Mitigating Hospital Design and Delivery Failure: A Retrospective Auto-Ethnography Study
 Anne Symons
Anne Symons There is an urgent need for further research in hospital design and delivery to understand the integrative, nuanced and intricate nature of healthcare project delivery and design management. Historically, each new hospital programme develops a new delivery model that takes a different approach to the management of design. However, this approach is not sustainable. Hospitals have a significant complexity, which may be impacted by role changes and procurement methods which can result in significant errors, costly delays and lack of ability to learn from failure. A retrospective abductive, auto-ethnographic case study approach was taken in the examination of five major hospital projects of similar size and complexity reflecting five temporal periods was carried out by a project architect who subsequently became a construction design manager spanning a career of over 30 years. This variant of action research involved a retrospective mode of abductive reasoning applied retrospectively. An approach to hypothesis testing (using literature) is used to explain and theoretically frame historical practices. It was found that National delivery models (and their change over time) have had a significant influence on hospital project delivery and particularly on design and engineering systems integration. The role standards have played in design have also played a significant role, and in part may have constrained innovation and unduly increased cost. Recommendations are made for a new integrated healthcare delivery model that supports an approach to innovative design and construction of new hospitals responding to advanced clinical and technology approaches.
Show LessFull Paper
Mitigating Hospital Design and Delivery Failure: A Retrospective Auto-ethnography Study
Dr Anne Symons 1,*
1 UCL Bartlett School of Sustainable Construction: anne.symons.14@ucl.ac.uk (corresponding author) ORCID 0000-0001-5882-7308
Names of the Topic editors: Clarine van Oel Names of the reviewers: Liesbeth van Heel Journal: The Evolving Scholar DOI:10.24404/624729750bd70f0d57ec64f6 Submitted: 12 Aug 2022 Accepted: 22 August 2023 Published: 6 March 2024 Citation: Symons, A. (2022). Mitigating Hospital Design and Delivery Failure: A Retrospective Auto-Ethnography Study. The Evolving Scholar | ARCH22. This work is licensed under a Creative Commons Attribution BY license (CC BY). © 2022 [Anne Symons] published by TU Delft OPEN on behalf of the authors. |
|---|
Abstract: There is an urgent need for further research in hospital design and delivery to understand the integrative, nuanced, and intricate nature of healthcare project delivery and design management. Historically, each new hospital programme has developed a new delivery model that takes a different approach to the management of design. However, this approach is not sustainable. Hospitals have significant complexity, which may be impacted by role changes and procurement methods that can result in significant errors, costly delays, and a lack of ability to learn from failure. A retrospective abductive, auto-ethnographic case study approach was taken in the examination of five major hospital projects of similar size and complexity reflecting five temporal periods. The examination was carried out by a project architect who subsequently became a construction design manager, spanning a career of over 30 years. This variant of action research involved a retrospective mode of abductive reasoning. An approach to hypothesis testing (using literature) is used to explain and theoretically frame historical practices. It was found that National delivery models (and their change over time) have had a significant influence on hospital project delivery , particularly on design and engineering systems integration. The role standards have played in design has also played a significant role, and, in part, may have constrained innovation and unduly increased cost. Recommendations are made for a new integrated healthcare delivery model that supports an approach to innovative design and construction of new hospitals responding to advanced clinical and technological approaches.
Keywords: Retrospective, autoethnography, integrated design and delivery
1. Introduction
The concept of integration in the design and construction of major hospitals in the UK is not new, but it has now been nearly 30 years since the last fully developed system of ‘Nucleus’ was phased out in England and Wales (Scotland adopted the standards but not the template). This rigid framework and template developed and controlled by the wider healthcare delivery system was replaced with over 50 major hospitals (throughout the UK) procured through the Private Finance Initiative and over 500 smaller schemes through the P21 and P22 Procurement Schemes. Following the setting up of individual NHS Trusts and allowing freedom of choice for patients, the former prescriptive briefs were abandoned and trusts were able to set their own project briefs. These briefs could be in the form of schedules of accommodation, or they could be written in terms of output specifications, where the designers, with the aid of healthcare planners, could prepare their own schedules. This latter method was seen as an opportunity for creating innovation. At the same time, the rigid template had outlived its ability to accommodate new models of care and advances in technology.
Not only did the wider delivery system change its approach to hospital design, but it also changed the methods of procurement, introducing contractor led design and build with the aim of achieving cost certainty with what was considered a more ‘integrated approach’ only a single contract between client and contractor. Now, after 30 years, this model is again under review.
