
Abstract
Background
In 1997, examination of at least 15 lymph nodes was recommended for adequate gastric cancer staging. However, the proportion of patients undergoing an adequate lymph node examination (LNE) has not been studied in a population-based manner.
Methods
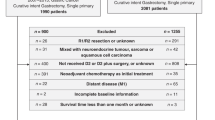
We used Surveillance, Epidemiology, and End Results cancer registry data to assess LNE adequacy in adults with nonmetastatic gastric adenocarcinoma. We selected patients aged 18 through 80 years whose disease was diagnosed from 1998 through 2001 and who underwent at least partial gastrectomy. We evaluated the overall number of nodes, estimated the likelihood of adequate LNE (i.e., ≥15 nodes examined), and determined the influence of selected tumor and patient characteristics on LNE.
Results
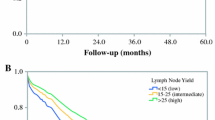
In this 4-year period, 3593 patients met our study’s selection criteria. The median number of nodes examined was 10: 32% of patients underwent adequate LNE, and 9% of patients had no nodes examined. Node-positive patients were more likely to have undergone an adequate LNE than node-negative patients (42% vs. 23%; P < .0001). Younger age, female sex, and more radical surgery were associated with adequate LNE in both univariate and multivariate analysis (P < .0001). Geographical site was an important predictor; patients from one registry (Hawaii) were significantly more likely to have undergone adequate LNE than patients from all other registries (56% vs. 30%; P < .0001).
Conclusions
Our 4-year review of the Surveillance, Epidemiology, and End Results database revealed that only a third of patients with gastric cancer underwent adequate LNE, i.e., had the recommended minimum of 15 nodes examined for gastric cancer staging. Better results at one registry (Hawaii) indicate that substantial improvements could be made.


Similar content being viewed by others

References
American Cancer Society. 2005 Cancer facts and figures. Available at: http://www.cancer.org/downloads/STT/CAFF 2005f4PWSecured.pdf. Accessed: February 15, 2005
Sobin LH, Wittekind C. TNM Classification of Malignant Tumors. 5th ed. New York: Wiley, 1997
Fleming ID, Cooper JS, Henson DE, et al., eds. American Joint Committee on Cancer Staging Manual. 5th ed. Philadelphia: Lippincott-Raven, 1997
Beahrs OH, Henson DE, Hutter RVP, Kennedy BJ, eds. American Joint Committee on Cancer Manual for Staging of Cancer. 4th ed. Philadelphia: JB Lippincott, 1992
Wanebo HJ, Kennedy BJ, Chmiel J, Steele G Jr, Winchester D, Osteen R. Cancer of the stomach. A patient care study by the American College of Surgeons. Ann Surg 1993;218:583–92
Wanebo HJ, Kennedy BJ, Winchester DP, Fremgen A, Stewart AK. Gastric carcinoma: does lymph node dissection alter survival? J Am Coll Surg 1996;183:616–24
Surveillance, Epidemiology, and End Results. Overview of SEER. Available at: http://seer.cancer.gov/ . Accessed: February 15, 2005
Baxter NN, Virnig DJ, Rothenberger DA, Morris AM, Jessurun J, Virnig BA. Lymph node evaluation in colorectal cancer patients: a population-based study. J Natl Cancer Inst 2005;97:219–25
Maruyama K. Surgical Treatment and End Results of Gastric Cancer. Tokyo: National Cancer Center Press, 1987
Hundahl SA, Menck HR, Mansour EG, Winchester DP. The National Cancer Data Base report on gastric carcinoma. Cancer 1997;80:2333–41
Kajitani T. Japanese Research Society for the Study of Gastric Cancer. The general rules for gastric cancer study in surgery and pathology. Jpn J Surg 1981;11:127–45
Bonenkamp JJ, Hermans J, Sasako M, van de Velde CJ. Extended lymph-node dissection for gastric cancer. Dutch Gastric Cancer Group. N Engl J Med 1999;340:908–14
Cuschieri A, Fayers P, Fielding J, et al. Postoperative morbidity and mortality after D1 and D2 resections for gastric cancer: preliminary results of the MRC randomised controlled surgical trial. The Surgical Cooperative Group. Lancet 1996;347:995–9
Cuschieri A, Weeden S, Fielding J, et al. Patient survival after D1 and D2 resections for gastric cancer: long-term results of the MRC randomized surgical trial. Surgical Co-operative Group. Br J Cancer 1999;79:1522–30
Sasako M. Risk factors for surgical treatment in the Dutch Gastric Cancer Trial. Br J Surg 1997;84:1567–71
Bonenkamp JJ, Songun I, Hermans J, et al. Randomised comparison of morbidity after D1 and D2 dissection for gastric cancer in 996 Dutch patients. Lancet 1995;345:745–8
Schwarz RE, Smith DD. Clinical impact of lymphadenectomy extent in resectable, advanced-stage gastric cancer. In: Proceedings of the American Society of Clinical Oncology GI Cancers Symposium, 2005, p 85
Karpeh MS, Leon L, Klimstra D, Brennan MF. Lymph node staging in gastric cancer: is location more important than number? An analysis of 1,038 patients. Ann Surg 2000;232:362–71
Hundahl SA, Macdonald JS, Benedetti J, Fitzsimmons T. Surgical treatment variation in a prospective, randomized trial of chemoradiotherapy in gastric cancer: the effect of undertreatment. Ann Surg Oncol 2002;9:278–86
Hayashi H, Ochiai T, Suzuki T, et al. Superiority of a new UICC-TNM staging system for gastric carcinoma. Surgery 2000;127:129–35
Lee HK, Yang HK, Kim WH, Lee KU, Choe KJ, Kim JP. Influence of the number of lymph nodes examined on staging of gastric cancer. Br J Surg 2001;88:1408–12
Hundahl SA, Phillips JL, Menck HR. The National Cancer Data Base Report on poor survival of U.S. gastric carcinoma patients treated with gastrectomy: fifth edition American Joint Committee on Cancer staging, proximal disease, and the “different disease” hypothesis. Cancer 2000;88:921–32
Gorog D, Nagy P, Peter A, Perner F. Influence of obesity on lymph node recovery from rectal resection specimens. Pathol Oncol Res 2003;9:180–3
Deurenberg P, Yap M, van Staveren WA. Body mass index and percent body fat: a meta-analysis among different ethnic groups. Int J Obes Relat Metab Disord 1998;22:1164–71
Candela FC, Urmacher C, Brennan MF. Comparison of the conventional method of lymph node staging with a comprehensive fat-clearing method for gastric adenocarcinoma. Cancer 1990;66:1828–32
Bunt AM, Hermans J, van de Velde CJ, et al. Lymph node retrieval in a randomized trial on Western-type versus Japanese-type surgery in gastric cancer. J Clin Oncol 1996;14:2289–94
Acknowledgments
The authors thank Dr. Mary Knatterud for her helpful editorial suggestions. Supported, in part, by the University of Minnesota Comprehensive Cancer Center. Both authors are supported by University of Minnesota Cancer Center Clinical Scholar Awards. N.N.B. is supported by an American Society of Clinical Oncology Career Development Award.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Baxter, N.N., Tuttle, T.M. Inadequacy of Lymph Node Staging in Gastric Cancer Patients: A Population-Based Study. Ann Surg Oncol 12, 981–987 (2005). https://doi.org/10.1245/ASO.2005.03.008
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/ASO.2005.03.008