Motor Ability and Mental Health of Young Children: A Longitudinal Study
 Shogo Hirata
Shogo Hirata Yosuke Kita
Yosuke Kita Kota Suzuki
Kota Suzuki Yuzuki Kitamura2,3†
Yuzuki Kitamura2,3† - 1Department of Elementary Education, Ibaraki Christian University, Hitachi, Japan
- 2Department of Developmental Disorders, National Institute of Mental Health, National Center of Neurology and Psychiatry, Kodaira, Japan
- 3Faculty of Education, Tokyo Gakugei University, Koganei, Japan
This study used a longitudinal method to investigate relations between motor abilities and mental health in young children. We analyzed longitudinal data of 38 Japanese children who were 3–6 years old. We administered the Movement Assessment Battery for Children–Second edition (MABC2) and Strength and Difficulties Questionnaire (SDQ) at 3–4 years and 5–6 years of age: MABC2 was used to evaluate each child’s motor ability; SDQ was used to assess the degree of their mental health difficulties and prosocial behavior. Logistic regression results indicated that the MABC2 score at 3–4 years can predict the risk of motor skill impairments at 5–6 years (adjusted odds ratio was 0.354). Motor ability assessed at 3–4 years, however, did not predict the risk of mental health problems at 5–6 years. Analyses of longitudinal quantitative changes in motor ability and mental health confirmed these results. Mental health problems that occurred at 5–6 years were related only to individual SDQ score differences at 3–4 years. The MABC2 total score at 3–4 years was not related to later prosocial behavior. Boys tended to obtain a lower MABC2 score at 5–6 years. Girls tended to obtain a higher SDQ prosocial score at 5–6 years. Results of this study suggest that motor skill impairment and SDQ-measured mental health are independent characteristics in young Japanese children aged 3–6 years.
Introduction
In recent years, relations between motor skill impairment and mental health in children have received increasing attention (Cairney et al., 2010; Hill, 2010; Mancini et al., 2019). Responses of parents to questionnaire surveys frequently indicate emotional and behavioral difficulties in children with developmental coordination disorder (DCD; Emck et al., 2009), a neurodevelopmental disorder characterized by motor skill impairment and difficulties related to daily living, academic, and vocational settings (American Psychiatric Association, 2013). Usually, DCD has been diagnosed after a child has become 6 years old (Blank et al., 2012). Epidemiological studies have revealed that children quite commonly have DCD and also that this disorder is much more common among boys than among girls (Kadesjo and Gillberg, 1999; Du et al., 2020). Many reports have described studies showing DCD comorbidity with other developmental disorders such as attention deficit hyperactivity disorder (ADHD), dyslexia, and autism spectrum disorders (ASD) (Hulme and Snowing, 2009; Hirata et al., 2015).
Skinner and Piek (2001) reported from analysis of subjective rating scales that children (8–10 years of age) and adolescents (12–14 years of age) with DCD had lower self-worth in various domains such as physical, social, and academic domains. Skinner and Piek (2001) also reported that children and adolescents with DCD had higher degrees of anxiety than their peers. Children with DCD (7–10 years of age) displayed higher rates of emotional and behavioral difficulties than their peers, based on their teachers’ and parents’ subjective ratings from the Strength and Difficulties Questionnaire (SDQ; Crane et al., 2017).
Reports of some studies have described that these mental health problems are secondary to motor-related problems that appear once a child begins elementary school, when they are challenged by social and peer demands (environmental stress hypothesis, Cairney et al., 2010; Mancini et al., 2019; Piek et al., 2008). These findings indicate that monitoring the mental health of children with a lower degree of motor ability is crucially important. Almost all such studies, however, have investigated relations between motor skills and mental health in elementary school children and adolescents (Emck et al., 2009; Rodriguez et al., 2019). Few researchers have examined these links in children as young as 3–6 years.
Almost all earlier reports of the relevant literature describe studies that have adopted cross-sectional methods (Cairney et al., 2010; Emck et al., 2009; Mancini et al., 2019). Cross-sectional methods analyze data from a population at one specific point in time. If children with low motor abilities are growing and developing along with their mental health problems (Piek et al., 2008; Cairney et al., 2010; Mancini et al., 2019), then their respective motor capabilities at an early age can facilitate prediction of the severity of mental health difficulties they might face at a later age. No report has described a study conducted using this longitudinal method to test this hypothesis in children as young as 3 years.
Another causal relation can be postulated. Empirical studies have revealed that one’s mental state, such as motivation, can improve movement test performance (Moreno et al., 2010). If some children have high severity of mental health problems in their early years, such as hyperactivity or anxiety, then these psychological conditions might prevent the subsequent development of motor skills (Cantell et al., 1994). It seems necessary and valuable to clarify relations between motor abilities and mental health in young children from a longitudinal perspective.
This study uses a longitudinal method to investigate the relation between motor abilities and mental health in young Japanese children (Anastassiou-Hadjicharalambous and Stylianou, 2011). We applied the Second version of the Movement Assessment Battery for Children (MABC2; Henderson et al., 2007) and SDQ (Goodman and Goodman, 2009) to examine 3–6-year-old Japanese children. The former, MABC2, is used to evaluate a child’s motor ability and is used worldwide to identify DCD (Blank et al., 2012). The latter, SDQ, is used worldwide to assess aspects of mental health (Goodman and Goodman, 2009; Kremer et al., 2015; Maurice-Stam et al., 2018). Many studies have confirmed the general validity and reliability of these two scales, and specifically for Japanese children (Matsuishi et al., 2008; Hirata et al., 2018). Despite the international use of MABC2 and SDQ, few reports of the relevant literature have described studies investigating these scales’ predictive value (Griffith et al., 2017; Neilsen et al., 2019). In actuality, MABC2 and SDQ can provide a quantitative score and a cut-off point to identify DCD risks and to clarify aspects of mental health. The cut-off point of each scale has been used to identify the risk of disorder (Hirata et al., 2015). The quantitative score provides continuous information of a participant’s ability. To confirm the predictive value of MABC2 and SDQ, we conducted longitudinal analyses using quantitative scores and cut-off points of these scales.
