Effects of rich cannabidiol oil on behavioral disturbances in patients with dementia: A placebo controlled randomized clinical trial
 Vered Hermush1,2*
Vered Hermush1,2*  Liora Ore3
Liora Ore3  Noa Stern1,2 Nisim Mizrahi1 Malki Fried1 Marina Krivoshey1 Ella Staghon1 Violeta E. Lederman4
Noa Stern1,2 Nisim Mizrahi1 Malki Fried1 Marina Krivoshey1 Ella Staghon1 Violeta E. Lederman4  Lihi Bar-Lev Schleider4,5
Lihi Bar-Lev Schleider4,5- 1Geriatric Wing, Laniado Hospital, Netanya, Israel
- 2Technion School of Medicine, Haifa, Israel
- 3Department of Graduate Studies in Health Systems Management, The Max Stern Yezreel Valley College, Jezreel Valley, Israel
- 4Research Department, Tikun-Olam Cannbit Pharmaceuticals, Tel Aviv, Israel
- 5Clinical Research Center, Soroka University Medical Center and Faculty of Health Sciences, Ben-Gurion University of the Negev, Be’er Sheva, Israel
Background: Almost 90% of patients with dementia suffer from some type of neurobehavioral symptom, and there are no approved medications to address these symptoms.
Objective: To evaluate the safety and efficacy of the medical cannabis oil “Avidekel” for the reduction of behavioral disturbances among patients with dementia.
Materials and methods: In this randomized, double-blind, single-cite, placebo-controlled trial conducted in Israel (ClinicalTrials.gov: NCT03328676), patients aged at least 60, with a diagnosis of major neurocognitive disorder and associated behavioral disturbances were randomized 2:1 to receive either “Avidekel,” a broad-spectrum cannabis oil (30% cannabidiol and 1% tetrahydrocannabinol: 295 mg and 12.5 mg per ml, respectively; n = 40) or a placebo oil (n = 20) three times a day for 16 weeks. The primary outcome was a decrease, as compared to baseline, of four or more points on the Cohen-Mansfield Agitation Inventory score by week 16.
Results: From 60 randomized patients [mean age, 79.4 years; 36 women (60.0%)], 52 (86.7%) completed the trial (all eight patients who discontinued treatment were from the investigational group). There was a statistically significant difference in the proportion of subjects who had a Cohen-Mansfield Agitation Inventory score reduction of ≥ 4 points at week 16: 24/40 (60.0%) and 6/20 (30.0%) for investigational and control groups, respectively (χ2 = 4.80, P = 0.03). There was a statistically significant difference in the proportion of subjects who had a Cohen-Mansfield Agitation Inventory score reduction of ≥ 8 points at week 16: 20/40 (50%) and 3/20 (15%), respectively (χ2 = 6.42, P = 0.011). The ANOVA repeated measures analysis demonstrated significantly more improvement in the investigational group compared to the control group at weeks 14 and 16 (F = 3.18, P = 0.02). Treatment was mostly safe, with no significant differences in the occurrence of adverse events between the two groups.
Conclusion: In this randomized controlled trial, ‘Avidekel’ oil significantly reduced agitation over placebo in patients suffering from behavioral disturbances related to dementia, with non-serious side-effects. Further research is required with a larger sample size.
Introduction
Dementia, characterized by a progressive decline in cognitive and functional abilities and challenging behavioral symptoms (1, 2), is one of the major causes of disability and dependency among older adults (3). Neuropsychiatric symptoms (NPS) occur in up to 90% of patients with dementia (4–6), and are associated with a reduced quality of life (7, 8). Symptoms contributing to decreased quality of life include agitation, mood disorders, hallucinations and delusions (psychosis), and sleep disorders (7, 9, 10). Agitation, a common NPS in dementia, is associated with an increased rate of cognitive and functional decline (11), rapid disease progression (12, 13), and an earlier death (14) compared to patients with dementia without agitation. In addition, patients with agitation are more likely to be admitted to institutions (15–18), and to require more antipsychotics and antidepressants (19), increasing the overall cost of care. Meta-analyses on the reasons patients with dementia are placed in nursing homes confirm the significant role of NPS symptoms that are ineffectively managed (20, 21).
In the absence of approved medications for NPS, antipsychotics are typically used off-label to treat agitation in dementia, although evidence for their efficacy is limited and usage may involve dangerous side-effects (22–26). A recent meta-analysis found an increased odds of cerebrovascular events, fracture, and death associated with antipsychotics; increased odds of falls associated with dextromethorphan-quinidine; and increased odds of death associated with anticonvulsants (22). Guidelines recommend the use of antipsychotics for the treatment of NPS in patients with dementia only when symptoms are dangerous or cause significant patient distress (22). Identifying an effective, low-risk therapeutic alternative for NPS, and specifically agitation, in patients with dementia is essential.
Cannabinoids work by interacting with receptors in the endocannabinoid system (ECS), especially cannabinoid 1 receptor (CB1R) and cannabinoid 2 receptor (CB2R). CB1Rs are extensively distributed throughout the body, with a significant presence in the central nervous system, whereas CB2Rs are found in immune cells and tissues (27). The ECS is an important neuromodulatory system linked to a variety of psychiatric, neurodegenerative, and motor illnesses, including schizophrenia, anorexia, Alzheimer’s disease, Parkinson’s disease, and Huntington disease (28, 29). Delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD) are the two most common cannabinoids found in the cannabis plant (30). CBD has anti-inflammatory, neuroprotective, antipsychotic, anxiolytic, and antidepressant properties (31). While THC is the primary psychoactive ingredient (32), CBD is non-intoxicating (30); and when combined with THC, may counterbalance the psychoactivity of THC (33). While each of the two main cannabinoids has been linked to clinical and physiological effects on its own, researchers have hypothesized that the main cannabinoid and minor cannabinoids operate synergistically (34). Several controlled studies suggest that CBD is safe and effective for the treatment of anxiety (35–38), Parkinson’s disease (37, 39), post-traumatic stress disorder (38), autism (40), epilepsy (41), and schizophrenia (42). Some clinical data supports the beneficial therapeutic effects of cannabinoids on behavioral symptoms, particularly on agitation in patients with dementia (43–45); however, reviews concluded that it is uncertain whether cannabinoids have any beneficial or harmful effects on behavioral disturbances related to dementia. All included studies tested THC and synthetic THC analogs; none of them examined the effect of CBD on agitation (46, 47). Although treatment with cannabinoids appears to be safe in patients with dementia (47), cancer (48), and older patients (49); overall evidence for the management of dementia-related NPS with medical cannabis has been equivocal (50). As CBD cannabis oils are becoming increasingly available, the need for further evaluation of CBD cannabis oils as a possible treatment option for agitation and identification of the treatment characteristics is increasing.
The primary objective of this trial was to evaluate the safety and efficacy of cannabis oil extracted from one chemovar “Avidekel” (30% CBD and 1% THC: 295 mg and 12.5 mg per ml, respectively), for behavioral disturbances in patients with dementia.
Materials and methods
Study design
This was a single-center, randomized (2:1), placebo-controlled, double-blind trial. Patients were recruited nationally by the principal investigator (VH). During enrollment, written informed consent was provided by the legal representatives of all participants, and an application for a cannabis treatment license was arranged (issuance took an average of seven weeks). Over 16 weeks of the treatment period, participants came in for follow-up every two weeks, with the option to terminate their participation. After completing the study, all trial participants were offered the option to renew their cannabis treatment license. The trial took place in a tertiary hospital in Israel from December 2017 to September 2019.
