Article Text

Abstract
Introduction Recurrent pulmonary exacerbations lead to progressive lung damage in cystic fibrosis (CF). Inhaled medications (mucoactive agents and antibiotics) help prevent exacerbations, but objectively measured adherence is low. We investigated whether a multi-component (complex) self-management intervention to support adherence would reduce exacerbation rates over 12 months.
Methods Between October 2017 and May 2018, adults with CF (aged ≥16 years; 19 UK centres) were randomised to the intervention (data-logging nebulisers, a digital platform and behavioural change sessions with trained clinical interventionists) or usual care (data-logging nebulisers). Outcomes included pulmonary exacerbations (primary outcome), objectively measured adherence, body mass index (BMI), lung function (FEV1) and Cystic Fibrosis Questionnaire-Revised (CFQ-R). Analyses were by intent to treat over 12 months.
Results Among intervention (n=304) and usual care (n=303) participants (51% female, median age 31 years), 88% completed 12-month follow-up. Mean exacerbation rate was 1.63/year with intervention and 1.77/year with usual care (adjusted ratio 0.96; 95% CI 0.83 to 1.12; p=0.64). Adjusted mean differences (95% CI) were in favour of the intervention versus usual care for objectively measured adherence (9.5% (8.6% to 10.4%)) and BMI (0.3 (0.1 to 0.6) kg/m2), with no difference for %FEV1 (1.4 (−0.2 to 3.0)). Seven CFQ-R subscales showed no between-group difference, but treatment burden reduced for the intervention (3.9 (1.2 to 6.7) points). No intervention-related serious adverse events occurred.
Conclusions While pulmonary exacerbations and FEV1 did not show statistically significant differences, the intervention achieved higher objectively measured adherence versus usual care. The adherence difference might be inadequate to influence exacerbations, though higher BMI and lower perceived CF treatment burden were observed.
- cystic fibrosis
- psychology
- nebuliser therapy
Data availability statement
Data are available on reasonable request. Requests for patient level data and statistical code should be made to the corresponding author and will be considered by members of the original trial management group, including the chief investigators and members of clinical trials research unit, who will release data on a case-by-case basis. Data will be shared following the principles for sharing patient level data as described by Tudur Smith C, et al BMC Medicine 2015;13:298 (https://doi.org/10.1186/s12916-015-0532-z). The data will not contain any direct identifiers, and we will minimise indirect identifiers and remove free-text data to minimise the risk of identification.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Key messages
What is the key question?
Can a multi-component self-management intervention increase and sustain adherence to inhaled therapies among adults with cystic fibrosis (CF) and does the intervention impact on exacerbation rates?
What is the bottom line?
The intervention did not show a statistically significant difference in exacerbation rates versus usual care but achieved higher objectively measured adherence to inhaled medications (sustained over 12 months), higher body mass index and lower perceived CF treatment burden.
Why read on?
This is the largest self-management intervention trial in CF, with 607 participants, and the only trial thus far to demonstrate a sustained difference in adherence versus a control arm, using a theory-based approach including habit formation.
Introduction
Cystic fibrosis (CF) is a multisystem genetic long-term condition (LTC) whereby recurrent pulmonary exacerbations drive progressive lung damage leading to premature death. Inhaled mucoactive agents and antibiotics have proven efficacy in reducing exacerbation frequency.1 2 CF is therefore an archetypal LTC; a cure is unavailable though efficacious treatments exist to improve health outcomes.
Low medication adherence, described by the WHO as ‘a worldwide problem of striking magnitude’3 is an important cause of treatment failure, poor health outcomes and increased healthcare costs in LTCs. In CF, low adherence to inhaled therapies is associated with more frequent and costly rescue treatments of exacerbations.4 Real-world objectively measured adherence of 30%–50% is lower than that of 80%–100% usually observed in clinical trials.5 Therefore, people with CF are unlikely to derive optimal benefit from inhaled therapies.5–10 At the same time, perceived treatment burden is high among people with CF11 and the James Lind Alliance Priority Setting Partnership identified ‘effective ways of simplifying treatment burden’ as the top CF research priority.12
Developing strategies to increase adherence is another CF research priority12 and could improve health outcomes by reducing exacerbation rates.6 Insufficient evidence exists to promote any particular adherence strategy.13 Large randomised controlled trials evaluating adherence interventions in CF continue to present negative findings,14 possibly because interventions are generally under-theorised and insufficiently tailored to individual needs.15 In addition, objectively measured adherence is largely absent in routine CF care, while self-reported and clinician estimates of adherence are notoriously unreliable,8 which prevents effective diagnosis, prescribing and provision of person-specific adherence support.