In fact, the SDQ can evaluate not only the severity of children’s mental health problems but also the prosocial behavior (Goodman, 1994). If children with high motor ability are growing and developing along with good mental health, then their respective motor capabilities at an early age can predict positive aspects of mental health at a later age. We also assessed this point from a longitudinal perspective.
Earlier studies have demonstrated sex differences for MABC2 (Hirata et al., 2018) and SDQ (Matsuishi et al., 2008; Kremer et al., 2015). Hirata et al. (2018) reported significantly higher MABC2 total scores for Japanese girls aged 3–6 years than for boys of similar age. Matsuishi et al. (2008) also reported significantly higher SDQ total scores for Japanese boys than for girls. In this study, we included participants’ sex for longitudinal analyses.
Aims
The purpose of this study was to clarify the relation between motor abilities and SDQ-measured mental health in Japanese 3–6-year-old children from a longitudinal perspective. We took two measurements using a longitudinal method. Then, we analyzed the correlation among variables. Dependent variables were quantitative scores and cut-off points of MABC2 and SDQ at the second measurement. Independent variables were quantitative scores of the MABC2 and SDQ at the first measurement. We also included participants’ sex among independent variables. We hypothesized that the degree of motor ability at an early age can predict the severity of mental health problems at a later age (Piek et al., 2008; Cairney et al., 2010; Mancini et al., 2019). The relation between motor ability at an early age and SDQ-measured prosocial behavior at a later age was also analyzed.
Materials
Participants
We requested study participation at nursery schools attached to a university. One nursery school agreed to participate in this longitudinal study. The activities of Japanese nursery schools follow the national curriculum. Therefore, this nursery school does not appear to be a special case. The selection of this school does not influence the generalizability of study results to any great degree. Children were included if they had normal or corrected-to-normal vision and had no apparent illness or condition that might affect motor skills. Children were excluded if they had a severe neurological disorder or any physical difficulty. Their condition was confirmed from interviews of their guardians and reviews of their records. The parental socioeconomic status, such as education and income level, was not investigated, similarly to an earlier Japanese MABC2 study (Hirata et al., 2018). Participants’ ethnic origins were not investigated because the Japanese population shows higher ethnic homogeneity than either European or North American countries.
Nursery schools typically have three grades in Japan. Each grade extends from April of 1 year through March of the next year. The nursery schools we investigated had two classes in each grade. For this study, two measurements were taken using the longitudinal method. The first measurement was taken during July–September of 2016 for children of the first-grade classes. This grade included children late in their third year of age to early in their fourth year of age. The second measurement was taken from November 2018 through January 2019 for children of third-grade classes. In other words, child data were collected at the beginning (late 3 years of age to early 4 years of age) and the end (late 5 years of age to early 6 years of age) of 3 years of a nursery school. The mean (standard deviation) duration between the first and second measurements was 28.4 (1.3) months.
Movement Assessment Battery for Children–Second Edition
MABC2 consists of eight subtests that produced a total motor score and three sub-component scores: Manual Dexterity (MD), Aiming–Catching (AC), and Balance (BAL). This assessment was used as an objective assessment of each child’s fundamental motor abilities. For this study, the test set for the age band 1 (3–6 years) was applied. The test manual was translated from English into Japanese by two expert psychologists, each of whom was familiar with psychological testing for young Japanese children. Then, after exchanging two independently translated manuals, they were confirmed as not being different from one another in terms of the methods of task administration, recording, and scoring of the child’s motor performance (Hirata et al., 2018).
The MD component includes three tasks: a one-hand posting task (e.g., “picking up the coins and putting them in the box one at a time”), a timed bi-manual assembly task (e.g., “picking up the beads and threading them one at a time”), and an untimed drawing task (e.g., “drawing as slowly as necessary to keep within the boundary lines”). The AC component includes tasks requiring the throwing of an object to a target (e.g., “throwing the beanbag with only one hand”), and the catching of an object using both hands (e.g., “catching the beanbag with two hands”). The BAL component consists of a static balance task (e.g., “remain standing on one foot in one place while balancing”) and two dynamic balance tasks that involve sustained, controlled movement (e.g., “walking along a line with heels raised without stepping off the line”), and more explosive action (e.g., “jumping on mats, inside their boundaries”). Test–retest reliability of the MABC2, for which the time frame was 2 weeks, was acceptable (Henderson et al., 2007). The internal consistency of the Japanese version of the MABC2 for age band 1 was acceptable (Hirata et al., 2018).
According to many earlier studies, and particularly according to a review by Emck et al. (2009), the norms attached to the test manual were used to convert raw scores to each age-adjusted standard score (SS) such as eight test items, three components, and the total score. Sex-specific norms were not provided (Henderson et al., 2007). The mean of these SSs was 10. The standard deviation was 3. Lower SS values reflect poor motor abilities. For the test set for age band 1, interpretation should be assigned primarily to the total test score based on confirmed factor analysis (Schulz et al., 2011; Hirata et al., 2018). The total test score was analyzed in this study. The 16th percentile of this score was used as a lower cut-off point to identify the risk of motor skill impairment or DCD (Henderson et al., 2007).
