Stress reduction through needs-oriented interior design
 Ute Ziegler,
Ute Ziegler,  Nicole Hartmann
Nicole Hartmann Based on two application-oriented research projects 2012-2014 Modular Cocoon and 2019-2022 Cocoon 2.0, which have been carried out in a Swiss psychiatric hospital, it is presented how a systemic research approach is used to implement a needs-oriented design that can address the needs of different disease patterns, gender and age with individualizable elements. In hospitals, there are numerous stressors for patients. Regardless of different previous experiences, these are perceived differently and also affect individuals on different physical and psychological levels. Accordingly, the question of which design elements in which configuration and design form are suitable for reducing stress and states of arousal individually was investigated. The research process is divided into four phases for each project: 1st phase: Site inspections, observation and measurement of the actual state. 2nd phase: Co-creations and Co-Designs with the relevant stakeholders 3nd phase: Data analysis, derivation of concept ideas and construction of prototype 4th phase: Implementation of prototype and testing In both tests, it has been shown that stress-reducing effects can be presented at different levels in all patients through the individual appropriation possibilities created by the configuration of the parameters wood, light and textile. The prototypes of both research projects have influence on the feeling of security and safety, which is related to well-being. The empirical data clearly show that the design approach of individualization enables patients to self-regulate, i.e. the configurability of the design parameters enables patients to self-regulate their stress.
Show LessTrack Title: Integration of needs
Stress reduction through needs-oriented interior design
Ute Ziegler, ute.ziegler@hslu.ch, Nicole Hartmann, nicole.hartmann@hslu.ch
Names of the Topic editors: Clarine van Oel Names of the reviewers: Jonathan Erskine Liesbeth van Heel Journal: The Evolving Scholar DOI: https://doi.org/10.24404/6230cefec681d9bb8216afce Submitted: 24 Jul 2022 Accepted: 22 August 2022 Published: 9 January 2024 Citation: Ziegler, U. & Hartmann, N. (2022). Stress reduction through needs-oriented interior design [preprint]. The Evolving Scholar | ARCH22. This work is licensed under a Creative Commons Attribution BY license (CC BY). © 2022 Ziegler, U. & Hartmann, N.] published by TU Delft OPEN on behalf of the authors. |
|---|
Abstract: Based on two application-oriented research projects, 2012-2014 Modular Cocoon and 2019-2022 Cocoon 2.0, which have been carried out in a Swiss psychiatric hospital, it is presented how a systemic research approach is used to implement a needs-oriented design that can address the needs of different disease patterns, gender, and age with individualizable elements. In hospitals, there are numerous stressors for patients. Regardless of previous experiences, these are perceived differently and also affect individuals on different physical and psychological levels. Accordingly, the question of which design elements in which configuration and design form are suitable for reducing stress and states of arousal individually was investigated. The research process is divided into four phases for each project:
1st phase: Site inspections, observation, and measurement of the actual state.
2nd phase: Co-creations and Co-Designs with the relevant stakeholders
3rd phase: Data analysis, derivation of concept ideas, and construction of prototype
4th phase: Implementation of prototype and testing
In both tests, it has been shown that stress-reducing effects can be presented at different levels in almost all patients through the individual appropriation possibilities created by the configuration of the parameters wood, light and textile. The prototypes of both research projects have influence on the feeling of security and safety, which is related to well-being.
The empirical data clearly show that the design approach of Self-Organized Design enables patients to self-regulate, i.e., the configurability of the design parameters enables patients to self-regulate their stress.
Keywords: Stress reduction, needs-oriented design, co-creations, individualization, enabling
1. Introduction
This paper describes two research projects and the development of two prototypes in a psychiatric clinic in Switzerland. In a participatory process with caregivers, patients, doctors, therapists, and researchers, two distinct prototypes, 'modular cocoon' and ' cocoon 2.0', were developed as a place for patients to retreat into. The prototypes were developed and tested over several months during two consecutive periods ( 2012-2014 and 2018-2022). The intention was to develop environments for the reduction of elevated states of arousal and stress in traumatized patients. The project aimed to answer the question: Which room parameters in which configuration are appropriate to enable an individual retreat for psychologically traumatized patients and to reduce stress?
