AUCTORES
Globalize your Research

Review Article | DOI: https://doi.org/10.31579/2578-8965/036
*Corresponding Author: Victor Manuel Vargas Hernandez, Gynecology Service, Hospital Juárez de México, SS, Women's Health Clinic, Insurgentes Sur 605-1403, Naples, CDMX 03810 Mexico: E- Mail: vvargashernandez@yahoo.com.mx
Citation: Victor Manuel V H, Victor Manuel V A. (2020) Clinical, Pathological, Preventive and Therapeutic Aspects in Cancer De Vulva. Obstetrics Genecology and Reproductive Sciences, 4(1): DOI: 10.31579/2578-8965/036
Copyright: © 2020. Victor Manuel Vargas Hernandez. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 11 January 2020 | Accepted: 20 January 2020 | Published: 23 January 2020
Keywords: vulvar cáncer; rare tumors, diagnosis; pathology; imaging, treatment; surgery, chemotherapy; radiotherapy
Vulvar cancer is rare, occupies the fourth most common type of gynecological cancer mainly affects postmenopausal, there are no screening tests or effective strategies to reduce its incidence, only the timely treatment of preneoplastic lesions; It is initially asymptomatic, chronic pruritus or vulvar pain is reported, or the presence of tumor or ulcer; alone, the biopsy confirms the diagnosis and histopathological type. Surgical staging involves the removal of the primary lesion and locoregional lymph node evaluation. In current practice, surgical management is conservatively substituted for radical vulvectomy and depends mainly on the histopathological type and staging, mainly the nodal state. Conclusion: The treatment of malignant neoplasms of the vulva, in general, surgery is the primary treatment.
Vulvar cancer is rare and accounts for only 2 to 5% of gynecological malignancies. Squamous cell carcinoma (SCC) of the vulva, is the most common subtype, is traditionally a disease of postmenopausal women, although the average age of incidence has decreased in recent years due to the increase in human papillomavirus infections (HPV) worldwide [1, 13]; This epidemiological change makes differences in its current incidence or age of presentation between countries and regions; it can be explained by a different local prevalence of HPV or other risk factors (FR); for example, ethnic distribution, smoking, atrophy and inflammation or infection by human immunodeficiency virus (HIV) [1,19].
The age-adjusted incidence of vulvar cancer in the United States was 2.5 per 100,000 women. Vulvar carcinoma is most often found in postmenopausal women. The average age at diagnosis is 65 years, but it is decreasing to 55 years 1-13. Risk factors for vulvar cancer include smoking, vulvar dermatosis (for example, lichen sclerosus lichen or cervical intraepithelial neoplasia (CIN), human papillomavirus (HPV), immunodeficiency syndromes, history of cervical cancer Vulvar carcinogenesis is currently divided into two types: the first related to HPV infection of the mucosa and the second related to chronic vulvar dermatoses or autoimmune processes. HPV has been shown to be responsible of 60% of vulvar cancer; mainly HPV-16 and 33 representing 55.5% percent of all HPV-related vulvar cancers.The rising incidence of intraepithelial vulvar neoplasia (VIN) related to HPV in young women makes that the average age of diagnosis of vulvar cancer decreases. HPV DNA is common in vulvar cancers of women of late reproductive age with smoking habits, which in postmenopausal women without smoking [1, 13].
The external genitals comprise the vulva and pubis or pubic area. The vulva is found in the anterior triangle of the perineum. Elements that make up the vulva include minor and major lips, clitoris, vaginal vestibule bulb and minor vestibular glands (Skene glands) and major (Bartholin glands) [18]. Most malignant tumors are associated with the skin of the lips. Malignant tumors that arise from the clitoris and vestibular glands are extremely rare. The lymphatic drainage of the vulva is mainly to the inguino-femoral region, and secondarily to the external and internal iliac region. This drain is shared with the lower third of the vaginal and the outermost part of the anus (under the anal sphincter). Depending on the location of the primary tumor, its size and its proximity to the midline, the lymphatic drainage can be unilateral or bilateral. In addition, if the lesion is near or over the clitoris, drainage can be directly to the iliac region [19, 21].
The clinical picture of vulvar cancer can be asymptomatic, most women have pruritus; which is common in most vulvar dermatoses; The biopsy is performed when there is a suspicion or the lesions are refractory to vulvar treatment or pain, or have noticed a mass or ulcer. Most are presented with a unifocal vulvar plaque, ulcer or mass (fleshy, nodular, or warty) on the labia majora; Minor, perineum, clitoris and mount of venus less frequently may also have abnormal bleeding or discharge, and many will have a history of vulvar dermatosis symptoms such as underlying lichen sclerosus or high-grade squamous intraepithelial lesion (HSIL) [22, 24]. Advanced vulvar cancer can occur with; vulvar bleeding or discharge, dysuria, or groin mass due to lymph node metastasis [5, 7,14] or enlarged lymph node in the groin are less frequent; Many patients are asymptomatic at the time of diagnosis. In 10%, the lesion is extensive to determine the actual site of origin. The lesions are multifocal in 5%, the entire vulva and perianal skin surfaces, as well as the cervix and vagina, should be evaluated; there is a synchronous cancer, and it is commonly the CIN in 22%.
The diagnosis of vulvar cancer is histopathological; Vulvar examination with the naked eye or with a magnifying glass is performed during a routine pelvic exam and suspicious lesions include any raised or warty or pigmented lesions. If the injury is not evident, but there is suspicion; The application of 5% acetic acid is performed vulvoscopy (or with a magnifying glass) to define the aceto-white lesions and their underlying vascular changes with abnormal vascular patterns, biopsy is taken, from the area (s) of the abnormal lesion, multiple to "map" All potential vulvar pathology sites not including areas of extensive necrosis [5, 9, 11, 13].
The biopsy is to exclude the invasion. This can be done under local anesthesia with a Keyes 3 or 4mm biopsy instrument, or with an incisional or wedge biopsy. Even if the lesion is small, it is better not to remove the entire lesion at the time of the biopsy, as this makes it difficult to plan the definitive subsequent surgery [5,7, 14]. If the diameter of the lesion is 2cm or less, and the depth of the stromal invasion is less than or equal to 1mm at the initial biopsy, it is usual to perform a wide and radical local excision of the lesion to assess the depth invasion maximum If no part of the lesion has a depth of invasion greater than 1mm, then this excision is the appropriate definitive treatment [22, 24] the examinations are as follows
1. Cytology or cervical Pap test (Pap) and colposcopy of the cervix and vagina, if applicable, due to the association of HPV-related cancers with other SILs.