Strength and Difficulties Questionnaire
The SDQ teacher-reported or parent-reported measure of a child’s mental health is a 25-item questionnaire. Each item is rated on a three-point scale. This questionnaire can produce a total difficulty score and five subscores such as emotional symptoms (e.g., often complaining of headaches, stomachaches, or sickness), negative conduct (e.g., often losing one’s temper), hyperactive/inattention (e.g., restless, overactive, cannot remain still for long), peer difficulties (e.g., rather solitary, preferring to play alone), and prosocial behavior (e.g., considerate of other people’s feelings). The total difficulty score is calculated by adding four subscores such as emotional symptoms, negative conduct, hyperactive/inattention, and peer difficulties. This score is 0–40. Higher scores indicate greater severity of mental health problems. The prosocial behavior subscore is 0–10. Higher scores indicate a greater degree of prosocial behavior. Test–retest reliability of the Japanese version of the SDQ, for which the time frame was 2 weeks, has been reported as acceptable (Doi et al., 2014). The internal consistency of the Japanese version of the SDQ is also acceptable (Matsuishi et al., 2008).
For early assessment of a child’s mental health, the use of the total difficulty score alone has been recommended (Elberling et al., 2010; Goodman and Goodman, 2009). According to the Japanese norm (Matsuishi et al., 2008), we classified the child’s mental health based on the total difficulties score. Sex-specific norms were not provided with the Japanese norms. A score of 12 or higher was regarded as a cut-off point to identify the risk of mental health problems, i.e., having some need or having high need for intervention.
Procedure
Ethical approval for the study was obtained from the Research Ethics Board of Tokyo Gakugei University (No. 282). Consent for each child’s participation in the study was obtained from proxies. MABC2 was administered twice. MABC2 was administered individually to each child in a quiet room of the nursery school. On average, 25 min were necessary to complete this test. Expert psychologists who had been fully trained to administer MABC2 conducted this test.
When the first and second measurement periods of MABC2 for children started, we provided each class teacher with SDQ questionnaires for participants. Young Japanese children typically spend 5 days a week in nursery school. Therefore, we used teacher-report ratings. The teacher was asked to evaluate each child’s behavior during recent months. The first author collected the completed SDQ questionnaires at the end of the first and second measurement periods. In Japanese nursery schools, class members and class teachers change every year. Consequently, SDQ raters differed each time.
Statistical Analyses
First, we analyzed the predictive values of the MABC2 total score and SDQ total difficulty score at 3–4 years for the risk of motor and mental health difficulties at 5–6 years using logistic regression analysis. Independent variables were the participant’s sex (male assigned 1; female assigned zero), MABC2 total score, and SDQ total difficulty score at 3–4 years. Dependent variables were binary, based on cut-off points of MABC-2 and SDQ at 5–6 years.
Second, we conducted multiple regression analyses using quantitative scores to model the longitudinal quantitative change of motor ability and mental health difficulties in young children. Independent variables were participants’ sex, the MABC2 total score, and SDQ total difficulty score at 3–4 years. Dependent variables were the MABC-2 total score, SDQ total difficulty score, and SDQ prosocial score at 5–6 years. These statistical analyses were conducted using software (IBM SPSS Statistics 22; SPSS Japan Inc., Tokyo). Significance of the results was inferred for p less than 0.05. The statistical power of each regression analysis using post-hoc procedures was calculated using G Power 3.1 (Faul et al., 2009). Power above 0.8 was regarded as acceptable (Cohen, 1992).
Results
This study analyzed the longitudinal data of 38 children (15 boys, 23 girls; aged 3–6 years) who were recruited from one nursery school in Japan. For the first measurement, we conducted MABC2 for all children in the first grade [N = 40, median (interquartile range) was 46.5 (6) months]. We examined all children in the third grade, but two children subsequently transferred to another nursery school. Eventually, 38 children participated in the second measurement [median (interquartile range) was 74.5 (5.8) months].
Descriptive Statistics
All measured values were tested for deviation from normality. Shapiro–Wilk normality tests revealed that not all measures were normally distributed: the MABC2 total score at 3–4 years was normally distributed (W = 0.957, p = 0.148); the SDQ total difficulty score at 3–4 years was not normally distributed (W = 0.874, p < 0.001); the SDQ prosocial score at 3–4 years was not normally distributed (W = 0.927, p = 0.016); the MABC2 total score at 5–6 years was not normally distributed (W = 0.943, p = 0.052); the SDQ total difficulty score at 5–6 years was normally distributed (W = 0.952, p = 0.102); and the SDQ prosocial score at 5–6 years was not normally distributed (W = 0.924, p = 0.013). According to earlier studies (Hirata et al., 2018), the statistical criteria for Cronbach’s alpha coefficients were set as follows: values of 0.70–0.80 were considered high; values of 0.60–0.69 were considered acceptable; and values less than 0.50 were regarded as having poor reliability. Values of the Cronbach’s alpha coefficients for each scale were ranged from 0.562 to 0.836, which indicates acceptable internal consistencies among test items (for the MABC2 total score at 3–4 years: α = 0.636; for the SDQ total difficulty score at 3–4 years: α = 0.625; for the SDQ prosocial behavior score at 3–4 years: α = 0.836; for the MABC2 total score at 5–6 years: α = 0.562; for the SDQ total difficulty score at 5–6 years: α = 0.775; for the SDQ prosocial behavior score at 5–6 years: α = 0.797).
