Article Text

Statistics from Altmetric.com
Introduction
The pediatric population spans a diverse age group,1 from neonates and infants to adult-sized teenagers, each with unique physiological characteristics that must be considered when performing diagnostic cerebral angiography (DCA). Herein we refer to pediatric patients as under the age of 18 years. Neonates will not be discussed further due to the very limited role of DCA in the absence of planned neurointervention, most commonly for vein of Galen malformations and other high-flow arteriovenous fistulas leading to life-threatening heart failure.
The number of pediatric neuroangiography procedures performed continues to grow2 and it is evident that the technical aspects of performing pediatric DCA are highly variable among practitioners, including our own Task Force members. This reflects the diversity of angiographers from different specialties and the varying levels of prior pediatric neuroangiography training and experience. In 2019, the Society of Neurointerventional Surgery (SNIS) surveyed its membership regarding their individual fellowship training and current practice as it relates collectively to pediatric neuroangiography, including both diagnostic and interventional procedures. Unpublished results indicate that pediatric neuroangiography training and current experience is limited across the nation (figure 1). Most respondents (94%) performed pediatric DCA during fellowship, though this experience was mostly limited and low volume. In children under 4 years of age, that experience was further reduced (40%: 0–10 cases; 45%: 11–49 cases). Despite this limited exposure, 76% of respondents reported currently treating pediatric patients, though in more than half (53%), that volume remains low: 0–10 pediatric cases per year. Practice guidelines for cervicocerebral catheter angiography have been published for adults,3 however, no similar recommendations exist for children. Given this information, Pediatric Neurointerventional Task Force Committee members of the SNIS sought to provide a framework with which safe pediatric DCA can be performed, detailing specific procedural considerations as well as peri-procedural evaluation and care.

Results from a 2019 SNIS membership survey on pediatric experience. 78 members of the SNIS responded to a 13-question survey on fellowship training and current practice involving pediatric patients. Number of cases performed includes both diagnostic and interventional angiographic procedures and sclerotherapy procedures for vascular malformations.
Despite widespread availability and advances in noninvasive vascular imaging, DCA remains a valuable diagnostic tool and is commonly performed to delineate the angioarchitecture of, and hemodynamic flow patterns for, many cerebrovascular pathologies including stroke, vasculopathy (ie, moyamoya), arteriovenous malformations, arteriovenous fistulas, and aneurysms. DCA has a low complication rate4 5 and maintaining this safety profile in children is an expectation for practitioners performing this procedure. This is predicated on supplementing prior training and experience with a sustained, consistent volume of pediatric cases, while paying special attention to the important nuances herein described.
Before the procedure
Pre-procedure evaluation
It is critical to review pertinent prior neuroimaging studies and confirm that DCA is indicated. For healthy children without other medical problems, a recent routine history and physical examination, (ie, 30–90 days prior) by their primary care or referring physician suffices for medical evaluation prior to DCA. This information can be updated during the immediate pre-procedure evaluation by the anesthesia and neuroangiography teams on the day of the DCA. Children with cardiopulmonary disease, complex medical histories, or with a history of difficult airway should also be assessed in a pre-operative anesthesia clinic for medical optimization. In select higher-risk patients, such as children with sickle cell anemia and critical arterial stenoses such as moyamoya, additional precautions may need to be implemented, such as preadmission the night prior to the procedure and supplemental hydration while nil per os (NPO). In addition, children with sickle cell anemia may also need a blood transfusion (eg, target hemoglobin of 10 g/dL) to help avoid a sickle cell crisis.
Routine laboratory tests are not universally required for all children undergoing DCA. A complete blood count, basic metabolic panel, and a coagulation profile should be considered in the subset of children with other medical comorbidities and history of coagulopathy, long-term medication intake, or substance abuse. Routine pregnancy testing is required after the onset of menstruation in females.
Contrast allergy risk and prophylaxis
Allergic reactions to contrast media are independent of contrast dose and occur in less than 3% of cases in adults.6 In children, the incidence is estimated to be lower with one study of 11 306 pediatric intravenous (IV) contrast injections reporting an allergic contrast reaction rate of 0.18%.7 Reactions may range in severity from hives, itching, urticaria rash, and wheezing to more serious reactions including angioedema, bronchospasm, or anaphylaxis, and are reportedly less frequent with low-osmolar non-ionic contrast media, which are the agents of choice.6 Several prophylaxis regimens exist to minimize the risk of an allergic reaction, and an example is provided in table 1.