2. Complete blood count, biochemical profile, liver profile and HIV tests.
3. Chest x-ray
4. Computed tomography (CT) or magnetic resonance imaging (MRI) of the pelvis or groin is useful, especially for locally advanced tumors, to detect any enlarged lymph nodes in the groin or pelvis, erosion in the underlying bone or other metastases; CT or MRI are useful in additional treatment planning.
5. Positron Emission Tomography (PET) with 18 F fluorodeoxyglucose (18 F-FDG) with CT (PET-CT) can more effectively assess and detect the involvement of the inguino-femoral lymph nodes compared to CT, which influences the planning of primary surgery and dissection of the inguinal lymph nodes to determine optimal extension surgery without sentinel node biopsy and use of frozen sections [5, 22] PET-CT is used with larger tumors when metastatic disease or recurrence is suspected [2]
It includes epidermal inclusion cysts, lentigos, Bartholin gland disorders, acrocordones, seborrheic keratoses, hydradenomas, lichen sclerosus and other dermatoses, and accumulated condyloma. If one of these disorders is initially suspected, but does not respond to proper treatment, a [1, 15] biopsy should be performed.
Prevention
Primary prevention (vaccination)
As for cervical premalignant lesions that predispose to cervical cancer, persistent HPV infection, particularly the HPV-16 genotype, has been associated with the long-term development of HSIL. And SCC of the vulva [1, 2, 23, 28]. It has been shown that the introduction of the HPV vaccine as a primary prevention strategy for cervical cancer also reduces the prevalence of non-cervical premalignant lesions among women vaccinated [12] in the long term the reduction in vulvar cancer associated with HPV in people vaccinated against and HPV [13,23, 28].
Secondary Prevention (Screening)
There is no evidence of specific screening tests for vulvar cancer. Self-examination should be encouraged in women with lichen sclerosus, injury related to the development of vulvar cancer and there should be an early evaluation of any patient with signs (for example, in pigmented lesions, irregular ulcers) or symptoms (such as Pruritus chronic vulvar) commonly associated with vulvar disease, which could be candidates for a vulvar skin biopsy [29, 31]. In women with squamous intraepithelial lesion (SIL) of the cervix, vagina or anus they should undergo vulvar inspection as part of the follow-up during the colposcopy exam.
Tertiary Prevention (Management Of Premalignant Lesions)
The effective strategy to reduce the incidence of vulvar cancer is the timely treatment of predisposing and preneoplastic lesions associated with the development of vulvar cancer; There are two main pathological pathways that lead to SCC of vulva [28, 31]:
1. Keratinizing SCC usually occurs in older women and is often associated with lichen sclerosus and / or differentiated vulvar intraepithelial neoplasia (dVIN).
2. Verrucous/basaloid SCC usually occurs in younger women; It is caused by persistent infection of high-risk HPV (HPV-ar) or oncogenic (particularly HPV-16, 18,31 and 33), and has SIL as its precursor lesion. The lesions are often multifocal and are associated with SIL in other parts of the lower genital tract (for example, cervix, vagina, anus). HIV infection and smoking are also common predisposing factors [1, 3,9].
There are two subtypes, both of which usually occur on the lips or vestibule:
Keratinizing, differentiated, or simple type is more common, occurs in elderly women, is not related to HPV infection, but is associated with vulvar dystrophies such as lichen sclerosus and, in developing countries, chronic granulomatous disease venereal.
The classic, warty, or write bowenoid is primarily associated with HPV 16, 18, and 33, and was found in young women. The risk factors associated with HPV infection are early age at the first sexual intercourse, multiple sexual partners, [HIV] infection, and cigarette smoking. These women tend to present with the disease at an early stage, although several cases of stage III/IV of the disease in HIV-infected women have been reported [5]. As shown in Table 1,
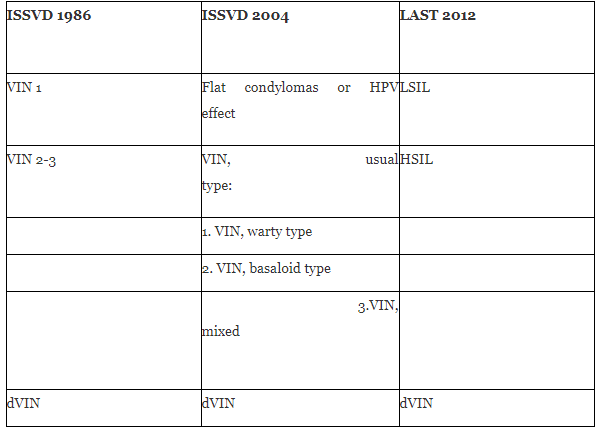
VIN (Intraepithelial vulvar neoplasia)
DVIN (Intraepithelial vulvar neoplasia, differentiated)
LSIL (Low-grade squamous intraepithelial lesion)
HSIL (High-grade squamous intraepithelial lesion)
LAST (Terminology of squamous lesions of the lower genital tract)
The terminology and definitions Premalignant lesions or precursors of vulvar cancer have changed in recent decades. Currently, such lesions that arise from the vulva and anus are included as "inferior anogenital squamous intraepithelial lesions". Under this classification, three subtypes for the vulva are distinguished: low-grade squamous intraepithelial lesions (LSIL); HSIL; and the differentiated variant. Such a distinction correlates with the risk of developing cancer over time [4, 7,30, 36].
To date, there is no definitive treatment for conditions such as lichen sclerosus. Standard measures include avoiding exposure to precipitating factors (eg, local irritant trauma, occlusive wet environment) and powerful and ultra-powerful topical corticosteroids. Alternative options include the use of topical calcineurin inhibitors (eg, tacrolimus) or retinoids and photodynamic therapy for selected cases and/or cases resistant to corticosteroid therapy. In women, surgery is limited to healing processes that lead to functional impairment [34,35]. Intraepithelial differentiated vulvar neoplasia (dVIN) represents less than 5% of preneoplastic vulvar lesions, characterized by a higher rate of progression to vulvar SSC; the shortest time interval for progression and the higher recurrence rate than HSIL. It is rarely associated with persistent HPV infection (less than 2%). Excision (with margins of 0.5–1cm) constitutes the treatment of choice, to allow adequate evaluation and exclusion of the hidden invasion [34, 39].
