Article Text

Statistics from Altmetric.com
History
A 24-year-old man presented to the trauma center with gunshot wounds to the neck, chest and back.
Examination
The patient was awake but lethargic with a heart rate of 120 beats per minute, a systolic blood pressure of 80 mm Hg and absent breath sounds on the right. He was noted to have an expanding hematoma of the left neck under a gunshot wound, a gunshot wound to the left chest at the level of the nipple, a gunshot wound overlying the left scapula, and a fourth gunshot wound penetrating the left deltoid muscle.
Question
The most appropriate first step in management of this patient in addition to resuscitation is:
Foreign body X-ray series.
Left anterolateral thoracotomy.
Orotracheal intubation/right thoracostomy tube.
Pressure dressing to left neck.
Management
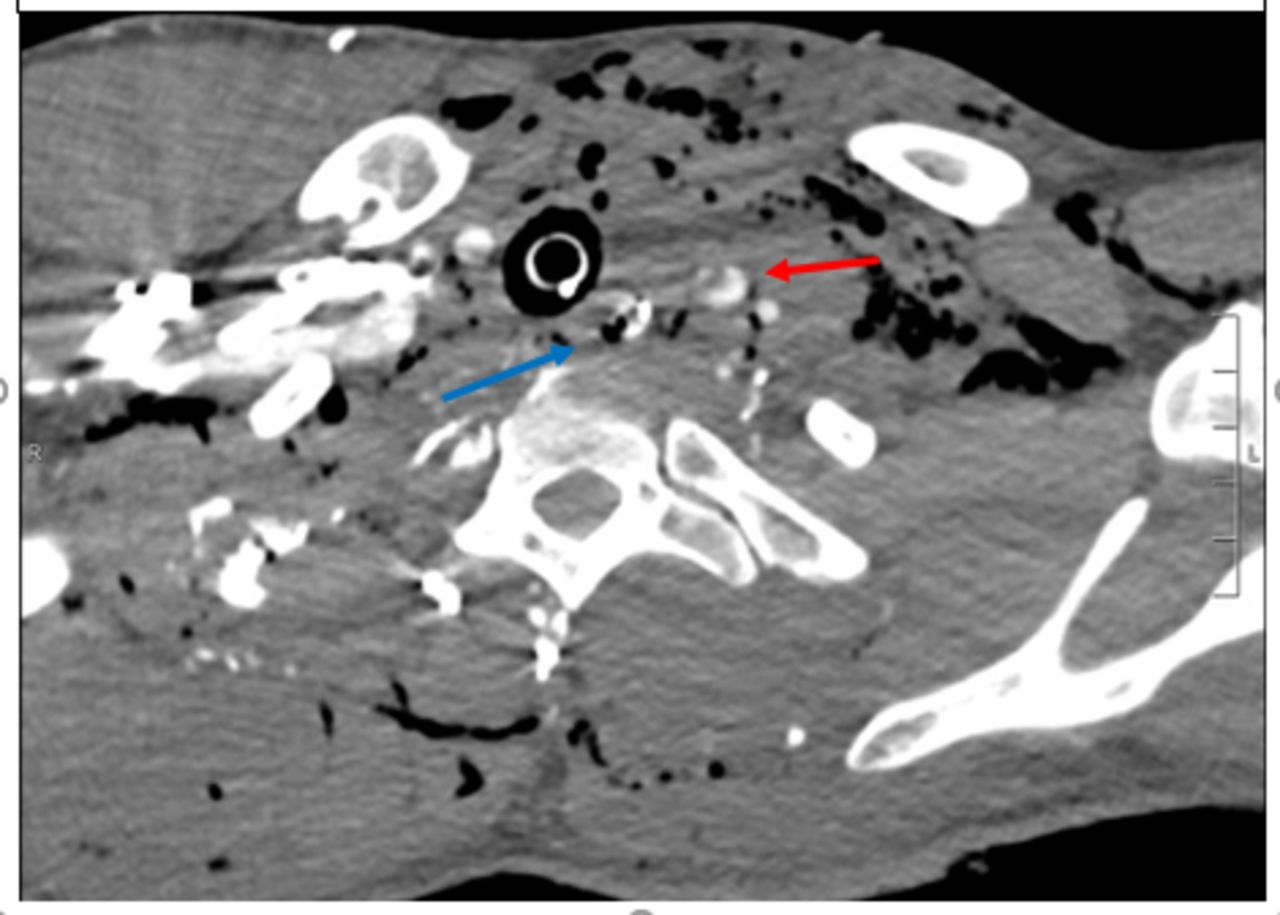
The patient underwent orotracheal intubation, insertion of a right thoracostomy tube, and transfusion of blood through large bore intravenous catheters. A foreign body series demonstrated a deep sulcus sign on the left with a pulmonary contusion, a retained bullet in the region of the right shoulder and several bullet fragments in the left shoulder (figure 1). Subsequently, a left-sided thoracostomy tube was inserted with drainage of a hemothorax. After transfusion of 3 units of packed red blood cells and 3 units of plasma, the patient’s systolic blood pressure increased to 120 mm Hg and his heart rate decreased to 80 beats per minute. As the patient’s cervical hematoma was stable, a CT scan of the neck and chest was performed with a single load of intravenous contrast. The CT scan demonstrated an intimal defect in the left common carotid artery and a trajectory highly concerning for esophageal perforation (figure 2).