The trial, registered in ClinicalTrials.gov: NCT03328676, was approved by the Laniado Hospital Ethics Committee (project LND 0111-16) and the clinical trials department at the Israel Ministry of Health (project 20173138). Study procedures were conducted in accordance with the Declaration of Helsinki and the International Conference on Harmonization Consolidated Guidelines on Good Clinical Practice and followed the CONSORT reporting guideline (51).
Participants
During screening, participants were evaluated for eligibility criteria, which included an age of 60 years or older, diagnosis of a major neurocognitive disorder according to the DSM-5 criteria (all types of dementia), Mini–Mental State Examination (MMSE) (52) score of < 26 for cognitive impairment measurement, clinically relevant neuropsychiatric behaviors defined as Neuropsychiatric Inventory–Nursing Home Version (NPI-NH) (53–55) sub-score of agitation ≥ 3, a stable medication regimen for at least two weeks prior to baseline visit, and residence in either an institutionalized setting or in a non-institutionalized setting subject to 24-h supervision. Exclusion criteria included severe heart disease [New York Heart association (NYHA) class IV] (56), epilepsy, anxiety disorder; psychotic conditions in the present or in the past (not related to dementia), family history of schizophrenia, current substance use disorder, recent cannabis experience, or scheduled surgery during the trial.
Randomization
Eligible participants were randomly assigned by a computerized random-number generator system in a 2:1 ratio to receive either ‘Avidekel’ oil or a placebo. Patients with dementia are required to have consent of legal representatives in order to enroll in clinical trials. To encourage caregivers’ interest in enrollment of this trial, the 2:1 ratio was employed (57). The randomized list of patients was set before the trial was initiated, and the investigational product (IP) and placebo were prepared. Patients, families, and the medical teams were masked to the individual patients’ treatment assignment. To ensure masking was maintained, “Avidekel” and placebo oils were manufactured to have an identical appearance and smell.
Investigational product
The IP or placebo was added to the routine medication regimen (Table 1). Subjects received the IP or the placebo as drops applied under the tongue three times a day. Participants in the investigational group received “Avidekel” (made in Israel by Tikun-Olam Cannbit Pharmaceuticals), an ethanol extraction of rich CBD (∼15%), low-THC (∼0.5%) cannabis chemovar dissolved in olive oil. The IP contained 30% CBD, 1% THC, 1% Cannabichromene (CBC), 0.5% Cannabigerol (CBG), and 0.5% Cannabidivarin (CBDV). One drop of 0.04 ml contains 11.8 mg CBD and 0.5 mg THC. Patients in the control group received a placebo containing olive oil and chlorophyll.
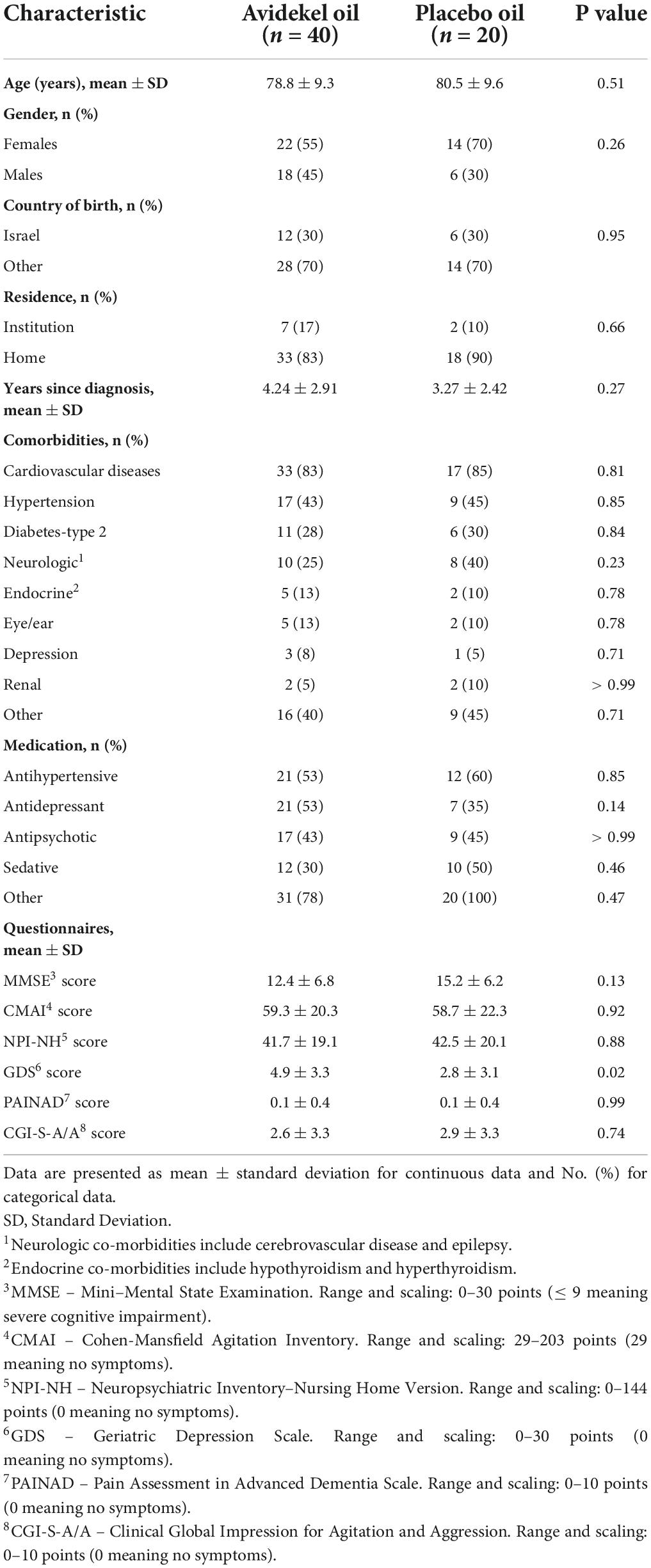
Table 1. Characteristics of the patient population at baseline.
Caregivers were instructed to shake the oil bottle, place the drops of oil with a tablespoon under the patient’s tongue, and wait one minute before swallowing to enhance oil absorption. The initial dose was one oil drop in the morning, afternoon, and evening, for two days. They were instructed to increase each dose by one drop in increments of two days. The dose was titrated gradually depending on the tolerance of each patient, to a maximum dose of 21 drops per administration or until an adverse reaction occurred. The caregivers were instructed to then taper down one level to a pre-adverse reaction dose. The time for each patient to “find” the therapeutic dose: a balance between maximum reduction in agitation and minimum side-effects, lasted up to six weeks. After the titration phase, patients entered a ten-week treatment phase of fixed-dose (Supplementary Table 1).
We selected this specific chemovar “Avidekel” aiming to minimize side-effects. This was based on earlier clinical experience with 39 patients with indications for dementia and on 93 patients with pediatric autism spectrum disorder with behavioral disturbances (58). In both cases, patients receiving this product showed improvement in agitation with low-frequency side-effects. This type of sublingual administration (59) is more accurate with fewer fluctuations than other routes of administration. A similar product was tested for pharmacokinetics parameters in Crohn’s disease patients and demonstrated blood concentrations of the main active ingredients and their metabolites (60).