There are multiple treatment modalities for the management of HSIL, but simple excision with 5mm margins and 4mm depth is the most common. Excision has the advantage of excluding the invasion histopathologically, but the lack of preservation of the vulvar skin produces psychosexual morbidity, particularly in younger women. An alternative option to preserve the anatomy is the carbon dioxide laser, but it lacks the evaluation of the hidden invasion. A less destructive option is the use of 5% imiquimod to prevent scars and sexual dysfunction, particularly in smaller lesions. Moderate quality evidence shows that the response rates with imiquimod and cidofovir, another topical treatment, are similar at 6 months compared to surgical treatment or laser vaporization; There is little evidence of the effectiveness of topical treatment for HSIL among immunocompromised women [34,35]. Regardless of the treatment chosen and the margin status, there is a risk of recurrence (up to 30 to 40%). Therefore, close monitoring is recommended for at least 2 to 3 years [36].
Anatomy of the spread of the disease.
Primary site
Malignant tumors of the vulva should be confirmed histopathologically and are classified as such when the primary site of origin of the tumor is the vulva. This includes tumors that involve both the vulva and the vagina, but excludes secondary tumors of the genital and extra-genital sites [1].
Lymph nodes
The inguinal and femoral nodes are the first sites of dissemination, followed by the pelvics. Depending on the tumor size and its location (closer to the midline or clitoris), the risk of lymph node involvement may be unilateral or bilateral.
Metastatic sites
Women who have lymph node involvement pelvic or extra-pelvic dissemination are considered to have stage IV disease.
Surgical Staging
Vulvar cancer has been surgically staged since 1988 and the final diagnosis is based on histopathological evaluation of lymph node and vulvar specimens [1,2]. The staging of the International Federation of Gynecology and Obstetrics (FIGO) [37] of vulvar carcinoma was last reviewed and modified in 2009 by the FIGO Committee of Gynecological Oncology table 2. [5, 8] This system is applicable for most malignant tumors that originate in the vulva, except melanoma.
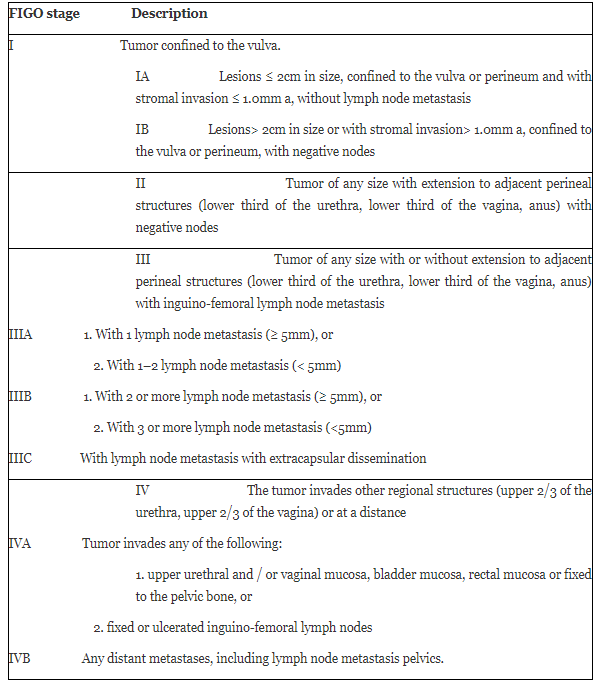
A The depth of the invasion is defined as the measurement of the tumor from the epithelial-stromal junction of the adjacent most superficial dermal papilla to the deepest point of the invasion.
SCC of the vulva represent the vast majority of vulvar cancers (more than 80%), and melanomas are the next most common cancer. The rarest histopathological types include:
1. Basal cell carcinoma
2. Verrucous carcinoma
3. Paget's disease of the vulva
4. Adenocarcinoma, not otherwise specified
5. Bartholin gland carcinoma
Histopathological degrees
1. GX: the grade cannot be evaluated
2. G1: well differentiated
3. G2: moderately differentiated
4. G3: poor or undifferentiated
Vulvar Biopsy
Stromal invasion
Local split
Simple vulvectomy
Lateral lesión
Treatment
The treatment of vulvar cancer depends mainly on histopathology and staging. Other variables that influence the treatment are age, co-existence of comorbidities and the functional status of the patient. The treatment is predominantly surgical, particularly for vulvar SCC, although concurrent Qt-Rt is an effective alternative, particularly for advanced tumors and those in which exenteration would be necessary to achieve adequate surgical margins [9]. Treatment should be individualized and performed by a multidisciplinary team in an oncology center with experience in the treatment of these tumors [2, 8,10]. Other therapies such as Qt and immunotherapies are generally reserved for metastatic or palliative settings, or for the treatment of rare histopathologies such as melanoma [2, 10,36, 40].
Carcinoma of Sculose Cells of The Vulva
Ssc Vulvar Surgical Management
Radical surgery for vulvar cancer often causes extensive soft tissue defects and, despite the tendency to poor wound healing, requires rapid postoperative recovery to allow adjuvant therapies. Reconstruction ranges from secondary healing to free tissue transfer, with pedicle flaps that are usually the first option. The main objectives of the reconstruction are the cutaneous closure without tension, with good quality tissues, the maintenance of the urethral and vaginal introite without contraction and deviation from its central position, restoration of the anovaginal partition and simultaneous closure of associated defects, such as the pubis or inguinal defects if necessary. In the presence of pelvic exenteration or abdominal-perineal resection, the pelvic support may be affected and a variable amount of devitalized space requires covering it to reduce the risk of complications. Secondary objectives include reconstruction to improve sensitivity, sexual function, aesthetics of the external shape and minimal morbidity of the donor site of the flap [41,42, 49], some drawbacks are mainly due to the size of the defect with minimal consideration for defects associated surrounding, beyond the vulvar and perineal edge. Defects of the groin, pubis, vagina or urethra are often present in gynecological surgery for vulvar cancer; this creates singular geometries of defects that must be considered three-dimensionally as a single form, in order to correctly choose the flap for reconstruction [42, 49]; There is a wide arsenal of traditional and piercing flaps. These flaps may be technically demanding but preferable in many cases, due to the longer pedicle, better mobility and decreased morbidity at the donor site. Other very important characteristics that should be considered are: possible previous radiotherapy (Rt), laxity of the inner skin of the thigh, often present if the patient is elderly without obesity, asymmetry of the defect, possibly associated abdominal-perineal resection or pelvic exenteration, with the possibility of fecal or urinary ostomies. In the presence of abdominal-perineal resection, anterior pelvectomy or pelvic exenteration, we need to fill the dead space.
