


Abstract
Esthesioneuroblastoma is rare, with limited therapeutic options when unresectable or metastatic; however, expression of somatostatin receptors qualifies it for peptide receptor radionuclide therapy (PRRT). We report outcomes of PRRT in esthesioneuroblastoma from 2 referral centers. Methods: Using PRRT databases at 2 European Neuroendocrine Tumor Society Centers of Excellence, cases were sought between 2004 and 2018 of patients who had PRRT with recurrent or metastatic esthesioneuroblastoma deemed unsuitable for further conventional therapies. Evaluations of survival and of response using a composite reference standard were performed. Results: Of 7 patients, 4 had partial response, 2 had disease stabilization, and one had early progression. Possible side effects include worsening cerebrospinal fluid leaks. Median progression-free survival was 17 mo (range, 0–30 mo), and median overall survival was 32 mo (range, 4–53 mo). Conclusion: PRRT shows promising efficacy and moderate survival duration in unresectable locally advanced or metastatic esthesioneuroblastoma warranting larger cohort studies incorporating measures of quality of life.
Esthesioneuroblastoma, which is also known as olfactory neuroblastoma, is a rare malignancy (incidence, 0.4 per million) accounting for 3%–6% of intranasal neoplasms (1,2). The pathology of esthesioneuroblastoma is intermediate between a pure neural neoplasm, such as neuroblastoma or paraganglioma, and an epithelial tumor with neuroendocrine differentiation (3). The Hyams histologic grading system comprises 4 grades ranging from well differentiated (I) to least differentiated (IV) (4). The clinical staging system introduced by Kadish and modified by Morita (5,6) is a good predictor of outcomes (5,7,8). Stage A is confined to the nasal cavity, stage B extends to the paranasal sinuses, stage C involves further local extension, and stage D includes nodal or distant metastases. A metaanalysis by Dulguerov et al. (7) showed that Hyams pathologic grade, nodal metastases, and response to treatment were prognostic. Late recurrences can occur, with a local recurrence rate of 29%, a regional recurrence rate of 16%, and a distant metastasis rate of 17%. Ten-year survival ranges from 52% to 69% (7,8).
Standard treatment for local disease is surgery followed by radiation, with or without chemotherapy (9). Options for metastatic disease are limited, with one metaanalysis suggesting a median clinical follow-up of only 9 mo after diagnosis of distant metastatic disease for the cohort (interquartile range, 5–9 mo; range, 0.25–224 mo) and only 19 patients alive at the last follow-up. The 6-mo overall survival rate after diagnosis of distant metastases was 63% (95% confidence interval, 51%–77%), and 2-y survival for patients receiving multimodality treatment was 63% (95% confidence interval, 43%–92%) (10). A potential molecular target for esthesioneuroblastoma is overexpression of cell surface somatostatin receptors (SSRs) (11,12). Somatostatin analogs bind to SSRs with high affinity, enabling theranostic applications. PET/CT with 68Ga-labeled somatostatin analogs can be used to image the density of SSR expression at disease sites, and therapy can be performed with a companion therapeutic pharmaceutical such as 177Lu-DOTATATE for peptide receptor radionuclide therapy (PRRT) (13,14). There is high-level evidence for PRRT in unresectable gastroenteropancreatic neuroendocrine tumors (15,16), but data on rarer forms of neuroendocrine neoplasia are limited, with only very scarce data regarding esthesioneuroblastoma.
We describe the outcomes of 7 patients with recurring or metastatic esthesioneuroblastoma who received PRRT with or without radiosensitizing chemotherapy from 2 referral centers, which are now accredited within the European Neuroendocrine Tumor Society Centre-of-Excellence Network.
MATERIALS AND METHODS
We retrospectively reviewed 7 consecutive patients with esthesioneuroblastoma who received PRRT from August 2004 to November 2018. Five patients were treated at the Peter MacCallum Cancer Centre in Melbourne and 2 at Hadassah–Hebrew University Medical Center in Jerusalem. Data were collected until death or the most recent available follow-up.