Modular Cocoon
For the development of the modular cocoon after quantitative measurements in a ward for psychologically traumatized patients, qualitative interviews were held with therapists, nurses, and patients. In addition, co-designs were performed with patients. After data analysis, the room parameters of light, colours, and textiles were brought into a framework as a basis for a first prototype modular cocoon, which enabled each patient to design his or her own place of retreat. In the testing phase of the prototype modular cocoon in the ward, possibilities for interaction, variations of use, and the modular cocoon’s function were studied. These patient tests demonstrated effects such as an increased sense of security, improved sleep quality, and less medication at night.

Figure 1. Prototype Modular Cocoon (2012-2014) with a wooden ceiling, biologically effective light (direct and indirect), and different textile layers
For the development of cocoon 2.0 in 2018, the data from the modular cocoon was re-used and supplemented by smaller surveys, leading to the second prototype. The room-in-room construction 'cocoon 2.0' was developed for a new building of the clinic and has to fulfil different requirements.
Cocoon 2.0 and Skylight
Cocoon 2.0 consists of three mobile components that can be used independently of the respective room: a wooden structure with textiles, a screen, and a floor lamp that can be used flexibly and mobilely. The mobile floor lamp 'Skylight' was developed with a therapeutic light effect spectrum that has both biological and emotional light and is controlled via an app. The daylight-like lighting is automated and largely escapes the visual perception of users. For the emotional light, 12 preset nature scenes with colored light were developed (for example, sunrise and sunset), from which the patient can choose. This idea results from the evaluation of the modular cocoon in 2014.
An essential feature of the final design was its flexibility— the potential to change the configuration of the two prototypes by the patients themselves, which came about through their processes of appropriation. The patients adjusted the prototype according to their needs until the effect of the self-perceived stress reduction was registered. Patients reported, among other things, a feeling of security, a more quiet and improved sleep, an increased ability to imagine, fewer stress-related medicines, and a better re-orientation after nightmares.
From the perspective of understanding health and wellbeing, the prototypes and their components of daylight, atmospheric light, wood, and textiles represent a sort of 'environmental catalyst'. These can be seen to promote the patient’s activity and condition depending on this activity, as well as the auto-regulation of patient emotions such as stress and anxiety.
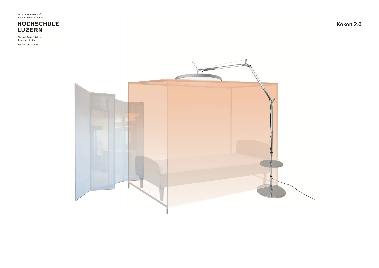
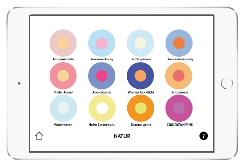
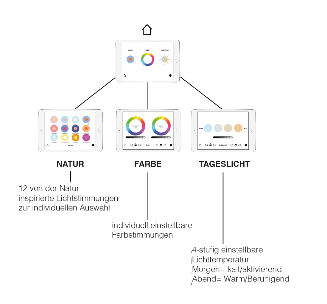
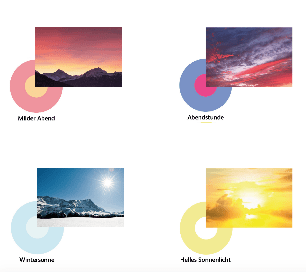
Figure 2. Top left: scheme room-within-a-room. Top right: smartphone app for the selection of the biologically and emotionally effective light. Bottom: the interface of the app shows emotionally effective colored light moods modeled on nature. Visualizations: Nicole Hartmann.
2. Theories and Methods
Evidence-based Design
In the Anglo-Saxon language area, especially in the USA, a movement has emerged since the 1970s that has constituted new concepts and approaches, such as evidence-based design. The pilot study ‘View through a window’ may influence recovery from surgery, conducted from 1972 to 1981, shows very clearly that even a minimal intervention such as visual contact with plants and landscape has a positive effect that supports healing and is associated with a reduction in length of stay and other positive effects. The U.S. architect Roger Ulrich retrospectively examined patient records (1974-1982) of gallbladder surgery patients in a Pittsburgh hospital. One group of patients had a room overlooking a green park with trees, and the other had a room overlooking a brick wall. Ulrich found differences in healing, length of stay, complication rates, and costs between the two groups. The patients with a view of the park were discharged an average of three days earlier and cost $300 less per capita (Ulrich 1984). These findings have prompted a flurry of interdisciplinary studies looking at all factors of a building or space (lighting, layout, materials, sounds, odors, signaling, etc.) in a hospital as well as other buildings. Evidence-based design is based on scientific studies and surveys that investigate and measure the effects of buildings on human recovery. From this, other complementary positions have developed, especially in England.