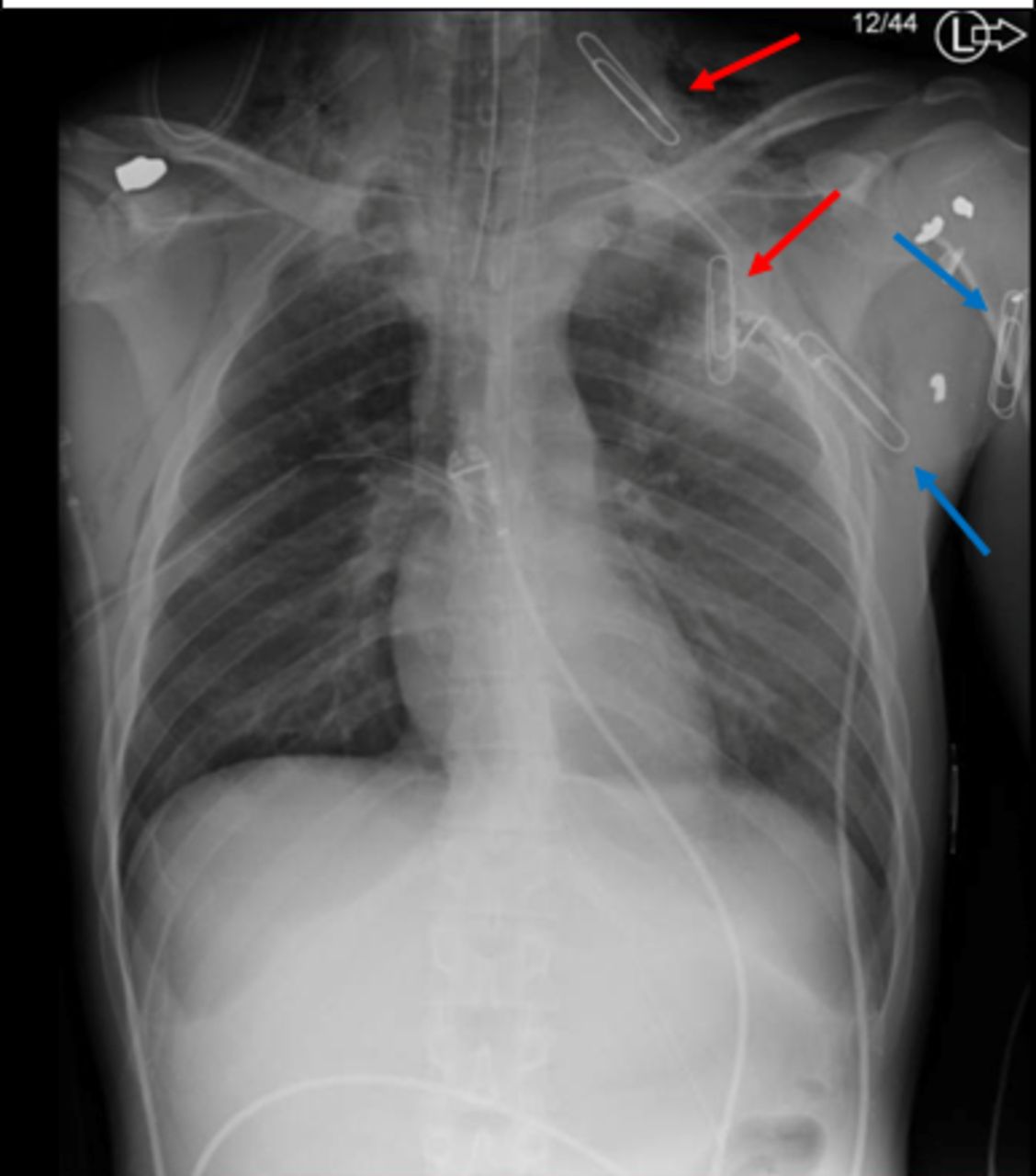
Paper clips mark gunshot wounds. Red arrows are anterior and blue arrows are posterior.