The Capability Opportunity Motivation-Behaviour model, based on a synthesis of frameworks of behavioural change, predicts that treatment taking depends on capability, opportunity and motivation.16 Reflective motivation is largely dependent on perceived necessity of adherence and treatment concerns17 and can be increased through education, persuasion and confidence building. For those motivated to adhere, increasing awareness of their objectively measured adherence through self-monitoring increases capability, that is, making visible the gap between objective and subjective adherence.8 Problem-solving techniques can be used to overcome individual capability and opportunity barriers. Theories of behavioural maintenance18 predict that supporting people to create habits for treatment, that is, taking treatments in response to specific contextual cues, can help to sustain adherence and to lower perceived treatment burden.19 We developed a multi-component (complex) self-management intervention to support sustained treatment adherence,20 incorporating objective adherence measurement, underpinned by behavioural science theory and designed to address gaps in CF care, with extensive input from people with CF. Since exacerbations are disruptive to patient life, they are an important patient-centred outcome and are commonly considered to indicate lung health.21 Therefore, the objective of this 12-month randomised controlled trial was to investigate the effectiveness of this multi-component self-management intervention compared with usual care in adults with CF using pulmonary exacerbation incidence rate as the primary outcome.
Methods
Study design, clinical interventionists and participants
We conducted a two-arm, open-label, parallel-group, usual care-controlled randomised clinical trial at 19 UK CF centres (trial registration ISRCTN55504164). The protocol (ethical approval REC: 17/LO/0035, IRAS ID: 218519) and statistical analysis plan (SAP) are available as supplementary material. The complex behavioural change intervention is designed to increase and sustain adherence to inhaled therapies. The development of the intervention is described elsewhere.22 Table 1 summarises the intervention, and further descriptions are in online supplemental appendix A. The study was monitored by an independent Trial Steering Committee. Data analysis was performed by the School of Health and Related Research, Sheffield. All authors vouch for fidelity to the protocol.
Supplemental material
Description of the intervention
Full-time interventionists (table 1) were employed and trained to deliver the intervention, underwent competency assessments (a theory test; practical assessments at first intervention visit, review and phase review) and received ongoing support (as detailed in online supplemental appendix A).
Participants were identified from the CF Registry, a UK database of people with CF. Potential participants were contacted by their usual clinical care team to seek permission for interventionists to discuss involvement. Eligible participants were aged ≥16 years and willing to take all inhaled mucoactive agents and antibiotics via eFlow Technology nebulisers with eTrack data-logging Controllers (PARI Pharma GmbH, Starnberg, Germany). Participants were excluded if: on the active lung transplant list; post-lung transplant; receiving care primarily palliative in intent; or using inhaled dry powder devices. All participants provided written, informed consent.
Randomisation and masking
Participants were allocated 1:1 to the intervention or usual care using a computer-generated pseudorandom list with random-permuted blocks of randomly varying sizes, via a central, web-based randomisation system. The allocation sequence was hosted by the Sheffield Clinical Trials Research Unit, with the sequence created by a statistician (not otherwise involved with trial) and held on a secure server. After recruiting each participant, the interventionist logged into the server and entered basic demographic information, then the allocation was revealed to the participants. Stratification was by centre and number of past year intravenous antibiotic days (≤14 and >14) – a predictor of current year intravenous days.23 The trial statistician remained blind to treatment allocation until database freeze. Participants and health professionals collecting primary outcome data were not blinded.
Treatment arms
All participants were given eTrack data-logging Controllers for their eFlow Technology nebulisers, which sent time-stamped and date-stamped data to a 2net Hub (Capsule Technologies, San Diego, California, USA) for accurate recording of inhalation and adherence calculation.
