Article Text

Abstract
Rationale For clinicians it remains very difficult to predict whether preschool children with symptoms suggestive of asthma will develop asthma in later childhood.
Objective To investigate whether measurement of fraction of exhaled nitric oxide (FENO), interrupter resistance (Rint) or specific immunoglobulin E (IgE) in 4-year-old children with suggestive symptoms can predict asthma symptoms up to age 8 years.
Methods Children were recruited from the PIAMA birth cohort. All children with symptoms suggestive of asthma at age 3 or 4 years, who were invited for medical examination at age 4 (n=848), were eligible. Associations of FENO (n=308), Rint (n=482) and specific IgE (n=380) at 4 years with wheezing and asthma at the ages of 5–8 years were assessed using repeated measurement analyses. The added predictive value of these objective tests was then investigated by including parameters for clinical history in the model.
Results FENO and specific IgE measured at 4 years were associated with wheezing and asthma at 8 years. Both tests also remained significant predictors after mutual adjustment and adjustment for clinical history: OR on wheezing at 8 years for FENO (10log-scale, per IQR) 1.6 (95% CI 1.1 to 2.2) and for specific IgE 2.8 (95% CI 1.9 to 4.1). Rint was significantly associated with wheezing at age 6, but not at 7 and 8 years.
Conclusions In preschool children with symptoms suggestive of asthma, both FENO and specific IgE measured at age 4, but not Rint, improved the prediction of asthma symptoms until the age of 8 years, independent of clinical history.
- Prognosis
- breath test
- airway resistance
- radioallergosorbent test
- paediatrics
- allergic lung disease
- clinical epidemiology
- exhaled airway markers
- paediatric asthma
Statistics from Altmetric.com
- Prognosis
- breath test
- airway resistance
- radioallergosorbent test
- paediatrics
- allergic lung disease
- clinical epidemiology
- exhaled airway markers
- paediatric asthma
Introduction
In preschool children, asthma-like symptoms such as wheezing and coughing are highly prevalent.1 Unfortunately, children with transient symptoms are not easily distinguished from those with persistent asthma on the basis of reported symptoms. Objective tests to support an asthma diagnosis include spirometry, to assess airway obstruction and reversibility; bronchoprovocation, to assess airway responsiveness; and sputum induction, to measure airway inflammation, a hallmark of asthma.2 These tests are difficult to perform in children under the age of 6 years since active cooperation is necessary.3 Non-invasive measurement of the fraction of exhaled nitric oxide (FENO) has received much interest due its ability to reflect eosinophilic airway inflammation.4 5 Several studies have shown elevated FENO values in children with asthma or atopy.6–12 Moeller et al showed that FENO could distinguish between the different phenotypes of preschool wheezers.13 However, prospective data on the prognostic value of FENO in preschool children for later symptoms are scarce. In clinical practice, measurement of FENO would only be worthwhile if it offers an added predictive value over information that is already available, such as a standard clinical history. This has not been investigated so far. Interrupter resistance (Rint) measurement can be easily performed in young children and correlates with asthma symptoms.14–16 Specific immunoglobulin E (IgE) to inhalant allergens in young children is associated with the risk of persistence of asthma symptoms.17–20
The aim of our study was to investigate prospectively whether FENO, Rint and/or specific IgE at the age of 4 years in children with respiratory symptoms could be used to predict asthma symptoms up to the age of 8. We used data from the ‘Prevention and Incidence of Asthma and Mite Allergy’ (PIAMA) birth cohort.21 Children were eligible if they reported ‘wheeze’, ‘shortness of breath’ or ‘nightly cough without a cold’ at the age of 3 or 4 years. FENO, Rint and specific IgE were measured at the age of 4 years and children were followed until the age of 8. The added value of the tests to predict asthma symptoms until the age of 8 was calculated.
Methods
Study population
Recruitment of the PIAMA cohort took place in 1996–1997; 7862 pregnant women were invited to participate; 4146 women (53%) agreed (1327 allergic and 2819 non-allergic, based on a validated screening questionnaire).22 Their children were followed up for 8 years, using questionnaires for parental completion, partly based on the International Study of Asthma and Allergies in Childhood (ISAAC) core questionnaires.23 At 4 years, all children with an allergic mother and a random sample of children with a non-allergic mother were invited for a medical examination, including measurement of FENO, Rint and specific IgE levels (n=1808). A detailed description of the study design has been published previously.21 The study protocol was approved by the medical ethics committees of the participating university hospitals. For the current study, we selected all children who were invited for the medical examination at 4 years and who reported at least one respiratory symptom suggestive of asthma (wheeze, shortness of breath, or cough at night without a cold) in the questionnaire at age 3 or 4 years (n=848) (figure 1).