Table 1 presents descriptive statistics of participant age and score for each scale in the first (3–4 years) and second measurements (5–6 years). Each median of the MABC2 total score of the present sample was of an age-appropriate level. Each median of the SDQ total difficulty score also indicated a low risk of mental health problems. Wilcoxon signed-rank test results revealed no significant difference between the first and second measurements of the MABC2 total score (V = 176.5, p = 0.06). No significant difference between the first and second measurements of the SDQ total difficulty score (V = 471.0, p = 0.07) was found from Wilcoxon signed-rank test results. Four children had been included in the risk of motor skill impairments group from the first measurement to the second measurement. Only one child had been included in the risk of mental health problems group from the first measurement to the second measurement. Wilcoxon signed-rank test results revealed significant difference between the first and second measurements of the SDQ prosocial score (V = 552.5, p < 0.01).

TABLE 1. Descriptive statistics (N = 38, 15 boys, 23 girls).
Predictive Values of MABC2 and SDQ Score at 3–4 Years for Risk of Motor and Mental Health Difficulties at 5–6 Years
Table 2 presents some results obtained from logistic regression analysis. As a model to predict the risk of motor skill impairment at 5–6 years, this model was able to distinguish between children at 5–6 years (χ2 = 18.237, p < 0.001). This model correctly identified 34 (89.5%) children. Participants’ sex was found to be significantly (p = 0.036) and positively associated with the dependent variable: boys had higher odds than girls for inclusion in the “risk of motor skill impairments” group (standardized partial regression coefficient (β) = 0.388; adjusted odds ratio (OR) = 195.245; 95% confidence intervals (CI) were 1.402–27173.172). The score of MABC2 at 3–4 years was significantly (p = 0.034) and negatively associated with the dependent variable, i.e., lower MABC2 scores at 3–4 years were associated with higher probability of inclusion in the “risk of motor skill impairment” group at 5–6 years (β = −0.464; OR = 0.35, 95% CI were 0.135–0.925). As a model for predicting mental health problem risks at 5–6 years, this model was not able to distinguish among children (χ2 = 4.128, p > 0.05).
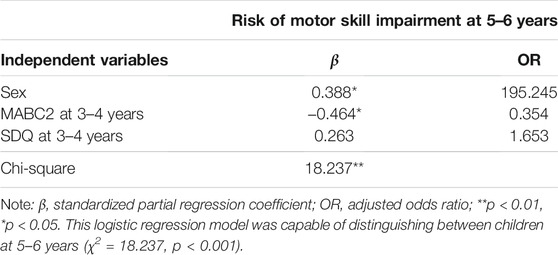
TABLE 2. Logistic regression analysis results.
Longitudinal Quantitative Change of Motor Ability and SDQ-Measured Mental Health
Three multiple regression analyses were conducted. Table 3 presents the results of these analyses. The multiple regression coefficients of each analysis were found to be significant (for the MABC2 total score at 5–6 years: F3. 34 = 6.462, p < 0.001; for the SDQ total difficulty score at 5–6 years: F3. 34 = 7.215, p < 0.001; for the SDQ prosocial behavior score at 5–6 years: F3. 34 = 8.241, p < 0.001). Post-hoc power analysis revealed that multiple regression analyses for MABC2 score at 5–6 years had adequate power: 0.92. Post-hoc power analysis also revealed that multiple regression analyses for SDQ total difficulty score at 5–6 years had adequate power: 0.95. Finally, post-hoc power analysis revealed that multiple regression analyses for SDQ prosocial behavior score at 5–6 years had adequate power: 0.97. Normal Q–Q plots of each analysis confirmed the normality of residuals. For the MABC2 total score at 5–6 years, participant sex was significantly (p = 0.032) and negatively associated, i.e., boys tended to obtain a lower MABC2 score (β = −0.310; 95% CI were −0.592–-0.028). The MABC2 at 3–4 years was significantly (p = 0.004) and moderately positively associated (β = 0.429; 95% CI were 0.144–0.715).
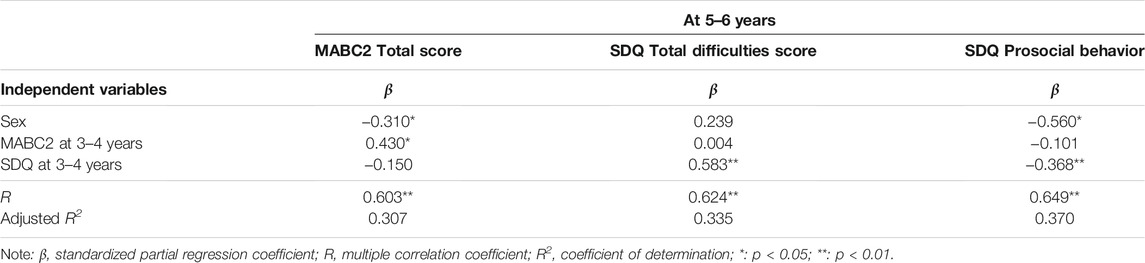
TABLE 3. Multiple regression analyses results.
For the SDQ total difficulties scores at 5–6 years, the SDQ at 3–4 years was found to be significantly (p < 0.001) and moderately positively associated (β = 0.583; 95% CI were 0.307–0.859). For the SDQ prosocial behavior score at 5–6 years, the SDQ total difficulty score at 3–4 years was significantly (p < 0.001) and moderately negatively associated (β = −0.368; 95% CI were −0.637–0.100), i.e., a higher SDQ total difficulty score at 3–4 years was associated with a lower SDQ prosocial behavior score at 5–6 years. Moreover, participant sex was significantly (p < 0.001) and negatively associated, i.e., girls tended to obtain a higher SDQ prosocial behavior score (β = −0.560; 95% CI were −0.829–0.291).
