Article Text

Statistics from Altmetric.com
A 47-year-old woman presented with exertional dyspnoea, cough, nausea and weight loss 2 years after a right pneumonectomy for non-small cell lung cancer. CT demonstrated marked mediastinal shift and herniation of the left lung into the pneumonectomy cavity (figure 1A). The left lower lobe bronchus was compressed between the aorta and left pulmonary artery and the oesophagus traversed a tortuous path through the right hemithorax (figure 1B). Respiratory function testing demonstrated gas trapping (residual volume/total lung capacity (RV/TLC) 51%). Flexible bronchoscopy demonstrated almost complete obstruction of the left lower lobe bronchus due to extrinsic compression (figure 2). Surgical intervention to correct the anatomical abnormalities was considered although the patient preferred ongoing conservative management due to perceived risks.

(A) Coronal CT image demonstrating marked mediastinal shift into the right hemithorax. (B) Axial CT image demonstrating left lower lobe bronchus (LLL B) compression between aorta (Ao) and the left pulmonary artery (Pa). The oesophagus (Oe) is seen within the right hemithorax.

{kind=link}
{kind=link}
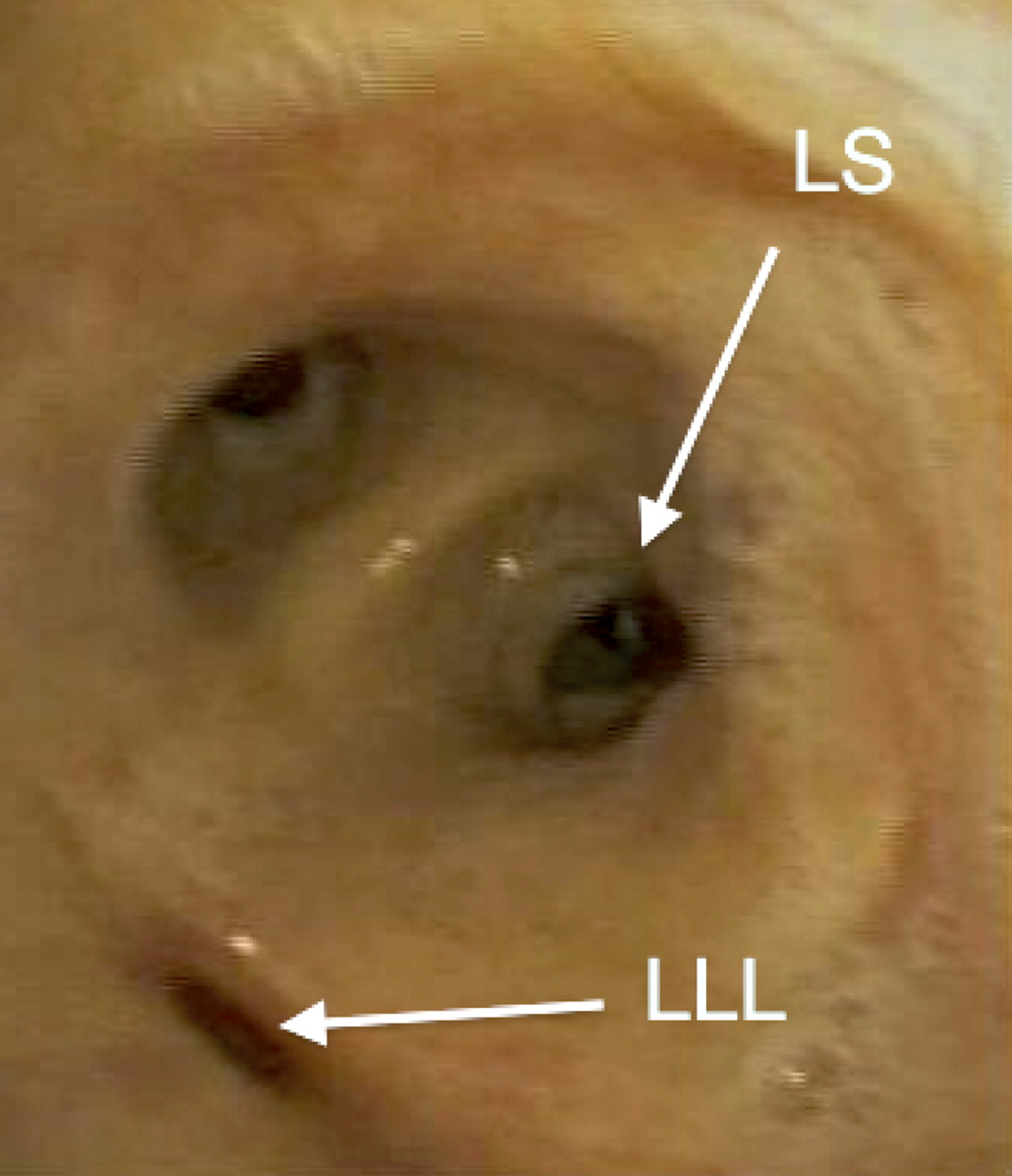
Endobronchial image from flexible bronchoscopy demonstrating marked extrinsic compression of the left lower lobe orifice (LLL) with the lingular segment (LS) and remainder of the left upper lobe visualised distal to this.
Pneumonectomy syndrome is a rare complication occurring after pneumonectomy, which was originally described in 1979.1 It is reported to occur more frequently in children, presumably due to increased tissue elasticity.2 ,3 Careful post-operative management of the pneumonectomy space may play a role in preventing excessive mediastinal shift;4 ,5 however, there are no published data examining methods to prevent this complication. Excessive traction and compression of mediastinal structures can produce gas trapping, dysphagia and reflux, recurrent laryngeal nerve palsy, tracheomalacia and vascular compromise.3 Surgical implantation of tissue expanders to reduce mediastinal shift has been reported in case series to be successful in improving symptoms and often spirometric parameters.1 ,2 ,6 Endobronchial stent placement has also been reported to provide symptomatic benefits.7
Learning points
Pneumonectomy syndrome is an uncommon complication produced by excessive mediastinal shift into the pneumonectomy space that can produce disabling respiratory and gastrointestinal symptoms.
Case series have suggested benefit from both surgical management (particularly with the use of tissue expanders placed in the pneumonectomy cavity) and endobronchial stent placement.
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.