Contrast allergy prophylaxis
Contrast agents
The risk of contrast agent-induced nephropathy in children is low, dose-dependent, and decreases with the use of non-ionic, low-osmolar agents.6 Although higher limits up to 8 mL/kg have been reported for endovascular interventions in the setting of urgent conditions,6 DCA can and should be performed using low volumes of contrast (2–4 mL/kg). This can be achieved by tailoring the examination to minimize both the number of vessels catheterized and the number of contrast injections per vessel. Diluting the contrast medium with saline (1:1, that is, half strength) is another effective way to reduce the contrast dose administered while maintaining diagnostic image quality. Adequate oral or IV pre- and post-procedure hydration may also help reduce the nephrotoxicity risk. Sodium bicarbonate infusion and administration of acetylcysteine can be considered to further mitigate the nephrotoxicity risk in select patients, although their use has not been validated in the pediatric population.8 Factors that increase the risk of nephrotoxicity include pre-existing renal impairment, dehydration, diabetes mellitus, heart failure, hyperuricemia, and use of nephrotoxic drugs.
Consent process
A family-centered approach is a core value of pediatrics, and key components of the procedure must be effectively communicated in order to achieve informed consent. The family and the patient, if age-appropriate and mature, should understand the cerebral angiogram in detail including its potential risks, benefits, and alternatives, as well as expected outcomes and the use of general anesthesia. Parents may have different preferences for the degree to which their child participates in this process. Children are often focused on specific aspects of the procedure such as when they can eat, how long they need to lie flat, and when they can resume physical activity.
Fasting and oral medication guidelines
Pre-procedural fasting guidelines vary among institutions and are constantly evolving9 to decrease the duration during which a child is NPO, as prolonged fasting may cause dehydration with subsequent hypotension.10 11 The patient and caregivers should receive clear instructions regarding essential oral medication use around the procedure, such as antiepileptics, aspirin, or anticoagulants.
Procedural considerations
General anesthesia
In select circumstances, mature middle adolescents (15–17 years)1 may be considered candidates for conscious sedation, if they are cooperative, calm, and can reliably remain motionless during frequent breath holds. Barring that, we recommend the use of general anesthesia (GA) for all pediatric DCAs, with few exceptions, such as a WADA test and balloon test occlusion (if performed with awake neurological testing). GA with the use of a paralytic agent eliminates unexpected body motion, improves image quality, and allows for safe and precise catheter maneuvers, likely shortening the duration of the procedure.2 11 While most of the authors use general endotracheal anesthesia (GETA) for DCA, some have advocated for the use of a laryngeal mask airway (LMA). Choosing between GETA and the use of an LMA is a decision to be made by the individual anesthesia and neuroangiography teams, ensuring that the LMA provides reliable airway protection and minimizes the risk of potential bronchospasm.12–15
As a part of a pre-procedure checklist (table 2) and time-out protocol, the neuroangiographer and anesthesiologist should establish open and free communication to discuss key components of the procedure as well as post-procedure care. This includes blood pressure control and fluid management, which are potential critical challenges during the induction and maintenance of GA, and which are particularly important in vulnerable patient cohorts, such as those with moyamoya. Physiologic hemodynamic parameters including pulse oximetry, blood pressure, heart rate, and end-tidal capnometry should be monitored in all children under GA. An arterial line and foley catheter are not routinely indicated for elective DCA, however, their use may be considered in critically ill patients. Monitoring and maintaining temperature control is also crucial, especially in the youngest children, who may lose body heat quickly. Use of a supplemental external warming device, a tabletop warmer, and raising room temperature are all methods to maintain warmth. Routine use of antibiotics prior to groin puncture for vascular access is not recommended.
Pre-procedure checklist
Vascular access
The common femoral artery is the recommended access site for pediatric DCA. In small children and when the femoral pulse is difficult to palpate, real-time ultrasound is a useful adjunct to visualize the common femoral artery and its bifurcation into the superficial and deep femoral arteries. The SNIS Standards and Guidelines Committee produced a report on transarterial and transvenous access,16 in which several recommendations are made including some for pediatric patients. Transradial access has been reported as feasible in children undergoing neuroangiography procedures, though this recent multicenter study also reports high rates of clinically significant radial artery vasospasm (13.1%) that restricted catheter movements and an 8.2% conversion rate to femoral access.17 Although there is a trend for increasing use of radial access in adults, we do not recommend this access route for pediatric DCA except for rare circumstances, such as in bilateral femoral artery occlusion or unrepaired severe aortic coarctation.
