
Abstract
Background
Despite regular surveillance colonoscopy, the metachronous colorectal cancer risk for mismatch repair (MMR) gene mutation carriers after segmental resection for colon cancer is high and total or subtotal colectomy is the preferred option. However, if the index cancer is in the rectum, management decisions are complicated by considerations of impaired bowel function. We aimed to estimate the risk of metachronous colon cancer for MMR gene mutation carriers who underwent a proctectomy for index rectal cancer.
Methods
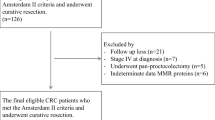
This retrospective cohort study comprised 79 carriers of germline mutation in a MMR gene (18 MLH1, 55 MSH2, 4 MSH6, and 2 PMS2) from the Colon Cancer Family Registry who had had a proctectomy for index rectal cancer. Cumulative risks of metachronous colon cancer were calculated using the Kaplan–Meier method.
Results
During median 9 years (range 1–32 years) of observation since the first diagnosis of rectal cancer, 21 carriers (27 %) were diagnosed with metachronous colon cancer (incidence 24.25, 95 % confidence interval [CI] 15.81–37.19 per 1,000 person-years). Cumulative risk of metachronous colon cancer was 19 % (95 % CI 9–31 %) at 10 years, 47 (95 % CI 31–68 %) at 20 years, and 69 % (95 % CI 45–89 %) at 30 years after surgical resection. The frequency of surveillance colonoscopy was 1 colonoscopy per 1.16 years (95 % CI 1.01–1.31 years). The AJCC stages of the metachronous cancers, where available, were 72 % stage I, 22 % stage II, and 6 % stage III.
Conclusions
Given the high metachronous colon cancer risk for MMR gene mutation carriers diagnosed with an index rectal cancer, proctocolectomy may need to be considered.

Similar content being viewed by others

References
Jenkins MA, Baglietto L, Dowty JG, Van Vliet CM, Smith L, Mead LJ, et al. Cancer risks for mismatch repair gene mutation carriers: a population-based early onset case-family study. Clin Gastroenterol Hepatol. 2006;4:489–98.
Baglietto L, Lindor NM, Dowty JG, White DM, Wagner A, Gomez Garcia EB, et al. Risks of Lynch syndrome cancers for MSH6 mutation carriers. J Natl Cancer Inst. 2010;102:193–201.
Senter L, Clendenning M, Sotamaa K, Hampel H, Green J, Potter JD, et al. The clinical phenotype of Lynch syndrome due to germ-line PMS2 mutations. Gastroenterology. 2008;135:419–28.
Bonadona V, Bonaiti B, Olschwang S, Grandjouan S, Huiart L, Longy M, Guimbaud R, et al. Cancer risks associated with germline mutations in MLH1, MSH2, and MSH6 genes in Lynch syndrome. JAMA. 2011;305:2304–10.
Vasen HFA, Abdirahman M, Brohet R, Langers AM, Kleibeuker JH, van Kouwen M, et al. One to 2-Year Surveillance Intervals Reduce Risk of Colorectal Cancer in Families With Lynch Syndrome. Gastroenterology. 2010;138:2300–6.
Parry S, Win AK, Parry B, Macrae FA, Gurrin LC, Church JM, et al. Metachronous colorectal cancer risk for mismatch repair gene mutation carriers: the advantage of more extensive colon surgery. Gut. 2011;60:950–7.
Kalady MF. Surgical management of hereditary nonpolyposis colorectal cancer. Adv Surg. 2011;45:265–74.
Kalady MF, Lipman J, McGannon E, Church JM. Risk of colonic neoplasia after proctectomy for rectal cancer in hereditary nonpolyposis colorectal cancer. Ann Surg. 2012;255:1121–5.
Coffey JC, Winter DC, Neary P, Murphy A, Redmond HP, Kirwan WO. Quality of life after ileal pouch-anal anastomosis: an evaluation of diet and other factors using the Cleveland Global Quality of Life instrument. Dis Colon Rectum. 2002;45:30–8.
Delaney CP, Fazio VW, Remzi FH, Hammel J, Church JM, Hull TL, et al. Prospective, age-related analysis of surgical results, functional outcome, and quality of life after ileal pouch-anal anastomosis. Ann Surg. 2003;238:221–8.
Fazio VW, Ziv Y, Church JM, Oakley JR, Lavery IC, Milsom JW, et al. Ileal pouch-anal anastomoses complications and function in 1005 patients. Ann Surg. 1995;222:120–7.