Discussion
Relation Between Motor Abilities and SDQ-Measured Mental Health in Young Children From a Longitudinal Perspective
We hypothesized that the degree of motor capability at an early age can predict the severity of mental health problems at a later age (environmental stress hypothesis, Piek et al., 2008; Cairney et al., 2010; Mancini et al., 2019). Based on the explanation presented above, we analyzed the MABC2 total score, the SDQ total difficulty score, and the SDQ prosocial behavior score. Results obtained from logistic regression analysis, however, indicated that motor abilities at 3–4 years are insufficient to predict the risk of mental health problems at 5–6 years. Individual differences in mental health at 3–4 years, and vice versa, were also insufficient to predict a risk of motor skill impairment at 5–6 years. Multiple regression analyses conducted using quantitative scores of each scale yielded similar results.
These results clarify motor skill impairments and mental health problems as independent characteristics for 3–6-year-old Japanese children. Pick et al. (2008), using a cross-sectional method, reported similar results obtained for 3–5-year-old children. Earlier studies indicated the possibility that “long-term” negative experiences related to low motor ability lead to mental health problems when growing up (Pick et al., 2007; 2008). Cairney et al. (2010) assumed that children are exposed to a “cascade” of negative psychosocial consequences when motor skill difficulties are a primary stressor. Results of many studies have indicated that children of this age have higher or optimistically perceived self-competence (Bouffard et al., 2003; Harter and Pike, 1984). This characteristic of young children might prevent the development of mental health problems at nursery school. Pick et al. (2008) pointed out a need to investigate the relation between motor and social aspects at different developmental stages. Mancini et al. (2018) emphasized the same point. Results obtained from the present study support this idea. Further research must be conducted to clarify the longitudinal link between motor ability and mental health during a longer period, such as from young childhood to adolescence. Individual differences of motor development are wide. Therefore, the diagnosis of motor skill impairment has been recommended for children above 6 years (Blank et al., 2012). From this perspective as well, an investigation conducted on a larger time scale is reasonable and necessary.
Contrary to the environmental stress hypothesis, Rodriguez et al. (2019) reported based on results from their cohort cross-sectional study that children aged 4–5 years with motor skill impairment have more Child Behavior Checklist (CBCL) points measuring psychological problems. To ascertain the nature of a link between motor ability and mental health, more research is expected to be necessary. Specific examination has been made of the high co-occurrence of motor skill impairments and other developmental disabilities (Hulme and Snowing, 2009; Hirata et al., 2015). Assessment of the degrees of various symptoms such as ADHD and ASD must be included in future research.
This study also investigated the relation between motor ability at an early age and SDQ-measured prosocial behavior at a later age. The MABC2 total score at 3–4 years was not related to later prosocial behavior. Bart et al. (2007) reported that the motor abilities of 88 children aged 5 years were positively related to social and emotional adjustment at an elementary school. Other studies, however, reported the SDQ prosocial behavior score as negatively related to fine motor skills in 245 children aged 5 years (Sargisson et al., 2014). These conflicting results are difficult to explain. Further research must be undertaken, especially because it is important to use the same scale such as the MABC2 and the SDQ among studies. Girls tended to obtain a higher prosocial behavior score at 5–6 years in this study. A study to establish the Japanese norm of the SDQ yielded the same result (Matsuishi et al., 2008). This tendency was in accord with the classical gender socialization theory (Brody, 1999). The Millennium Cohort Study of England (n = 9,850) revealed that the SDQ total difficulty score of children aged 3–7 years was related negatively and in a longitudinal manner to SDQ prosocial behavior (Flouri and Sarmadi, 2016). The same result was obtained from the present study.
Predictive Value of the MABC2
Results indicated that the score of MABC2 at 3–4 years can predict risk of motor skill impairment at 5–6 years. Multiple regression analysis supported similar results. Griffith et al. (2017) reported similar results, indicating the MABC2 score at 4 years of age as predictive of motor skill impairment at 8 years in children who had been born preterm. This study was unable to correct neonatal information such as birth weight and gestational age. Investigating the relation between neonatal information and MABC2 scores in our participants is necessary, but this study provided evidence of the longitudinal validity of MABC2. This study’s results indicate the possibility of the usefulness of MABC2 for assessment and early detection of motor skill impairments in young children.
As described in Methods, MABC2 can produce three sub-component scores: Manual Dexterity, Aiming–Catching, and Balance. Hirata et al. (2018) reported that this theoretical three-component model of MABC2 does not fit Japanese children aged 3–6 years. For that reason, only the MABC2 total score was used for this study. It might be valuable to ascertain whether the MABC2 sub-components differently reflect children’s mental health. Additional research must be conducted to elucidate the use of MABC2 sub-components for assessment of young Japanese children.
Similarly to earlier studies (Kadesjo and Gillberg, 1999; Du et al., 2020), this study also revealed that boys tend to have a risk of motor skill impairment. Du et al. (2020) reported that boys have a much higher prevalence of DCD than girls based on a nationally representative sample. They also acknowledged that this phenomenon is not attributable to single-factor contributions such as personal, environmental, and genetic factors. Many studies have indicated that boys have a higher prevalence of various neurodevelopmental disorders such as dyslexia (Arnettet al., 2017), ADHD (Sauver et al., 2004), and ASD (Hulme and Snowing, 2009). Garcia (1994) reported that sex-related differences in young children can be attributed more to socio-environmental factors than to biological factors when learning motor skills. For example, boys are more likely than girls to define advantaged social status in terms of motor skills (Chase and Dummer, 1992). More research is necessary to clarify the nature of sex-related differences for the MABC2 score of young Japanese children, especially addressing the two perspectives of biological factors and socio-cultural factors.