Safety assessments
For safety evaluation, serious adverse events (SAEs; defined as: death, life-threatening events, hospitalization, debilitation, or immobility), and all adverse events (AEs), with a severity score on a Likert scale of 1 to 10, were collected in all trial visits. In this population with many comorbidities and medications, the symptom list of main AEs was also evaluated at baseline and documented as a non-IP-related AE report. An AE was defined as any unfavorable symptom, sign, syndrome, or disease that occurred during the study, having been absent at baseline, or, if present at baseline, appeared to worsen. Clinical data included vital signs and physical examination information collected in all trial visits, as well as blood chemistry and hematology labs collected every other visit.
Outcomes measures
The primary efficacy endpoint was the proportion of subjects achieving a 4-point decrease in the Cohen-Mansfield Agitation Inventory (CMAI) at week 16 compared to baseline (61–65). A total CMAI score was obtained by summing all items from a caregivers’ rating questionnaire consisting of 29 agitated behaviors, each rated on a 7-point scale of frequency, with higher scores indicating greater severity. A total score of > 45 was regarded as clinically significant agitation, and a total reduction of 8 points or more was considered a clinically significant change (65). We determined that a 4-point decrease in CMAI score represents a better outcome compared to a similar randomized controlled trial that used oral THC (in which a 2.3 points reduction in the active group was not significant) (66), and above the placebo effect of two points decrease in the CMAI (67).
Secondary outcomes included: The proportion of subjects achieving an 8-point decrease in mean CMAI score, proportion of patients achieving 30% and 50% reduction in CMAI scores, the time necessary to achieve a 4-point reduction in CMAI, mean change in NPI-NH agitation/aggression sub-score. In the NPI-NH, the higher the score, the more severe and frequent the behavioral disturbances. The following questionnaires were also administered: the Geriatric Depression Scale (GDS), the Pain Assessment in Advanced Dementia Scale (PAINAD), the Clinical Global Impression for Agitation and Aggression (CGI-S-A/A), and the MMSE.
At each visit, a geriatrician and a trained occupational therapist examined the patients. All study questionnaires were administered and completed on paper by the trained staff and answered by the patient’s main caregiver (a family member or a hired caregiver) on every visit and recorded to an electronic Case Report Form.
Statistical analysis
Sample size was calculated using the Power and Precision version 4 software (68), for a power of 80% and for two-sided α level of 0.05 to detect a difference in the proportion of successful reduction in CMAI scores between the investigational group compared to control at week 16. Success was defined as at least a 4-point reduction. For an expected difference of 35% in the proportion of success between the groups, an unbalanced sample of 42 and 22 was selected for the investigational and placebo group, respectively. Thus, 64 patients were randomly assigned to the investigational or control group (4 patients withdrew immediately after randomization, leaving 60 patients who started treatment to be included in the analysis). A 35% difference in proportion between the two groups was selected based on findings from an un-published report on the IP that was used to treat 14 patients with dementia-related behavioral disturbances.
The efficacy analyses were performed according to the intention-to-treat (ITT) principle, in order to provide unbiased comparisons among groups. The ITT analysis was done in all patients randomized and receiving treatment, with missing data imputation for patients who did not complete the trial (using last-observation-carried-forward method). We further performed a per protocol (PP) analysis (for 52 patients) as a sensitivity analysis, in which only patients who completed the trial according to protocol and had data available from all time points were counted toward the results. The primary outcome, CMAI reduction of >8 points and proportion of patients achieving 30% and 50% reduction in CMAI scores, were analyzed with the chi-square test including Yates’ corrected chi-square (continuity correction).
The baseline CMAI distribution was tested for normality using the Kolmogorov-Smirnoff test. The Mauchly’s Test of Sphericity was used to test whether the variances of the differences were equal. Baseline characteristics between groups are presented as means and standard deviations for continuous variables and as frequencies and percentages for categorical variables. Chi-square tests and independent t-tests were performed to compare groups for categorical and continuous baseline variables, respectively.
The GLM (general linear models) ANOVA Repeated Measures procedure was used to provide an analysis of variance for repeated CMAI measurements for nine visits on each subject. The analyses involve one within factor (time) and one between factor (groups). Changes over time and differences within groups were calculated (time*group), including contrasts tests to test differences among factor levels (1 factor, 9 levels), with a total significant level of 5%. Mauchly’s Test of Sphericity indicated that the assumption of sphericity had been violated [χ2(35) = 353.4, P < 0.001 for ITT and χ2(35) = 299.4, P < 0.001 for PP], meaning the F-statistic is positively biased rendering it invalid and increasing the risk of Type I error. To overcome this problem, we corrected the degrees of freedom using the Greenhouse-Geisser correction to obtain a valid critical F-value. The contrast was compared by method: difference, each level was compared to baseline. Analyses were performed on two full data sets (without missing data), the ITT set (n = 60) and the PP set (n = 52). In addition, the GLM test was performed again with a post hoc analysis based on the MMSE score to compare the change in CMAI in patients with higher or lower score than the median MMSE score.
Kaplan Meier survival analysis was performed to compute the time to achieve a CMAI ≥ 4-point reduction (success) for each group and the group difference was tested using the log rank chi-square test. Comparison of CMAI mean score between the two groups was analyzed by the independent t-test.
Comparison between groups in NPI-NH frequencies of all sub-categories (as dichotomous variables: yes/no) were analyzed by the Fisher’s exact test for baseline and end of study. NPI-NH factors scores, total NPI-NH, and all other variables were tested by independent t-test. Frequency of AEs and medications consumption between the two groups was compared by using the Fisher’s exact test.
Data were analyzed with IBM SPSS statistics software version 27.0 (SPSS Inc. Headquarters, Illinois, United States). Significance levels were set at 0.05.
Results
Of 67 patients screened for a possible enrollment, three patients were not eligible and four opted not to participate in the trial. Among the 60 randomized patients initiating treatment, the mean age was 79.4 ± 9.4 years; 36 (60.0%) were female and 52 (86.7%) completed 16 weeks of trial (Figure 1).