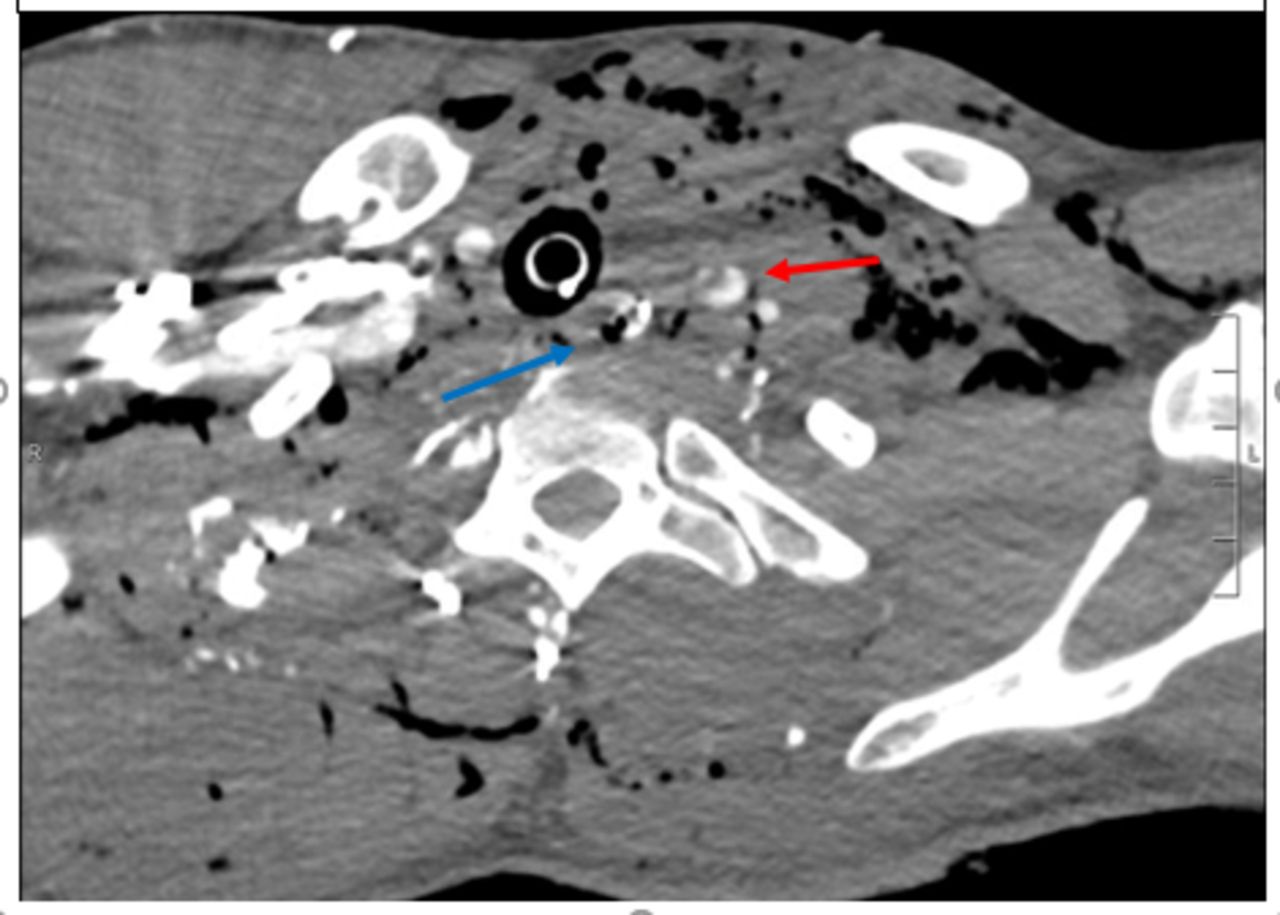
CT scan demonstrating carotid (red arrow) and esophageal (blue arrow) injuries.