Eligibility criteria were recurrent unresectable or progressive metastatic disease by imaging or symptoms despite conventional treatment, high SSR expression on SSR imaging (uptake higher than background liver activity), and adequate renal and hematologic function. PRRT was administered with renoprotective amino acid infusion as per unit protocol.
Responses were assessed at 3 mo after PRRT. Clinical response was measured subjectively by the referring physician. Imaging response was measured using a composite reference of both molecular and anatomic imaging, with the former assessed by the number and intensity of lesions (using a modified Krenning score related to tomographic rather than planar imaging) and the latter as defined by RECIST 1.1. Progression-free survival was calculated from PRRT initiation to tumor progression or death from any cause and was defined by symptomatic or imaging progression. Overall survival was defined from PRRT initiation to death from any cause. Toxicity was defined by the Common Terminology Criteria for Adverse Events, version 5.0.
All patients provided written informed consent for PRRT under compassionate-use authority. Retrospective analysis and reporting of results were granted a patient-consent waiver by the ethical committees of Peter MacCallum Cancer Centre and Hadassah–Hebrew University Medical Center.
RESULTS
Database review identified 7 patients who were treated with PRRT (4 men, 3 women; 39–77 y old). All patients had Kadish stage D disease; The Hyams grade was II in 4 patients.
Four patients had high-volume and 3 had small- to moderate-volume disease, either locally advanced or metastatic. All had prior (sometimes repeated) conventional multimodality treatment, including surgery, chemotherapy, and radiation therapy. One had a remarkable response and remained relatively asymptomatic early in the course of disease; 3 had favorable partial responses both clinically and by imaging; 2 had disease stabilization by imaging (1 patient had a marked clinical response with complete resolution of headaches); and 1 had locoregional recurrence involving the retropharyngeal region, which progressed shortly after PRRT. Details of the disease course and therapy are presented in Tables 1 and 2, and examples of multimodality scans are shown in Figures 1–4.
Demographics and Baseline Data
Peptide Receptor Radionuclide Therapy (PRRT) Details
Peptide Receptor Radionuclide Therapy (PRRT) Outcomes

Patient 1: locally extensive disease involving sinuses and orbit with brain metastases and partial response to PRRT after 3 induction cycles of 177Lu-DOTATATE. Shown are 68Ga-DOTATATE before PRRT (left) and after PRRT (right) and CT, fused, and posttherapy SPECT scans (middle, from left to right).
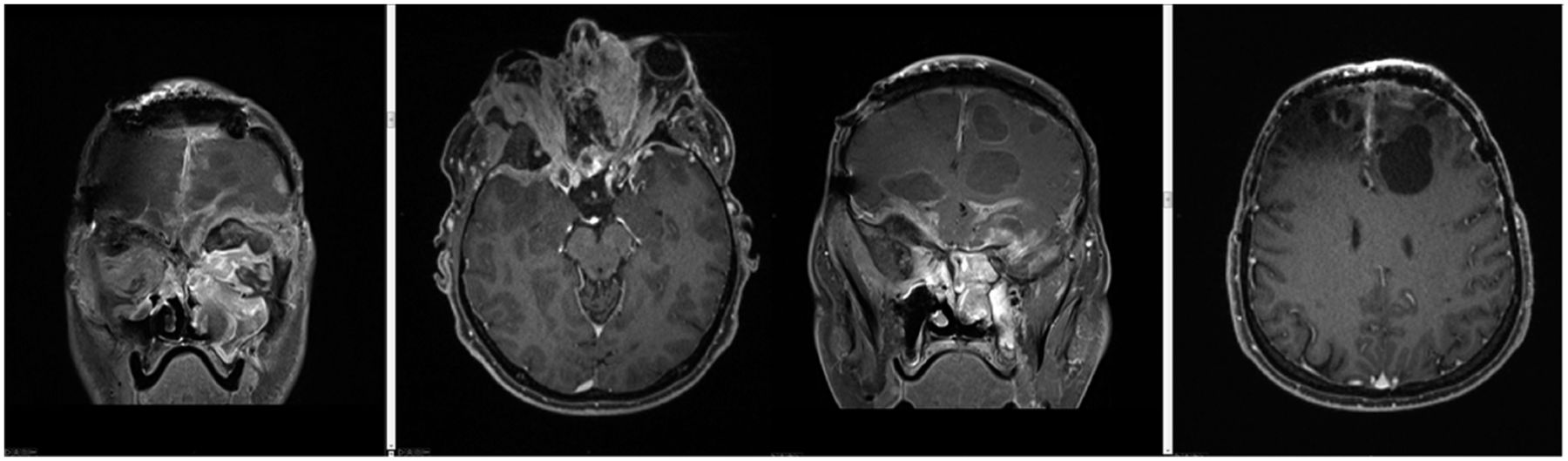
Patient 1: contrast-enhanced T1-weighted MRI sections of head, brain metastases, and local disease. Patient experienced subsequent progression with orbital, maxillary, and base-of-skull extension.