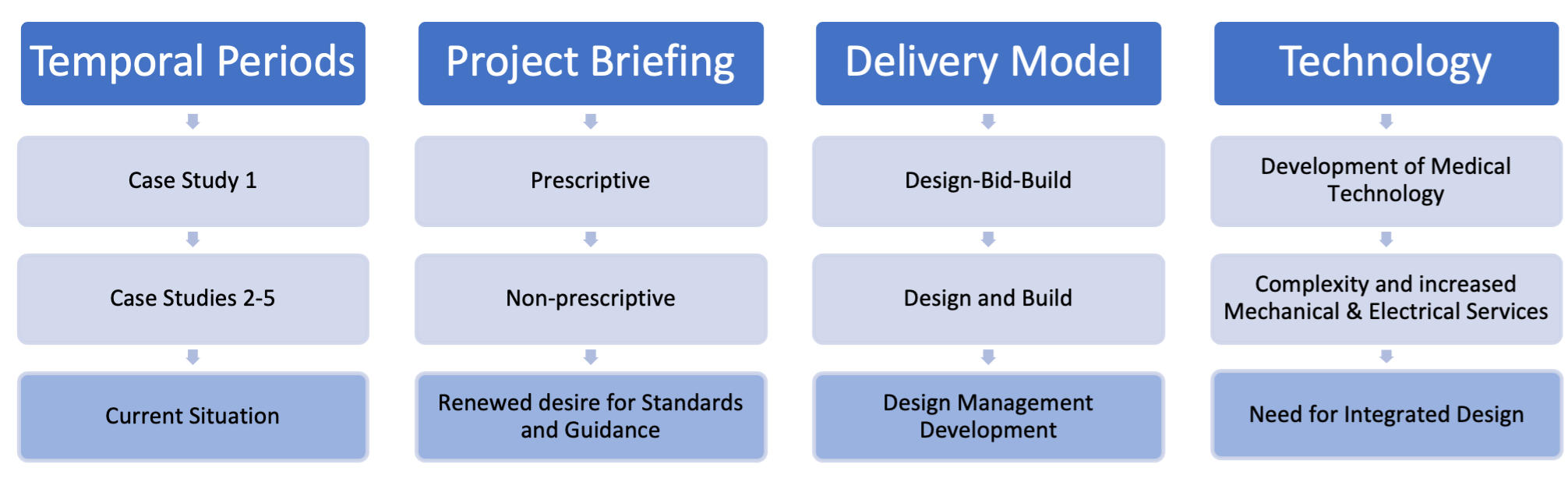
This paper looks at five major hospital projects, four of them having been completed and the fifth under construction, to ascertain the level of integration achieved and how design management has developed within both the wider delivery and project delivery systems. All of the case studies deliver secondary and tertiary care, acute facilities such as emergency departments, and are associated with university medical and nursing education. Design management is researched as to how it can integrate the diverse activities that contribute to the design and construction of these hospitals. Figure 1 sets out the developments and relationships over the five temporal periods.
Figure 1. Development through Temporal Periods
2. Theories and Methods
2.1 Design Management
There are different definitions of design management in terms of when it occurs during the project cycle and the roles and responsibilities involved. Enyon (2013) defines design management in three project stages:
Pre-project: defined as ‘Project Definition’;
Project: defined as ‘Project Procurement’ and ‘Project Delivery’; and
Post-project: defined as ‘Project Operation’.
The design management roles are defined according to the project stages as:
Strategic Front-End Design Manager during the pre-project phase;
Preconstruction Design Manager during procurement;
Delivery Design Manager (site based) during project delivery; and
Strategic Back-End Design Manager post project/ project operation.
Although these stages correspond roughly with the RIBA Plans of Works (1964, 1976, 2007, 2013, and 2020), the descriptions align with design and build procurement rather than the traditional route of the RIBA – design-bid-build. In identifying the different design management roles, Enyon (2013) suggests that strategic design managers could possibly be consultants to the client and that the preconstruction design manager could be either a member of the construction company or the lead designer, with the delivery design manager being a member of the site team. Hillebrandt (1984) recognised that in many large construction firms, the role of project manageror project director is carried out by civil engineers. While they are fully engaged on engineering projects, on building projects, once the frame has been completed their involvement ceases.
Emmitt (2007 and 2014) looks at a different role of the design manager, one that relates to design quality within the architects’ office, where “the design manager is employed to oversee (manage) all design activity within the office and ensure a consistent and coordinated approach to every project in the project portfolio’’. (p.9). The creation of this role is to allow the design architect to concentrate on creating and developing the design with the engineers by reducing unnecessary administration and the burden of office management. The role exists in many architectural offices but is given different titles; on some large projects this role is designated as ‘project manager’. In this model, the Design Manager is the link between the architectural team and the contractor’s ‘Construction Design Manager’. Emmitt develops this further in Den Otter and Emmitt (2007), Emmitt (2010, 2011 and 2016), and Emmitt and Ruikar (2013).