Predictive Value of the SDQ
The SDQ score at 3–4 years was moderately associated with the SDQ score at 5–6 years, but it did not predict a child’s risk of mental health problems at 5–6 years. Only one child had been included in the group with risk of mental health problems from the first measurement (3–4 years) to the second measurement (5–6 years). These results revealed that the predictive value of SDQ was not high for young children aged 3–6 years. Neilsen et al. (2019) reported that the SDQ sub-scores at 5–7 years were sufficient to identify mental disorders at 11–12 years. Nevertheless, they emphasized the importance of continuous assessment throughout childhood. One can reasonably infer mental health problems in early years as risk factors, but not as decisive factors, leading to mental health problems in later years. Longitudinal characteristics of SDQ have not been investigated adequately (Neilsen et al., 2019). Results of this study indicate the importance of continuous assessment throughout childhood.
Limitations
This study has some limitations. Only one nursery school participated in this study. Because of the small sample size, some statistical analyses might not have adequate power. Based on results of a priori power analyses, more participants and nursery schools must be included to reinforce the validity of these results. Moreover, the 3-year design of this study might not reflect causal relations between motor skill impairments and mental health. Future studies must use a longer time scale, such as that from young childhood to adolescence.
Another shortcoming was that only the teacher-rating SDQ was used. Triangulation of reporting involving multiple perspectives such as reported information from parents, teachers, and clinical psychologists (Crene et al., 2017) must be incorporated into further studies. The raters differed at each measuring time point, but earlier studies revealed that SDQ had good inter-rater reliability (van Widenfelt et al., 2003). Moreover, the SDQ score at 3–4 years was moderately associated with the SDQ score at 5–6 years in this study. Therefore, we think that rater-differences posed no particular shortcoming. The gap separating objective motor assessment such as the MABC2 and the subjective child’s mental health questionnaire such as the SDQ must also be considered. The subjective child’s psychological questionnaire has a risk of overestimation and underestimation (e.g., Hirata et al., 2015). To confirm the reliability of subjective evaluation of a child’s mental health, triangulation by different raters must be used.
The results of this study of gender differences were consistent with those found from earlier studies. In the nursery school investigated this time, unfortunately, there were fewer boys than girls. This point should also be resolved through future studies.
Conclusion
This study investigated relations between motor abilities and the SDQ-measured mental health of young children using a longitudinal method. Although some difficulty arose because of the small sample size, the study results indicate the importance of investigating the longitudinal relation between motor ability and mental health from young childhood to adolescence.
Data Availability Statement
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Research Ethics Board of Tokyo Gakugei University. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author Contributions
SH, YoK, SK, and YuK acquired the data. SH analyzed and interpreted the data. SH wrote the manuscript. All the authors made substantial contributions to the conception and design of the study.
Funding
This study was supported by the Grants-in-Aid for Scientific Research (B) (17H02145 to MK) and Grants-in-Aid for young scientists (18K17899 to SH) of the Japan Society for the Promotion of Science.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders. Fifth Edition. Arlington: American Psychiatric Association Publishing.
Anastassiou-Hadjicharalambous, X., and Stylianou, M. (2011). “Longitudinal Methods,” in Encyclopedia of Child Behavior and Development. Editors S. Goldstein, and J. A. Naglieri (Boston, MA: Springer), 898–900. doi:10.1007/978-0-387-79061-9_1684
Arnett, A. B., Pennington, B. F., Peterson, R. L., Willcutt, E. G., DeFries, J. C., and Olson, R. K. (2017). Explaining the Sex Difference in Dyslexia. J. Child. Psychol. Psychiatry 58 (6), 719–727. doi:10.1111/jcpp.12691
Bart, O., Hajami, D., and Bar-Haim, Y. (2007). Predicting School Adjustment from Motor Abilities in Kindergarten. Inf. Child. Develop. 16 (6), 597–615. doi:10.1002/icd.514
Blank, R., Smits-Engelsman, B., Polatajko, H., and Wilson, P. (2012). European Academy for Childhood Disability (EACD): Recommendations on the Definition, Diagnosis and Intervention of Developmental Coordination Disorder (Long Version). Dev. Med. Child. Neurol. 54 (1), 54–93. doi:10.1111/j.1469-8749.2011.04171.x