Question
The most appropriate management of this patient’s cervical injuries would be (controversial):
Esophagoscopy and stenting of carotid artery.
Stenting of carotid artery and left cervical exploration.
Stenting of carotid artery and esophagus.
Esophagoscopy and left cervical exploration.
Management
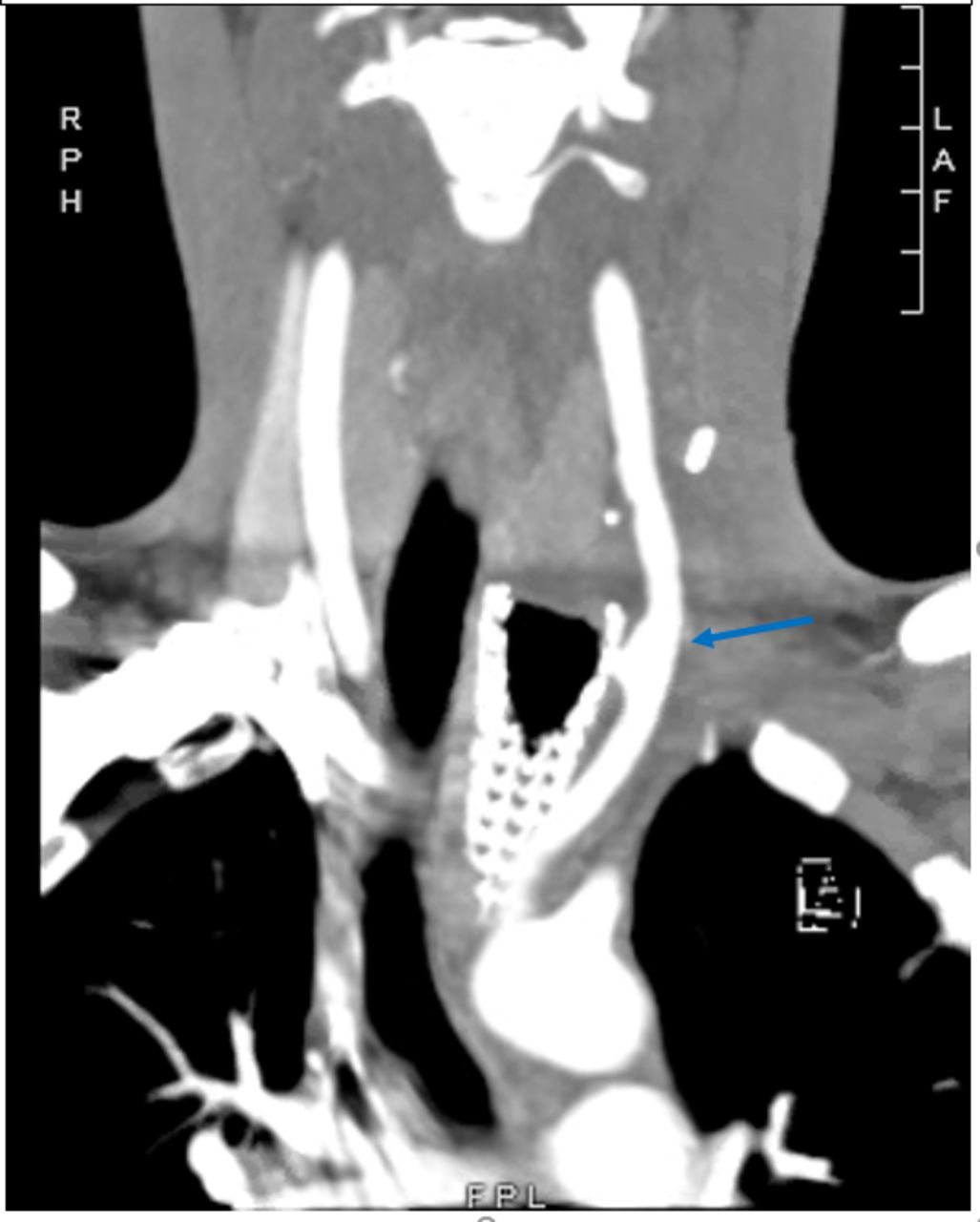
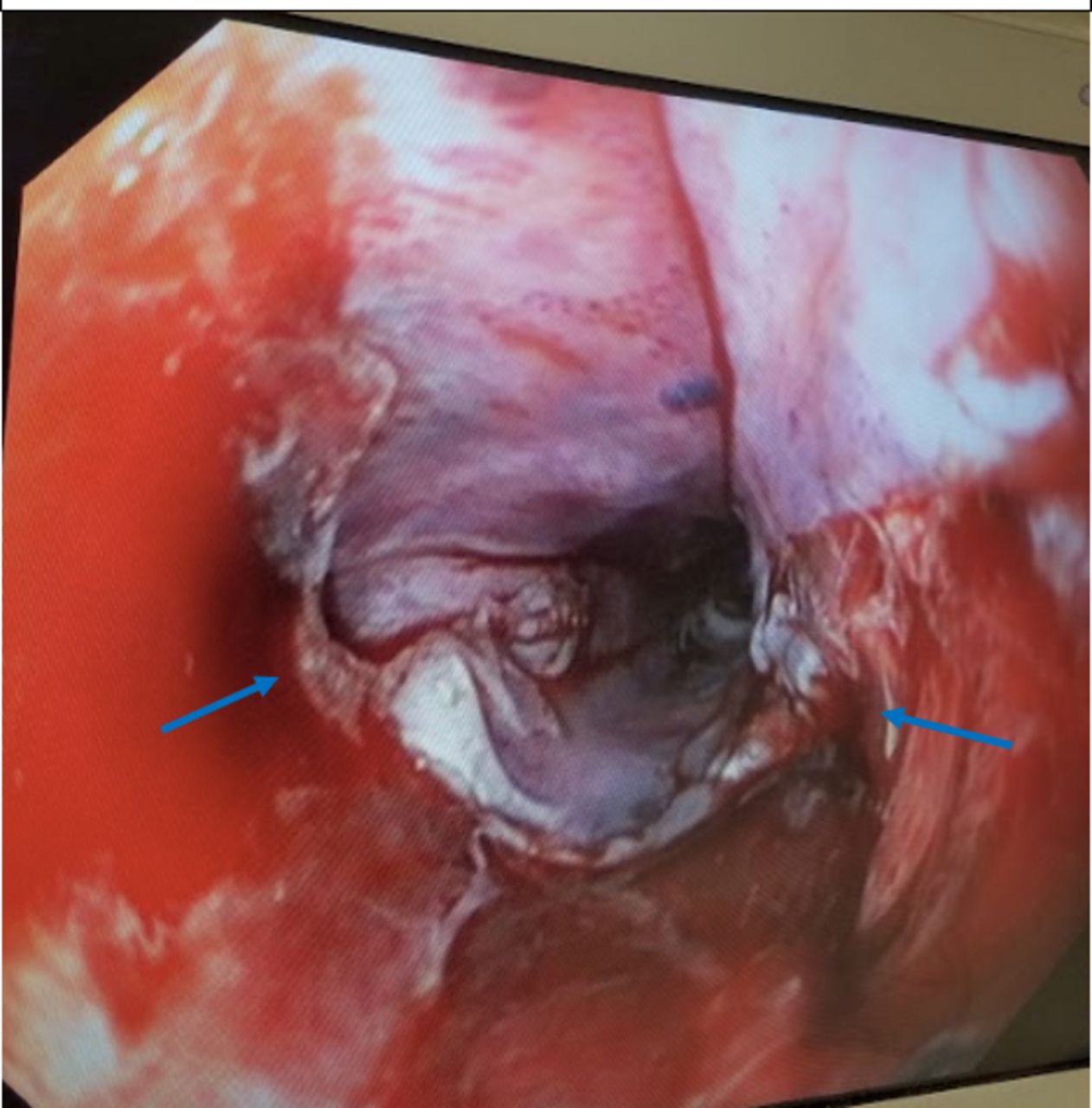
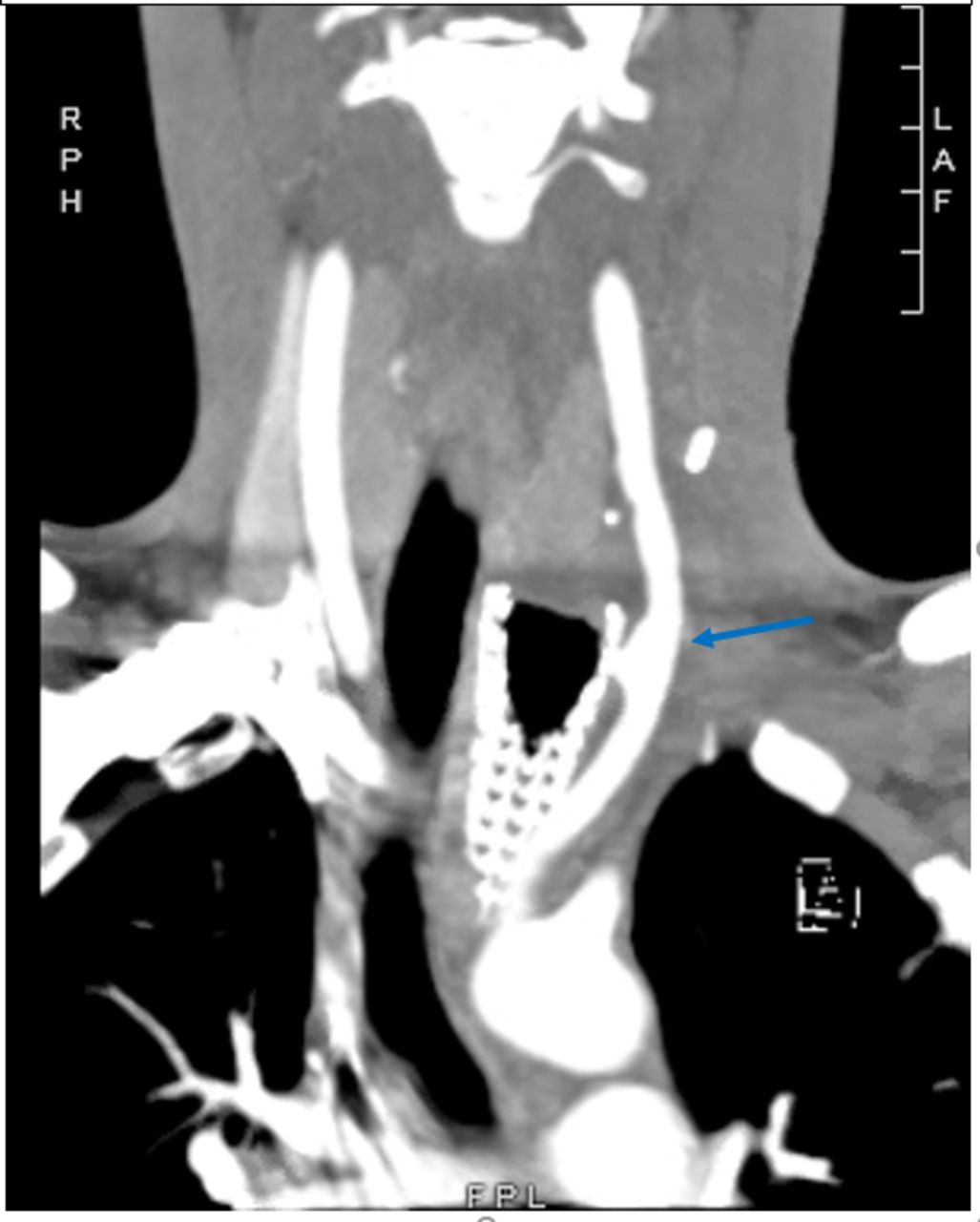
After the administration of a cephalosporin antibiotic, the patient was taken to the operating room. Flexible esophagoscopy was performed and showed irregularities in the esophagus at 20 cm from the incisors (figure 3). The patient’s head was then rotated to the right on the operating room table, and his neck and entire chest were prepped and draped into the field. A left oblique, cervical incision was made anterior to the sternocleidomastoid muscle, which was retracted laterally. The facial vein was divided and ligated. The left common carotid artery was exposed to the point where it disappeared behind the sternum. A small ecchymosis was noted on the common carotid artery but no defect or irregularities were palpated. The dissection then proceeded medially, and the esophagus was exposed. It was dissected circumferentially and looped with a Penrose drain. After extensive mobilization protecting the left recurrent laryngeal nerve, the esophagus was then retracted cephalad and two large perforations comprising approximately 75% of the circumference were identified. The defects were closed with an inner layer of interrupted 4–0 vicryl sutures on the mucosa and a layer of 3–0 silk sutures on the muscularis propria. A leak test was performed and was negative. A silastic drain was left in the retroesophageal space extending down into the posterior mediastinum. A postoperative CT arteriogram of the neck