Lee JS, Petrelli NJ, Rodriguez-Bigas MA. Rectal cancer in hereditary nonpolyposis colorectal cancer. Am J Surg. 2001;181:207–10.
Moslein G, Nelson H, Thibodeau S, Dozois RR. [Rectal carcinomas in HNPCC]. Langenbecks Arch Chir Suppl Kongressbd. 1998;115:1467–9.
Newcomb PA, Baron J, Cotterchio M, Gallinger S, Grove J, Haile R, et al. Colon Cancer Family Registry: an international resource for studies of the genetic epidemiology of colon cancer. Cancer Epidemiol Biomarkers Prev. 2007;16:2331–43.
Southey MC, Jenkins MA, Mead L, Whitty J, Trivett M, Tesoriero AA, et al. Use of molecular tumor characteristics to prioritize mismatch repair gene testing in early-onset colorectal cancer. J Clin Oncol. 2005;23:6524–32.
Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, editors. AJCC Cancer Staging Manual. 7th ed. New York: Springer; 2010.
Win AK, Young JP, Lindor NM, Tucker KM, Ahnen DJ, Young GP, et al. Colorectal and other cancer risks for carriers and noncarriers from families with a DNA mismatch repair gene mutation: a prospective cohort study. J Clin Oncol. 2012;30:958–64.
Rogers WH. Regression standard errors in clustered samples. Stata Tech Bull. 1993;3:19–23.
Williams RL. A note on robust variance estimation for cluster-correlated data. Biometrics. 2000;56:645–6.
Stata Statistical Software: Release 11 [computer program]. College Station: StataCorp LP; 2009.
Young J, Simms LA, Biden KG, Wynter C, Whitehall V, Karamatic R, et al. Features of colorectal cancers with high-level microsatellite instability occurring in familial and sporadic settings: parallel pathways of tumorigenesis. Am J Pathol. 2001;159:2107–16.
Lynch HT, de la Chapelle A. Hereditary colorectal cancer. N Engl J Med. 2003;348:919–32.
Pohl H, Robertson DJ. Colorectal cancers detected after colonoscopy frequently result from missed lesions. Clin Gastroenterol Hepatol. 2010;8:858–64.
Martinez ME, Baron JA, Lieberman DA, Schatzkin A, Lanza E, Winawer SJ, et al. A pooled analysis of advanced colorectal neoplasia diagnoses after colonoscopic polypectomy. Gastroenterology. 2009;136:832–41.
Acknowledgment
The authors thank all study participants of the Colon Cancer Family Registry and staff for their contributions to this project.
Disclosure
The authors have no conflict of interest to declare with respect to this manuscript.
Funding
This work was supported by the National Cancer Institute, National Institutes of Health under RFA #CA-95-011 and through cooperative agreements with members of the Colon Cancer Family Registry and Principal Investigators. Collaborating centers include Australasian Colorectal Cancer Family Registry (U01 CA097735), Familial Colorectal Neoplasia Collaborative Group (U01 CA074799) [USC], Mayo Clinic Cooperative Family Registry for Colon Cancer Studies (U01 CA074800), Ontario Registry for Studies of Familial Colorectal Cancer (U01 CA074783), Seattle Colorectal Cancer Family Registry (U01 CA074794), and University of Hawaii Colorectal Cancer Family Registry (U01 CA074806). AKW is supported by the Picchi Brothers Foundation Cancer Council Victoria Cancer Research Scholarship, Australia. MAJ is a Senior Research Fellow and JLH is an Australia Fellow of the National Health and Medical Research Council, Australia.
Author information
Authors and Affiliations
Corresponding author
Additional information
A. K. Win, S. Parry equally contributed to this work.
(1) 15th Annual Meeting of Collaborative Group of the Americas on Inherited Colorectal Cancer (CGA-ICC), Montreal, Canada, Oct 10–11, 2011. Metachronous colon cancer risk following surgery for first primary rectal cancer in Lynch syndrome.
(2) Digestive Disease Week, San Diego, CA, May 19–22, 2012. Metachronous colon cancer risk following surgery for first rectal cancer in mismatch repair gene mutation carriers.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Win, A.K., Parry, S., Parry, B. et al. Risk of Metachronous Colon Cancer Following Surgery for Rectal Cancer in Mismatch Repair Gene Mutation Carriers. Ann Surg Oncol 20, 1829–1836 (2013). https://doi.org/10.1245/s10434-012-2858-5
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-012-2858-5