, and the literature about the topic is scarce. This is not the only neurological condition that presents with psychiatric comorbidities: several brain alterations, both structural and pathophysiological, can result in psychiatric symptoms.19 Moreover, neurodevelopmental factors have been found to be involved in the aetiology of schizophrenia,20–22 and the cerebellum appears to play an important role in this process.23–26
Here we present the case of a patient diagnosed with Dandy-Walker variant who presented with schizophrenia-like psychosis. The identification and description of such cases is of clinical relevance, since Schizophrenia-like symptoms induced by neurological conditions may present clinical features that differentiate them from primary schizophrenia, which may result in the need for different treatment approaches. Further on we present a narrative review of the association between psychosis and DWS, which, to our knowledge, is the first review conducted on the topic.
Case presentation
A man in his 30s was admitted to an acute psychiatric unit after presenting with delusions and violent behaviour.
The patient had been diagnosed with Dandy-Walker variant as a child, manifesting as mild cognitive impairment and epileptic seizures. Electroencephalogram had revealed the presence of a rolandic focus, and MRI studies had shown vermian hypoplasia and dilatation of the fourth ventricle. He was treated with valproate for several years until seizures stopped around the age of 15 years. He lived with his mother, had no friends and worked as a janitor in a primary school.
A year prior to his admission, he started to feel suspicious of his neighbours and thought the children in the school where he worked made fun of him. He occasionally manifested aggressive behaviour, insulting and threatening his neighbours. The day before his admission, at the age of 32, the patient stepped into a school class wielding a knife and threatened the children and their teacher. He was arrested but was declared legally unaccountable after forensic psychiatric evaluation. He was transferred to the emergency room and later admitted to a psychiatric emergency ward.
At admission, the patient presented with persecutory delusions, claiming that the schoolchildren and other townspeople were planning to end his life and defended his actions as self-defence. He also presented with auditory hallucinations, claiming he could hear the voices from the deceased with whom he talked daily. He did not display thought disorder, but some limitations in abstract thinking and a mild intellectual disability (Wechsler Adult Intelligence Scale III score of 65) were evident on examination.
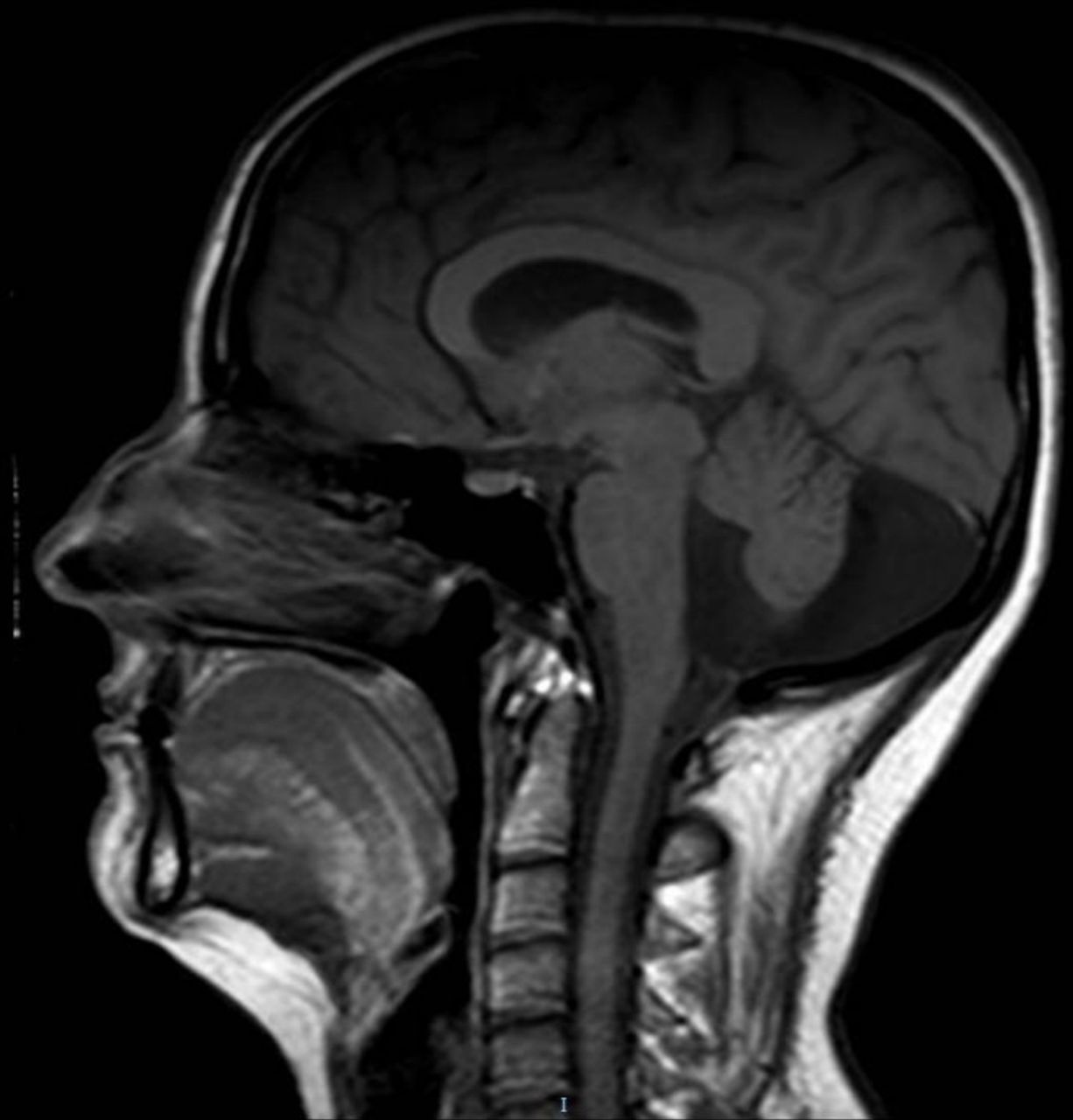
The patient gave written informed consent to all diagnostic procedures and allowed us to use the available data for scientific reports. An MRI was performed, showing the typical alterations of Dandy-Walker variant. No other alterations were found (figure 1).