2.2 Integrated Design and Open Building Theory
Integrated design, as developed by Louis Khan, Giurgola and Mehta (1976), was seen as a turning point in defining the separate engineering systems and demonstrating how they needed to be integrated. In 1971, Sir Alex Gordon, RIBA President, coined the phrase ‘Long life, loose fit, low energy’. Brand (1994) looked at the stages in a building’s lifespan, and Habraken (2000 and 2008) introduced ‘Open Building Concept’, all of which led towards a structured or systems approach to design. Jones (2008) identifies an important factor in healthcare construction as the ability of the infrastructure to support the use of support technology. He recognises that changes are likely to be required during the building programme and suggests:
Building unfinished or shelled space in strategic locations or entire floors in a building tower to provide room for expansion in service areas where growth is expected;
Designing and building acuity-adaptable patient rooms that are easily converted from standard medical/surgical rooms to critical-care rooms; and
Building additional capacity into the system infrastructure.
The open building concept is developed by Kendall (2007), who concludes there is little systematic research carried out and lessons learned, resulting in comments such as “we should design column-free spaces, make floor to floor heights greater, and don’t bury pipes in concrete”. These are comments that we still hear today. Kendall and Ando (2011)and Kendall (2015 and 2019) conclude that open building outlines systems separation where the different levels of construction and fit-out can allow for flexibility and future proofing, describing healthcare architecture as infrastructure. Astley et al (2015), Olsson and Hansen (2010), and Hansen and Olsson (2011) continue with the theme of flexibility, linking it with lean thinking and a layered approach. They highlight the difference between the design stages and construction in terms of lean thinking and how, by adopting a layered approach, this not only aids flexibility but can embrace lean thinking into the design. Hansen and Olsson (2011) describe the three levels as:
The Primary System: Fixed: building frame designed to last 100 years, which can accommodate different hospital departments;
The Secondary System: Adaptable: internal fit-out in terms of partitions, services designed to function for a maximum of 20 years; and
The Tertiary System: Flexible: room focused, fixtures and fittings and interior design with a useful life of 5-10 years.
The Netherlands Board for Healthcare Institutions (2007) Layers Approach to Building separates the building functions into four categories:
Hot Floor: high-tech, capital-intensive functions specific to hospitals;
Hotel Accommodation: patient accommodation, nursing care;
Office: outpatient consultation, offices, staff accommodation, management activities; and
Industry: all medical supporting and facilitating functions.
Caixeta and Fabricio (2012), who focus on reconfiguration of healthcare projects, and Mills et al. (2015) demonstrate the difficulties in trying to apply standardisation in contrast to Montgomery (2007), who defended the Nucleus capability to be flexible. Fawcett (2011), referring to the “Duffle Coat Theory” Llewelyn-Davies Weeks et al. (1973) conclude there is no evidence that confirms that modular room sizes lead to flexibility and activity-space tolerance.
2.3 Delivery Models and Systems Integration
Cacciatori and Jacobides (2005) describe the recent changes in the British Construction Industry as going from vertical specialisation to vertical reintegration. This is due to the introduction of the Private Finance Initiative with the use of design and build contracts and the perception of a single systems integrator, as described by Smyth and Edkins (2006), Barlow and Koberle-Gaiser (2008). Several papers are also written about major and complex projects, including Davies et al. (2009), Davies and Mackenzie (2014), and Davies and Brady (2016). The focus is on infrastructure rather than healthcare projects, which have a much higher percentage of mechanical and electrical services. By contract, Lightig (2005), Chambers (2010), Lostuvali et al. (2014), and Mesa et al (2016) concentrate on the delivery of healthcare projects using Integrated Project Delivery (IPD) using the American Institute of Architects (AIA) form of contract (2007), where the architect, contractor, and client adopt a tripartite agreement. Jorgensen and Emmitt (2008) also discuss lean construction.
2.4 Methodology
The research methodology used was retrospective autoethnography for case studies one to four and a form of action research for case study five. Autoethnography is a research method that uses personal experience to describe and interpret cultural texts, experiences, beliefs, and practices (Adams et al., 2017). Anderson (2006), in response to Hayano (1979), addresses some of the paradigmatic problems associated with group relationships, the role of the researcher, and their level of subject matter knowledge and issues of subjectivity by setting out five key features in what he describes as “Analytical Autoethnography”.