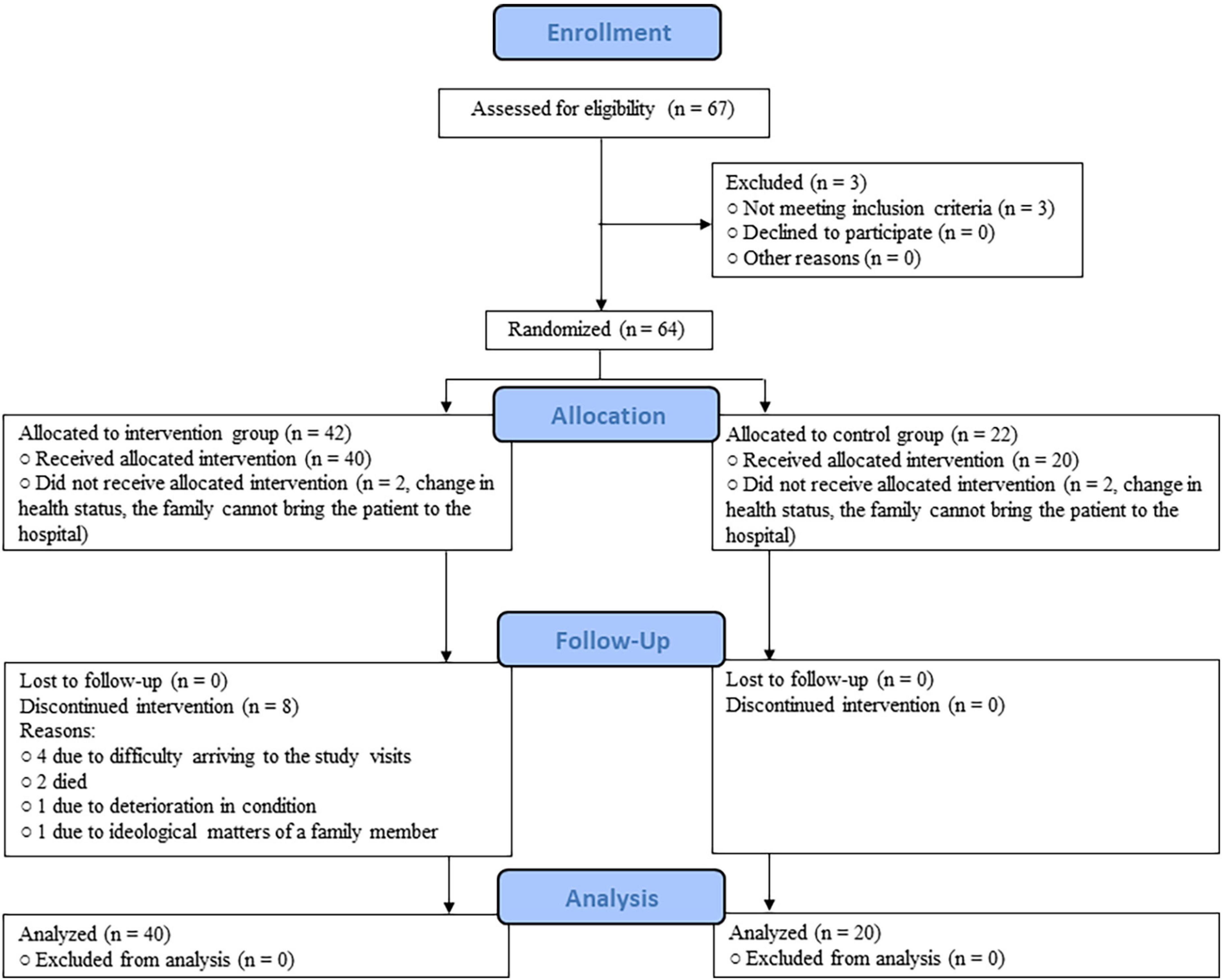
Figure 1. CONSORT diagram.
Upon enrollment, no meaningful differences were found. At baseline, all recruited patients presented MMSE scores of ≤ 25 (Table 1). In the repeated measures analysis, there was no difference in MMSE change from baseline to week 16 between the two groups (F = 1.58, P = 0.21). Overall, 32 of 40 participants in the investigational group (80.0%) and all participants in the control group completed the 16-week treatment. Two patients died of non-product-related causes. For the remaining six patients, attrition seemed due to personal and caregiver difficulties. AEs were not reported as a reason to leave the trial. At baseline, there were no statistically significant differences between completers and those who did not completed the trial.
Participants in the active and control groups consumed on average 14.9 and 17.9 drops per administration, respectively (44.7 and 53.7 drops per day, respectively) (Supplementary Figure 1). Mean CBD and THC consumption per administration was 175.8 mg and 7.4 mg, respectively (527.5 mg and 22.3 mg per day, respectively) (Supplementary Figure 2). Dose was not correlated with age (r = –0.17, P = 0.28) or with the outcome, both the change in CMAI (r = –0.23, P = 0.21), and the reductions of ≥ 4 point (t = 0.21, P = 0.83).
Primary outcome
The primary endpoint of the trial was the proportion of subjects achieving a CMAI ≥ 4-point decrease during the treatment period. For the ITT set, the proportions observed were 24/40 (60.0%) and 6/20 (30.0%) for investigational and control groups, respectively (χ2 = 4.80, P = 0.03; with continuity correction χ2 = 3.67, P = 0.06). For the PP set (52 completers), the proportions observed were 22/32 (68.7%) and 6/20 (30.0%) for investigational and control groups, respectively (χ2 = 7.44, P = 0.006; with continuity correction χ2 = 5.96, P = 0.01).
Secondary outcomes
The main hypothesis that the consumption of the IP will reduce behavioral disturbances and restlessness in older patients with dementia was tested by the CMAI reduction over time between groups (Figure 2). The CMAI baseline measures were slightly skewed, but we were unable to observe a significant skewed distribution when splitting into groups (Kolmogorov-Smirnoff P > 0.05). We compared the CMAI reduction from baseline to week 16 in both ITT and PP sets. Both demonstrate a significantly greater reduction in the investigational group, compared to the control group. In the ITT set, the reduction in CMAI scores at week 16 was of 10.7 ± 15.2 and 2.5 ± 9.4 points (t = –2.20, P = 0.03) for the investigational and control group, respectively. In the PP set, the reduction was of 13.3 ± 15.3 and 2.5 ± 9.4 (t = –2.85, P = 0.006) for the investigational and control group, respectively. The average CMAI score in the last visit for the investigational group was 44.03 ± 13.21. The CMAI aggressive behavior sub-score also showed significantly greater improvement in the investigational group compared to the control group (t = 1.30, P = 0.02 for the PP set). There was a statistically significant difference in the proportion of subjects who had a CMAI score reduction of ≥ 8 points at week 16: 20/40 (50%) and 3/20 (15%), respectively (χ2 = 6.425, P = 0.011). To test the reduction of CMAI over time, we used two full data sets: an ITT set and a PP set of completers. The GLM ANOVA repeated measures over time of CMAI scores for the ITT data demonstrate a significant decrease over time in the multivariate test for both groups (within-subject effect F = 4.74, P = 0.001). Analysis demonstrated a significantly greater improvement in the investigational group compared to the control group, for tests of week 14 (F = 6.13, P = 0.01) and week 16 (F = 7.07, P = 0.01) compared to baseline. The same analysis for the PP data demonstrates a significant decrease over time (F = 6.45, P < 0.001) and with different reduction trends between the two groups (F = 3.18, P = 0.02). Results present a wide confidence interval; however, tests of difference between groups at week 14 (F = 4.83, P = 0.03) and at week 16 (F = 4.84, P = 0.03) were significantly different.