Flow chart of the study population. All 848 eligible children enter each of the three arms of the flowchart. *Respiratory symptoms were defined as a positive response to at least one of the following three questions: ‘Has your child had wheezing or whistling in the chest in the last 12 months?’ and/or ‘Has your child had tightness of the chest or shortness of breath in the last 12 months?’ and/or ‘Has your child had a cough during the night, when he/she did not have a cold or a chest infection, in the last 12 months?’ †Out of 306 children with available FENO (fraction of exhaled nitric oxide), 51 used steroids at the age of 4 years; these children were not excluded from the analysis. ‡The following six airborne allergens were tested for: house dust mite (Dermatophagoides pteronyssinus), cat, dog, grass pollen (Dactylis glomerata), birch and Alternaria alternata. IgE, immunoglobulin E; Rint, interrupter resistance.
FENO, Rint and specific IgE measurement
FENO at age 4 was measured offline according to European Respiratory Society (ERS)/American Thoracic Society (ATS) guidelines.24 For every child, duplicate exhaled air samples and an ambient air sample were collected in Mylar balloons, and analysed using a chemoluminescence analyser (Sievers NOA 280B, Boulder, Colorado, USA). FENO was expressed in parts per billion (ppb). Rint was measured in kPa/l with MicroRint (MicroMedical, Rochester, Kent, UK) during expiration, with occlusion of the airway at peak expiratory flow. Median values for at least five acceptable measurements were calculated. Detailed descriptions of both measurement techniques were previously published.8 16 25 Sensitisation was defined as specific IgE of ≥0.70 IU/ml for at least one of six tested airborne allergens. To assess the added predictive value of these measurements over reported clinical history, three variables previously shown to have the highest predictive value on later symptoms were selected26: (1) allergic mother (yes/no); (2) doctor's diagnosis of eczema ever until age 4 (yes/no); and (3) wheezing frequency during the fourth year of life (no/1–3 times per year/≥ 4 times per year). Mothers were considered ‘allergic’ if they reported any of the following items: asthma, hay fever, house dust allergy, house dust mite allergy or pet allergy.
Outcomes
Based on data from the annual questionnaires at age 5– 8 years the following dichotomous outcomes were defined, each pertaining to the past 12 months:
Wheezing: at least one episode
Inhaled steroid prescription by a medical doctor
Doctor's diagnosis of asthma: a parental report of a doctor's diagnosis of asthma at any time AND a parental report of asthma symptoms during the past 12 months.
Statistical analysis
Univariate associations between FENO, Rint and specific IgE measurements and respiratory outcomes were investigated with logistic regression. FENO values had a right-skewed distribution; a normal distribution was achieved after 10log-transformation. Generalised estimating equations were used to take into account the correlation between repeatedly measured outcomes in the same individual. Variables for clinical history were included in the model to examine additional predictive value of the tests over clinical history. The study design was stratified for allergy of the mother, and any interaction with this variable was investigated. After a complete case analysis, missing data were imputed multiple times to check for any bias that could result from complete case analysis.27 28 The ‘Multivariate Imputation by Chained Equations’ (MICE) procedure in the statistical program R version 2.6.2 was used to create 10 imputed data sets (n=848).29 30 Results were combined using PROC MIANALYZE in SAS 9.1 (SAS Institute, Carey, North Carolina, USA). Finally, a model was built including clinical history, specific IgE and FENO, which allowed us to estimate the added predictive value of FENO over the combination of clinical history and specific IgE. The online data supplement provides a detailed description of study design, analysis and the multiple imputation procedure (table E1).