obtained the same day documented that the intimal defect of the left common carotid artery was now a small pseudoaneurysm. During the next few days, minimal output was noted from the drain, and the patient was advanced to a clear liquid diet. On postoperative day 8, he had bloody output from the drain as well as hematemesis. A CT scan with oral contrast confirmed an esophageal leak. He was taken back to the operating room and found to have a small defect on the medial aspect of the left common carotid artery. This was debrided and a bovine pericardial patch was placed. A left sternocleidomastoid muscle flap was placed between the esophagus and the carotid patch, and a new silastic drain was inserted. Two days later, a covered esophageal stent was placed by the gastroenterology service and his diet was slowly advanced. On postoperative day 38 from his index operation, the esophageal stent was removed and a persistent esophageal defect was noted with the cervical drain visible through the defect on endoscopy. The drain was removed, and the esophageal stent was replaced. Two weeks later, he developed hematemesis and represented to the hospital. A CT arteriogram demonstrated a new left common carotid artery pseudoaneurysm at the level of the proximal end of the esophageal stent (figure 4). This was covered with 10×8 mm endovascular stent. Endoscopy demonstrated an ulcer at 30 cm from the incisors and a healed perforation at 20 cm from the incisors after removal of the stent. A subsequent esophagram did not demonstrate a leak. He was slowly advanced from a liquid to a soft diet during 2 days and discharged home.

Initial endoscopy demonstrating defects in the esophagus (arrows).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Common carotid artery pseudoaneurysm at the level of the proximal end of the esophageal stent (arrow).