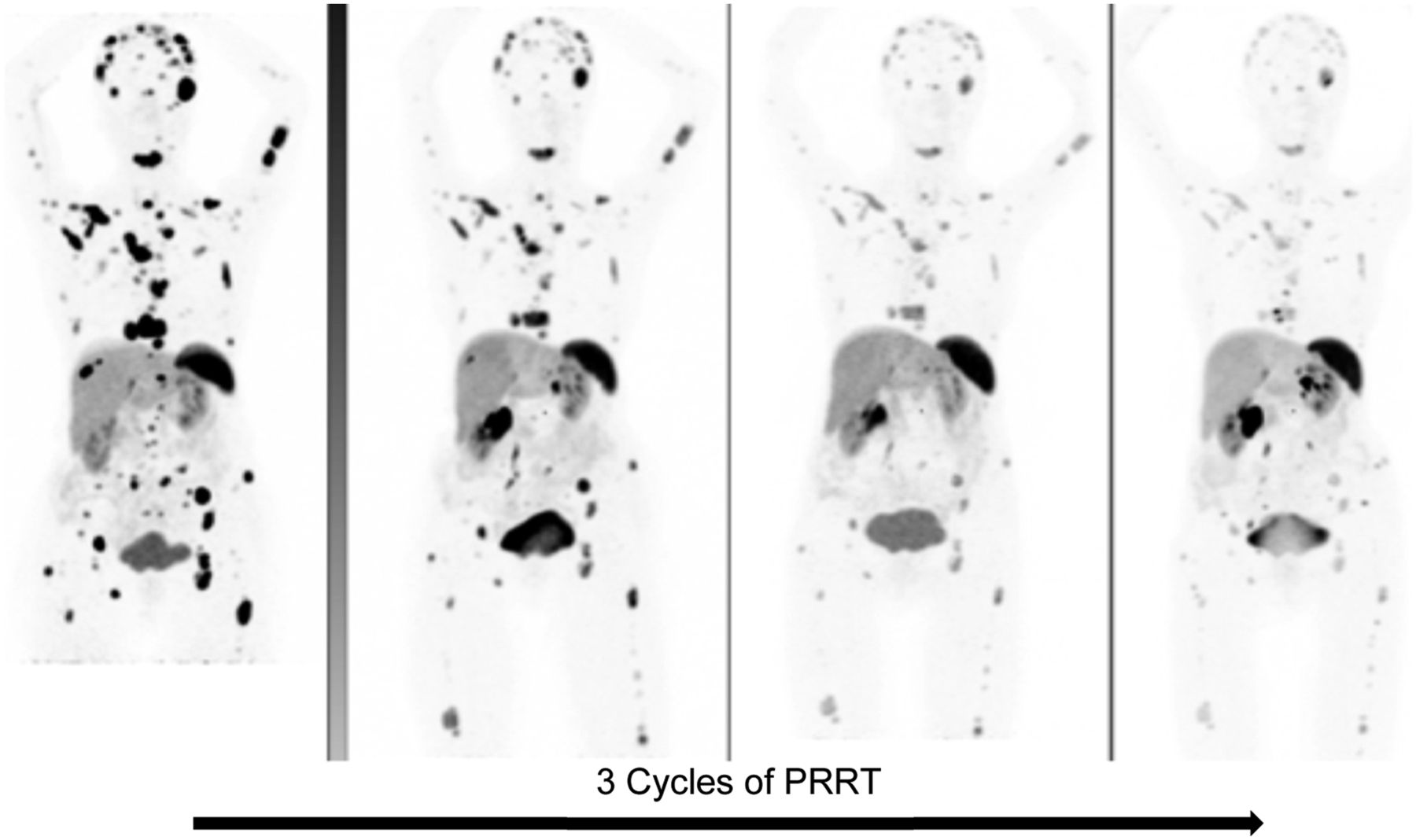
Patient 2: multiple-time-point 68Ga-DOTATATE scans showing multiple metastatic deposits involving both axial and appendicular skeleton. Patient showed remarkable response to PRRT after 3 cycles of 177Lu-DOTATATE.