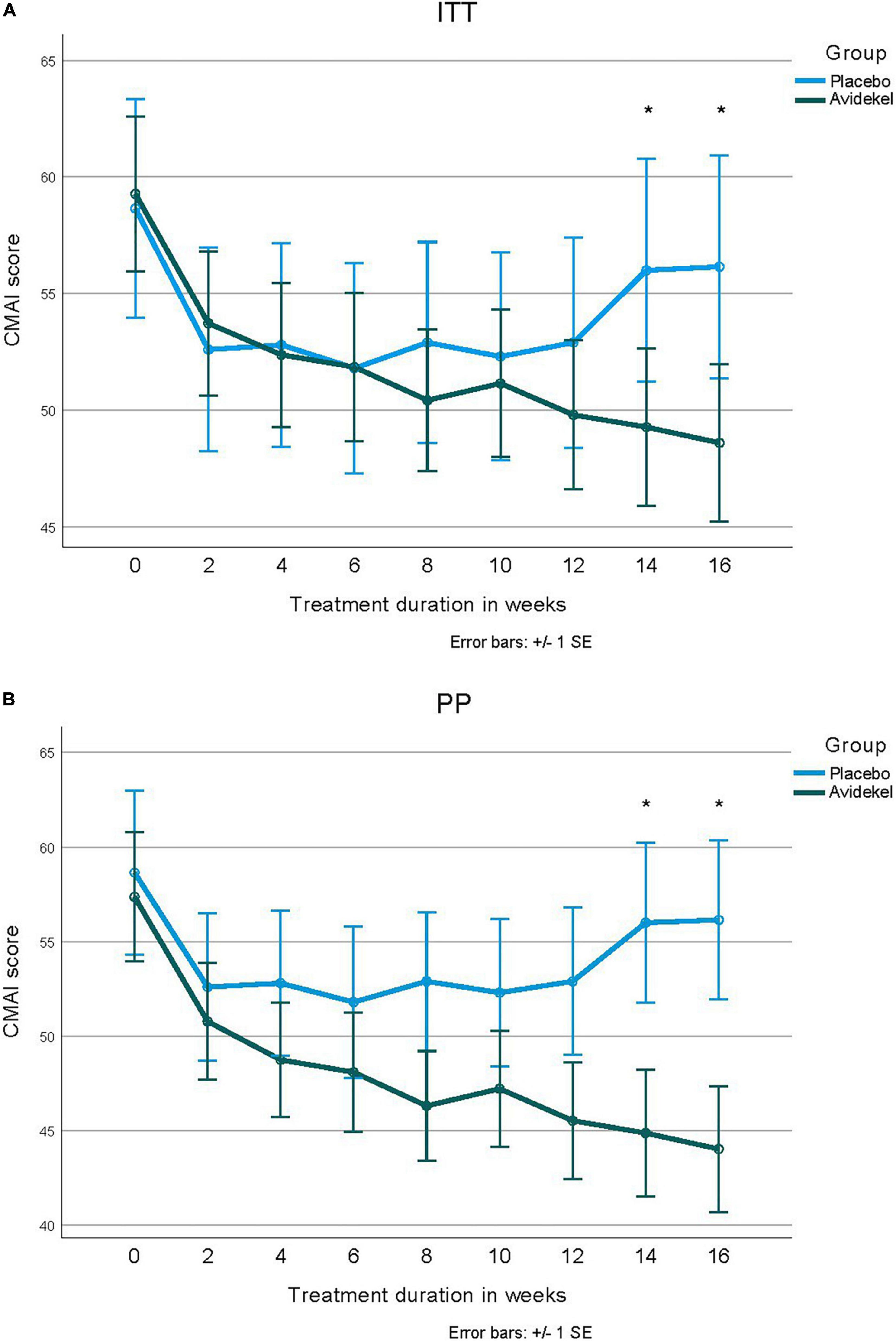
Figure 2. The Cohen-Mansfield Agitation Inventory score reduction over time between groups. Panels (A,B) present mean CMAI scores in the two groups, throughout the trial visits both in intention-to-treat analysis of all randomized patients that initiated treatment (n = 60), and per protocol analysis of patients who completed the trial according to protocol (n = 52). (A) Intention-to-treat analysis. (B) Per-protocol analysis.
We tested whether patients with lower MMSE scores (14 and below) were different from patients with MMSE scores of 15 or higher in the CMAI change through time. We could not find a significant difference in either the entire group (F = 1.73, P = 0.12) or within the interventional group alone (F = 1.23, P = 0.33). For patients in the investigational group who achieved a ≥ 4-point decrease in CMAI (60.0%), it took a mean of 8.8 weeks (95% CI: 6.7–11.1 weeks), whereas patients who received the placebo and achieved a ≥ 4-point decrease in CMAI (30.0%) took 12.9 weeks (95% CI: 10.2–15.6). This difference was significant (log rank χ2 = 5.19, P = 0.02).
Table 2 demonstrates the differences between groups in clinical parameter scores for completers at baseline and at the end of the trial. NPI-NH results demonstrate a significant reduction (29.4%) in agitation/aggression (χ2 = 5.98, P = 0.01) and a significant reduction (22.5%) in sleep disturbances (χ2 = 5.19, P = 0.03) in the investigational group compared to the control group, as well as a significant difference in the mean NPI-NH Agitation/Aggression factor score at week 16 (t = 2.01, P = 0.03). Chang was from 12.1 ± 5.8 to 6.7 ± 6.9 in the investigational group, and from 15.5 ± 7.8 to 11.4 ± 8.7 in the control group. There was no statistically significant difference in the GDS, PAINAD, CGI-S-A/A or MMSE questionnaires. An improvement of < 30% in CMAI total score was achieved by 24.3% of patients in the investigational group, and 10% in the control group (χ2 = 0.94, P = 0.30). Similarly, an improvement of < 50% in CMAI total score was achieved by 8% of patients in the investigational group and 0% in the control group (χ2 = 0.24, P = 0.54). The most improved behaviors of the CMAI questionnaire that improved in all patients in the investigational group included making physical sexual advances, throwing things, spitting, hurting themselves or others, tearing things or destroying property, intentional falling, eating/drinking inappropriate substances, and making verbal sexual advances.
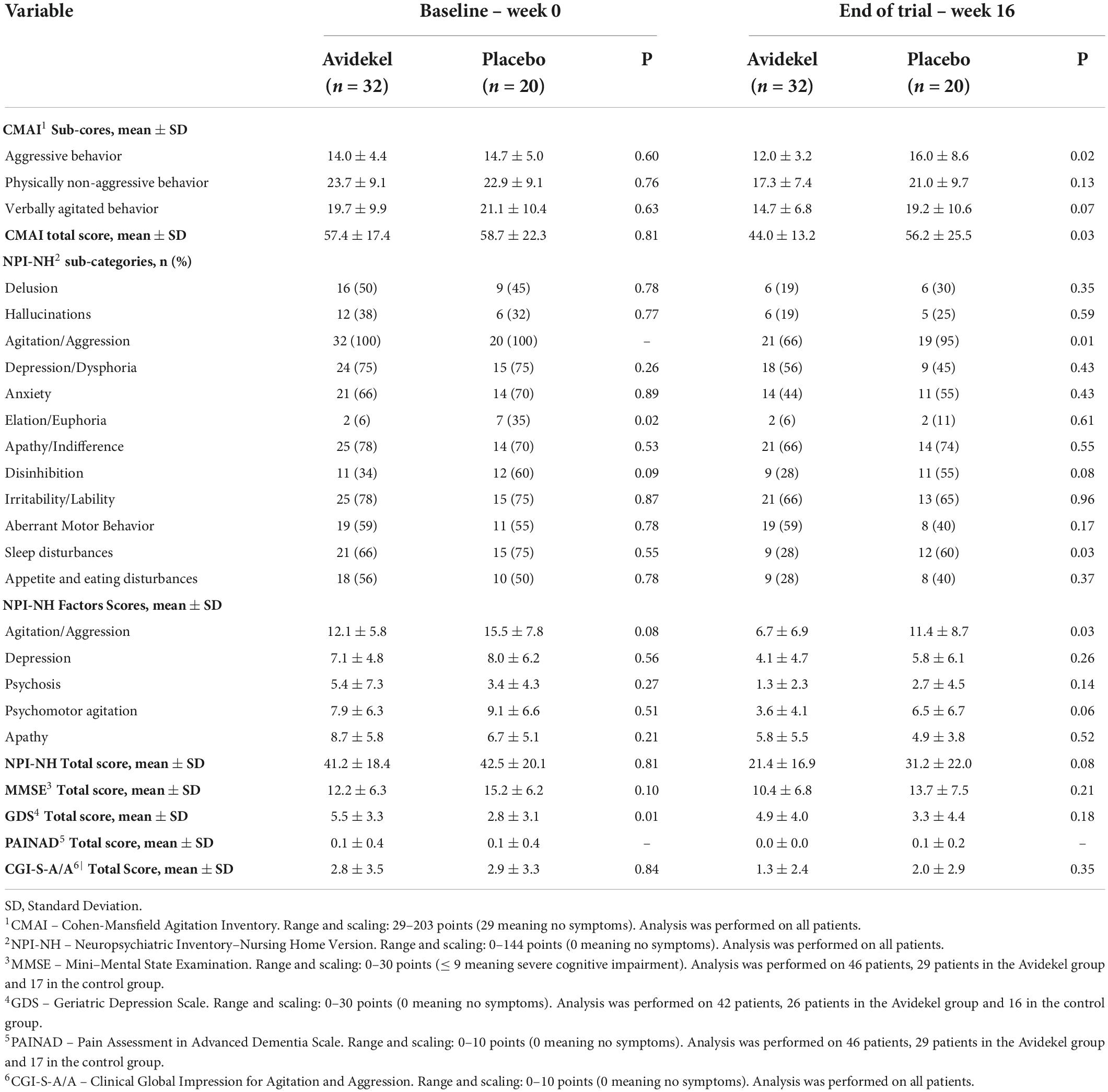
Table 2. Effects on neuropsychiatric signs and symptoms for completers, at baseline and end of trial.