In the presence of abdominal-perineal resection, anterior pelvectomy or pelvic exenteration, we need to fill the dead space. Therefore, myocutaneous flaps [5, 7, 41] The surgical treatment of vulvar cancer must be individualized, and the most conservative operation that will result in the cure of the disease must be performed [40,41]. More importantly, when considering treatment options, the most appropriate treatment for: (1) the primary lesion; and (2) the lymph nodes in the groin, should be considered independently of each other, to maximize the possibility of cure, while minimizing the morbidity related to the treatment [1, 2,10, 12, 40, 41].
Vulvar cancer is one of the less common gynecological cancers, and the role of its prognostic factors is unclear [50]. The impact of the age-adjusted Charlson comorbidity index (ACCI) on CSS, cancer-specific survival possibly associated with the highest probability of receiving suboptimal treatment in patients with multiple comorbidities, which increases the risk of disease recurrence and mortality [50], the initial evaluation of the patient, ACCI could be useful to assess the risk of mortality due to cancer and, ultimately, could be used as a tool for a more personalized and individualized management of the patient.
Vulvar Microinvasive Cancer (Stage Ia)
Stage IA vulvar carcinoma is defined as a lesion measuring 2cm or less in diameter, with an invasion depth of 1.0mm or less. The depth of the invasion is measured from the epithelial-stromal junction of the most adjacent superficial dermal papilla to the deepest point of the invasion [1]. These lesions must be treated with radical local excision and inguinal LDN is not necessary [51].
Early Vulvar Cancer
Early vulvar cancers are those confined to the vulva, and where there are no suspicious lymph nodes, either on clinical examination, or imaging; ultrasound or other [1, 15].
The gold standard of treatment for early vulvar cancers is radical local excision or tumor radical. This is as effective as a radical vulvectomy to prevent local recurrence, but substantially reduces the psychosexual morbidity of treatment [5, 7, 51,52].
The associated pre-invasive disease must also be removed to exclude other areas of invasion and to prevent new tumors that arise in the so-called "abnormal field." While the surgeon must point to surgical margins of 2cm to achieve pathological margins of at least 8mm (which allows fixed tissue contraction), it is now recognized that many "recurrent" vulvar cancers are probably new tumors that have developed in the surrounding abnormal tissue, instead of recurrences due to inadequate margins [53,54].
The deep margin of the excision should be the inferior fascia of the urogenital diaphragm and, if necessary, 1cm distal from the urethra can be removed to achieve an adequate margin, without compromising urinary continence [1,35].
Proper management of the lymph nodes in the groin is the most important factor in reducing mortality from early vulvar cancer, since recurrences in the groin are associated with a poorer survival despite using multimodal therapies as "rescue" treatments [5, 7]. The current standard involves resection of the primary tumor and lymph nodes through separate incision [2]. This approach allows for better healing compared to block resection of the vulva and inguinal. Both inguinal and femoral nodes should be removed, since inguinal node dissection alone is associated with a higher incidence of groin recurrence. While some reviews have suggested that Rt alone can control microscopic groin disease, a small randomized trial suggested that dissection of the groin, with postoperative Rt for patients with lymph node metastasis, is greater than the Rt of the groin. All women who have stage IB or stage II cancers must undergo inguinofemoral LDN; LDN is a constant and independent prognostic parameter and allows the stratification of patients in three different risk groups [51, 58].
Less than 1% of patients who have small lateral lesions (less than 4cm and ≥ 2cm of the vulvar midline) and negative ipsilateral nodes have lymph node metastasis of the contralateral groin and, therefore, an ipsilateral LDN is the appropriate treatment for these patients [8, 40, 51,53]. Patients who have closer tumors (< 2cm) or that cross the midline, especially those involving the anterior labia minora, and those women who have very large lateral tumors (> 4cm) or lymph node metastasis ipsilateral, must have a bilateral inguinal ganglion of dissection.
The procedure of sentinel node biopsy in vulvar cancer, sentinel node biopsy is being used more and more in the treatment of women with early vulvar cancer. The objective of the procedure is to detect lymph node metastasis in the sentinel node biopsy (which mainly drains the tumor) and then omit a complete LDN in patients with negative sentinel node biopsy, thus decreasing the morbidity associated with a complete LDN inguino-femoral [21,51]. The indications for a sentinel node biopsy procedure are:
1. Unifocal tumors confined to the vulva.
2. Tumors less than 4 cm in diameter.
3. Stromal invasion of more than 1 mm
4. Clinically negative groin nodes
The sentinel node biopsy are identified using radiolabeled technetium and blue dye. There were recurrences in the groin in 2.3% of patients, with a median follow-up of 35 months. The disease-specific SV was 97% after 3 years, and surgical morbidity was substantially reduced. It is noteworthy that when it is not detected in the ipsilateral sentinel node biopsy, a complete ipsilateral inguino-femoral LDN should be performed. If a ipsilateral sentinel lymph node is positive, a complete bilateral inguino-femoral LDN is recommended [2, 55, 56, 57,59]. The sentinel node biopsy in vulvar cancer are increasing over time and in older women with comorbidities they are more likely to have a groin evaluation by sentinel node biopsy; but it is not uniform in all centers and barriers to its realization must be explored. Predictive factors of prevalence and extent of N + in vulvar cancer, invasion of the lympho-vascular space, tumor stage, age and depth of infiltration are associated with the prevalence of lymph node metastasis; The stage and tumor size are associated with the number of lymph node metastasis [57, 59,60, 62]. Sentinel node biopsy
In particular, the early stage of the management of patients with inguinal lymph node metastasis [37, 51, 57] showed that when they had > 1 lymph node metastasis in inguinal LDN, they had better results with pelvic and inguinal adjuvant Rt compared to pelvic LDN. Women with lymph node metastasis who received targeted adjuvant Rt improve suvirval [56].