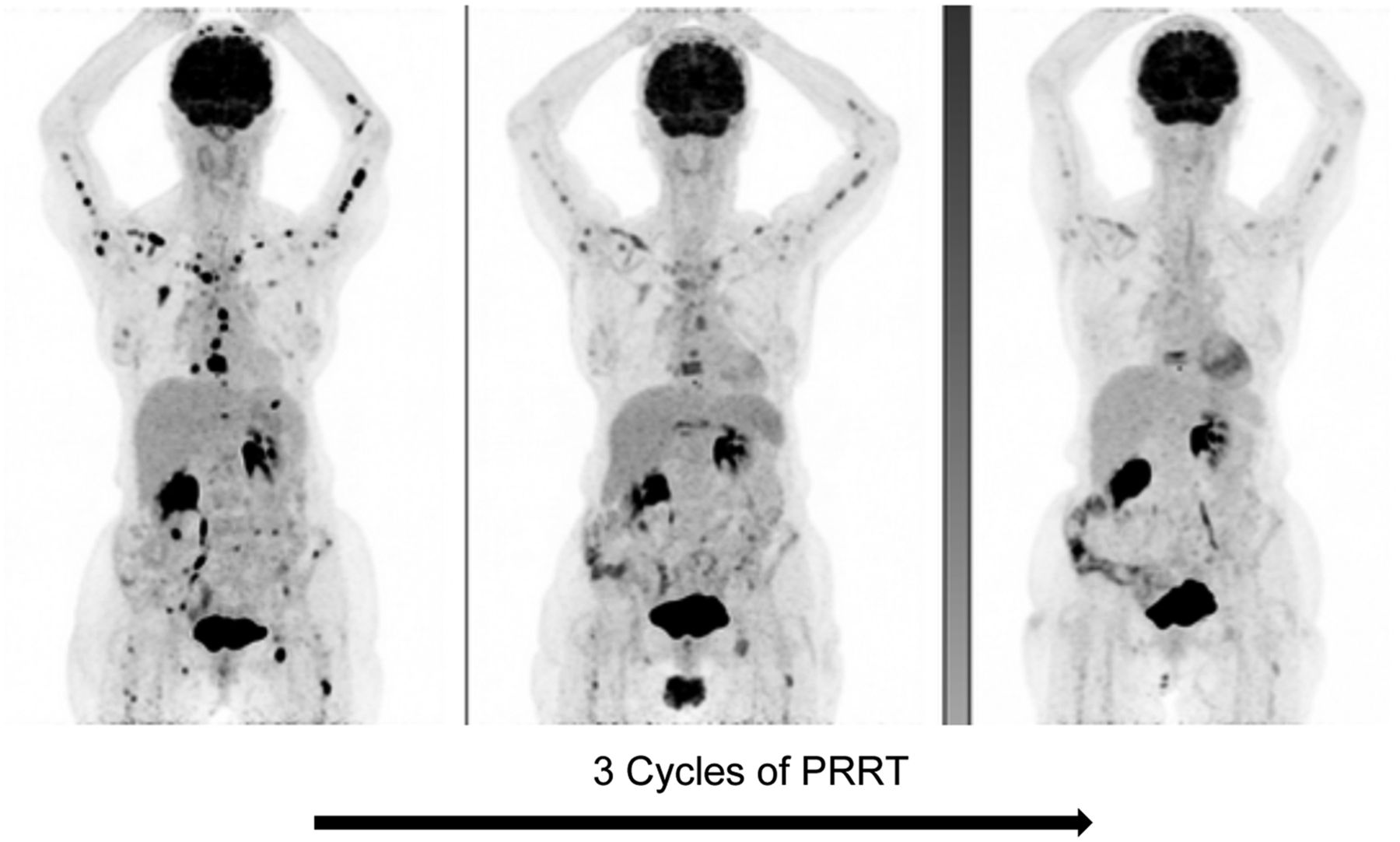
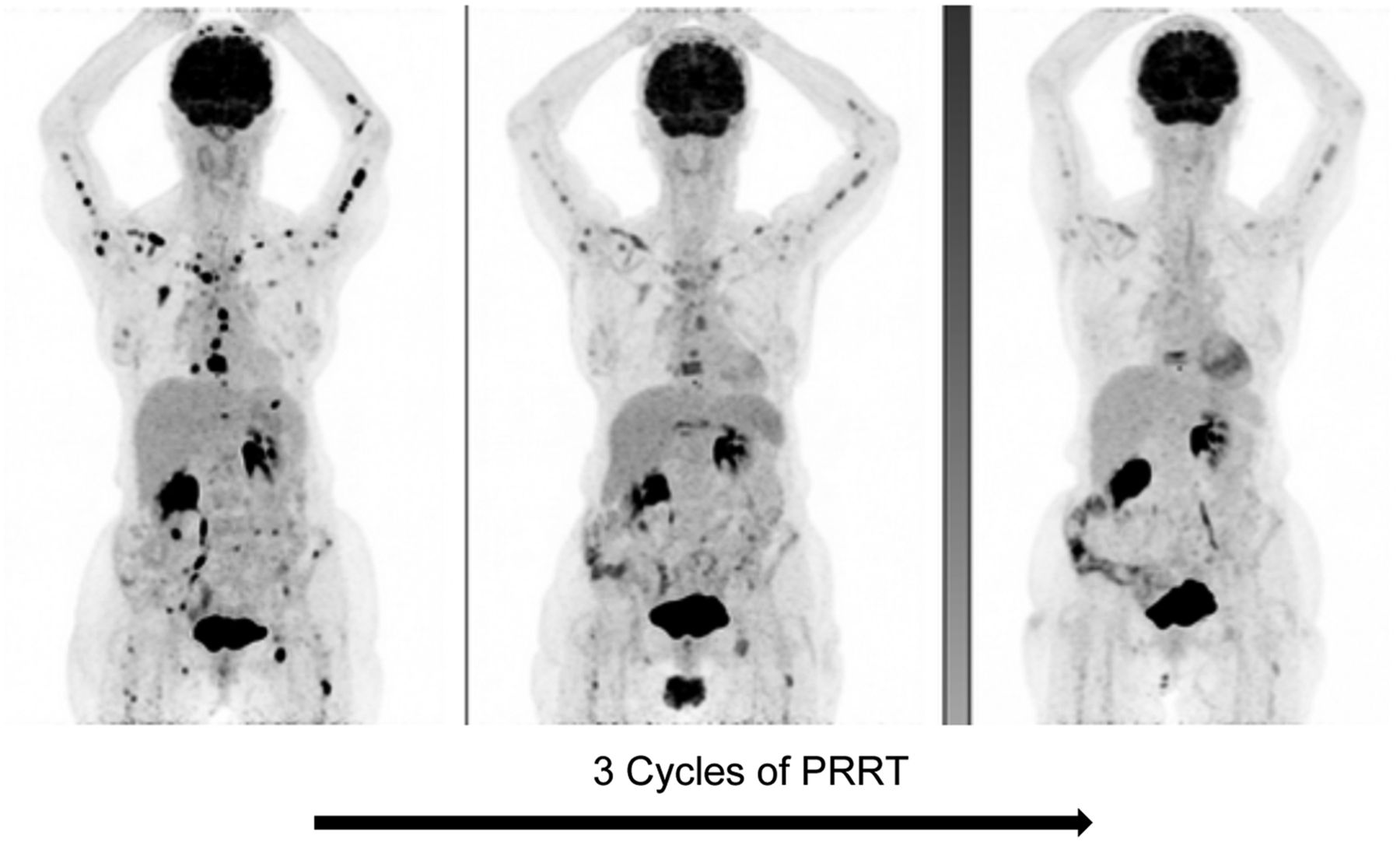
Patient 2: multiple-time-point 18F-FDG PET/CT. Patient showed concordant remarkable response to PRRT after 3 cycles of 177Lu-DOTATATE and no disease discordance.