Bouffard, T., Marcoux, M. F., Vezeau, C., and Bordeleau, L. (2003). Changes in Self-Perceptions of Competence and Intrinsic Motivation Among Elementary Schoolchildren. Br. J. Educ. Psychol. 73, 171–186. doi:10.1348/00070990360626921
Cairney, J., Veldhuizen, S., and Szatmari, P. (2010). Motor Coordination and Emotional-Behavioral Problems in Children. Curr. Opin. Psychiatry 23 (4), 324–329. doi:10.1097/YCO.0b013e32833aa0aa
Cantell, M. H., Smyth, M. M., and Ahonen, T. P. (1994). Clumsiness in Adolescence: Educational, Motor, and Social Outcomes of Motor Delay Detected at 5 Years. Adapted Phys. Activity Q. 11 (2), 115–129. doi:10.1123/apaq.11.2.115
Chase, M. A., and Dummer, G. M. (1992). The Role of Sports as a Social Status Determinant for Children. Res. Quart. Exercise Sport 63 (4), 418–424. doi:10.1080/02701367.1992.10608764
Crane, L., Sumner, E., and Hill, E. L. (2017). Emotional and Behavioural Problems in Children with Developmental Coordination Disorder: Exploring Parent and Teacher Reports. Res. Dev. Disabil. 70, 67–74. doi:10.1016/j.ridd.2017.08.001
Doi, Y., Ishihara, K., and Uchiyama, M. (2014). Reliability of the Strengths and Difficulties Questionnaire in Japanese Preschool Children Aged 4-6 Years. J. Epidemiol. 24 (6), 514–518. doi:10.2188/jea.je20140050
Du, W., Ke, L., Wang, Y., Hua, J., Duan, W., and Barnett, A. L. (2020). The Prenatal, Postnatal, Neonatal, and Family Environmental Risk Factors for Developmental Coordination Disorder: A Study with a National Representative Sample. Res. Dev. Disabil. 104, 103699. doi:10.1016/j.ridd.2020.103699
Elberling, H., Linneberg, A., Olsen, E. M., Goodman, R., and Skovgaard, A. M. (2010). The Prevalence of SDQ-Measured Mental Health Problems at Age 5-7 Years and Identification of Predictors from Birth to Preschool Age in a Danish Birth Cohort: the Copenhagen Child Cohort 2000. Eur. Child. Adolesc. Psychiatry 19 (9), 725–735. doi:10.1007/s00787-010-0110-z
Emck, C., Bosscher, R., Beek, P., and Doreleijers, T. (2009). Gross Motor Performance and Self-Perceived Motor Competence in Children with Emotional, Behavioural, and Pervasive Developmental Disorders: a Review. Dev. Med. Child. Neurol. 51 (7), 501–517. doi:10.1111/j.1469-8749.2009.03337.x
Faul, F., Erdfelder, E., Buchner, A., and Lang, A. G. (2009). Statistical Power Analyses Using G*Power 3.1: Tests for Correlation and Regression Analyses. Behav. Res. Methods 41 (4), 1149–1160. doi:10.3758/BRM.41.4.1149
Flouri, E., and Sarmadi, Z. (2016). Prosocial Behavior and Childhood Trajectories of Internalizing and Externalizing Problems: The Role of Neighborhood and School Contexts. Dev. Psychol. 52 (2), 253–258. doi:10.1037/dev0000076
Garcia, C. (1994). Gender Differences in Young Children's Interactions when Learning Fundamental Motor Skills. Res. Q. Exerc. Sport 65 (3), 213–225. doi:10.1080/02701367.1994.10607622
Goodman, A., and Goodman, R. (2009). Strengths and Difficulties Questionnaire as a Dimensional Measure of Child Mental Health. J. Am. Acad. Child. Adolesc. Psychiatry 48 (4), 400–403. doi:10.1097/CHI.0b013e3181985068
Goodman, R. (1994). A Modified Version of the Rutter Parent Questionnaire Including Extra Items on Children's Strengths: a Research Note. J. Child. Psychol. Psychiatry 35 (8), 1483–1494. doi:10.1111/j.1469-7610.1994.tb01289.x
Griffiths, A., Morgan, P., Anderson, P. J., Doyle, L. W., Lee, K. J., and Spittle, A. J. (2017). Predictive Value of the Movement Assessment Battery for Children - Second Edition at 4 years, for Motor Impairment at 8 years in Children Born Preterm. Dev. Med. Child. Neurol. 59 (5), 490–496. doi:10.1111/dmcn.13367
Harter, S., and Pike, R. (1984). The Pictorial Scale of Perceived Competence and Social Acceptance for Young Children. Child. Dev. 55 (6), 1969–1982. doi:10.2307/1129772
Henderson, S. E., Sugden, D. A., and Barnett, A. L. (2007). The Movement Assessment Battery for Children – 2. London: Pearson Education.
Hill, E. L. (2010). The Importance of Motor Skill in General Development. Dev. Med. Child. Neurol. 52 (10), 888. doi:10.1111/j.1469-8749.2010.03700.x
Hirata, S., Nakai, A., Okuzumi, H., Kitajima, Y., Hosobuchi, T., and Kokubun, M., (2015). Motor Skills and Social Impairments in Children with Autism Spectrum Disorders: A Pilot Study Using the Japanese Version of the Developmental Coordination Disorder Questionnaire (DCDQ-J). SAGE Open. doi:10.1177/2158244015602518
Hirata, S., Kita, Y., Yasunaga, M., Suzuki, K., Okumura, Y., Okuzumi, H., et al. (2018). Applicability of the Movement Assessment Battery for Children-Second Edition (MABC-2) for Japanese Children Aged 3-6 Years: A Preliminary Investigation Emphasizing Internal Consistency and Factorial Validity. Front. Psychol. 9. doi:10.3389/fpsyg.2018.01452
Hulme, C., and Snowling, M. (2009). Developmental Disorders of Language, Learning and Cognition. Chichester, England: Wiley-Blackwell.