Results
Study population
At the age of 4 years 1808 children were invited for medical examination, of whom 848 (46%) reported at least one of the following symptoms at 3 or 4 years: wheeze (n=379), shortness of breath (n=385) or nightly cough (n=592). The eligible study population therefore consisted of 848 children. An acceptable FENO measurement was obtained from 306, Rint from 482 and specific IgE from 380 children (figure 1). We compared children with and without available values for these measurements separately, with respect to baseline characteristics and symptoms at 8 years (table 1). Children with available FENO values (n=306) were similar to children without (n=542), the only difference being the educational level of the mother. Children with Rint values (n=482) were also more likely to have a mother with higher education than children without Rint measured (n=366), and had significantly fewer symptoms at the age of 8. Children with IgE data were more likely to be boys, to have an allergic mother, older siblings and to be exposed to cigarette smoke in utero, compared with children with missing IgE data. With respect to symptoms at baseline and at 8 years, there were no major differences. The distribution of clinical symptoms and objective tests that were used to predict later asthma symptoms is given in table 2.
General characteristics of the eligible study population
Variables used to predict asthma symptoms
Predictive value of FENO
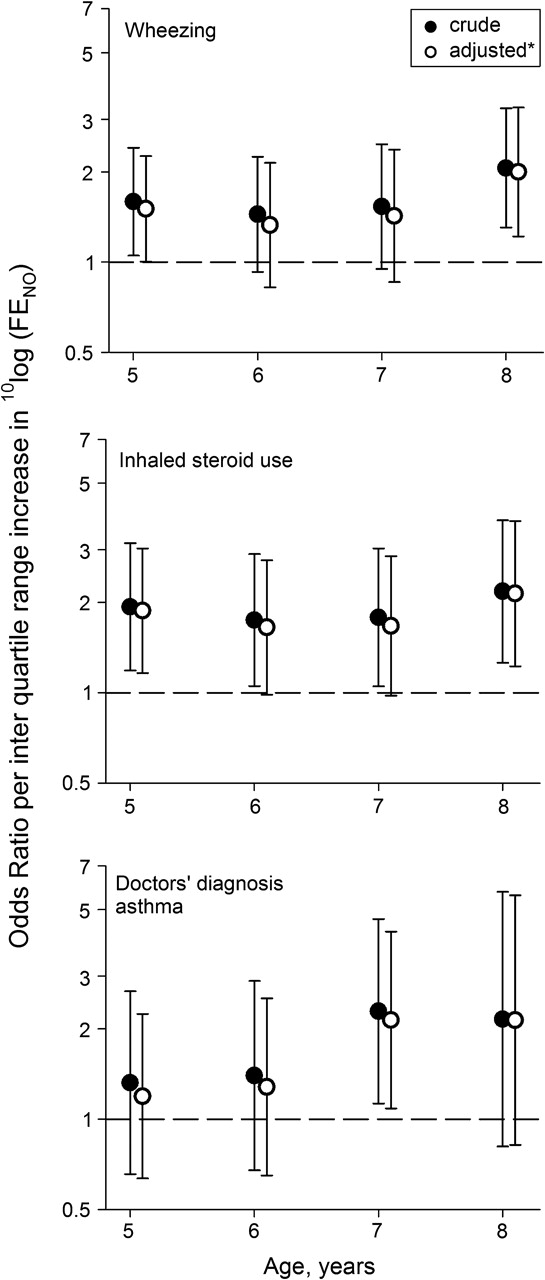
A higher FENO at 4 years was associated with significantly more wheezing and steroid use between the ages of 5 and 8 years. The association remained more or less stable over the 4 year follow-up period, with an OR per IQR increase in 10log(FENO) on ‘wheezing’ at 8 years of 2.1 (95% CI 1.3 to 3.3, figure 2). A significant association with doctor's diagnosis of asthma was present only at age 7. Inclusion of three variables for clinical history in the model had very little effect on the ORs: FENO remained significantly associated with later symptoms, independent of clinical history. Multiple imputed data analyses produced similar associations (online supplement). Fifty-one children used steroids at the age of 4, which may have influenced FENO measurement. In a sensitivity analysis, exclusion of these children from the analysis led to slightly stronger associations with the outcomes ‘doctor's diagnosis of asthma’ and ‘steroid use’. A charcoal NO scrubber was used while collecting exhaled air to eliminate an influence of ambient NO on FENO measurements, but some association between FENO and ambient air NO remained. Adjustment of our models for ambient NO did not change our results.