The prognostic importance of the number and size of inguinal lymph node metastasis, as well as the presence of extracapsular dissemination. Patients with small lymph node metastasis appear to have a good prognosis after inguino-femoral LDN alone, unless there is extracapsular dissemination, and these women do not appear to benefit from adjuvant Rt, indications for pelvic and inguinal Rt [56,61,62] in patients with lymph node metastasis they are:
1. Presence of extracapsular dissemination.
2. > 2 lymph node metastasis inguinals [40, 41]
Patients who have a positive sentinel node biopsy (> 1 lymph node metastasis, in addition to performing a complete dissection of the inguino-femoral lymph nodes, should receive Rt in the groin and pelvis, if indicated. The efficacy of groin Rt without inguino-femoral LDN for patients with only 1 ganglion in the sentinel node biopsy sentinel node biopsy of 2mm or less in diameter [40, 42, 46, 51,52].
In terms of Rt, the radiation fields during external beam Rt (EBRT) should include the inguino-femoral and external and internal iliac lymph nodes in most patients. If there are many bulky positive inguinal nodes or if pelvic lymph node metastases are suspected, the upper edge of the radiation field may extend [61,63] Sometimes, brachytherapy can be added as an impulse to anatomically susceptible primary tumors.
There are a variety of Rt techniques to choose from, depending on the size, shape of the patient's body, and extent of the disease (for example, 3D-shaped fields 7 Anterior-Posterior/Posterior-Anterior [AP/PA], Rt de modulated intensity) therapy [IMRT]). To ensure adequate tumor coverage, clinical examination, imaging findings (CT or MRI) and nodal size should be considered to adequately define the target volume during 3D planning [43, 45,51, 55,61, 63].
Combined photon and electron techniques are often used to treat regional nodes, without overdosing the femoral heads. It is important to properly include both superficial and deep inguinal lymph nodes. Underdosing of the superficial inguinal ganglia by high-energy photon beams is a risk in thin patients, and care must be taken to avoid this. Enough energy must be used to cover the femoral nodes, if electron beams are used [5, 22,43-45].
IMRT or other computer-controlled and reverse-controlled radiation management techniques are more modern methods that have been used in recent years to treat vulvar cancer. The benefits of this are the reduction of the adverse effects of acute Rt on the skin and soft tissues, but as the treatment planning and administration of IMRT are complex, and the risk of under-dosing is substantial, these techniques are better used by doctors who have the necessary experience [22,43-45].
The dose of Rt is determined by the initial extent of the disease and any known residue. After a groin LDN where microscopic inguinal metastases are found, 50Gy in fractions of 1.8–2.0Gy are usually sufficient. In the case of multiple N + or extracapsular dissemination, doses of Rt of up to 60Gy can be administered at a reduced volume. Macroscopic residual disease generally requires 60 to 70Gy to achieve a high probability of regional control of the disease [5,22, 43-45]. Women with vulvar cancer with lymph node metastasis benefited more from the addition of Qt to Rt [49].
Advanced Vulvar Cancer
Advanced vulva cancer includes tumors that extend beyond the vulva and / or where there are bulky lymph node metastasis in the groin [5, 22,37]. The treatment of women with advanced vulva cancer is complex and should be individualized and performed by a multidisciplinary team. When faced with advanced vulva cancer, the ideal is to determine the lymph node state before planning treatment [29, 41,44, 54]. Patients with clinically suspicious nodes should have fine needle aspiration or lymph node biopsy, and pelvic CT, MRI or PET-CT may be useful in determining the extent of inguinal and pelvic lymphadenopathy and the presence of metastatic disease a distance [5, 22, 43-45].
If there are no suspicious nodes, either clinically or in images, bilateral inguino-femoral LDN can be performed, and if the nodes are negative, Rt in English and pelvic nodes will not be necessary, if histology reveals positive nodes, then it should be offer adjuvant radiation to the groin and pelvis for early stage disease [51]. In cases where surgery is considered inappropriate for the individual patient, primary Qt.Rt can be used to treat the primary tumor, as well as the groin and pelvic ganglion [59, 61].
In patients with lymph node metastasis, the enlarged groin and pelvic nodes should be removed if possible, and the patient should be given postoperative inguinal and pelvic Rt. Complete LDN should not be performed because a dissection of the entire groin followed by Rt of the groin can cause severe lymphedema. The fixed or ulcerated lymph nodes in the groin should be biopsied to confirm the diagnosis, and then treated with primary Rt, with or without Qt; if there is an incomplete response to Rt, the nodes can be resected if appropriate [62]. In terms of the treatment of the primary tumor, surgical excision of the primary tumor with clear surgical margins and no sphincter damage, whenever possible, constitutes the Optimal way to treat advanced vulva cancer, as well as to alleviate symptoms such as local and offensive pain [5,22]. If proper removal of the primary tumor can only be achieved by exenteration and the formation of a bowel or urinary stoma, radiation therapy (with or without concurrent Qt) may be a preferred treatment alternative. Survival improves if any residual post-Rt [62] tumor is resected. Concurrent Qt-Rt is a well-described treatment alternative for those patients with large tumors in whom primary surgical resection would damage the central structures (anus, urethra), and have reported full long-term responses [5, 13]. The groin and pelvis nodes may need to be included in the radiation field depending on the state of the groin nodes [60, 62]. It has been reported that neoadjuvant treatment with cisplatin and 5-fluorouracil, or other combinations of Qt, is effective for the preservation of the anal sphincter and/or urethra in patients with advanced vulva cancer.
In relation to the planning of Rt in advanced vulva cancer, if the lymph node metastasis in the groin and comply with the indications described above for adjuvant Rt, the treatment fields of Rt should include the pelvis, inguinal and vulva. These should be treated with a total dose of at least 50Gy, with attention to adequate coverage of the inguinal nodes [62].
Severe disease or high-risk areas can be enhanced with appositional fields of selected electrons to provide a suitable dose to the surface and in depth, or with a conformal external beam therapy. Large vulvar tumors probably require 60–70Gy to achieve local control, although the relationship between dose and local control remains the subject of ongoing research [62,63].
Most recurrences of vulvar cancer at the same site in the vulva. It is believed that surgeons should aim for tumor-free pathological margins of 8mm or more to minimize local recurrence of the disease. Multiple retrospective studies have tried to evaluate the factors that can determine vulvar recurrence, and other clinical determinants have been suggested in addition to inadequate excision margins, although it is not clear which combination of factors is more significant [63,64]. Two types of local recurrences were described, those of the same site as the original (primary) tumor and those of a different vulvar site. An analysis of patients with vulvar cancer showed that recurrences at the primary site occurred with a mean disease-free interval of 21 months and were associated with a histopathological margin of 8mm or less, as reported in several other documents [22,53]. "Recurrences" in remote vulvar sites occurred later, with a mean disease-free interval of 69 months, and were more commonly associated with lichen sclerosus [40, 42].