Complete member researcher
Analytical reflexivity
Narrative visibility of the researcher’s self
Dialogue with informants beyond the self
Commitment to theoretical analysis
Giorgio (2013) looks at memory, the re-living and re-imaging of what happened, in a form of storytelling using a short story method, something that I have adopted in my “ramblings”. She defines autoethnography as, question “How do you begin to write autoethnography?”, to which she replies, “By closing your eyes and remembering”. Jarzabkowski et al. (2014) examine various techniques for presenting ethnographic evidence, with particular reference to vignettes built up through rich storytelling.
This variant of action research involved a retrospective mode of abductive reasoning. It occurred in the context of ontological, conceptual, and theoretical assumptions, where the researcher does not start with a blank slate. But rather, it involves abductive reasoning applied retrospectively making a hypothesis (from literature) that appears to explain what has been observed (in practice); it is observing some phenomenon and then iteratively claiming what it was that gave rise to it (based on literature and theoretical framing). Auto-interviewing was used as a technique for recording one’s own views, as defined by Boufoy-Bastick (2004), used in conjunction with autoethnography. It was used to extract and recall retrospective case study data. The process involves creating a narrative of the project history and then identifying critical incidents and significant developments. It allowed for the analysis of critical incidents that show implemented changes in action that are later evaluated for their impact (Greenwood & Levin, 2007; Susman & Evered, 1978).
2.5 Study Methods
The study method analysed five case studies,Yin (2014) creating data from narratives or ‘ramblings’, the term used to set down my recollections of the projects. They were narratives from which data could be collected. For each of these narratives, critical incidents (events that required immediate action to prevent serious consequences for the project (Flanagan, 1954)) and instances of positive integration were identified. As critical implies a serious or negative bias, the use of positive integration enabled a more balanced approach for ‘lessons learnt’, as if something works well, it is not recorded for future adoption. These incidents were tabulated using temporal bracketing (Langley, 1999) in five project stages:
Pre-Design
Concept Design
Design Development
Works Package Design
Design in Construction
A different form of analysis was developed for Case Study 5 based on Ferrance’s (2000) six-stage action research model for use in education adapted for construction. As part of the ‘rescue plan’, the existing design had to be validated and a due diligence exercise carried out before construction work could recommence with a new design and build contractor. The six stages therefore reflect the stages carried out in Case Study 5, as in Table 1, where the data is interpreted differently rather than additional data collected.
Table 1: Ferrance's Model Adapted for Case Study 5
| Stage | Design | Construction |
|---|---|---|
| Identify | Areas of design requiring validation | Compliance of construction works |
| Gather Data | Desk top design study | Survey existing construction works |
| Interpret Data | Due diligence exercise | Analyse survey results |
| Act on Evidence | Make proposals to the Client | Estimate time and cost to rectify |
| Evaluate Results | Agreement on how to proceed | Agree time and cost |
| Next Steps | Proceed with validated design | Recommence construction |
These critical incidents and positive integration instances were then tabulated according to type, e.g., mechanical and electrical services, who caused them, who resolved them, and whether they recurred. These findings were then reviewed with literature and grey literature (post occupancy studies, mini case studies, and a revue of the Nucleus Hospital System).
The five case studies resulted in five temporal periods, which I defined as shown in Table 2 below.
Table 2: Temporal Periods
| Temporal Period | Reference | National Delivery Model | |
| Prescriptive Integration | 1975-1993 | Case Study 1 | Nucleus/Design-Bid-Build |
| Dysfunctional Integration | 1993-2001 | Case Study 2 | First Wave PFI/Design and Build |
Adaptive Integration 1 |
2001-2006 | Case Study 3 | Second Wave PFI/Design and Build |
Adaptive Integration 2 |
2007-2012 | Case Study 4 | Third Wave PFI/Design and Build |
| Disintegration | 2013-2020 | Case Study 5 | PF2 / Design and Build |
3. Results
The key findings from the study are set out in terms of issues relating to the temporal periods and a summary of the critical incidents.
3. 1. Temporal Periods
The outcomes are set out in Table 3
Table 3: Outcomes from Temporal Periods
| Temporal Period | Positives | Negatives |
|---|---|---|
| 1. | Understanding roles and responsibilities Underpinning of professional qualifications Support from central government Standards and guidance |
Rigidity of the Nucleus Template Lack of stakeholder engagement Designers did not need to understand user requirements (England and Wales) |
| 2. | Enablement of major hospital schemes (PFI) Trusts are able to prepare their own briefs Contractors are able to introduce innovation (construction techniques) |
Architects lacked knowledge of healthcare design (England and Wales) Steep learning curve for contractors Quality control transferred to the contractor Move from professionalism to commercialism |
| 3. | Contractors recognise the need for design management | Department of Health began to reduce investment and support for standards and guidance. Architects losing skills in client engagement and construction detailing due to lack of site inspection |
| 4. | Trusts begin to realise the importance of standards and guidance in formulating the Trust Core Requirements (TCRs) | Further reduction in healthcare research |
| 5. | Department of Health ceases to update standards and guidance Failures start to appear: 1. Wall collapse at Edinburgh Schools PFI 2. Fire at Grenfell Tower 3. Collapse of Carillion during two major hospital PFIs |
3.2. Critical Incidents:
The analysis of the critical incidents highlighted a number of re-occurring themes relating to:
The integration of mechanical and electrical services, with a particular problem relating to coordinated ceiling layouts
The integration of the structure
The integration of major medical equipment and new developments in hospital infrastructure, such as pneumatic tube systems
The interpretation of roles and responsibilities of individuals and how they reacted
The use of a structured approach to design and project compliance checking
Table 4 outlines the critical incidents for Case Studies 1-4.