There was no statistically significant difference in medications used between groups and over time, demonstrating stable medication consumption throughout the trial in both groups (Supplementary Table 2).
Adverse events
All withdrawals occurred in the investigational group. The reported reasons for withdrawals were: four patients discontinued treatment due to difficulty commuting to the study appointments (one patient completed baseline visit, two patients completed 2 weeks, and one completed 4 weeks); one patient left after 4 weeks due to the ideological concerns of her son; one patient withdrew after the baseline visit due to a deterioration in his condition (dialysis patient).
Thirteen SAEs included two deaths and eleven hospitalizations (Table 3). There were no significant differences in the occurrence of SAEs (9 and 4 in the investigational and control groups, respectively). The two deaths were in the investigational group. The first patient, 94 years old, suffering from colonic cancer and chronic renal failure, died from septic shock after completion of 4 weeks in the study. The second patient, 87 years old, experienced recurrent hospitalizations due to severe hyponatremia and anemia, for which he was recurrently intubated, and died from breathing difficulties (only baseline results were recorded). There was no statistically significant difference in the death rate between the two groups (active group 6.25% versus placebo group 0.0%, χ2 = 1.28, P = 0.52). We did not see a direct link between the SAEs and the IP.
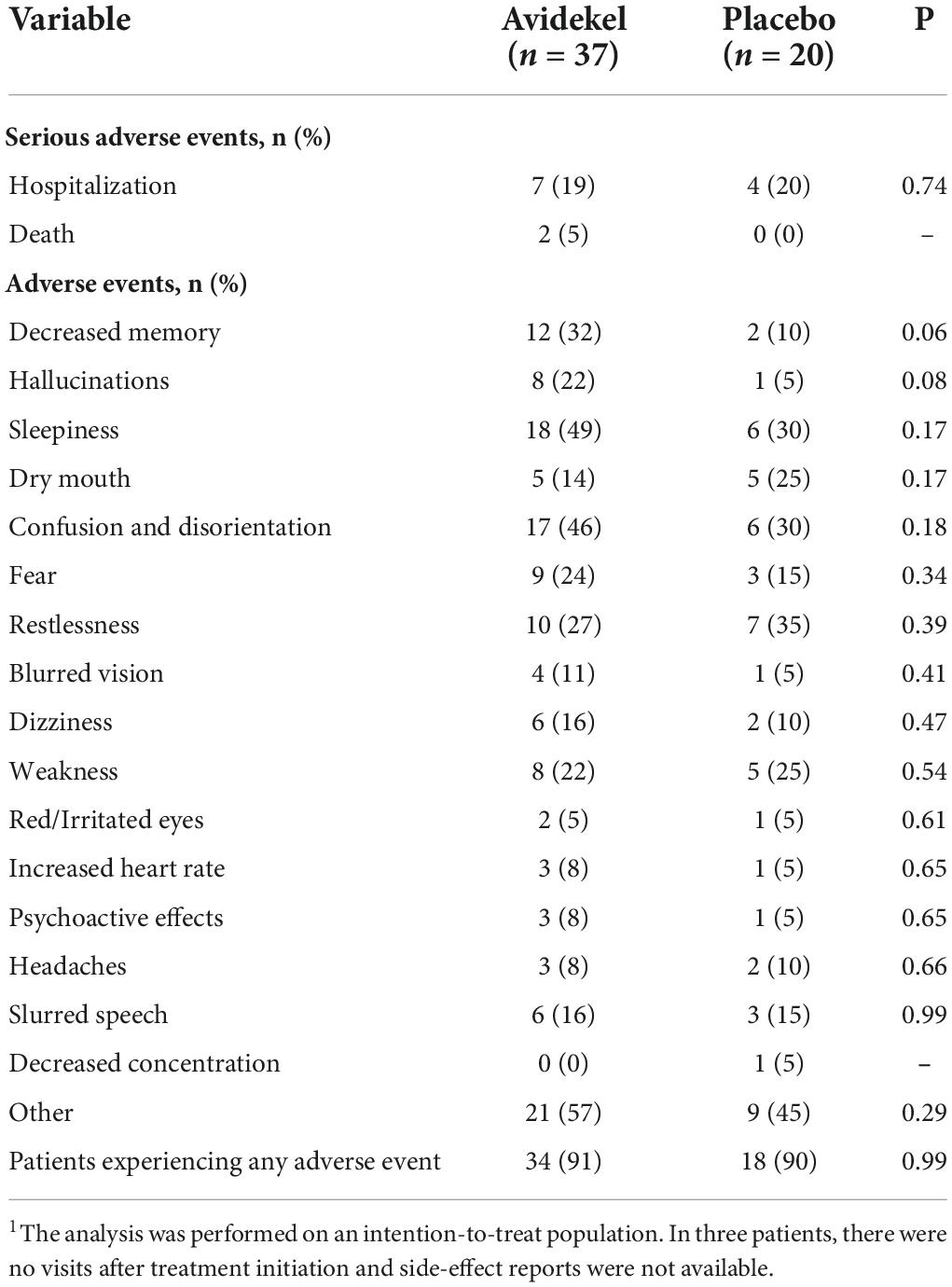
Table 3. Patients experiencing adverse events1.
Sleepiness (48.6%), confusion and disorientation (45.9%), and decreased memory (32.4%) were the most frequent complaints among participants in the investigational group. No significant differences were observed in the occurrence of AEs between groups (Table 3). However, in the investigational group there were notably higher rates of decreased memory (χ2 = 3.52, P = 0.06), hallucinations (χ2 = 2.72, P = 0.08), sleepiness (χ2 = 1.85, P = 0.17), and confusion and disorientation (χ2 = 1.42, P = 0.18). No change in pulse or blood pressure were observed throughout the study.
Discussion
In this randomized placebo-controlled trial, we aimed to test the hypothesis that broad-spectrum rich CBD medical cannabis oil differs from a placebo in alleviating behavioral disturbances in patients with dementia. Patients in the investigational group experienced a significantly greater reduction in sleep disturbances, and in agitation and aggression sub-score using two different measurement tools. The improvements were accompanied with non-serious side-effects.