Since most vulvar squamous carcinomas arise in an atypical skin fund such as HSIL, lichen sclerosus and dVIN, and as they characteristically recur locally but often in remote sites of the original tumor, it is suggested that many "recurrences" may actually be secondary. Primary tumors, which arise in a "cancer field", an area of genetically altered preneoplastic epithelium that has a predisposition to undergo a malignant transformation [40, 43].
Patients with close surgical margins (less than 5mm) benefit from postoperative Rt, if it is not possible to remove the margins. A study of 205 women with vulvar cancer reported that margins of 5mm or less represented the highest risk of vulvar recurrence, and that patients who received a dose of more than or equal to 56Gy had a lower risk of relapse than those who received less than or equal to 50.4G and [5, 13, 68].
Occasionally, positive margins can be increased with brachytherapy, although care must be taken to avoid the risk of necrosis. An alternative is to treat the surgical bed with an appositional electron field or with external beam Rt according to [61]. In recent years, efforts have been made to individualize and reduce radical treatment, with special emphasis on quality of life (QOL) after treatment of patients [10, 13], figure 1
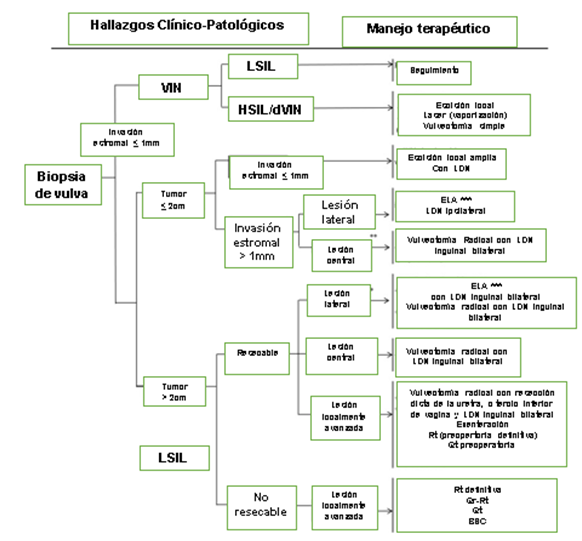
** Injuries to the midline
*** Isolated lesions without suspicion of positive nodes
Low-grade squamous intraepithelial lesion (LSIL)
High Gado Intraepithelial Squamous Injury (HSIL)
Intraepithelial vulvar neoplasia (VIN)
Intraepithelial differentiated vulvar neoplasia (VIN)
Chemotherapy (Qt
Radiotherapy (Rt)
Basal cell squamous carcinoma or Basosquamous cell carcinoma (BSC)
Melanoma Of The Vulva
Vulvar melanoma is the second most common vulvar malignant neoplasm. Any pigmented vulvar lesion should be biopsied or removed for diagnosis, unless it has been present and has not changed for some time [39]. Most vulvar melanomas involve the clitoris or the labia minora [22]. Clark or Breslow modifications of the system of Staging, as included in the American Joint Committee on Cancer (AJCC) system and based on the depth of the invasion, should be used for staging these lesions instead of the FIGO staging system, as it is the only system prospectively proven to correlate with recurrence and survival [69].
Surgery is the treatment of choice for vulvar melanomas. The lesions should be treated by ALS and radical, with margins around the lesion of at least 1cm [22]. The current trend leans towards a more conservative resection of vulvar melanomas because no difference in SV has been found in patients undergoing local excision versus those with radical vulvectomy [70, 71].
The role of lymphatic LDN is also controversial and, to date, no advantage has been demonstrated in survival for inguinal LDN [71], although the prospective, randomized, multi-institutional study of the Intergroup Program of Surgical Melanoma, elective LDN versus Observation of intermediate thickness (1–4mm) cutaneous melanomas revealed that elective LDN resulted in a significantly better survival for patients 60 years of age or younger, patients with 1–2mm thick tumors, and patients without tumor ulcer. Sentinel node biopsy has also been screened for vulvar melanoma, and although it is feasible, a false negative rate of 15% has been reported; It has been suggested that the procedure may increase the risk of locoregional recurrences and, therefore, is not a current standard practice [72, 74].
Bartholin Gland Cancer
Bartholin gland carcinomas are rare forms of vulvar cancer; some are associated with HPV-ar; the age varies from 38 to 72 years (with an average of 58.3 years); they are typically deep within the vulva and diagnosis is frequently delayed; As the extension to the overlying skin is a late manifestation and the extension through the Bartholin duct to the vagina, with the consequent bleeding as a presenting symptom is generally according to the tumor size; that this mass of the Bartholin complex is often diagnosed as Bartholin abscess or cyst; 50% of complex Bartholin cancers are of squamous histology and are believed to originate in the Bartholin duct instead of the gland. The rest includes a variety of rare adenocarcinomas including adenoid / c cystic carcinomas with indolent natural history, proneness to perineural invasion, and rare lymph node spread. All SCCs of the Bartholin gland expressed p16 diffusely and intensely regardless of histological characteristics and grade; they support the etiological role of HPV in the pathogenesis of SCC of the Bartholin gland. Bartholin gland cancers can be transitional cells or SCCs that arise from the duct, or adenocarcinomas that arise from the glands. There are also cystic and adenoscamosal adenoid variants. All SSCs showed a diffuse and intense p16 expression consistent with the presence of HPV [70, 75]. Most are in the early stage. . The average clinical follow-up was 53.7 months (range, 3-181 months), they are disease free (75%).
Diagnosis is often made after resection of a persistent or recurrent Bartholin cyst. [22]; The traditional approach to therapy is radical vulvectomy with bilateral and pelvic inguinal LDN or with a radical hemivulvectomy and a bilateral groin LDN; Due to the location of these tumors, deep in the ischiorectal fossa, adequate surgical margins are difficult to achieve and postoperative Rt decreases the probability of local recurrence and adjuvant Rt is recommended for positive margins or perineural invasion [75].
A complete excision of the disease often requires extensive and deep dissection. Less radical cleavages, such as local radical excision or partial vulvectomy with ipsilateral inguinal LDN, also appear to be effective. Surgical margins are often microscopically positive due to the proximity of the primary to the anus-rectum and pubic arch and require postoperative Rt to reduce the incidence of local recurrence. In the case of ipsilateral inguinal nodes, pelvic bilateral inguinal radiation and the frequency of regional recurrence may decrease. Primary Qt-Rt or brachytherapy are therapeutic options that may allow preservation of rectal function or obviate the need for surgery as a whole in women with primary carcinoma of the Bartholin gland. Qt-Rt is particularly effective in cancers with squamous histology. For advanced disease, individual case reports describe the activity for liposomal doxorubicin and paclitaxel [5, 22,75].