A 4-French pediatric micropuncture set that includes a 4 cm (or 7 cm for older children) micropuncture needle is used to perform a single wall puncture. The delicate tissue requires smooth, gentle advancement of the micropuncture wire into the common femoral, external iliac, and common iliac arteries. The slightest resistance to wire advancement should prompt one to assess the micropuncture wire position fluoroscopically and redirect the wire as needed. Multiple repeated attempts to gain access and forceful technique should be avoided. A saved fluoroscopic image showing the access point and expected arterial course of the micropuncture wire is sufficient for documentation (figure 2). Dedicated femoral angiography should be reserved for situations in which there is a concern for an access-related complication or in the less frequent case of a planned closure device. For the latter, a saved fluoroscopic scene after contrast injection or femoral roadmap may be sufficient and reduces radiation exposure. Complications related to vascular access include vasospasm, hematoma, pseudoaneurysm, retroperitoneal hemorrhage, vascular occlusion, and limb ischemia. High rates of femoral artery spasm and subsequent occlusion (9.6%) had been previously reported in small children undergoing cardiac catheterization18, however, amalgamated data from the existing literature on DCA in children found a far lower rate of local groin complications (2.8%, 18 out of 653 patients),19 and this should be the expectation for practitioners performing pediatric DCA. Beyond technique itself, a critical feature in the risk of developing vasospasm and subsequent occlusion is the diameter difference between the parent vessel and the sheath or device placed,20 which underscores the need to choose the smallest system that can accomplish the goals of the study.

{kind=link}
{kind=link}
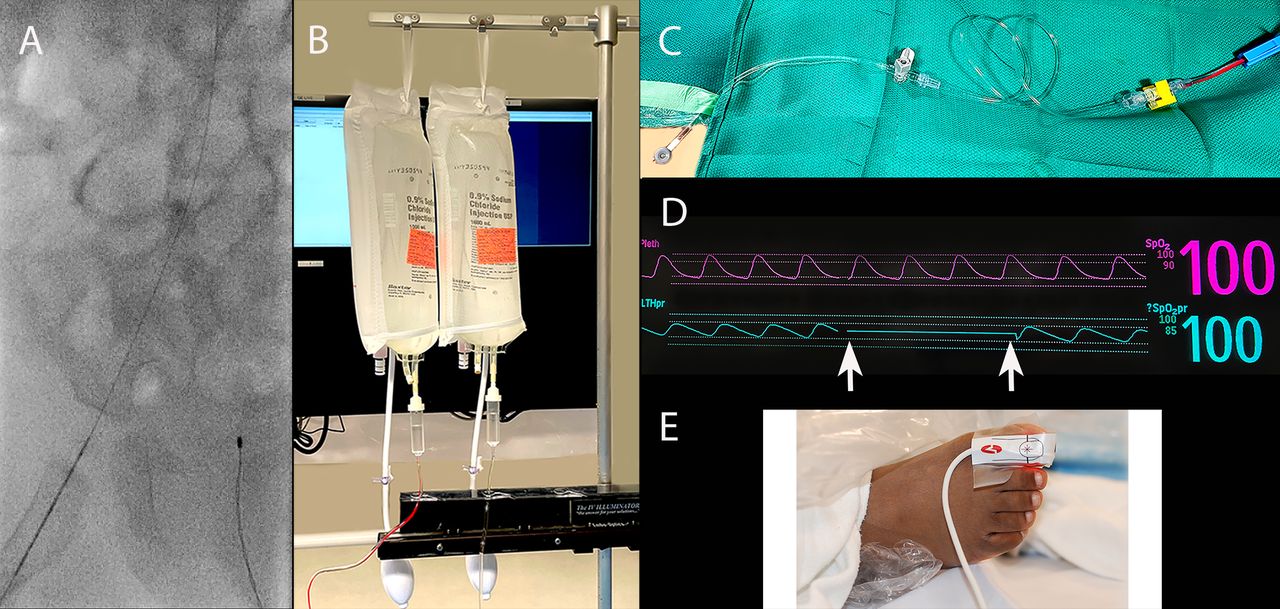
Femoral access-related considerations. A). Saved fluoroscopic image showing the micropuncture needle tip (arrow) over the femoral head and the wire coursing to the patient’s left along the expected arterial course. B). Pressurized heparinized saline flush bags are labeled with the heparin concentration. Note the drip chambers are incompletely filled to permit visualization of flow rate through the tubing. Vigilance is required to ensure that the lines are bubble-free. C). The femoral sheath is inserted in the direction of the tubing directed to the flush bags. Care is made to avoid rotating the sheath after insertion. An intervening flow-limiting device is in place between the sheath and heparinized saine. D). Example of normal waveform and it’s flattening (between white arrows) during manual compression when excessive pressure is applied. E). A pulse oximeter placed on the great toe of the foot ipsilateral to the femoral sheath allows for monitoring and titration of the level of compression for hemostasis.