Agitation CMAI scores decreased significantly in the investigational group over the course of treatment. Over the years, CBD has been suggested to have a positive clinical effect in patients suffering from neurological conditions. It has been found to be effective in reducing anxiety (69), Parkinson’s disease related symptoms (39), disruptive behavior, and other autism related symptoms (40). CBD has been also found to be effective as an anticonvulsant (41). There are no studies describing the effect of CBD on behavioral disturbances in dementia patients. Existing studies only tested THC and its analogs. In our study, 31% of patients in the investigational group reached the maximum dose allowed of 10.5 mg THC and another 15.6% reached 10 mg THC per administration; therefore, a direct effect of THC contributing to the decrease of behavioral disturbances cannot be ruled out. On the other hand, controlled studies with THC administration as a single active compound for the management of behavioral disturbances in dementia patients showed no significant decrease (66, 70, 71). Some pre-clinical studies demonstrated that the compounds in Avidekel work synergistically and that the combination of active ingredients in the IP is responsible for the observed effect. If this is the case, administering one component as an isolated material would not reproduce the same effect (72, 73). The difference in the average CMAI scores between groups only became significant at week 14, highlighting the importance of patience in the first few months of treatment based mainly on CBD.
In one study on the effects of antipsychotic drugs (74) on behavioral disturbances in dementia, the primary end point proportions in the antipsychotic group compared to the control resemble the numbers we received. In some other antipsychotics studies using the CMAI tool (75–77), results were different, and they did not find significant improvement in agitation compared to placebo. There was an improvement in behavioral symptoms in 30% of patients in the control group. This improvement may be explained by the placebo effect and by the non-specific benefit of being enrolled in a trial (78), with thorough bi-weekly medical monitoring. In the NPI-NH, the results of our study demonstrate a significant reduction in agitation/aggression total scores and are close to the NPI-NH total scores obtained in the investigational and control groups from other antipsychotic drugs studies (74). Further investigation is required to explore rich CBD cannabis oil as a treatment option for agitation in patients with dementia, especially because the average CMAI score in the Avidekel group at 16 weeks was below the definition of clinically significant agitation.
Although the etiology of dementia-related agitation involves psychological and social components, it is often predominantly characterized by anatomical and neurochemical changes in the brain (79). In a review on the pharmacological treatment addressing the etiology of dementia-related agitation and aggression, pharmacological modulation of specific molecular targets was suggested as management options (80). Some of the proposed molecular targets are affected by CBD, which acts on more than 65 targets [for a review, see (81–83)]. The mechanisms of action underlying the direct and indirect effects of CBD on agitation involve the regulation of the serotonin 1A receptor, CB1Rs, the hypothalamic-pituitary-adrenal axis, anandamide, CB2Rs, and GABAA receptors (81, 82, 84). Animal models showed that chronic administration of CBD led to a reduction in inflammation and increased clearance of amyloid beta (85), while also reducing anxiety, depression, and stress-related behaviors (86).
Sleep disturbances in the NPI-NH were significantly lower in the investigational group at week 16 compared to baseline. This finding is in line with the published literature demonstrating the positive effect of THC on sleep, in the context of different medical indications, both in controlled (87–89) and uncontrolled studies (45, 90–92). Similar results were found in controlled studies on a combination of THC and CBD (93–95). As for the effect of CBD on sleep, one study showed that CBD does not impair sleep (96), and several uncontrolled studies have shown that CBD improves sleep (69, 97). In this study, 49% of the investigational group reported drowsiness as a side-effect. The improvement in behavioral disturbances along with the reduction in sleep disturbances raises concerns regarding the anesthetizing characteristics of the IP. However, IP consumption does not appear to be related to increased apathy, as there were no differences between groups in NPI-NH apathy scores.
The treatment appears to be relatively safe. Common adverse events included sleepiness, confusion and disorientation, restlessness, fear, weakness, and hallucinations, among others. The safety profile of CBD cannabis oil appeared to be high in other studies as well (98, 99), including in pediatric populations (100–102). Although not statistically significant, the higher rates of decreased memory, sleepiness, and hallucinations in the investigational group should be further explored. It may indicate that the dose of 10 mg THC per administration for patients with dementia may be too high, even when combined with an increased presence of CBD. The occurrence of reported AEs in patients who discontinued treatment were not different from the rest of the cohort. Although we did not find a link between the IP and the study discontinuation, we cannot exclude the possibility that the IP might have a tolerability barrier.
Limitations
Our trial has several limitations. All eight patients who discontinued the treatment belonged to the investigational group and the sample size of 60 participants for our main outcome in an ITT analysis has a power of only 60%. The small number of participants, recruited in a single medical center, with no comparison between sub-types of dementia (Alzheimer’s disease, Lewy body and vascular dementia), made the study group highly heterogenous, providing limited ability to define the safety profile of the IP. However, heterogeneity, specifically in dementia patients, increases the importance of the results. Outcome measures did not include measures that would rule out functional impairment following treatment with a product containing THC, and pharmacokinetic indices of the IP were not collected in this trial. Although the GDS questionnaire has been shown to retain acceptable qualities when applied to older patients with dementia, it is a less sensitive questionnaire compared to the Cornell Scale for Depression in Dementia (103). Due to the limited availability of “Avidekel” in most countries, there is a lack in necessary research required to compare chemovars and to identify which specific compounds in “Avidekel” resulted in the superior effect “Avidekel” has shown over other chemovars in the clinic, with similar concentrations of THC and CBD. Subsequent research should also aim to identify new efficacious chemovars.
Conclusion
Our findings suggest that rich-CBD cannabis oil may alleviate agitation in older patients with dementia. One trial is not enough to make conclusions on the safety and efficacy of broad-spectrum CBD. We recommend conducting a large scale randomized controlled trial on behavioral disturbances related to dementia and to compare clinical sub-types of dementia.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the principal investigator, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Laniado Hospital Ethics Committee (project LND 0111-16) and the Clinical Trials Department at the Israel Ministry of Health (project 20173138). The patients/participants provided their written informed consent to participate in this study.
Author contributions
VH and LB-L conceived the study, wrote the protocol, and drafted the manuscript. VH was the guarantor. All authors acquired, analyzed, or interpreted the data, and critically revised the manuscript for important intellectual content.
Funding
This study was funded by TO Pharmaceuticals LLC., which had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Acknowledgments
We thank Victor Novack, MD, Ph.D., Ben-Gurion University of the Negev, for his insightful suggestions that improved the manuscript without compensation for his contributions. We also thank Nira Koren, Ph.D., Tel Aviv University, for conducting the statistical analyses; she was compensated for her contribution.