Radical local excision is usually adequate, such as locally invasive warty carcinoma, but rarely metastasizes. Suspicious lymph nodes should do a biopsy; if positive, then inguino-femoral lymphadenectomy is indicated. Rt is contraindicated because it is thought to induce anaplastic transformation and increase the probability of metastasis, but there is no evidence. Recurrences are usually treated with surgery [5, 22].
Paget's Disease Of The Vulva
Paget's disease is rare and affects the apocrine glands of the vulva. There are two types: the primary form begins as an intraepithelial lesion, but the secondary form is due to the invasion of an underlying adenocarcinoma, which can be anorectal, urothelial or genital tract carcinoma (for example, endocervical or endometrial) [77,78]. Paget vulvar disease occurs predominantly in postmenopausal women who present with vulvar pruritus and pain and, on examination, an eczematoid suppurative lesion is often observed. The diagnosis is usually confirmed by a biopsy, which will also help to differentiate between an intraepithelial and invasive lesion [24].
The treatment of choice for intraepithelial Paget's disease is wide local excision. Clear margins are difficult to achieve since histopathological changes often extend well beyond what is macroscopically visible; Even with adequate margins, recurrence rates are high. Treatment with Mohs micrographic surgery (ie, microscopically controlled systematic excision of cancerous tissue) may be associated with a lower recurrence rate, particularly for recurrent tumors, [5,22].
Due to the high recurrence rate and surgical morbidity, there is a current movement to perform a less radical resection for intraepithelial lesions, with a new excision at a later date if the lesions recur. Lesions involving the urethra or anus also present a management challenge and require laser therapy [20]. Another conservative treatment option is local imiquimod [5,22]. A Cochrane meta-analysis that investigated treatment options concluded that there was no "better" intervention for Paget vulvar disease [77]. If there is an underlying adenocarcinoma, the treatment should be a radically wide local excision with margins of at least 1cm. An inguine-femoral LDN should be performed, with adjuvant Rt for the same indications as for squamous carcinomas [78, 81], figure 2.
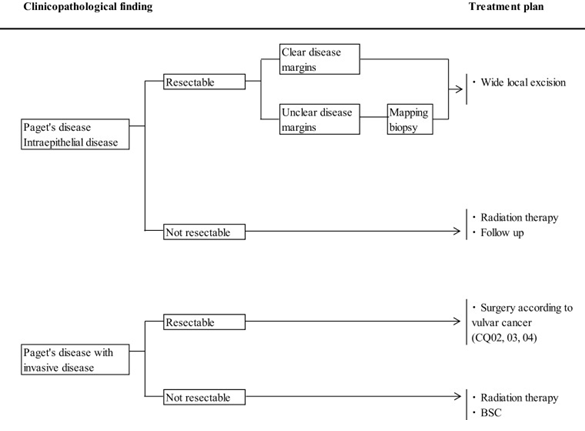
Positive surgical margins (M+)
Negative surgical margins (M-)
Basal cell squamous carcinoma or Basosquamous cell carcinoma (BSC)
Wide local excision is the standard method, lymph node metástasis are uncommon. Among the most common histological types are angiomyxoma and rhabdomyosarcoma; The latter is diagnosed in children. Surgical treatment is usually accompanied by preoperative or postoperative radiotherapy in analogy with the treatment of limbs and soft tissue sarcomas in anatomical sites where wide surgical margins cannot be obtained significantly absent, debilitating sequelae such as amputation of limbs [5, 22, 81].
Basal Cell Carcinoma
Basal cell squamous carcinoma or Basosquamous cell carcinoma (BSC), represents 2% of vulvar cancer, affect postmenopausal Caucasian women can be locally invasive; although, without metastatic; its typical appearance is the ulcer with irregular central borders; The lesion may be pigmented or pearly or gray. They are often asymptomatic, but itching, bleeding or pain may occur; associated with a high incidence of antecedent or concomitant malignancy in other parts of the body, a thorough search of other primary malignant tumors should be performed [5, 22,81].
Histopathological Considerations
In relation to sample analyzes, the following should be taken into account [29, 31]:
1. Orientation: the correct orientation of the surgical piece is important.
2. Photographs: of the complete sample, of the origin of each tissue block.
3. Measurements: sample size, dimensions of any visible tumor, tumor-free macroscopic margins and tumor depth (sections taken through the tumor). Sections should also be taken from the urethral, anal and vaginal resection margins
4. Lymph nodes: the site from which they were removed must be dissected, a complete cross section of each lymph node must be embedded.
The following histopathological points [27, 31] should be taken into account:
1. Type of tumor
2. Depth of invasion: measured from the epithelial-stromal junction of the adjacent dermal papilla to the deepest point of invasion by the tumor.
3. Tumor grade.
4. Histopathological measurement of tumor-free margins and declaration of whether the tumor is completely removed.
5. Presence or absence of perineural lymphovascular space invasion.
6. Nature of the adjacent squamous epithelium, for example, dVIN, lichen sclerosus and changes associated with HPV.
7. Sites and number of nodes examined, number of lymph node metástasis and presence or absence of extracapsular extension.
Vulvar cancer metastasizes by a variety of mechanisms. Understanding these potential pathways is important for the evaluation and treatment of these tumors; The spreads include:
Direct extension to adjacent structures (for example, the vagina, urethra, clitoris, anus).
Lymph node regional lymph nodes may occur early in the course of the disease, even in patients with small lesions; 10% of superficially invasive vulvar cancer (lesions > 1 but < 3mm of stromal invasion) had lymph node metastases at diagnosis [29, 31,41]. Most vulvar cancers first spread in the lymph nodes in the groin (inguinal-femoral), so these nodes are sampled as part of staging. Lesions found on one side of the vulva generally spread only to the ipsilateral inguinal nodes. Hematogenous dissemination, which usually occurs late in the course of the disease, is rare in patients without inguino-femoral lymph node involvement. In patients with less than three positive lymph nodes at the time of initial diagnosis they had a lower risk of hematogenous dissemination, compared to those with three or more positive lymph nodes (4 vs. 66%, respectively) [46, 53,57].