Femoral sheaths
Routine use of a femoral arterial sheath is recommended as it securely maintains arterial access, minimizes manipulation at the femoral access site, and has a reported lower incidence of bleeding at the puncture site.21 Attention should be paid to avoid rotating the femoral sheath after insertion to minimize the risk of vessel injury, particularly in the youngest infants when the difference between the femoral artery diameter and sheath outer diameter (OD) is smallest. Routine DCA and many neurointerventional procedures can be successfully performed using a 4-French system.22 The 1.96 mm OD of a conventional 4-French sheath, however, may still be too large for some of the smallest infants. Newly developed thinner walled 4-French sheaths designed for radial access can be used for femoral access in children. Advantages include the smaller OD (1.78 mm) without compromising inner diameter, allowing for the use of the existing array of 4-French diagnostic catheters. A recent study on the variation in the OD of common vascular sheaths used in pediatric cardiac catheterization showed that radial sheaths, as a class, have ODs 1-French smaller than the OD of conventional sheaths. Interestingly, the OD of the 4-French Prelude Ideal radial sheath (Merit Medical) was found to be smaller than the ODs of both the 3-French (Galt Medical) and 3.3-French (PediaVascular) conventional sheaths, specifically designed for pediatric use.23
Heparin
After femoral access is obtained, the arterial sheath is flushed with heparinized saline and connected to a flow control device limiting the infusion rate through the sheath (figure 2), thereby preventing the inadvertent administration of large volumes of heparinized saline. A systemic heparin bolus of 20–60 units/kg is recommended by most Task Force members to reduce the risk of femoral artery thrombosis and catheter-related thrombus formation. This IV bolus dose should also take into account the duration of the procedure and the dose of heparin infused when using a continuous saline flush system, as heparin is also added to the saline flush bags. Heparin doses vary between 1000 and 4000 units of heparin per 1 L normal saline with lower heparin concentrations used in younger and smaller children: for example, 2000 units of heparin/L NS for those weighing less than 40 kg.
Contraindications to, and precautions for, bolus administration of IV heparin include hypersensitivity, uncontrolled bleeding, recent hemorrhage, thrombocytopenia, severe hepatic, biliary, or renal dysfunction, and recent surgery. Even in these circumstances (except for children with hypersensitivity), the continuous catheter flush solution should be heparinized. Patients with heparin-induced thrombocytopenia should not receive heparin. Argatroban, a synthetic direct thrombin inhibitor, has been used as an alternative anticoagulant in these patients. However, as with many other agents, its safety and effectiveness have not been established in children.
Closed heparinized saline flush systems
Continuous pressurized flush systems (figure 2) maintain a constant flow through the catheter and may result in less stagnation and less blood loss. Their use, however, requires vigilant monitoring throughout the entire procedure to ensure adequate antegrade flow of bubble-free heparinized saline. Operators must be cognizant of the volume of injected contrast and infused heparinized saline throughout the procedure in order to minimize the risks of nephrotoxicity, volume overload, and hazardously elevated levels of circulating heparin particularly in the smallest children.
Stroke related to iatrogenic embolization is very rare, reported in 14 of 1581 (0.9%) pediatric patients undergoing cerebral angiography in a 1981 study,24 with zero or near zero rates reported in several more recent pediatric series.4 5 25 As for groin complications, near zero rates of thrombotic complications from DCA should be the expectation for practitioners performing DCA in children.