Discussion
The most appropriate management of a small asymptomatic, intimal defect after a penetrating injury to the carotid artery is unclear. Much of our knowledge about the management of penetrating carotid injuries comes from symptomatic patients with ‘hard’ signs of a vascular injury or those with a positive arteriogram after presenting with ‘soft’ signs of vascular injury. The historic algorithm is quite clear in terms of operative repair in these latter patients with a penetrating wound to the artery.1
Options at operation for management of the injury to the common carotid artery noted on the original CT-arteriography in the patient described were as follows: (1) observation/palpation and postoperative administration of unfractionated heparin (much as if this was a Grade I–II blunt cerebrovascular injury); (2) intraoperative vascular ultrasound of the area to analyze extent of intimal injury and need for arteriotomy with intimal repair or (3) arteriotomy with intimal repair vs resection and end-to-end anastomosis or insertion of interposition graft. The observation/palpation approach was chosen, but a postoperative CT arteriogram documented that a traumatic false aneurysm was present. In retrospect, immediate insertion of an endovascular stent graft or reoperation with arterial repair would have been appropriate.
In the modern era, the other controversy is whether open repair of the stable patient with a penetrating wound to the carotid artery should be replaced by an endovascular approach.2 In a retrospective series of 19 patients with penetrating carotid injuries from stab wounds, treatment with stent grafts was successful both immediately and in the long term for 17 patients. One patient died early in the postoperative period from cerebral edema and another died after occlusion of the stent and secondary neurologic injury.3