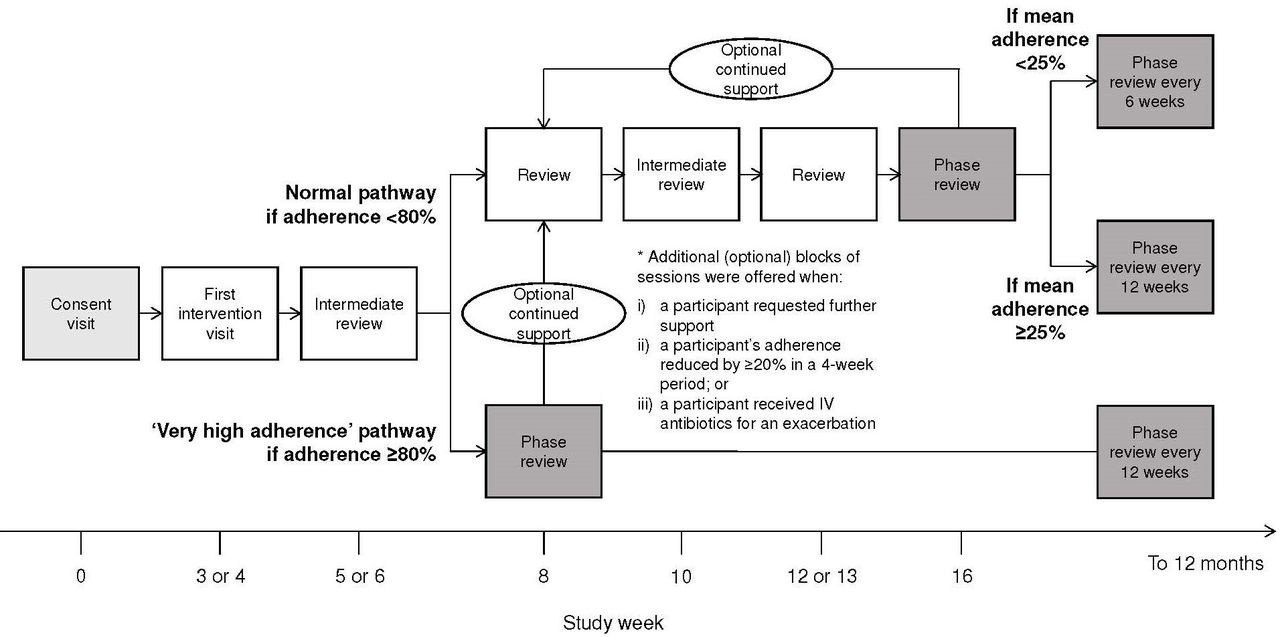
Intervention participants had access to the CFHealthHub digital platform (website and smartphone application) and received tailored flexible support from the interventionist throughout the 12-month trial period (table 1 and figure 1; further details in online supplemental appendix A).

Schedule of intervention delivery: normal and ‘very high adherence’ pathways. Adherence level to reflect baseline was calculated using objectively measured effective adherence data from weeks 1 and 2, as stated in the ‘Methods’.
The usual care arm used eTrack data-logging Controllers for adherence data collection. Contamination was minimised since there was no access to CFHealthHub, behavioural change tools and content. Adherence results were also invisible to participants and care teams.
At the final visit (at 12 months) or when a participant dropped out in either arm, a systems check was performed to ensure that all adherence data had been transferred from the eTrack data-logging Controller, thereby minimising missing data. The eTrack can store 3000 inhalations, which exceed the annual total number of doses even when the maximum prescription of eight daily doses occurred (table 2 gives prescribed doses), ensuring no missing data if eTrack was downloaded at the end of trial.
Baseline demographic and clinical characteristics, by randomised treatment group
Outcomes
The primary outcome was the pulmonary exacerbation incidence rate over 12 months. Using modified Fuchs’ criteria,24 an exacerbation occurred if intravenous antibiotics were administered for any one of 12 prespecified symptoms. Exacerbation forms were completed by a healthcare professional (clinical team or interventionist), and documented assessments were conducted at each clinical encounter (generally every 3 months) determined whether a participant was displaying an exacerbation.
To reflect effective medication use, adherence was calculated as normative (effective) adherence9 10 using objective data from weeks 3–52 as the outcome and weeks 1 and 2 as the ‘baseline’. Objectively measured effective adherence was calculated daily as a composite of all inhaled medications then aggregated weekly for analysis (appendix B), as we have detailed elsewhere.9 10 Other secondary endpoints were percent predicted FEV1), measured at each clinical encounter, and body mass index (BMI), calculated at baseline and 12 months. Patient-reported outcomes collected at baseline and 12 months included: CF Questionnaire-Revised (CFQ-R; eight subscales), measuring quality of life and including a perceived CF treatment burden subscale; Beliefs About Medicines Questionnaire (BMQ)-specific concerns and necessities; Self-Report Behavioural Automaticity Index (SRBAI), measuring habit strength; perceptions of treatment adherence (three-item scale); perceived effort of nebuliser treatments (one item); subjective adherence (self-reported % adherence); Confusion, Hubbub and Order 6-item Scale (CHAOS-6); Patient Activation 13-item Measure (PAM-13); and EuroQol 5-dimension and 5-level generic health status. Patient Health Questionnaire eight-item depression scale and Generalised Anxiety Disorder seven-item scale (GAD-7) were safety measures to understand whether the intervention worsens depression or anxiety. Adverse events were recorded using case report forms and were categorised as whether or not expected in relation to medications, or common among people with CF. Full details and references for outcomes are in the protocol and SAP.
Statistical analysis
Power calculations (online supplemental table 1) informed the choice of pulmonary exacerbation as the primary outcome and individual (vs cluster) randomisation. Cluster trials are complicated by recruitment bias. While contamination that reduces effect size may be a risk with individual randomisation, this can usually be overcome by increasing the sample size, which often still requires a smaller sample than cluster randomisation.25 The sample size was predicted based on reducing two exacerbations per year to 1.5 per year (equivalent to an incidence rate ratio of 2.0/1.5=0.75). Assuming a mean difference of 0.5 pulmonary exacerbations between the intervention and usual care arms over 12 months, an SD of 1.5, a design effect of 1.16 to allow for any clustering of outcomes by centre (intraclass correlation 0.01; cluster size 17) and an attrition rate of 20%, 556 participants were required to provide 90% power at a two-sided 5% level of significance.