Radiation dose
A commitment to radiation protection is a cardinal responsibility for any physician performing cerebral angiography in children, equally as important as the technical aspects of the angiogram itself. Children are more sensitive to stochastic radiation dose effects than adults and implications of this increased vulnerability have been recently described.26 Reported radiation doses for DCA range from 350 to 4100 mGy27 and this wide variability is largely explained and controlled by operator technique. While intrinsic patient characteristics cannot be altered, default manufacturer settings and operator practices (table 3) can be modified and are highly effective in decreasing radiation dose. Numerous studies highlight specific techniques28 that can reduce radiation exposure to children by up to 65%.29
Factors and techniques for reducing radiation dose
DCA in children should be performed using modern biplane angiography systems equipped with flat-panel detectors. These systems have incorporated advanced technology that includes hardware and software features that enable dose reduction while maintaining diagnostic image quality. Neuroangiographers should be familiar with their equipment configurations and work closely with their radiation physicist, vendor applications specialists, and engineering support to optimize dose settings and create dedicated pediatric protocols. During and after each case, delivered radiation dose parameters (Ka,r in mGy, PKA in μGym2, and fluoroscopy time) should be routinely monitored and recorded.30 Establishing one’s typical baseline dose parameters for DCA is a valuable practice that allows one to detect and react quickly to anomalously high doses.
Rotational angiography
Flat-panel CT (FPCT) and 3D or 4D rotational angiography are valuable techniques that may help define anatomic relationships more clearly than conventional 2D angiography alone and may reduce the need for additional 2D imaging.31 In children, the additive value of these applications must be carefully considered as their use entails additional radiation exposure and contrast administration. In terms of contrast, typical rotational angiography injection protocols require more contrast (eg, 18–21 mL for a carotid injection) compared with a standard 2D injection, which may limit the remaining contrast dose available for completion of the DCA. Protocols can be further tailored using lower radiation dose protocols32 and various dilutions of contrast (eg, 25% for FPCT, 50% for 3D studies) in order to meet the imaging needs and stay within contrast dose limitations.
After the procedure
Hemostasis
Non-occlusive manual compression at the femoral access site for a total of 15–20 min is the preferred technique for achieving hemostasis with few exceptions for adult-sized teenagers in whom a closure device may be considered. If use of a vascular closure device is planned, one may consider devices that achieve hemostasis without leaving an indwelling intra-vascular component.33 In small children, attention must be paid to avoid sustained occlusion beyond 1–2 min after removing the femoral sheath in order to minimize the risk of femoral artery occlusion and limb ischemia. A pulse oximeter placed on the ipsilateral great toe can be monitored during compression and used to titrate the degree of compression in order to avoid bleeding at the femoral access site while maintaining a normal arterial waveform (ie, “patent hemostasis”) (figure 2).
Bed rest
Recovery after DCA via a femoral approach involves a variable duration of bed rest with leg immobilization. A conservative approach is a 4-hour period of bedrest after removal of a 4-French sheath when hemostasis is achieved by manual compression. There are, however, reports in adults suggesting that a shorter period of 2–3 hours is sufficient.34 Limiting knee and hip flexion can be aided by tightly tucking a sheet around the leg or securing a padded board to the leg in infants.
Prevention and treatment of emergence delirium or agitation
In general, age, type of anesthesia, prior reaction to anesthesia, and pre-procedural behaviors can be used to predict the possibility of emergence agitation or an uncooperative state.35 Treatment options include prolonging GA, transitioning to an infusion of sedative medications, or giving a medication bolus at the time of emergence. Recent studies have suggested that α2-adrenergic agonists, e.g., dexmedetomidine, are effective in reducing post-emergence agitation from a volatile anesthetic in both bolus and short infusion forms.35 36 These α2-adrenergic agonists are effective opioid-sparing alternatives to bolusing narcotics or agents such as midazolam and are not associated with a significant risk of respiratory depression. Adequate pain control is also an important factor to consider in reducing post-procedure agitation, especially in young patients who may have difficulty verbalizing discomfort.
Conclusion
DCA is a safe and increasingly used imaging tool that is practiced by a diverse group of operators with varying levels of prior pediatric neuroangiography training and experience. A consistent volume of pediatric cases as well as modifications in device sizes, medication dosing, radiation protocols, and technique are necessary to maintain the expected favorable safety profile. Referral to a higher-volume pediatric center or practitioner is recommended for those operators who seldom perform cerebral angiography in children.
Ethics statements
References
Footnotes
Twitter @SandraNarayanan
Contributors This work was a collective effort with all authors contributing to the design, content, and drafting of the manuscript. NC, DO, and MSP revised the manuscript for important intellectual content. All authors approved of the final version and agree to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.