Repairs of concomitant injuries to the carotid artery and esophagus, carotid artery and trachea, and trachea and esophagus should be separated by a viable muscle flap. The reason for this is the up to 20% to 25% leak rate after repairs of penetrating injuries to the cervical esophagus. The sternocleidomastoid muscle is ideal for this purpose, as its tripartite blood supply allows for the sternal head or entire inferior (or superior) muscle to be easily detached and rotated to cover the esophageal repair although remaining well vascularized.4 Another consideration is careful placement of any cervical drain in a position that prevents contact with the repair of the carotid artery.
Cervical esophageal leaks can be managed expectantly if adequately drained, as most will spontaneously close over time.5 With the advent of advanced endoscopic techniques, covered stents are being increasingly utilized as an adjunct to drainage when a gastrointestinal leak occurs. Insertion of a stent in the patient described allowed for early resumption of oral intake without fear of enlarging the underlying perforation. The patient did, however, subsequently develop a traumatic false aneurysm of the common carotid artery in close proximity to the esophageal stent, raising the question as to whether direct contact with the stent led to the development of this new lesion. A systematic review of several small, retrospective studies of esophageal perforations and/or leaks treated with stent therapy documented clinical success rates as high as 81%, although much of the data are from patients with iatrogenic perforations and elective esophagectomies.6 The risks of esophageal stent placement in the setting of concomitant injuries to the esophagus and carotid artery are unknown.
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.