Baseline characteristics were reported descriptively using summary statistics. The primary outcome incidence rate ratio, 95% CI and p value were estimated using a negative binomial regression model, with a random effect to adjust for clustering by centre. Log follow-up time was an offset in the model, and past year intravenous days (≤14 and >14 days) and treatment arm were fixed effects. Details of the sensitivity analyses performed on the primary outcome data (including adjustment for missing data) are in the SAP. Objectively measured effective adherence was analysed using a linear mixed-effects model, with random slopes and intercepts; treatment arm, time in weeks, baseline adherence (measured in the first 2 weeks post randomisation) and past year intravenous days were fixed effects. Treatment effects and 95% CI for all other secondary outcomes were produced using a mixed-effects model adjusting for baseline and past year intravenous days and with a random effect to adjust for clustering by centre. To aid interpretation, standardised effect sizes (Cohen’s d) were calculated for all secondary outcomes by dividing treatment effect with pooled SD
All analyses were prespecified and performed by intent to treat using R software V.3.6.1 and SAS V.9.4. CI widths were not corrected for multiplicity.
Results
Between October 2017 and May 2018, 3510 adults with CF were screened, with 608 enrolled and randomised (intervention n=305; usual care n=303) and 556 declined participation (figure 2). Participant recruitment is discussed in appendix C. One participant randomised to intervention withdrew on the day of consent prior to baseline data collection, thus was not included in analyses. The last recruited participant was followed until 30 June 2019, when the trial ended. Baseline demographic and clinical characteristics are in table 2. The intervention group was slightly older, with slightly higher FEV1, slightly lower past year intravenous days and slightly higher baseline objectively measured effective adherence (measured 2 weeks post randomisation)—this imbalance is explored in appendix D. Primary outcome data were available for all participants; adherence data were missing for 3.1% (19/607) of participants as explained in figure 2. Week-by-week breakdown of adherence data completeness is in online supplemental table 2.

Trial profile. *Exclusions due to missing covariates. †Adherence level to reflect the effect of intervention was calculated using objectively measured effective adherence data from week 3 (ie, from the point of intervention delivery) through to week 52 (ie, the end of the trial), as stated in the ‘Methods’ and ‘Results’. The intervention effect is best reflected by the cumulative adherence level throughout the trial period, similar to the approach of calculating cumulative exacerbation events throughout the trial. Though there were drop-outs during the trial, exacerbation data were available for all participants (expect for a participant who withdrew on the day of randomisation) since exacerbation events prior to drop-out were analysed. In a similar vein, adherence data available prior to the point of drop out were analysed as long as adherence data from week 3 onwards were available. Only 19 participants did not provide any adherence data from week 3 onwards, that is, adherence data were missing for outcome analysis among 19/607 (3%) of participants. Week-by-week breakdown of adherence data completeness is provided in online supplemental table 2.
The median (IQR) number of interventionist sessions per participant was 7.0 (6.0–10.0). The median (IQR) total interventionist delivery time per participant (including contact time and preparation outside of sessions) was 185 (126–263) min. Fidelity of intervention delivery median (IQR) scores were 97.2% (92.3–100.0), 92.6% (87.0–98.1) and 94.4% (91.7–97.2) at the first intervention visits, reviews and phase reviews, respectively (4)).
For the primary outcome, over 12 months, there were 526 pulmonary exacerbations in the usual care arm (adjusted rate 1.77/year, n=303) compared with 482 in the intervention arm (1.63/year, n=304). Incidence rate ratios (95% CI) of the primary analysis (0.96 (0.83 to 1.12); p=0.64), sensitivity analyses (online supplemental table 3) and subgroup analyses (online supplemental figure 1) indicated no significant between-arm difference in exacerbations.
