
Abstract
Background
Pelvic exenteration has increasingly been shown to improve disease-free and overall survival for patients with locally advanced pelvic malignancies. Squamous cell carcinoma (SCC) is the second most common pelvic malignancy requiring exenteration.
Objective
The aim of this study was to report the clinical and oncological outcomes from patients treated with pelvic exenteration for anal and urogenital SCC from a single, high-volume unit.
Methods
A review of a prospectively maintained database from 1991 to 2018 at a high-volume specialised institution was performed. Primary endpoints included R0 resection rates, local recurrence and overall survival (OS) rates.
Results
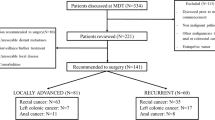
From January 1999 to July 2018, 361 patients underwent pelvic exenteration of which 31 patients were identified with SCC (15 anal SCC, 16 urogenital SCC). The majority of patients were females (n = 24, 77.4%). Median age was 59 (range 35–81). Twenty-seven patients underwent resection with curative intent with an R0 resection rate of 81.5%. Four patients underwent a palliative procedure [R1 = 3 (8%), R2 = 1 (3.3%)]. Mean hospital length of stay was 32 days (range 8–122 days). Disease-free survival was significantly increased in anal SCC with no significant difference in OS compared to urogenital SCC (p = 0.03, p = 0.447 respectively). Advanced pathological T stage was associated with decreased OS (p = 0.023). In the curative intent group the disease-free survival and OS rate was 59.3% and 70% at 24 months, respectively.
Conclusion
Complete R0 resection is achievable in a high proportion of patients. Urogenital SCC is associated with significantly worse disease-free survival, and advanced T-stage was a significant prognostic factor for OS.