Experience-based Design, Constructivism, and Participatory Design
Experience-based design is a participatory approach that incorporates the needs of patients even more into the design. In workshops with patients, caregivers, and other stakeholders, ideas and proposed solutions for spaces, processes, and services are developed together and made usable for planning and design (Bate 2007). In this way, a wide range of needs and problems can be addressed that are often not consciously accessible to planners, designers, and health care workers. The positive effects relate to issues such as patient autonomy, control, self-responsibility, and protection of privacy, which have a decisive influence on well-being and, downstream, on recovery.
From a systems theory and constructivist perspective, reality is considered a result of a perception process in its own right. This process is due to the separate conditions of the observer and the idiosyncratic forms of perception and not to a so-called objective reality. Accordingly, the respective reality of each singular patient is constituted by her or his personal observation and perception. Environmental stressors (light - dark, loud - quiet, cold - hot, etc.) are differently perceived, experienced, and interpreted by everyone; therefore, they have different effects. The same “stress dose” can trigger multiple responses in varying organs in different people. The effect depends on the current mental and physical condition of the patient. When transferring this knowledge to the design of hospital environments, it is to be expected that the same standardized patient rooms will have different effects on the individual patient.
Based on this knowledge, we derived collaborative approaches for the design practice, since different people in a system should formulate their own perceptions and experiences of an event to describe and explore this event in a multi-perspective way (von Foerster, 1992). Since the 1980s, this constructivist perspective has given new impetus to design and design research (Jonas, 1994), which distinguishes between different participatory approaches. Participatory design approaches often use this multi-perspective point of view for the development of prototypes. Ideally, prototypes will be co-created by potential users. In the context of the project, we started off with a strong patient-centered approach for a specific patient group. In this patient group, the ideas and wishes of the patients were implemented in a prototype. At the suggestion of doctors and therapists, it was assumed that maximum freedom of choice and control should be given to the patients in both the development and the subsequent use of the artefact (the modular cocoon and the cocoon 2.0).
Self-organization and self-organized design
To maintain or restore their mental balance, traumatized patients need opportunities and offers that respond to their higher state of arousal. A study shows that individual choices and personalization of the environment have a positive significance for wellbeing and the reduction of stress (Ulrich et al., 2006). In a therapeutic sense, a conversation, a stress-reducing drug, or, as shown here, an individually designed non-pharmacological intervention, can provide opportunities for self-organization.
Self-organization in this paper is related to the respective individual use and appropriation of the prototypes of the modular cocoon and cocoon 2.0 by the patients. The different design parameters were developed in such a way that they allowed for a continuous design process of use for patients to achieve an effect of stress reduction. So in this context, self-organization describes the momentum of systemic operations of the external influences of the environment (the technical and social systems) on the systems of the body and psyche. Ideally, the systems of body and psyche will be prevented from experiencing stress development through the customizable external influences of the environment (here the modular cocoon and the cocoon 2.0).
This self-organized process also describes a further development of the concept of design-in-use (Bredies, 2014) with a different focus. During design-in-use, the user determines how, where, and for what purpose artefacts are used;the use itself becomes the design. Also, in the concept of self-organized design, the use itself becomes the design, but in a specific context. First of all, it is intended for the user context of mentally ill people in hospitals. It's primarily about minimizing possible stressors during their stay in the clinic. By providing a customizable environment, patients feel less stressed. Self-organized design describes here the dynamics of the systemic processes of the effects of the environment on psyche and body.
3. Results
The evaluation of the Modular Cocoon in 2014 showed that the seven patients examined experienced a stress-reducing effect on different levels as a result of the appropriation (Table 1 and 2). All patients reported improved sleep, faster reorientation after nightmares, and overall faster calming as a result of the cocoon. Through the individual settings and appropriation of textiles and light, a greater sense of security can be created in the room by the patients themselves (Figure 3).
Figure 3. The patients experimented with the different settings of the Modular Cocoon and very quickly found suitable configurations for themselves. Photos: Benjamin Manser and Ute Ziegler.