Predictive value of FENO (fraction of exhaled nitric oxide) measured at 4 years on all outcomes at 5–8 years. Filled circles are crude ORs for FENO (per IQR increase in 10log(FENO)). *Open circles are adjusted for clinical history (allergic mother/doctor's diagnosis of eczema/wheezing at age 4).
Predictive value of Rint
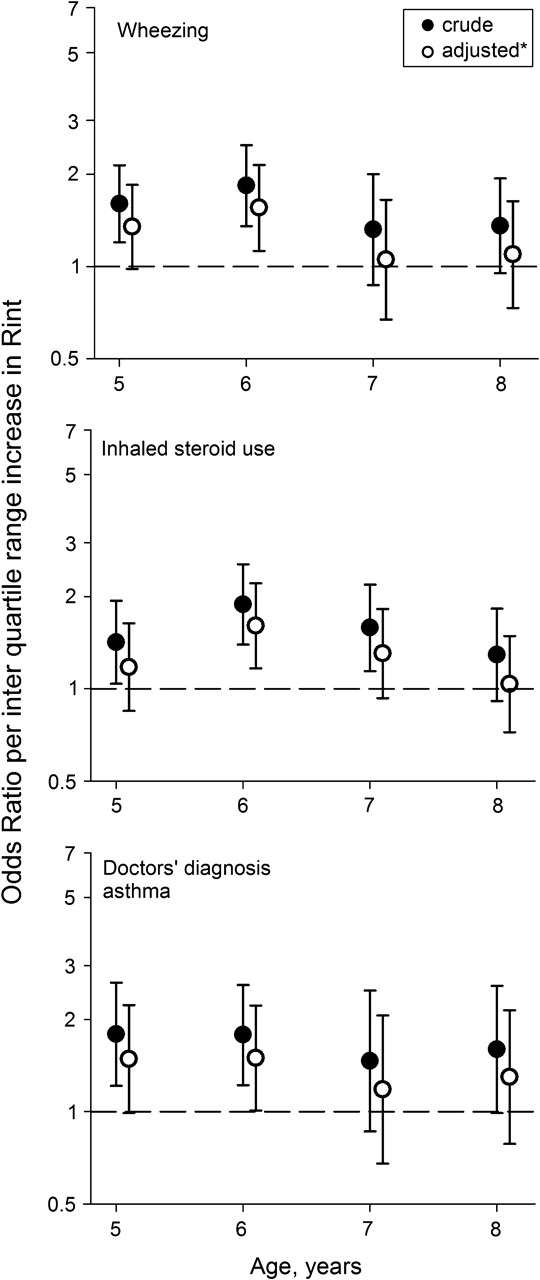
Rint values at age 4 were associated with symptoms at age 5 and 6. The association decreased after the age of 6 and was no longer significant at 8 years (figure 3). Adjustment for clinical history further decreased the association between Rint and all outcomes. The adjusted OR per IQR increase in Rint for wheezing at 8 years was 1.1 (95% CI 0.7 to 1.6). Multiple imputed analyses did not change this (online supplement).

Predictive value of Rint (interrupter resistance) measured at 4 years on all outcomes at 5–8 years. Filled circles are crude ORs for Rint (per IQR increase). *Open circles are adjusted for clinical history (allergic mother/doctor's diagnosis of eczema/wheezing at age 4).
Predictive value of specific IgE
A positive specific IgE to any airborne allergen had a strong association with later symptoms (figure 4). The association remained stable over the 4 year follow-up. At age 8 the OR for ‘wheezing’ was 6.6 (95% CI 3.5 to 12.7). When clinical history was taken into account the ORs decreased considerably, but the associations remained strongly significant for all outcomes (OR 4.3 (95% CI 2.1 to 9.1) for wheezing at 8 years). ORs for specific IgE decreased considerably on all outcomes in the multiple imputed analysis. Since such analyses are less likely to be influenced by selection bias, these estimates are probably more reliable. In the imputed analyses, specific IgE remained the strongest predictor of later symptoms, even when clinical history was taken into account.

Predictive value of specific IgE (immunoglobulin E) measured at 4 years on all outcomes at 5–8 years. Filled circles are crude ORs for specific IgE. *Open circles are adjusted for clinical history (allergic mother/doctor's diagnosis of eczema/wheezing at age 4).