Table 4: Critical Incidents in Case Studies
| Activities | Issues | Case Studies | |||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | ||
| Client Engagement | Briefing | 0 | 3 | 1 | 1 |
| Stakeholders | 2 | 2 | 3 | 3 | |
| Design Integration | Layouts | 0 | 1 | 2 | 1 |
| Structure | 0 | 2 | 2 | 4 | |
| M&E Services | 2 | 3 | 2 | 0 | |
| Ceilings | 1 | 1 | 1 | 0 | |
| Design Information | Issue to contractor | 1 | 0 | 0 | 2 |
| Quality | 0 | 0 | 0 | 1 | |
| Programming | Activities | 1 | 1 | 0 | 0 |
| Phasing | 0 | 1 | 1 | 0 | |
| Equipment | Imaging | 1 | 1 | 0 | 0 |
| Theatre Tables | 1 | 0 | 0 | 0 | |
| Medical Gas Pendants | 0 | 1 | 1 | 1 | |
| Cost | Cost Control | 1 | 0 | 1 | 0 |
| Commercial | Procurement | 0 | 2 | 0 | 2 |
| Construction Works | Buildability | 0 | 0 | 0 | 2 |
| Installation | 0 | 2 | 3 | 0 | |
| Management | SPV/Contractor | 0 | 0 | 0 | 2 |
| Totals | 10 | 20 | 17 | 19 | |
| . | |||||
Design integration in Table 4 highlights how developing an integrated approach with the mechanical and electrical engineers and subcontractors (common to case studies 2, 3 and 4) led to the elimination of critical incidents in case study 4. In contrast, the close relationship between the main contractor, the structural engineer, and the steelwork subcontractor led to reoccurring issues with wind bracing in Case Study 4.
Table 5 shows how some of the critical incidents were translated into positive integration. Of the eight examples, six originated in Case Study 2 in Dysfunctional Integration and were adopted in Case Studies 3 and 4. It took until Case Study 4 to achieve the fully coordinated ceiling layouts (Item 7) and the integrated approach for major medical equipment (Item 8), developed during Case Study 3, being fully adopted in Case Study 4.
Table 5: Translation of Critical Incidents
| Translation of Critical Incidents into Positive Integration through Lessons Learnt | ||
|---|---|---|
| 1. | Schedule of Accommodation | Standard format |
| 2. | Checking Requirements | Departmental Reviews |
| 3. | Information exchange | Electronic Data Management |
| 4. | Building Control | On site presence |
| 5. | Quality Control | Prefabricated Bathroom Pods |
| 6. | Specialist Installations | Integrated packages (Aseptic Suites) |
| 7. | Ceiling Layouts | Prepared by M&E Engineers |
| 8. | Major Medical Equipment | Integrated approach |
It was found that the national delivery models have had a significant influence on hospital project delivery and particularly systems integration by changing the method of procurement, transferring project control to individual trusts, allowing freedom of choice in relating to clinical functionality (self-derogation), and failing to maintain standards and guidance, or encouraging new research.
3.3 Summary
Results of the case study analysis can be summarised as follows:
Healthcare design is unique in its complexity; it takes time to understand and assimilate all its requirements and communicate effectively with healthcare professionals.
The wider system needs to support a framework of standards and guidance that keeps pace with innovation, new technology, and models of care.
Design integration as design concept starts with integration of the structure and engineering services, which has the potential to develop into a layering system to deliver healthcare design.
Design management is integral to all stages of the design process and involves several skill sets.
When critical incidents arose, someone with a design background was required to solve them regardless of role or responsibility, suggesting that a systems integrator should be part of the design management team.
The importance of teamwork and continuity of major players across the stages.
Ensuring that the right people are involved at the right time and recognising individuals’ skills and experiences.