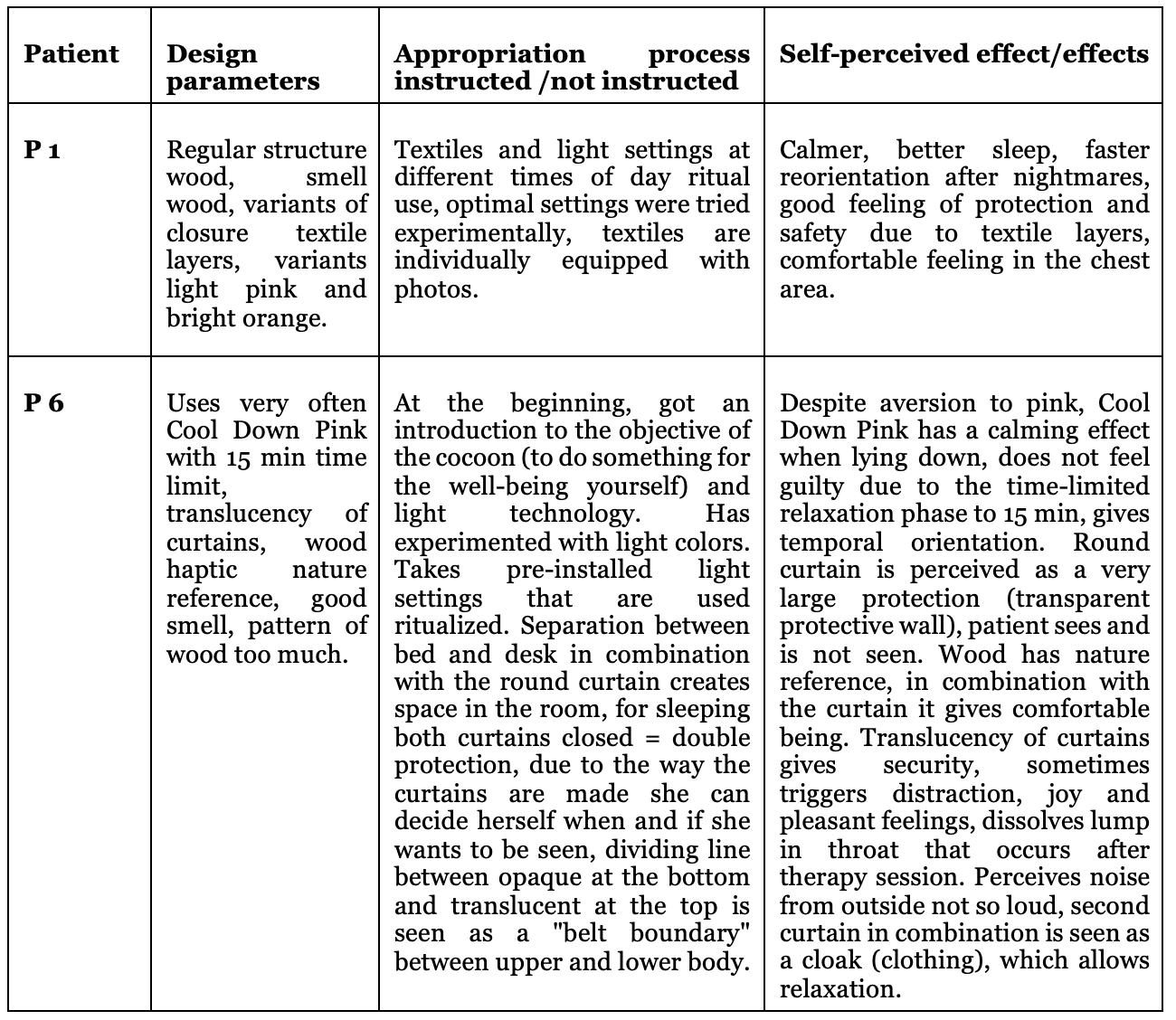
Table 1. The table presents an example of the assessment and evaluation (paraphrased) of two patients who lived in a patient room with a cocoon during their hospital stay. The other five patients also reported stress reducing effects (Ziegler 2021).