Kadesjö, B., and Gillberg, C. (1999). Developmental Coordination Disorder in Swedish 7-Year-Old Children. J. Am. Acad. Child. Adolesc. Psychiatry 38 (7), 820–828. doi:10.1097/00004583-199907000-00011
Kremer, P., de Silva, A., Cleary, J., Santoro, G., Weston, K., Steele, E., et al. (2015). Normative Data for the Strengths and Difficulties Questionnaire for Young Children in Australia. J. Paediatr. Child. Health 51 (10), 970–975. doi:10.1111/jpc.12897
Mancini, V., Rigoli, D., Roberts, L., and Piek, J. (2019). Motor Skills and Internalizing Problems throughout Development: An Integrative Research Review and Update of the Environmental Stress Hypothesis Research. Res. Dev. Disabil. 84, 96–111. doi:10.1016/j.ridd.2018.07.003
Mancini, V. O., Rigoli, D., Roberts, L. D., Heritage, B., and Piek, J. P. (2018). The Relationship between Motor Skills and Psychosocial Factors in Young Children: A Test of the Elaborated Environmental Stress Hypothesis. Br. J. Educ. Psychol. 88 (3), 363–379. doi:10.1111/bjep.12187
Matsuishi, T., Nagano, M., Araki, Y., Tanaka, Y., Iwasaki, M., Yamashita, Y., et al. (2008). Scale Properties of the Japanese Version of the Strengths and Difficulties Questionnaire (SDQ): a Study of Infant and School Children in Community Samples. Brain Dev. 30 (6), 410–415. doi:10.1016/j.braindev.2007.12.003
Maurice-Stam, H., Haverman, L., Splinter, A., van Oers, H. A., Schepers, S. A., and Grootenhuis, M. A. (2018). Dutch Norms for the Strengths and Difficulties Questionnaire (SDQ) - Parent Form for Children Aged 2-18 years. Health Qual. Life Outcomes 16 (1), 123. doi:10.1186/s12955-018-0948-1
Moreno, J. A., González-Cutre, D., Martín-Albo, J., and Cervelló, E. (2010). Motivation and Performance in Physical Education: an Experimental Test. J. Sports Sci. Med. 9 (1), 79–85.
Nielsen, L. G., Rimvall, M. K., Clemmensen, L., Munkholm, A., Elberling, H., Olsen, E. M., et al. (2019). The Predictive Validity of the Strengths and Difficulties Questionnaire in Preschool Age to Identify Mental Disorders in Preadolescence. PLoS One 14 (6), e0217707. doi:10.1371/journal.pone.0217707
Pick, J. P., Bradbury, G. S., Elsley, S. C., and Tate, L. (2008). Motor Coordination and Social–Emotional Behaviour in Preschool-Aged Children. Int. J. Disabil. Development Education 55 (2), 143–151.
Piek, J. P., Rigoli, D., Pearsall-Jones, J. G., Martin, N. C., Hay, D. A., Bennett, K. S., et al. (2007). Depressive Symptomatology in Child and Adolescent Twins with Attention-Deficit Hyperactivity Disorder And/or Developmental Coordination Disorder. Twin Res. Hum. Genet. 10 (4), 587–596. doi:10.1375/twin.10.4.587
Rodriguez, M. C., Wade, T. J., Veldhuizen, S., Missiuna, C., Timmons, B., and Cairney, J. (2019). Emotional and Behavioral Problems in 4- and 5-year Old Children with and without Motor Delays. Front Pediatr. 7, 474. doi:10.3389/fped.2019.00474
Sargisson, R. J., Powell, C., Stanley, P., and de Candole, R. (2014). Predicting Motor Skills from Strengths and Difficulties Questionnaire Scores, Language Ability, and Other Features of New Zealand Children Entering Primary School. Aust. Educ. Developmental Psychol. 31 (1), 32–46. doi:10.1017/edp.2014.1
Schulz, J., Henderson, S. E., Sugden, D. A., and Barnett, A. L. (2011). Structural Validity of the Movement ABC-2 Test: Factor Structure Comparisons across Three Age Groups. Res. Dev. Disabil. 32, 1361–1369. doi:10.1016/j.ridd.2011.01.032
Skinner, R. A., and Piek, J. P. (2001). Psychosocial Implications of Poor Motor Coordination in Children and Adolescents. Hum. Mov Sci. 20 (1-2), 73–94. doi:10.1016/s0167-9457(01)00029-x
St Sauver, J. L., Barbaresi, W. J., Katusic, S. K., Colligan, R. C., Weaver, A. L., and Jacobsen, S. J. (2004). Early Life Risk Factors for Attention-Deficit/hyperactivity Disorder: A Population-Based Cohort Study. Mayo Clin. Proc. 79 (9), 1124–1131. doi:10.4065/79.9.1124
Keywords: preschool children, longitudinal study, motor ability, prediction, SDQ-difficulty
Citation: Hirata S, Kita Y, Suzuki K, Kitamura Y, Okuzumi H and Kokubun M (2021) Motor Ability and Mental Health of Young Children: A Longitudinal Study. Front. Educ. 6:725954. doi: 10.3389/feduc.2021.725954
Received: 16 June 2021; Accepted: 20 September 2021;
Published: 11 November 2021.
Edited by:
Robbert Smit, St.Gallen University of Teacher Education, SwitzerlandReviewed by:
Per A. Gustafsson, Linköping University, SwedenJohn Cairney, The University of Queensland, Australia
Sanja Tatalović Vorkapić, University of Rijeka, Croatia
Copyright © 2021 Hirata, Kita, Suzuki, Kitamura, Okuzumi and Kokubun. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shogo Hirata, r093002g@st.u-gakugei.ac.jp
†Present address: Shogo Hirata, Faculty of Education, Tokyo Gakugei University, Tokyo, Japan; Yosuke Kita, Mori Arinori Institute for Higher Education and Global Mobility, Hitotsubashi University, Tokyo, Japan and Cognitive Brain Research Unit (CBRU), Faculty of Medicine, University of Helsinki, Helsinki, FinlandKota Suzuki,Faculty of Education, Shitennoji University, Osaka, Japan;Yuzuki Kitamura,Department of Design, Graduate School of Design, Kyushu University, Fukuoka, Japan