Combination of clinical history, FENO and specific IgE
These results imply that both FENO and specific IgE, independent of clinical history at 4, significantly improve the prediction of asthma symptoms up to the age of 8 years. The question remains of whether FENO still has an added value, when clinical history and specific IgE are already known. We investigated this in a combined model which included FENO, specific IgE and clinical history. Complete data on all variables were available from 185 children; the eligible population comprised 848 children. Analyses on the outcome ‘wheezing’ at age 8 were performed in both populations (table 3). Estimates for FENO and specific IgE were constant in both analyses. The level of significance increased in the multiple imputed analysis, but even in the complete case analysis (n=185) FENO remained borderline significant (table 3). Importantly, we found no interaction between FENO and either ‘specific IgE’ or ‘allergic mother’. To visualise the clinical implications of our findings, the predicted probability of wheezing is plotted against FENO values measured at 4 years (figure 5). Different lines represent children with different subsets of risk factors. When all risk factors are absent, FENO appears to be of limited clinical value, because the post-test probability remains low even at higher FENO values. However, in children with an intermediate or high pretest probability of later wheezing, an FENO test at the age of 4 could change the post-test probability to a degree that would be relevant in clinical practice. For example, in children with an allergic mother, eczema and specific IgE, but with infrequent wheezing at 4 (thick dashed line, figure 5), risk of asthma symptoms at 8 ranged from 25% to 70% depending on FENO measured at 4 years.
Predictive value of FENO and specific IgE on ‘wheezing’ (with mutual adjustment and adjustment for clinical history)*

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Predicted probability of ‘asthma symptoms’ depending on FENO (fraction of exhaled nitric oxide) at 4 years. Predicted probability for ‘wheezing’ at age 8 is modelled for FENO values (unit: parts per billion) measured at age 4, adjusted for specific immunoglobulin E (IgE), allergic mother, doctor's diagnosis of eczema and wheezing frequency at age 4. Different lines represent children with different subsets of risk factors. The horizontal axis is in log scale. *The vertical grey line represents the geometrical mean FENO in the study population and can be used to determine the pretest probability of wheeze at 8 for individual children.
Discussion
We show that in preschool children with symptoms suggestive of asthma, measurement of FENO and specific IgE could predict later asthma symptoms, up to the age of 8. Both tests had an added predictive value, independent of each other and of clinical history.
Several studies investigating the association between FENO and airway symptoms in children reported a higher FENO in children with wheezing and asthma.6 7 9 11 Malmberg and colleagues even reported an 86% sensitivity and 92% specificity of FENO to diagnose asthma, clearly superior to conventional bronchoprovocation testing and spirometry.9 Importantly, these studies selected children already known to have asthma, and healthy controls. Such a case–control design is likely to cause selection bias, with overestimation of a test's diagnostic performance.31 In unselected groups of schoolchildren, a much lower diagnostic performance of FENO was reported.12 32 Age is important when comparing different studies, due to heterogeneous respiratory disorders and changing FENO during childhood.33 34 In children aged 4 years, higher FENO values were measured in recurrent wheezers and in children with doctor-diagnosed asthma, with considerable overlap.8 10 Moeller et al showed that FENO could be used to distinguish between different phenotypes of preschool wheezers, based on their clinical history up to the age of 4. However, FeNO will only have a clinical benefit if it offers additional information compared with clinical history.13 Previous studies were cross-sectional, and very little is known about the predictive value of FENO on later asthma in preschool children. We performed a 4 year follow-up and took the child's clinical history into account to assess the true additional predictive value of FENO for later asthma. This reflects the clinical setting in which FENO would be used. Our prospective analysis shows that FENO measured at 4 years indeed improved prediction of asthma until the age of 8 years.
Cross-sectional studies have reported higher Rint in those with asthma compared with controls, with considerable overlap.14 15 35 Previous analysis of our own data at age 4 showed a higher Rint in persistent wheezers, compared with children who never or transiently wheezed.25 The only prospective study on the predictive value of Rint measurements was performed in a cohort of 110 children diagnosed with asthma (aged 2–5 years) and found no association between Rint and asthma medication after 3 years follow-up.36 Our study recruited children from a population-based cohort, based on reported respiratory symptoms, and results were similar: Rint at age 4 did not discriminate between children with or without symptoms at 8 years. Although Rint was associated with symptoms up to 2 years after measurement, it was not useful in the long-term management of individual children. Thirty-nine children (7%) were excluded because bronchodilators were used within 24 h prior to Rint measurement. When these children were included, the predictive power of Rint was even smaller. Nonetheless, selective exclusion of this group of high risk children may have decreased the power to detect an association of Rint with later symptoms.