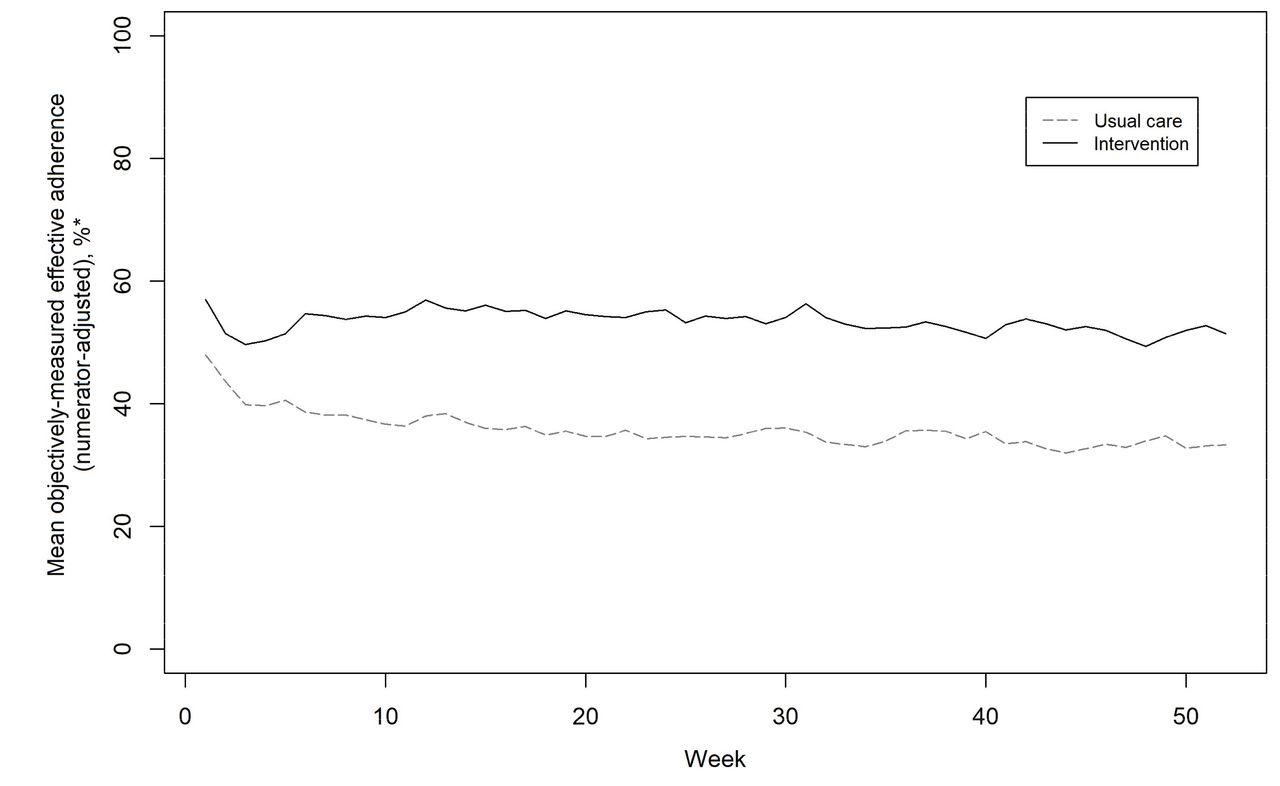
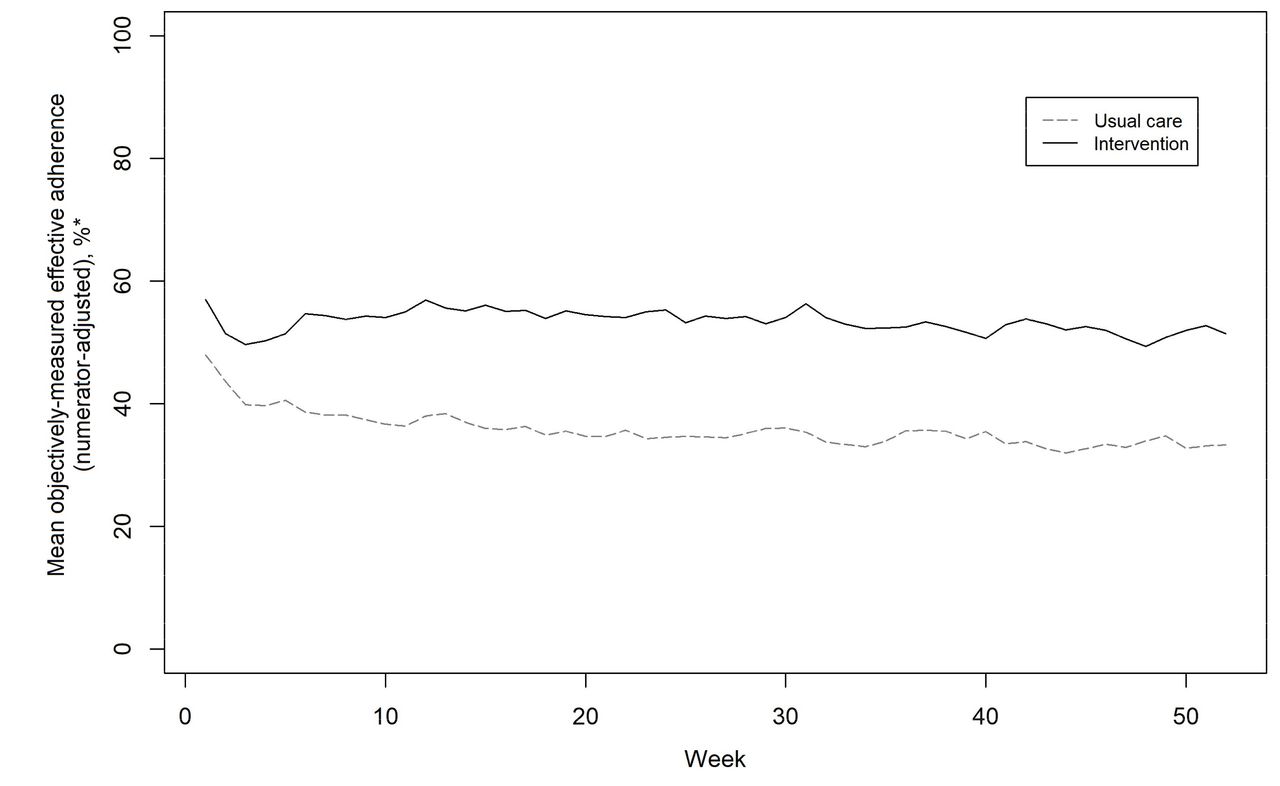
Mean objectively measured effective adherence in weeks 3–52 was 52.9% in the intervention arm versus 34.9% in the usual care arm, with an adjusted mean difference of 9.5 percentage points (95% CI 8.6 to 10.4). Figure 3 shows that adherence declined rapidly at a similar rate in both groups during the first 3 weeks of the trial. The decline among usual care participants continued over the subsequent 12 weeks, then stayed at the level until the end of the trial. In the intervention group, adherence subsequently improved following delivery of the behaviour-change intervention from week 3 onwards (further details in online supplemental appendix D).
{kind=link}
{kind=link}
{kind=link}
Medication adherence over 12 months, by randomised group (usual care n=295; intervention n=293). *Objectively measured effective adherence (sum of doses taken/sum of doses prescribed) was calculated on a weekly basis, with adjustments made against what may be considered an ideal treatment for effectiveness, as based on the following rules: all participants should receive at least a muco-active agent; and all participants with chronic Pseudomonas should receive at least both a mucoactive agent and an antibiotic. Adherence data were aggregated and plotted weekly for the purpose of detecting whether adherence is actually changing to smooth out daily fluctuations that may just be noise, for example, due to weekday versus weekend differences in adherence.40
Over 12 months, percent predicted FEV1 declined by 1.4 (from 58.3±22.6 to 56.9±23.0) among usual care and 0.1 (from 60.7±23.5 to 60.6±24.2) among intervention participants. The adjusted mean differences (95% CI) in per cent predicted FEV1 and BMI at 12 months were 1.4 (−0.2 to 3.0) and 0.3 kg/m2 (0.1 to 0.6), respectively (table 3).