Five patients died, 4 secondary to esthesioneuroblastoma. The median progression-free survival was 17 mo (range, 0–30 mo), and the median overall survival was 32 mo (range, 4–53 mo). Two patients are still alive at 33 and 11 mo of follow-up.
The toxicity of PRRT was generally mild but included 1 case each of transient grade 4 neutropenia (in the context of prior chemotherapy), grade 2 thrombocytopenia, and a transient grade 1–2 pancytopenia. These were likely multifactorial and related to multiple previous therapies, as the hemotoxicity of PRRT is known to usually be transient and of low grade (16). One patient developed worsening of his preexisting tumor-related cerebrospinal fluid leak, secondary to measurable shrinkage of tumor, which extended intracranially through the dura.
DISCUSSION
Treatment of unresectable recurrent or metastatic esthesioneuroblastoma remains challenging, with limited therapeutic options. High SSR expression in some of these tumors makes a theranostics approach using PRRT a therapeutic option. Outside this series, there have been only 3 single esthesioneuroblastoma cases treated with PRRT reported in the literature, with dates ranging from 2015 to 2018 (17–19). Our first patient was treated in 2008 at the Peter MacCallum Cancer Centre. Our series encompasses complicated and heterogeneous clinical presentations and disease courses. For most patients, PRRT was able to achieve favorable clinical and imaging responses despite progression after conventional therapies. Treatment was generally well tolerated, without significant toxicity.
The single patient with progressive disease in our series may have had a particularly poor outcome for several reasons. External-beam radiation therapy in our experience diminishes subsequent local PRRT response, possibly secondary to radiation-induced vasculopathy with eventual compromise to lesional blood flow or selection for radioresistant disease clones (20). This may partly explain the poor response despite high SSR expression. Additionally, patients with esthesioneuroblastoma who develop retropharyngeal nodal metastasis are known to have a poorer prognosis (18,19,21).
Esthesioneuroblastoma is a rare entity, and collecting data is challenging. Although on a very limited series, this study is, to our knowledge, the only one to report outcomes of PRRT in a consecutive cohort of patients. A further limitation is the retrospective nature of the study, with nonuniform PRRT protocols and prior therapies reflecting different institutional practices. Furthermore, variability in administered activity, number of cycles, and use of radiosensitizing chemotherapy reflecting personalized treatment regimens may limit the generalizability of results.
CONCLUSION
PRRT with radiolabeled somatostatin analogs appears to be a safe and effective option for unresectable, locally extensive, or metastatic esthesioneuroblastoma. Case selection depends on symptoms, SSR expression, disease volume, and prior intervention. In our limited series, PRRT improved symptoms and provided promising disease control and encouraging survival duration. Further prospective studies incorporating formal quality-of-life assessments and standardized response assessment are warranted.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is PRRT effective for unresectable metastatic esthesioneuroblastoma?
PERTINENT FINDINGS: This study was a retrospective case-series review. PRRT shows promising efficacy and moderate survival duration in unresectable locally advanced or metastatic esthesioneuroblastoma, warranting larger cohort studies incorporating measures of quality of life.
IMPLICATIONS FOR PATIENT CARE: PRRT shows potential for use in the treatment of esthesioneuroblastoma patients.
Footnotes
Published online Jan. 31, 2020.
- © 2020 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication November 13, 2019.
- Accepted for publication January 10, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.