Prospective studies showed that children with positive specific IgE for inhalant allergens were more likely to develop wheeze19 and asthma18 in childhood. Even when information from patient history is considered, specific IgE improved prediction of later asthma.17 20 Our results show that the predictive value of specific IgE measured at 4 years remains high until the age of 8. Importantly, our data allowed us to investigate the independent added value of specific IgE and FENO measurements at 4. Several authors reported raised FENO levels in children with atopy rather than asthma.32 37 Consequently, it has been proposed that any predictive value of FENO for asthma might be explained by its correlation with specific IgE.38 Our combined analysis shows that even though FENO and specific IgE are correlated, they both independently contributed to the prediction of later asthma symptoms.
Major strengths of this study are its longitudinal design and large sample size. In the selection of the eligible population and the statistical analysis we aimed to mimic the clinical setting. This enabled us to estimate the true added value of the tests and hence their clinical relevance.
Selection bias could have resulted from incomplete data. However, we found that children with complete data did not differ from those with incomplete data. Furthermore, a multiple imputed analysis including all eligible children led to similar results and did not change any of our conclusions (online data supplement). Secondly, the PIAMA study is an unselected birth cohort, but due to over-representation of children with an allergic mother in the medical examination at 4, our eligible population included more children with an allergic mother. If the predictive value of FENO, Rint or specific IgE differs between children with and without an allergic mother, this would limit the generalisability of our findings. We consider this unlikely since there was no interaction between any of the tests and the variable ‘allergic mother’. Hence, our findings may be generalisable to all children in the general population with asthma symptoms at 3–4 years. Although steroid use is well known to decrease FENO, we decided to include 51 (17%) children who used inhaled corticosteroids at age 4. This may have led to some underestimation of the predictive power of FENO, but we preferred this over selective exclusion of 51 high risk children. Finally, in order not to overestimate the added prognostic value of FENO, Rint and specific IgE over a clinical history we tested which variables for clinical history were the best prognostic indicators for later symptoms, and added the three variables with the strongest association in our multivariable analysis.39 Including a variable for wheezing phenotype (multitrigger wheeze/viral induced wheeze/no wheeze) in our models did not decrease the predictive ability of any of the three investigated tests.
Do our findings have clinical relevance? In the management of wheezing preschool children a first step will always be to take a full medical history. Secondly, a specific IgE test has the highest predictive value for symptom persistence. FENO measurement as a next step can significantly improve prediction of later asthma symptoms, especially in children with an intermediate pretest risk.
In conclusion, we demonstrated that in preschool children with symptoms suggestive of asthma, both FENO and specific IgE at age 4 predicted asthma symptoms until the age of 8 years independently, and independent of clinical history. Specific IgE had the highest predictive value; the added value of FENO was limited. Nevertheless, in children with an intermediate or high risk, FENO substantially changed the risk of later wheezing and asthma to a degree that may be relevant in clinical practice.
Acknowledgments
The authors gratefully acknowledge Dr Maarten Schipper for providing valuable discussion and suggestions on the data analysis.
References
Supplementary materials
Web Only Data thx.2010.126912
Files in this Data Supplement:
Footnotes
Funding The Netherlands Organisation for Health Research and Development; the Netherlands Organisation for Scientific Research; the Netherlands Asthma Fund; the Netherlands Ministry of Spatial Planning, Housing, and the Environment; and the Netherlands Ministry of Health, Welfare and Sport. The salary of DC was paid by a ‘Toptalent’ grant from the Netherlands Organisation for Scientific Research (NWO). None of the funding sources had a role in either the study design, data collection, analyses, interpretation of the data, writing of the report or decision to submit this paper for publication.
Competing interests None.
Ethics approval The study protocol was approved by the medical ethics committees of the participating university hospitals: ErasmusMC, University Medical Centre Rotterdam, University Medical Centre Groningen, University Medical Centre Utrecht.
Provenance and peer review Not commissioned; externally peer reviewed.