The difference in team structures are visualised in Figure 2: from a design led team as in Case 1 to the contractor led team in Case Studies 2-5 separates the designers from the specialist subcontractors at an earlier stage and, without strong design management, fails to produce an integrated design as demonstrated in Case Study 5.
| Case Study 1 | Case Studies 2-5 |
|---|
Figure 2: Team Structures
4. Discussion
The findings from the case studies and literature review suggest that there is a need for design integration in both the wider delivery system to inform project delivery and within the project delivery system to create an integrated design management structure with defined roles and responsibilities that reflect the required capabilities.
The transfer from design,build to design and build in a short period of time failed to allow time for the development of design management and contract administration within the construction companies,which resulted in people being allocated roles in design management rather than being trained for the new roles or recruited from design disciplines, as demonstrated in the case studies. Design roles were created within construction companies at the preconstruction level but then transferred to site design management roles with the loss of continuity. Without a detailed transfer of project history, knowledge is lost, and a weak link is created. The preconstruction team, knowing that their involvement has ended, move on to the next project, and the site team is too busy planning the construction to make a detailed study of the project background. Similarly, at the end of the construction work, the site team is anxious to move on to the next project and fails to carry out project closure meetings related to ‘lessons learnt’. The common link amongst these issues concerns design management and its ability to integrate with the different forms of contracts, where roles and responsibilities change according to the type adopted. The role of design manager varies considerably through the case studies, ranging from Senior Project Managers with backgrounds in civil engineering to junior engineers being assigned as design coordinators who actually carry out design information management and then develop into design managers as a means of promotional status to my role as a Senior Design Manager .Whereas I was able to introduce design management skills that I had developed through my role as a Project /Site Architect and Supervising Officer in Case Study 1, the lack of design training and client engagement skills limits their ability to deliver integrated design management.
The transfer of risk from the client to the contractor, which is appealing to clients, is no longer seen as such by contractors due to the complexity, the requirement of specialist knowledge, and the lack of up-to-date standards and guidance. Understanding the integration of the mechanical and electrical design, with the structure in the spatial design before splitting into work packages, is essential. Case Study 5 demonstrates this lack of coordination: many of the standard room types are derogated; ‘shelled space’ has been built into the design, but once the building has been occupied, these areas are very difficult to access.
In relation to the individual case studies, the outcomes of Case Study 4 in Temporal Period 4 reflected a good example of lessons learnt relating to the importance of continuity and the concept of alliancing, resulting from many of the same team members being involved in both Case Study 3 and Case Study 4.
5. Conclusions
I have tried to defend why the design and construction of major hospitals is different from infrastructure projects and requires independent research by taking the view of Symons et al. (2016) that the structural and engineering services provide the infrastructure to support the hospital.
This longitudinal study has spanned a period of over 40 years and five temporal periods. It has demonstrated the cyclical nature of the construction industry and the fact that despite proposed reforms suggested by Latham (1994) and Egan (1998), there are major issues, particularly in relation to the building of major hospitals, including the collapse of a major contractor in Temporal Period 5, marking the demise of PFI. It signals the need for a review or ‘deep dive’. It should not, however, replicate the situation at the end of Temporal Period 1, where both the wider delivery model and the form of contract were abandoned without analysis.
In relation to the wider delivery system, the need for greater direction and control by the Department of Health is apparent, as is the need for investment in research and development. Rather than creating a standard hospital, which will result in derogations, the softer approach taken in Scotland during the nucleus era, adopted standards and guidance without a rigid footprint, allowing greater flexibility. The failure to maintain standards and guidance is only partly to blame for the current situation. A form of contract that separates the designers from the client is also partially responsible.
Architectural projects involve both design and construction, but they are not like the car industry, where the prototype is designed and tested before going into mass production. The car designer is also an employee of the car company, unlike in construction, where design and construction are not integrated within one company. Effective integrated design management between the design team and the construction company can bridge this gap. Case Study 2 represented a huge learning curve for contractors trying to manage the design process.
The current design and build contracts have not proved any more successful than design, bid build in terms of design integration and have not reduced the acronymity between designers and contractors.
Consideration should be given to exploring different forms of contract, such as Integrated Project Delivery (IPD) (Figure 3), which has been successfully used in America on major hospital projects where the client, architect, and contractor are in a tripartite contract and share risk. This is also a leaner contract (AIA 2007), reducing the need for duplicate design teams.
|
|---|
Figure 3. Perceived Benefits from IPD
This study also confirms the value of using ethnographic and autoethnographic research in construction, particularly in relation to design management, an area previously not researched using these methods and not as a longitudinal study. It provides an opportunity for further research in relation to lessons learnt and knowledge transfer.