Outcomes at 12 months, by randomised treatment group
Of the eight CFQ-R subscales, seven showed no between-group difference, but there was lower perceived CF treatment burden (3.9 (1.2, 6.7) points) in the intervention arm. Of the other 11 patient-reported outcomes at 12 months (including two safety measures; table 3), six showed differences for intervention versus usual care (adjusted difference in means (95% CI)), with increases in beliefs about medication necessities (0.1 (0.0 to 0.2) on BMQ-Specific necessities), habit strength for using nebuliser (1.2 (0.5 to 1.8) on SRBAI), perceptions of treatment adherence (0.7 (0.2 to 1.2) on three-item scale) and patient activation (3.4 (1.3 to 5.4) on PAM-13), and decreases in concerns about treatment (0.2 (0.1, 0.2) on BMQ-Specific concerns) and perceived effort of nebuliser treatments (0.3 (0.1 to 0.5) for one item). Other outcomes, including the safety measures of depression (−0.1 points (−0.8 to 0.7) on PHQ-8) and anxiety (0.3 points (−0.4 to 1.0) on GAD-7), showed no between-group difference.
No intervention-related serious adverse events were reported (online supplemental table 4). Sixty-four serious adverse events (21 in expected categories due to disease or treatment) in 43 usual care participants were recorded and 71 (28 expected) in 56 intervention participants.
Discussion
In this randomised, usual care-controlled trial, we investigated the effectiveness of a self-management intervention designed to reduce pulmonary exacerbation rates among adults with CF, by supporting their adherence to inhaled mucoactive agents and antibiotics. Over 12 months, a significant difference in pulmonary exacerbations or FEV1 was not detected. However, compared with usual care, the intervention achieved higher objectively measured effective adherence, higher BMI and lower perceived CF treatment burden.