{kind=link}
Midsagittal magnetic resonance T1-weighted scan shows cystic dilatation of the fourth ventricle and vermal hypoplasia.
He was treated with olanzapine 10 mg/d. Apart from mild sedation, which decreased after the first week, he tolerated the medication. His psychotic symptoms greatly improved a month after admission, with full remission of auditory hallucinations and a reduction from 87 to 51 in the Positive and Negative Syndrome Scale (PANSS). His delusions persisted but greatly decreased in intensity. He was discharged from the hospital and his care was transferred to his local mental health outpatient team.
Discussion
This case illustrates the association between Dandy-Walker variant and schizophrenia-like psychosis.
To review the association between DWS and psychosis, we carried out a search on the MEDLINE database using the terms [(Psychosis OR Schizophrenia) AND Dandy-Walker], in all fields, without filter restrictions.
The initial search generated 17 articles, of which 12 were included in the review, while the other 3 were discarded due lack of relevance or unavailability. Searching the references of these articles, we found three additional studies. A total of 15 articles, reporting 19 patients, were included in the review.
Fifty-three percent of the patients were female. The mean age of onset of psychosis was 23 years. Dandy-Walker variant was the subtype more frequently associated with psychosis. Additional psychiatric comorbidities, such as obsessive-compulsive disorder, post-traumatic stress disorder or mania, were described in some of the cases. Atypical antipsychotics were the main treatment for psychosis in most of the cases reviewed. Complete results are shown in table 1.
Articles that include cases report of DWS with comorbidity with psychiatry symptoms
A coincidental association between DWS and psychosis cannot be ruled out. However, the high number of cases of comorbidity reported, considering the rareness of the condition, suggests a causal relationship.
DWS may cause psychosis via its cerebellar alterations, which may explain why Dandy-Walker variant, characterised by vermian hypoplasia, is the subtype more strongly associated with psychosis, despite being the milder condition of the group. Some studies have shown a smaller vermian volume and other cerebellar alterations in patients with schizophrenia.22–25 According to the model proposed by Andreasen et al, psychotic symptoms may be the result of a dysfunction in the circuit connecting prefrontal, thalamic and cerebellar areas, a neurodevelopmentally derived ‘misconnection syndrome’ that would result in ‘cognitive dysmetry’, which has been described as a difficulty in prioritising, processing, coordinating and responding to information. According to this, a ‘poor mental coordination’ may explain both the cognitive deficits of schizophrenia and the wide range of symptoms. They opined that a decrease in the Purkinje cell size and decreased excitatory input to them from the granule cells have major implications that explain cerebellar and corticocerebellar–thalamic–cortical circuit dysfunction in schizophrenia and related abnormalities in symptoms and cognition.21 We think that these findings could predispose the occurrence of the other mentioned psychiatric disorders (table 1).
In conclusion, this case report provides further evidence linking DWS with psychosis. Considering these findings, some clinical features seem to be common in this kind of psychosis: earlier age of onset, higher prevalence of treatment resistance and frequent comorbid intellectual disability. One of the challenges that this condition poses is that of differentiating which symptoms are related to psychosis and which are caused by the primary neurological condition, especially in the case of intellectual disability, since it can often be mistaken for negative symptoms. Additionally, the management of non-psychiatric complications of DWS can improve the patient’s general well-being.
Despite the body of evidence linking schizophrenia to brain abnormalities, current Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, diagnostic criteria for schizophrenia exclude this diagnosis when symptoms are considered to be caused by a neurological condition. Thus, we must refer to this entity as schizophrenia-like psychosis, even if the rest of the criteria for schizophrenia are met. As research advances and the aetiology of schizophrenia become clearer, the boundary between primary and secondary schizophrenia may become blurrier.26 27 Further research is needed to establish the prevalence and characteristics of psychotic symptoms in patients with DWS. This association may contribute to the understanding of the aetiopathogenesis of schizophrenia.
References
Alejandro Porras-Segovia completed her medical training at the University of Granada in Spain. She has made four university degrees from the University of Alcalá de Henares in Mental Health Emergencies and Affective Disorders, University of Granada in Neuroscience and Pain, International University of Valencia in Third Generation Psychotherapies and University of La Rioja in Sanitary Management and Direction. Currently she is developing her PhD in Clinical Medicine and Public Health. She is also working as a psychiatrist specialist in the Virgen de las Nieves Hospital (Granada). Alejandro performed the specialization via Médico Interno Residente in psychiatry in the Granada Sur Clinical Management Area, working a posteriori in the Community Mental Health Unit in this área for a year. Her main research interests include clinical Neuroscience and Health.

Footnotes
Contributors All the authors have been clinically involved in the planning, conducting, reporting, writing, reviewing and publishing of this case. The patient consented to publish this clinical case.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.