References
Adams, T.E., Ellis, C. and Holman Jones, S. (2017) Autoethnography, The International Encyclopaedia of Communication Research Methods, 2017 John Wiley & Sons
ADB (Activity s Data Base) Department of Health, computer programme related to HBNs and HTMs
AIA (2007) Integrated Project Delivery: A Guide, Version 1, The American Institute of Architects/ AIA California Council
Anderson, L. (2006) Analytical Autoethnography, Volume 35, Number 4 2006, 373-395
Astley, P.D., Symons, A.W. and Mills, G.R.W. (2015a) Rates of Change – Design Evaluation of Rapid Clinical and Technological Advances in a Children’s Surgical Unit, ETH Zurich
Barlow, J. and Koberle-Gaiser, M. (2008), the private finance initiative, project form and design innovation: the UK’s Hospitals programme, Research Policy 37 (2008) 1392-1402
Boufoy-Bastic, B., (2004) Auto-interviewing, Auto-ethnography and Critical Incident Methodology for Eliciting a Self-conceptualised Worldview, Forum: Qualitative Social Research, Volume 5, No. 1 Art 37 January 2004
Brady, T., Davies A. and Gann D.M (2005) Creating value by delivering integrated solutions, International Journal of Project Management, 23 (2005) 360-365
Brand, S. 1994, How Buildings Learn: What happens after they're Built, Penguin, New York.
Cacciatori, E and Jacobides, M.G. (2005) The Dynamic Limits of Specialisation: Vertical Integration Reconsidered. Sage Publications Organisation Studies 26(12): 1851-1883
Caixeta, M.C.B.F. and Fabricio, M.M. (2012) A conceptual model for the design process of interventions in healthcare buildings: a method to improve design, Architectural Engineering and Design Management, 2013 Vol 9, No. 2 95-109
Chambers, D., The Sutter Health Prototype Initiative, (2010) Improving Healthcare through Built Environment Infrastructure, Practitioner Contributions, Chapter 7, p.102-108, Oxford, UK: Wiley‐Blackwell
Davies A., Gann D.M and Douglas, T. (2009) Innovation in Megaprojects: Systems Integration at London Heathrow Terminal 5, California Management Review, Vol 51 No. 2. Winter 2009
Davies A. and Brady T. (2016) Explicating the dynamics of project capabilities, International Journal of Project Management, 34 (2016) 314-327
Davies, A and Mackenzie, I. (2014) Project complexity and systems integration: Constructing the London 2012 Olympics and Paralympics Games, International Journal of Project Management, 32 (2014) 773-790
Den Otter, A and Emmitt, S (2007) ‘Exploring effectiveness of team communication: balancing synchronous and asynchronous communication in design teams’ Engineering, Construction and Architectural Management, 14(5): 408-419
Department of Health Estates Directorate (1990) Nucleus Hospitals: A briefing and planning system developed by the Department of Health
Egan, J. (1998) Egan Report (Rethinking construction)
Emmitt, S (2007 and 2014) Design Management for Architects, Wiley Blackwell
Emmitt, S (2010) Managing Interdisciplinary Projects: a primer for architecture, engineering and construction Abingdon: Spon Press
Emmitt, S. (2011) Lean Design Management, Architectural Engineering and Design Management, 2011, Volume 7, 67-69
Emmitt, S (2016) The construction design manager – a rapidly evolving innovation, Architectural Engineering and Design Management, 2016 Vol.12, No.2, 138-148
Emmitt, S. and Ruikar , K. (2013) Collaborative Design Management, Routledge 2013
Eynon, J, (2013) CIOB: The Design Manager’s Handbook
Flanagan, J.C.(1954) The Critical Incident Technique, Psychological Bulletin, VOL. 51, No. 4 JULY, 1954
Fawcett, W (2011) “The Sustainable Schedule of Hospital Spaces: Investigating the ‘duffle coat’ theory of flexibility”, published in Sustainable Environmental Design in Architecture: Impacts on Health, Eds. Stamatina, R. et al. (Springer), 56.
Ferrance, E. (2000) Action Research, LAB Northeast and Islands Regional educational Laboratory Brown University, RI, USA
Giogio, G.A. (2013) Reflections on Writing through Memory in Autoethnography Handbook of Autoethnography Chapter 20, 406-424
Giurgola, R. and Mehta, J. (1976) Louis I. Khan
Greenwood, D. J. & Levin, M. (2007) Introduction to Action Research: Social Research for Social Change, London, Sage Publications.
Habraken, N.J., (2000). The Structure of the Ordinary: Form and Control in the Built Environment. Cambridge Massachusetts: MIT Press.