It is possible that the primary outcome was not achieved due to insufficient between-group difference in adherence. It is also possible that using exacerbation as an endpoint was problematic. Exacerbation is a robust, sensitive outcome for blinded efficacy drug trials,21 but an unblinded, pragmatic evaluation of self-management support presents challenges to its use. There is a discretionary element to the use of intravenous antibiotics as rescue therapy; previous studies suggest only around 50% of events meeting 3/4 Rabin exacerbation criteria or acute 10% decline in FEV1 receive additional antibiotics.26 Increasing a person’s adherence to treatment may improve their acceptance of intravenous antibiotics,27 and more intense monitoring can detect more exacerbations.28 It is possible that increased clinician contact time in the intervention group created differential surveillance that biased the exacerbation rate towards unity (ascertainment bias). In UK practice, intravenous antibiotics will always be started by the CF care team, whereas oral antibiotics can be started in the community and may be much more susceptible to differential surveillance. To avoid this bias, oral courses were not collected. As a consequence, it is possible that improvement in milder exacerbations may have been missed. Adding a standardised criteria, for example, the Fuchs criteria, as part of the definition allowed exacerbation measurement across different centres to be comparable. However, recent work has suggested that this may result in reduced sensitivity.29
The graph for objectively measured effective adherence (figure 3) has several features that merit discussion (further details in appendix D). The pragmatic trial design of providing data-logging nebulisers and revealing trial allocation to participants on day 1, then measuring baseline adherence in the first 2 weeks of the trial creates complexity. The baseline between-group difference in objectively measured effective adherence was 8.6% in favour of the intervention group (54.1%±33.0% vs 45.5±34.1%), with the intervention group being older yet having higher FEV1 and lower IV days in the 12 months prior to study entry. Over the 49 weeks of the intervention, there was a between-group difference in objectively measured effective adherence of 18.0% in favour of the intervention group (52.9%±31.4% vs 34.9±31.7%), with an adjusted mean difference of 9.5% (95% CI 8.6% to 10.4%) taking into account the baseline adherence. Analysis comparing the adherence response stratified by baseline adherence (appendix D (figure D2)) shows that a significant between-group difference in adherence emerged at all levels of baseline adherence, emphasising that there was genuine divergence in adherence between the intervention and usual care independent of baseline adherence. It can be seen (figure 3) that in both groups there was an initial rapid decline in adherence. Among usual care participants not receiving any intervention, this decline continued over the next 12 weeks to around 35% and stayed at this level until the end of the trial. Real-world objective inhaled therapy monitoring has demonstrated similar levels of adherence among adults with CF not receiving intervention.8 9 In the intervention group, the initial rate of decline was similar to usual care until the behavioural change intervention started from week 3 onwards and adherence subsequently improved. Given the rapid initial decline of both groups over the first 3 weeks of the study, it seems possible that the adherence at study entry was a short-term manifestation of device novelty30 and white coat adherence.31
Since people with low adherence may find adherence data threatening,32 it is important to note that the differential adherence in the intervention arm was achieved without increasing anxiety. The intervention also achieved increase in necessity and reduction in concerns for treatment taking, consistent with literature highlighting that self-management of LTCs may be improved by addressing treatment beliefs.17 Policy makers who emphasise the importance of patient activation in LTCs33 can be reassured that the intervention significantly increased knowledge, skills and confidence (patient activation). The intervention achieved clinically important improvements in perceived treatment burden,34 which was identified as the number one research priority by the CF community.12 That total nebuliser use should increase while the perceived burden and effort of nebuliser treatment decrease may relate to a moderating role for habit.18 19 Literature in LTCs emphasises that sustained adherence is generally more strongly associated with habit than reflective motivation, which is more effortful.35
In considering the effective components of the intervention, data feedback is an obvious candidate. However, participants consulted data infrequently outside of supervised sessions. A qualitative analysis undertaken as part of the pilot work reported the value of the range of behaviour change techniques used in the intervention as well as the importance of building a relationship with the interventionist.36 It is unlikely that unsupported feedback alone is sufficient to explain the reduced treatment burden, the improved necessity and concerns for treatment or the increased habit strength.
A strength of the trial is the automatic capture of objective adherence with data-logging nebulisers that record every dose taken. Online supplemental table 2 demonstrates similar levels of week-by-week data completeness for both groups. Robust adherence data allowed us to demonstrate a sustained adherence difference for 12 months, which is the first for inhaled medications in any LTC. Sustained objectively measured adherence benefits for behavioural interventions in other LTCs are limited to two studies, both for oral medications among older adults in the hypertension and post-transplantation settings.37 38 CFHealthHub as a multi-component self-management intervention has now been established as a digital learning health system (ISRCTN14464661) in >50% of UK adult CF centres. Limitations of the trial include the delivery of both behavioural change and research procedures by interventionists, a period of server downtime that affected intervention delivery, the fact that the trial powered for exacerbation was not designed to detect the observed point estimate in FEV1 and the recruitment of a convenience sample whereby a third of the participants had objectively measured effective adherence levels >75%. The vulnerability of adherence studies to differential inclusion of more engaged patients is likely to reduce both the impact of the adherence intervention on studied behaviour and reduce the impact on health outcomes.39 This may mean that the positive behavioural findings observed in this study are particularly noteworthy. The direction of bias and implications of these limitations are further discussed in appendix E.