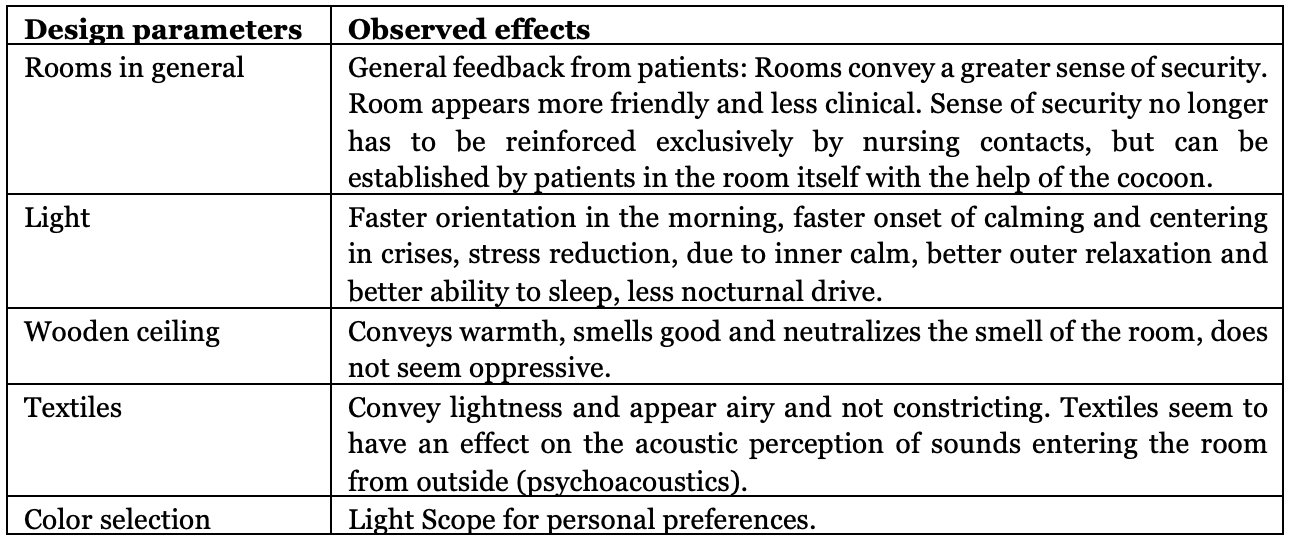
Table 2. The table presents the assessments and effects that were perceived by the nurses and therapists due to the implementation of the cocoon in the patients' rooms. The assessments were gathered through individual interviews.
Results: Cocoon 2.0 and Skylight
Since December 2019 until the interim evaluation in 2021, 15 female patients and two male patients aged 21-63 years have voluntarily completed a questionnaire with 23 questions, the interim results of which are presented as examples. The survey will continue until 30 patients have completed the questionnaire. The questionnaire consists partly of open-ended questions, the answers to which can be formulated by the patients themselves, and partly of questions in which patients can more or less strongly agree or disagree with the question on a five-part scale to measure their personal experience. The respective questions can be answered with not at all, a little, partly, mostly, and very, or with can't/won't.
The interim evaluation of the first 17 questionnaires shows that the use of the Cocoon 2.0 and the Skylight lamp has a great influence on the feeling of security and safety, which is to be seen in connection with well-being. The patients reported positive effects on sleep quality when falling asleep and sleeping through the night. Depending on the situation, the patients also stay in the cocoon during the day and use it specifically to self-regulate their state of arousal. To the question of whether the subjective feeling of stress has been reduced by the use of the cocoon, four participants answered with very much, four with mostly, four with partly and four with a little. When asked if the cocoon reduced the need to take reserve medication, four participants indicated that they needed less reserve medication. Several questions were asked about the light fixture, primarily related to patients' individual attitudes towards the use of daylight and preset nature scenes at different times of day.
As a result, patients use, appreciate, and experiment with the choices. Some use the same settings ritualistically after certain events or at certain times of day, and others keep trying new light variations. For others, however, there are too many choices. To the question of whether cocoon 2.0 has brought a perceived added value in the course of treatment, 14 patients answered in the affirmative and three patients answered in the negative.
Not all 17 patients answered all questions equally. For example, 15 out of 17 patients answered the 7th question: What changes can you perceive by using the cocoon or the individual components?
Pat. responses
P1 Safety calm security warmth
P2 It is like a ritual to prepare the bed in the evening: to close almost all the curtains and thus prepare for sleep; the same in the morning; gradually open the curtains; cozy start
P3 More pleasant mood, more motivation/well-being, and a feeling of security through individual lighting mood, especially in gray weather outside
P4 I feel safe in the four-poster bed and the lighting has a positive effect on my mood.
P5 My sleep pulse has dropped and is more stable (doesn't beat out so extremely) - see thermoprints. I calm down faster in crises and feel safer from external influences.
P6 Safety, security and mood improvement due to the color of the light.
P7 Feel protected and securely supported privacy
P8 Feeling secure
P9 Faster relaxation; feel safe and secure
P10 Curtains make you feel much more protected. With the right lighting, especially in the evenings, you can relax quite well and it creates a "homey" feeling
P11 Secure, new world, takes time to get used to.
