

Overview of elbow anatomy and the role of the ulnar collateral ligament (UCL)
The ulnar collateral ligament (UCL) is a key component of the elbow joint and is the primary restraint to valgus instability. Anatomically, The UCL complex of the elbow is composed of three distinct bands: the anterior band, which assists in flexion and extension; the inferior band, which helps to secure lateral stability; and the posterior oblique band, which runs along a different plane than its counterparts and helps to direct ulnar forces during pronation and supination as well as resisting valgus stress. The anterior bundle is the strongest component of the ligamentous complex and from a functional standpoint; its primary purpose is to restrict valgus stress on the medial aspect of the elbow. The anterior bundle is also composed of two separate bands (anterior and posterior) that provide a reciprocal function with the anterior band being tight in extension, while the posterior band is tight in flexion. Attenuation or rupture of the UCL can result in valgus instability.
Exploring the diagnostic criteria for various UCL injuries
There are three main types of UCL injury: partial tear, complete tear, and avulsion fracture. Partial tears are further classified into either grade 1 or grade 2, depending on the severity of the injury. Grade 1 tears are small tears or fraying of the ligament, while grade 2 tears are more significant tears with some loss of function. Complete tears are when the ligament is completely torn, and avulsion fractures occur when a small piece of bone is pulled away from the bony attachment along with the ligament.
The diagnosis of UCL injury relies on an accurate history and physical examination. Clinicians must consider several factors when diagnosing UCL injuries, such as activity level, history of any prior injuries, and the individual’s presenting symptoms. Typically, patients with UCL injury will present with either acute or chronic onset of medial elbow pain. Symptoms of UCL injuries include pain and tenderness on the medial side of the elbow, swelling, loss of range of motion, and weakness in grip strength. Physical examination can often reveal crepitus (grating or grinding sensation) and joint line tenderness with palpation. Provocation testing can further localize the symptoms to the medial elbow. Particular attention should be given to ensuring that no other underlying condition is present when diagnosing a UCL injury. Imaging studies such as static radiographs, stress radiographs, and magnetic resonance imaging can be helpful in making the diagnosis.
Incorporating musculoskeletal ultrasound in the diagnosis of UCL injuries
The diagnosis of UCL injuries can be complex; however, MSK-US is a useful and effective, noninvasive imaging modality for evaluating the UCL of the elbow due to its simplicity and convenience. Since MSK-US is not a radiation-based technology, its use is generally safe and painless for patients. Coupled with fast results and a smaller risk of complications, MSK-US is quickly becoming the go-to imaging method for diagnosing soft tissue issues such as ligament or tendon tears in the elbow region.
MSK-US offers several benefits compared to other imaging modalities in the diagnosis of elbow injuries making it increasingly easier to identify and diagnose UCL tears and other similar pathologies. MSK-US can provide instant real-time images during an examination, allowing examiners to accurately identify and grade any tear that may have occurred due to overuse, trauma or congenital anomalies. The common imaging findings associated with these conditions can be grouped into three distinct categories of MSK-US findings: tendinopathy, discontinuity of the ligament/tendon substance, and foreign bodies such as small particles of debris.
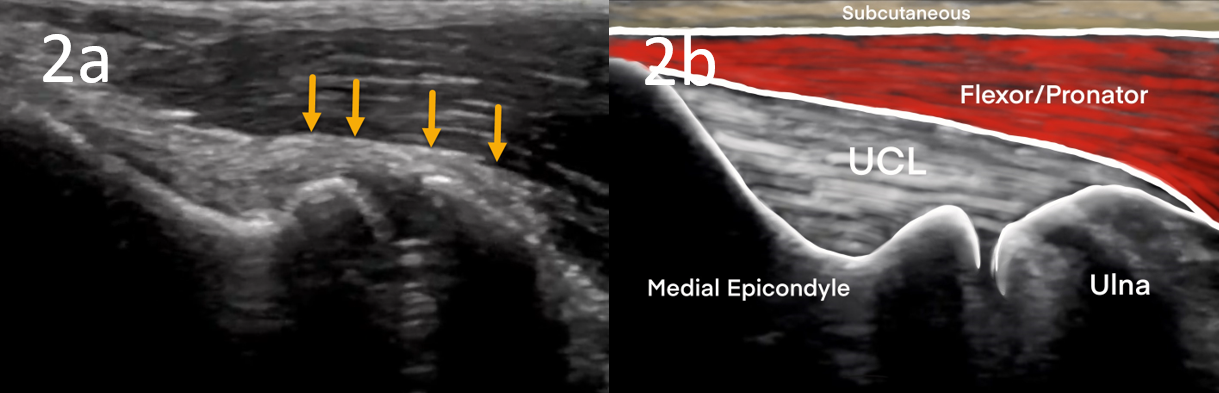
When evaluating a UCL tear with MSK-US, one may observe a widened UCL or redundant folds, irregular hyperechoic structures, clefts or gaps in the ligament coaptation line, discontinuity of continuous fibers within the UCL fibers, or pseudo fluid collections at some locations with laxity. Discontinuity appears as an apparent tear or gap between the proximal and distal ends of the tendon/ligament with intra-tendinous hyperechoic areas. A high-resolution MSK-US image can also reveal other pathologies such as tendinopathies, swelling, joint effusions, and cartilage lesions. Tendinopathy consists of irregular fibers within affected muscles or tendons and occasionally thickening around the tendon which may present with hypoechoic regions. Debris in a joint space indicates foreign bodies such as bacteria or nutrient crystals which can cause inflammation and damage to the surrounding tissue. MSK-US can help differentiate these pathologies from chronic disruptions such as UCL tears or instability events. By accurately isolating these imaging findings together with the history and physical examination, MSK-US can safely diagnose and monitor musculoskeletal disorders providing accurate guidance for treatment options.



Technical considerations for musculoskeletal ultrasound examination of the elbow
An MSK-US examination of the elbow requires several technical considerations to achieve an optimal diagnostic result. The transducer must be carefully prepared with a coupling gel and placed perpendicular to the skin surface for a clear picture of the anatomy. Higher frequency transducers do not penetrate tissue as well but provide resolution of a more superficial structure. Scanning during dynamic movement should also be incorporated when imaging the elbow, as it can provide more detailed images essential for diagnosis in a clinical setting. Additionally, optimize the patient’s position so they feel comfortable during imaging and the angle of view is maximized. Following these technical considerations will ensure an optimal MSK-US examination of the elbow.
MSK-US has become a popular modality for evaluating UCL injuries due to its advantages of being cost-effective and avoiding the need for x-rays. Not only does MSK-US offer advantages over traditional diagnostics methods like radiology, but its recent advancements have made it even more efficient and successful in evaluating UCL tears. An advantage of MSK-US is that it can be used in the outpatient setting without prior preparation, such as an injection of contrast materials. In this setting, MSK-US provides excellent imaging of the elbow anatomy which aids in the accurate diagnosis and treatment of UCL injuries. Because of its reliability, MSK-US should be considered when diagnosing possible UCL tears or other elbow pathologies.