Similar content being viewed by others

References
Brunschwig A. Complete excision of pelvic viscera in the male for advanced carcinoma of the sigmoid invading the urinary bladder. Ann Surg. 1949;129(4):499–504.
Brown KGM, Solomon MJ, Koh CE. Pelvic exenteration surgery: the evolution of radical surgical techniques for advanced and recurrent pelvic malignancy. Dis Colon Rectum. 2017;60(7):745–54.
Quyn AJ, Austin KK, Young JM, Badgery-Parker T, Masya LM, Roberts R, Solomon MJ. Outcomes of pelvic exenteration for locally advanced primary rectal cancer: overall survival and quality of life. Eur J Surg Oncol. 2016;42(6):823–8. https://doi.org/10.1016/j.ejso.2016.02.016.
PelvEx Collaborative. Surgical and survival outcomes following pelvic exenteration for locally advanced primary rectal cancer: results from an international collaboration. Ann Surg. 2019;269(2):315–321.
Ferenschild FTJ, Vermaas M, Verhoef C, Ansink AC, Kirkels WJ, Eggermont AMM, et al. Total pelvic exenteration for primary and recurrent malignancies. World J Surg. 2009;33(7):1502–8.
Grulich AE, Poynten IM, Machalek DA, Jin F, Templeton DJ, Hillman RJ. The epidemiology of anal cancer. Sex Health. 2012;9(6):504–8.
Barnholtz-Sloan JS, Maldonado JL, Pow-sang J, Giuliano AR. Incidence trends in primary malignant penile cancer. Urol Oncol. 2007. 25(5):361–7.
Nigro ND, Seydel HG, Considine B, Vaitkevicius VK, Leichman L, Kinzie JJ. Combined preoperative radiation and chemotherapy for squamous cell carcinoma of the anal canal. Cancer. 1983;51(10):1826–9.
Schiller DE, Cummings BJ, Rai S, et al. Outcomes of salvage surgery for squamous cell carcinoma of the anal canal. Ann Surg Oncol. 2007;14:2780–9.
Eeson G, Foo M, Harrow S, McGregor G, Hay J. Outcomes of salvage surgery for epidermoid carcinoma of the anus following failed combined modality treatment. Am J Surg. 2011;201:628–33.
van der Wal BCH, Cleffken BI, Gulec B, Kaufman HS, Choti MA. Results of salvage abdominoperineal resection for recurrent anal carcinoma following combined chemoradiation therapy. J Gastrointest Surg. 2001;5(4):383–7.
Minhas, S., Kayes, O., Hegarty, P., Kumar, P., Freeman, A. and Ralph, D. What surgical resection margins are required to achieve oncological control in men with primary penile cancer? BJU Int. 2005;96:1040–3.
Yang HY, Park SC, Hyun JH, Seo HK, Oh JH. Outcomes of pelvic exenteration for recurrent or primary locally advanced colorectal cancer. Ann Surg Treat Res. 2015;89(3):131–7.
Hall BL, Hamilton BH, Richards K, Bilimoria KY, Cohen ME, Ko CY. Does surgical quality improve in the American College of Surgeons National Surgical Quality Improvement Program: an evaluation of all participating hospitals. Ann Surg. 2009;250(3):363–76.
Pawlik TM, Skibber JM, Rodriguez-Bigas MA. Pelvic exenteration for advanced pelvic malignancies. Ann Surg Oncol. 2006;13(5):612.
Ogura A, Akiyoshi T, Konishi T, et al. Safety of laparoscopic pelvic exenteration with urinary diversion for colorectal malignancies. World J Surg. 2016;40(5):1236.
Tan KK, Pal S, Lee PJ, Rodwell L, Solomon MJ. Pelvic exenteration for recurrent squamous cell carcinoma of the pelvic organs arising from the cloaca—a single institution’s experience over 16 years. Colorectal Dis. 2013;15(10):1227–31.
Aleksic I, Rais-Bahrami S, Daugherty M, Agarwal PK, Vourganti S, Bratslavsky G. Primary urethral carcinoma: a surveillance, epidemiology, and end results data analysis identifying predictors of cancer-specific survival. Urol Ann. 2018;10(2):170–74. https://doi.org/10.4103/ua.ua_136_17.
Flam M, John M, Pajak TF, Petrelli N, Myerson R, Doggett S, et al. Role of mitomycin in combination with fluorouracil and radiotherapy, and of salvage chemoradiation in the definitive nonsurgical treatment of epidermoid carcinoma of the anal canal: results of a phase III randomized intergroup study. J Clin Oncol. 1996; 14(9):2527–39.
Ajani JA, Winter KA, Gunderson LL, et al. Inter-group RTOG 98-11: a phase III randomized study of 5-fluoruracil (5-FU), mitomycin, and radiotherapy versus 5-fluorouracil, cisplatin and radiotherapy in carcinoma of the anal canal. J Clin Oncol. 2006;24:180s.
Das P, Bhatia S, Eng C, Ajani JA, Skibber JM, Rodriguez-Bigas MA, Chang GJ, Bhosale P, Delclos ME, Krishnan S, Janjan NA, Crane CH. Predictors and patterns of recurrence after definitive chemoradiation for anal cancer. Int J Radiat Oncol Biol Phys. 2007; 68(3):794–800.
Glynne-Jones R, James R, Meadows H, et al. Optimum time to assess complete clinical response (CR) following chemoradiation (CRT) using mitomycin (MMC) or cisplatin (CisP), with or without maintenance CisP/5FU in squamous cell carcinoma of the anus: results of ACT II. 2012 ASCO annual meeting. J Clin Oncol. 2012;30:abstr 4004.
UKCCCR. Epidermoid anal cancer: results from the UKCCCR randomised trial of radiotherapy alone versus radiotherapy, fluorouracil, and mitomycin. UKCCCR Anal Cancer Trial Working Party. UK Co-ordinating Committee on Cancer Research. Lancet. 1996;348:1049–54.
SEER Stat Fact Sheets: Anal Cancer. NIH Surveillance, Epidemiology and End Results Program. http://seer.cancer.gov/statfacts/html/anus.html. Accessed 5 Sept 2018.
Nelson AM, Albizu-Jacob A, Fenech AL, Chon HS, Wenham RM, Donovan KA. Quality of life after pelvic exenteration for gynecologic cancer: findings from a qualitative study. Psychooncology. 2018;27(10):2357–62. https://doi.org/10.1002/pon.4832.
Armbruster SD, Sun CC, Westin SN, Bodurka DC, Ramondetta L, Meyer LA, et al. Prospective assessment of patient-reported outcomes in gynecologic cancer patients before and after pelvic exenteration. Gynecol Oncol. 2018;149(3):484–490. https://doi.org/10.1016/j.ygyno.2018.03.054.
Lau YC, Brown KG, Lee P. Pelvic exenteration for locally advanced and recurrent rectal cancer—How much more? J Gastrointest Oncol. 2019. https://doi.org/10.21037/jgo.2019.01.21.
Lago V, Poveda I, Padilla-Iserte P, et al. Pelvic exenteration in gynecologic cancer: complications and oncological outcome. Gynecol Surg. 2019;16:1. https://doi.org/10.1186/s10397-019-1055-y.
Diver EJ, Rauh-Hain JA, Del Carmen MG. Total pelvic exenteration for gynecologic malignancies. Int J Surg Oncol. 2012;2012:693535.
Ahmadi N, Tan K-K, Solomon MJ, Al-Mozany N, Carter J. Pelvic exenteration for primary and recurrent gynecologic malignancies is safe and achieves acceptable long-term outcomes. J Gynecol Surg. 2014;30(5):255–9.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Nicholas Smith and Peadar S. Waters are co-first authors.
Rights and permissions
About this article

Cite this article
Smith, N., Waters, P.S., Peacock, O. et al. Pelvic Exenteration for Anal and Urogenital Squamous Cell Carcinoma: Experience and Outcomes from an Exenteration Unit Over 12 Years. Ann Surg Oncol 27, 2450–2456 (2020). https://doi.org/10.1245/s10434-020-08229-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-020-08229-8