Habraken, N. J. (2008) Design Flexibility, Building Research and Information, 36 (3) 290-296
Hansen, G.K. and Olsson, N.O.E (2011) Layered Project- Layered Process: Lean Thinking and Flexible Solutions, Architectural Engineering and Design Management, 2001, Volume 7, pp70-84
Hayano, D.M. (1979) Auto-Ethnography: Paradigms, Problems and Prospects, Human Organisation, Vol.38, No. 1 Spring 1979
Hillebrandt, P.M. Analysis of the British Construction Industry (1984) London, Macmillan
Jarzabkowski, K. and Bednarek, R. (2014) Producing2008persuasive findings: Demystifying ethnographic textwork in strategy and organisation research, Strategic Organisation 2014 Vol.12(4) 274-287
Jones, W. (2008). Healthcare Construction: Drivers, Challenges, and Solutions. Available from: http://www.buildings.com/article-details/articleid/6470/title/healthcare-construction-drivers-challenges-and-solutions.aspx
Jorgensen, B., and Emmitt, S., (2008) Lost in transition: the transfer of lean manufacturing to construction, Engineering, Construction and Architectural Management Vol. 15 No.4 (2008) pp 383-398
Kendall, S. (2007) Open Building: A systematic approach to designing change-ready hospitals, Healthcare Design; New York Vol.7. Iss.4. (May 2007): 26-28, 32-33
Kendall, S. (2011) Hospitals on the Time Axis: Trends in the Real World and Implications for Architectural Education, HERD Journal, Volume 4, Number 4, pp 130-142
Kendall, S. (2015) Reflections on the History and Future of the Open Building Network
Kendall, S. (2019) Healthcare Architecture as Infrastructure: Open Building in Practice, Routledge
Kendall, S. and Ando, M. (2011) “Theory and Methods in Support of Adaptable Buildings”, Architecture in the Fourth Dimension Methods and Practices for a Sustainable Building Stock, Proceedings of the Joint Conference of CIB W104 and W110 November 15 – 17.
Langley, A. (1999) Strategies for Theorizing from Process Data, The Academy of Management Review, Oct. 1999 24, 691-710
Latham, M. 1994. Constructing the team: final report: joint review of procurement and contractual arrangements in the United Kingdom Construction Industry, London HMSO
Llewelyn-Davies Weeks Forestier-Walker & Bor: Long-life Loose-fit: a Comparative Study of Change in Hospital Buildings. Privately published (1973)
Lichtig,W.A. (2005) Sutter Health: Developing a contracting model to support lean project delivery, Lean Construction Journal, Vol. 2(1) pp.105-112
Lostuvali, B.,Alves, T.C.L., and Modrich, R-U., (2014) Learning from the Cathedral Hill Hospital Project during the Design and Preconstruction Phases, International Journal of Construction Education and Research, 10 pp 160-180
Mesa, H.A., Molenaar, K.R., and Alarcon, L.F., (2016) Exploring performance of the integrated project delivery process on complex building projects, International Journal of Project Management 34 (2016) 1089-1101
Mills, G.R.W., Phiri, M., Erskine, J. and Price, A. (2015) Rethinking healthcare building design quality: an evidence based strategy (2015) Building Research and Information Vol. 43 pp. 499-515
Montgomery, R., (2007) Nucleus Hospitals: Do they have a future? MSc submission LSBU
Netherlands Board for Healthcare Institutions (2007) Building Differentiation of Hospitals - Layers Approach, Report number 611, NBHI, Utrecht, The Netherlands
Olsson, N.O.E and Hansen, G.K, Identification of Critical Factors Affecting Flexibility in Hospital Construction Projects, Health Environments Research & Design Journal, Winter 2010
RIBA Plan of Work 1964, RIBA Publications
RIBA Plan of Work 1976, RIBA Publications
RIBA Plan of Work 2007, RIBA Publications
RIBA Plan of Work 2013, RIBA Publications
RIBA Plan of Work 2020, RIBA Publications
Smyth, H. and Edkins, A. (2007) Relationship Management of PFI/PPP projects in the UK, International Journal of Project Management, 25(2007) pp. 232-240
Symons, A.W., Mills, G.R and Roberts, A., (2016) Stakeholder Integration and Its Relationship with the Requirements Crunch Point in the design of Major Hospital Projects, ID@50 Bath
Yin, E.K. (2014) Case Study Research, Design and Methods, 5th Edition Sage
Figures (1)
More details
- License: CC BY
- Review type: Open Review
- Publication type: Conference Paper
- Submission date: 12 August 2022
- Publication date: 6 March 2024
Citation
Symons, A. (2024). Mitigating Hospital Design and Delivery Failure: A Retrospective Auto-Ethnography Study. The Evolving Scholar | ARCH22. https://doi.org/10.24404/624729750bd70f0d57ec64f6
No reviews to show. Please remember to LOG IN as some reviews may be only visible to specific users.