P12 Increased calmness, less nervousness
P13 Greater sense of security
P14 I felt safer, more secure, and protected. I felt much more at peace in this room than in the other one. (By ‘the other room’ is meant a patient room without a cocoon.)
P15 Better concentration, better sense of security, more shares show up, my sleep improved. I feel safe and comfortable.



Figure 3. The photographs show three different nature moods: autumn light, warm moonlight, and sunrise, from which the patients can choose. Photos Jürgen Beck.
4. Discussion
The research approach described above is systemic in nature, meaning that all of the parameters described above are evaluated as a whole for their viability and not derived individually. Through the design framework with the textile and the light, a self-controllable external and "internal" protective space can be established. The effect of biologically effective light on psychiatric patients has been proven in numerous quantitative studies. However, there is still very little literature on the effects of atmospheric light. The effect of control is also well researched in environmental and architectural psychology.
The data presented for the two projects was largely collected using qualitative methods. In order to be able to quantify the stress reduction achieved, physiological parameters are also measured in current similar projects, which allows conclusions to be drawn about stress in this respect. In a future project, the measurement results will be extended by measuring the stress hormone cortisol.
5. Conclusions
From the empirical data collected in the patient rooms of the two projects presented here, the design approach of the Self-Organized Design was developed. The Self-Organized Design represents how patients can individually regulate their states of arousal and stress within a framework of predetermined design factors introduced into a standardized patient room. This approach shows how a radically needs-oriented design can be individually tailored to patients in consultation with therapists, physicians, and nurses, given appropriate instruction. Against the background of different experiences, a room for manoeuvre is made available that allows individualization and self-regulation within a defined framework. A patient room designed in this way can thus become a supportive health resource.
Through the cocoons and the lamps, an individual, self-controllable protective zone can be created for patients, which helps them to reduce tension, states of agitation, or stress themselves. Self-design means for patients, on the one hand, more self-determination in the patient's room, but on the other hand, they also take responsibility for themselves. The two cocoons were developed specifically with and for psychologically traumatized patients, but this also means that their principles cannot be arbitrarily transferred to other mental diseases. All of the patients studied used the cocoons to self-regulate their states of arousal and stress. However, it is also conceivable that the cocoons could promote regression in a ward for depressive disorders and possibly have counterproductive effects here.
Data Availability Statement
The data presented are based on a German questionnaire issued to patients by the Clienia Littenheid Clinic. The evaluation is carried out by nursing manager, Mrs. Karen Windmüller karen.windmueller@clienia.ch.
Contributor statement
The luminaire Skylight was developed in collaboration with Moos Licht AG Lucerne and built by Moos Licht.
Acknowledgments
My thanks go to all the staff and patients of Clienia Littenheid who worked on the two cocoons.
References
Bate, P. , et al. (2007). Bringing user experience to healthcare improvement. The concepts, methods and practices of experience-based design. Oxford, England
Bredies, K. (2014). Gebrauch als Design: Über eine unterschätzte Form der Gestaltung. Bielefeld, Deutschland:
Transcript Verlag
Foerster, H. v. (1992). Kypernetische Reflexionen. In: H.R. Fischer Hg., Das Ende der grossen Entwürfe. Frankfurt, Deutschland
Jonas, W. (1994). Design – System – Theorie. Überlegungen zu einem systemtheoretischen Modell von Design-Theorie. Essen, Deutschland
Ulrich, R.S. (1984). View through a Window May Influence Recovery from Surgery, in: Science, New Series, Vol. 224, No. 4647
Ulrich, R.S., et al., (2006). Effects of Interior Design on Wellness. Theory and Recent Scientific Research, J Adv Nurs 56 (2)
Ziegler, U. (2021) Multisensorisches Design als Gesundheitsressource: Individualisierbare und stressregulierende Räume. Ein Systemischer Designansatz, der Design mit Medizin und Neurowissenschaften verbindet. https://doi.org/10.5281/zenodo.4449655
Figures (13)



More details
- License: CC BY
- Review type: Open Review
- Publication type: Conference Paper
- Submission date: 24 July 2022
- Publication date: 9 January 2024
Citation
Ziegler, U. & Hartmann, N. (2024). Stress reduction through needs-oriented interior design. The Evolving Scholar | ARCH22. https://doi.org/10.24404/6230cefec681d9bb8216afce
No reviews to show. Please remember to LOG IN as some reviews may be only visible to specific users.