In this randomised controlled trial, an intervention for adults with CF that combines measurement of objective adherence to prescribed medication using data-logging nebulisers, a digital platform and manualised behavioural-change sessions delivered by trained clinical interventionists did not significantly affect pulmonary exacerbations and FEV1 but did result in higher objectively measured effective adherence, higher BMI and lower perceived CF treatment burden versus usual care, without increasing anxiety. This is the first iteration of a self-management intervention that may have the potential to be improved by continual iteration in a digital learning health system. Analogous to the overwhelming success in the CF drug pipeline of building on early signals with ongoing developments and trials, we plan to continue iterating and evaluating the CFHealthHub-based intervention by building on signals we have observed to further improve the intervention. Given that adherence is low in LTCs and that prescribed medications only work if taken appropriately, focusing on further evaluation of adherence interventions is important.
Data availability statement
Data are available on reasonable request. Requests for patient level data and statistical code should be made to the corresponding author and will be considered by members of the original trial management group, including the chief investigators and members of clinical trials research unit, who will release data on a case-by-case basis. Data will be shared following the principles for sharing patient level data as described by Tudur Smith C, et al BMC Medicine 2015;13:298 (https://doi.org/10.1186/s12916-015-0532-z). The data will not contain any direct identifiers, and we will minimise indirect identifiers and remove free-text data to minimise the risk of identification.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by a UK Research Ethics Committee, following submission through the Integrated Research Application System (REC: 17/LO/0035, IRAS ID: 218519).
Acknowledgments
We would like to thank: all trial participants and those who contributed to the development of the intervention; Professor Kathy Rowan as Independent Chair of both the National Institute for Health Research (NIHR) Programme Grant and Trial Steering Committees for ACtiF Programme; the members of the Independent Trial Steering Committee (including Professor David Torgerson); the members of the Patient and Public Involvement panel (including Caroline Greenslade; Martin Cameron; Karen Leyland; Ruth Day); trial support officers (including Louise Turner); the data management support team (Dr Amanda Loban; Chris Turtle); Carla Girling for support in the Programme Management Groups; and Daniel Hind for help with designing the study, data interpretation and drafting the manuscript. Cath Carsberg, PhD, provided editorial assistance, with funding provided by the Sheffield Teaching Hospitals Research Fund (BSAGCY9881504).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Collaborators CFHealthHub Study Team Members: H Cantrill, J Nicholl, S Michie, S Waterhouse, L Robinson, A Scott, S Antrobus, E Lumley, AN Biz, D Hind, C Orchard, E Nash, J Whitehouse, I Ketchall, J Rendall, H Rodgers, C Elston, S Bourke, W Flight, A McGowen, N Patel, D Watson, R Thomas, D Shiferaw, K Bateman, N Bell, N Withers, C Sheldon, M Pasteur, D Derry, D Waine, U Hill, J Myers, N Shafi, C Ohri, G Fitch, S Madge, S Elborn, K Miles, L Kent, V Mills, P Moran, G King, L Funnell, J Choyce, J Williams, C Evans, K Dack, J Trott, A Damani, S Raniwalla, D Tature, A Anderson, P Galey, L Warnock, J Faulkner, K Barbour, M Thomas, H Gledhill, K Donohue, H Seabridge, M Martin, K Lee, N Robson, C Weir, L Barlow and C Whitton.
Contributors MJW, AO'C, DH and MAA conceived and designed the study; CFHealthHub study team members collected data; SJW, LM and LS performed data analysis; MJW, AO'C, DH, MA and SJW performed data interpretation, and MJW drafted the manuscript. All authors reviewed and revised the manuscript and approved the final version. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. MJW and SJW are the guarantors.
Funding This report presents independent research funded by the NIHR under its Grants for Applied Research Programme (RP-PG-1212-20015) and NHS England Commissioning for Quality and Innovation (IM2 Cystic Fibrosis Patient Adherence).
Disclaimer The views and opinions expressed are those of the authors and do not necessarily reflect those of the National Health Service, the NIHR, Medical Research Council, Central Commissioning Facility, the Programme Grants for Applied Research Programme or the Department of Health and Social Care.
Competing interests All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no direct influence of any competing interest on the submitted work; support for MJW from Philips Respironics for early data transfer experience; support for the University of Manchester software team from PARI Pharma to create a medication reporting component within the CFHealthHub software; funding for MJW from Zambon; funding for IB from Microsoft Research; SJW is an NIHR Senior Investigator; IB became Chief Data Scientist (advisory) for AstraZeneca in September 2019; no other financial relationships that might have an interest in the submitted work in the previous three years; and no other relationships or activities that could appear to have influenced the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.