Postoperative Complications
In vulvar cancer it is relatively high. The rate of complications of the vulva in the wound varies from 9 to 58%, while frequent urination or urinary incontinence are confirmed in 8 to 28% of cases. The frequency of inguinal complications after inguinal lymphadenectomy is reported as 21 to 39% for infection, 17 to 39% for wound dehiscence, 21 to 57% for cellulite, 11 to 40% for lymphocele, and 14 to 48% for lymphedema. Most cases of lymphedema occur in the legs within the first 12 months after surgery and are chronic. Lymphedema is aggravated by obesity, infection, the addition of radiotherapy and deep vein thrombosis after surgery [29, 31, 41,46]. In addition, psychological and social problems occur frequently after surgery for vulvar cancer, including psychological stress, pain during sexual intercourse, decreased libido, frequent urination and incontinence. Because these problems are detrimental to the quality of life of a patient [41, 46, 53,57].
Local Recurrence
Treatment recommendations for patients with recurrent vulvar cancer take into account the patient's functional status, previous treatment modalities received, and recurrence sites [42].
Vulvar cancer recurrences are classified as (n primary or residual tumor bed in the vulva) or local, regional (in ganglia) or distant (hematogenous). The distribution of recurrences in 37% of which recurred after primary oncological (surgical) management: local recurrences in vulva or inguinal regions in 53 and 19%, respectively. The recurrences to distant involved the pelvis or extra-pelvic in 6 and 8%, respectively and the multiple recurrences [53, 55,56] in 14%.
Local Recurrence
Isolated local recurrence, which comes from a new excision instead of systemic therapy; local perineal recurrences are often treated successfully with re-excision, and inguinals their prognosis is worse; with 5-year survival rates according to recurrence site [5, 22]: in vulva 60%; inguinal and pelvic 27%, distance 15%, multiple 14%. Patients with a local recurrence who are not candidates for surgery should be offered local radiation if this has not been previously used. If previous radiation has been of a limited dose, it is prudent to return to irradiation at small target volumes along with concurrent chemotherapy may be a reasonable option in carefully selected patients with manageable late toxicity. For patients without surgical options or Qt-Rt, systemic chemotherapy, similar to the approach of women with metastatic disease, may be offered 5.22. The recommended treatments for recurrent disease, [10, 53, 55,56], figure 3
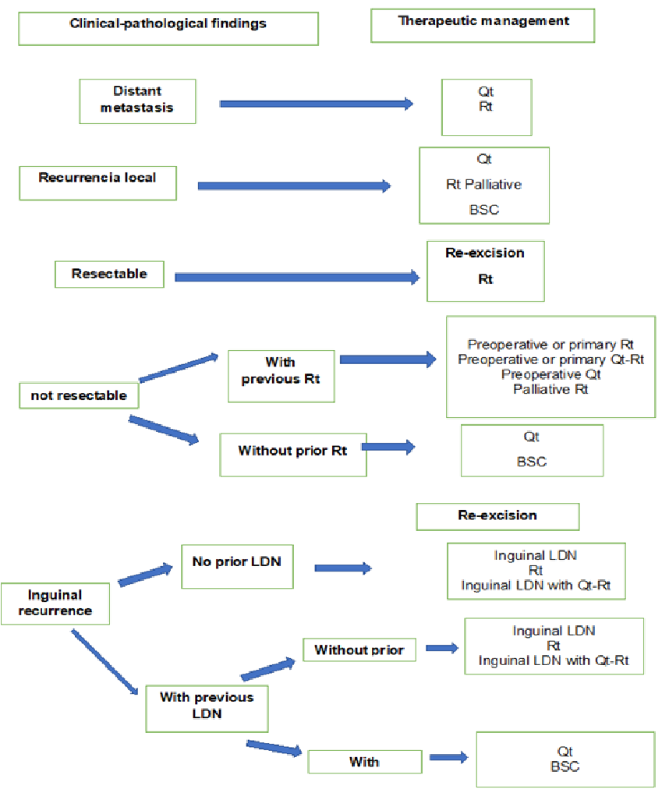
Qt (Chemotherapy), Rt (Radiotherapy), Basosquamous cell carcinoma (BSC), LDN (Lymphadenectomy)
For patients with recurrent disease that involves the pelvic region, multiple sites and/or distant metastatic disease, we offer chemotherapy, provided that the patients are candidates for systemic treatment. If patients are not candidates for or reject systemic treatment, referral to palliative care is appropriate.
There are no prospective first-line chemotherapy trials for this population. Therefore, we extrapolate our treatment of metastatic cervical cancer management, in which platinum-based treatment is routinely administered in this environment [10]. Our preference is to administer carboplatin plus paclitaxel because this combination has been shown to be better tolerated than cisplatin plus In paclitaxel in a trial of women with metastatic cervical cancer, there is little data on the efficacy of the first and adjuvant Qt. The Qt-Rt that are active in other types of squamous cell cancer are not as active in vulvar metastatic carcinoma [22]. Women who are not candidates for chemotherapy due to comorbidities or poor general condition should receive palliative care. For these patients, Rt can provide relief to symptomatic sites [10, 22, 42, 53, 55,56].
Follow-Up And Surveillance After Treatment
The majority of vulvar cancer relapses occur in the first year, 10% had a second malignancy diagnosed ≥ 5 years after initial treatment, demonstrating the need for long-term follow-up; interrogating, the symptomatology and performing exploration of the vulva, skin and inguinal nodes; in early stage, it is done every six months during the first 2 years and then annually; in advanced stage, every three months for the first 2 years, and then every six months for 3 to 5 years, and then annually (the Pap cervical or vaginal if the cervix has been removed annually). Routine use of imaging studies should be avoided. Most salvageable recurrences are easily detected by physical examination. If recurrence is suspected, computed tomography and / or positron emission tomography are performed, colposcopy and vulvar biopsy are indicated when abnormalities are observed on physical examination [79, 81]. Sexual dysfunction and alterations in body image are common after treatment and should be addressed during follow-up visits [22].
Vulvar cancer is one of the less common gynecological cancers, and the role of its prognostic factors is far from clear; is associated with a greater probability of receiving a suboptimal treatment in patients with multiple comorbidities, which increases the risk of disease recurrence and mortality because vulvar cancer is difficult to perform a prospective evaluation of prognostic factors, age represents a Confusion factor when assessing the impact of comorbidities on Survival, to be used as a tool for a more personalized and individualized management of the patient.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.