Conflict of interest
LB-L and VL report employment at Tikun-Olam Cannbit Pharmaceuticals Ltd., with stock options in the company. LB-L reports consulting role with TO Pharmaceuticals LLC. As a consultant of the company, LB-L was registered as an inventor on a patent on the investigational product for behavioral disturbance in patients with dementia.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.951889/full#supplementary-material
References
1. Grand JH, Caspar S, Macdonald SW. Clinical features and multidisciplinary approaches to dementia care. J Multidiscip Healthc. (2011) 4:125–47. doi: 10.2147/JMDH.S17773
2. Chertkow H, Feldman HH, Jacova C, Massoud F. Definitions of dementia and predementia states in Alzheimer’s disease and vascular cognitive impairment: consensus from the Canadian conference on diagnosis of dementia. Alzheimers Res Ther. (2013) 5:S2. doi: 10.1186/Alzrt198
4. Alzheimer’s Association. 2017 Alzheimer’s disease facts and figures. Alzheimers Dement. (2017) 13:325–73. doi: 10.1016/j.jalz.2017.02.001
5. Cerejeira J, Lagarto L, Mukaetova-Ladinska EB. Behavioral and psychological symptoms of dementia. Front Neurol. (2012) 3:73. doi: 10.3389/fneur.2012.00073
6. Muller-Spahn F. Behavioral disturbances in dementia. Dialogues Clin Neurosci. (2003) 5:49–59. doi: 10.31887/DCNS.2003.5.1/fmuellerspahn
7. Desai AK, Grossberg GT. Recognition and management of behavioral disturbances in dementia. Prim Care Companion J Clin Psychiatry. (2001) 3:93–109. doi: 10.4088/pcc.v03n0301
8. Banerjee S, Smith S, Lamping D, Harwood R, Foley B, Smith P, et al. Quality of life in dementia: more than just cognition. An analysis of associations with quality of life in dementia. J Neurol Neurosurg Psychiatry. (2006) 77:146–8. doi: 10.1136/jnnp.2005.072983
9. O’Donnell BF, Drachman DA, Barnes HJ, Peterson KE, Swearer JM, Lew RA. Incontinence and troublesome behaviors predict institutionalization in dementia. J Geriatr Psychiatry Neurol. (1992) 5:45–52. doi: 10.1177/002383099200500108
10. Scarmeas N, Brandt J, Albert M, Hadjigeorgiou G, Papadimitriou A, Dubois B, et al. Delusions and hallucinations are associated with worse outcome in Alzheimer disease. Arch Neurol. (2005) 62:1601–8. doi: 10.1001/archneur.62.10.1601
11. Scarmeas N, Brandt J, Blacker D, Albert M, Hadjigeorgiou G, Dubois B, et al. Disruptive behavior as a predictor in Alzheimer disease. Arch Neurol. (2007) 64:1755–61. doi: 10.1001/archneur.64.12.1755
12. Peters ME, Schwartz S, Han D, Rabins PV, Steinberg M, Tschanz JT, et al. Neuropsychiatric symptoms as predictors of progression to severe Alzheimer’s dementia and death: the Cache County dementia progression study. Am J Psychiatry. (2015) 172:460–5. doi: 10.1176/appi.ajp.2014.14040480
13. Wilcock GK, Ballard CG, Cooper JA, Loft H. Memantine for agitation/aggression and psychosis in moderately severe to severe Alzheimer’s disease: a pooled analysis of 3 studies. J Clin Psychiatry. (2008) 69:341–8. doi: 10.4088/jcp.v69n0302
14. Bränsvik V, Granvik E, Minthon L, Nordström P, Nägga K. Mortality in patients with behavioural and psychological symptoms of dementia: a registry-based study. Aging Ment Health. (2021) 25:1101–9. doi: 10.1080/13607863.2020.1727848
15. Deutsch LH, Bylsma FW, Rovner BW, Steele C, Folstein MF. Psychosis and physical aggression in probable Alzheimer’s disease. Am J Psychiatry. (1991) 148:1159–63. doi: 10.1176/ajp.148.9.1159
16. Herrmann N, Lanctôt KL, Naranjo CA. Behavioural disorders in demented elderly patients. CNS Drugs. (1996) 6:280–300. doi: 10.2165/00023210-199606040-00004
17. Miller EA, Rosenheck RA. Risk of nursing home admission in association with mental illness nationally in the Department of Veterans Affairs. Med Care. (2006) 44:343–51. doi: 10.1097/01.mlr.0000204008.83633.ed
18. Miller EA, Weissert WG. Predicting elderly people’s risk for nursing home placement, hospitalization, functional impairment, and mortality: a synthesis. Med Care Res Rev. (2000) 57:259–97. doi: 10.1177/107755870005700301
19. Aigbogun MS, Stellhorn R, Hartry A, Baker RA, Fillit H. Treatment patterns and burden of behavioral disturbances in patients with dementia in the United States: a claims database analysis. BMC Neurol. (2019) 19:33. doi: 10.1186/s12883-019-1260-3
20. Toot S, Swinson T, Devine M, Challis D, Orrell M. Causes of nursing home placement for older people with dementia: a systematic review and meta-analysis. Int Psychogeriatr. (2017) 29:195–208. doi: 10.1017/S1041610216001654
21. Andren S, Elmstahl S. Effective psychosocial intervention for family caregivers lengthens time elapsed before nursing home placement of individuals with dementia: a five-year follow-up study. Int Psychogeriatr. (2008) 20:1177–92. doi: 10.1017/S1041610208007503
22. Watt JA, Goodarzi Z, Veroniki AA, Nincic V, Khan PA, Ghassemi M, et al. Safety of pharmacologic interventions for neuropsychiatric symptoms in dementia: a systematic review and network meta-analysis. BMC Geriatr. (2020) 20:212. doi: 10.1186/s12877-020-01607-7
23. Reus VI, Fochtmann LJ, Eyler AE, Hilty DM, Horvitz-Lennon M, Jibson MD, et al. The American Psychiatric Association Practice Guideline on the Use of Antipsychotics to Treat Agitation or Psychosis in Patients with Dementia. Am J Psychiatry. (2016) 173:543–6. doi: 10.1176/appi.ajp.2015.173501
24. Sink KM, Holden KF, Yaffe K. Pharmacological treatment of neuropsychiatric symptoms of dementia: a review of the evidence. JAMA. (2005) 293:596–608. doi: 10.1001/jama.293.5.596
25. Kales HC, Kim HM, Zivin K, Valenstein M, Seyfried LS, Chiang C, et al. Risk of mortality among individual antipsychotics in patients with dementia. Am J Psychiatry. (2012) 169:71–9. doi: 10.1176/appi.ajp.2011.11030347
26. Schneider LS, Dagerman KS, Insel P. Risk of death with atypical antipsychotic drug treatment for dementia: meta-analysis of randomized placebo-controlled trials. JAMA. (2005) 294:1934–43. doi: 10.1001/jama.294.15.1934
27. Zou S, Kumar U. Cannabinoid receptors and the endocannabinoid system: signaling and function in the central nervous system. Int J Mol Sci. (2018) 19:833. doi: 10.3390/ijms19030833
28. Fernández-Ruiz J, Romero J, Ramos JA. Endocannabinoids and neurodegenerative disorders: parkinson’s disease, Huntington’s chorea, Alzheimer’s disease, and others. Handb Exp Pharmacol. (2015) 231:233–59. doi: 10.1007/978-3-319-20825-1_8
29. Basavarajappa BS, Shivakumar M, Joshi V, Subbanna S. Endocannabinoid system in neurodegenerative disorders. J Neurochem. (2017) 142:624–48. doi: 10.1111/jnc.14098
30. Baron EP. Medicinal properties of cannabinoids, terpenes, and flavonoids in cannabis, and benefits in migraine, headache, and pain: an update on current evidence and cannabis science. Headache. (2018) 58:1139–86. doi: 10.1111/head.13345
31. Fernandez-Ruiz J, Sagredo O, Pazos MR, Garcia C, Pertwee R, Mechoulam R, et al. Cannabidiol for neurodegenerative disorders: important new clinical applications for this phytocannabinoid? Br J Clin Pharmacol. (2013) 75:323–33. doi: 10.1111/j.1365-2125.2012.04341.x
32. Vandrey R, Herrmann ES, Mitchell JM, Bigelow GE, Flegel R, LoDico C, et al. Pharmacokinetic profile of oral cannabis in humans: blood and oral fluid disposition and relation to pharmacodynamic outcomes. J Anal Toxicol. (2017) 41:83–99. doi: 10.1093/jat/bkx012
33. Devinsky O, Cilio MR, Cross H, Fernandez-Ruiz J, French J, Hill C, et al. Cannabidiol: pharmacology and potential therapeutic role in epilepsy and other neuropsychiatric disorders. Epilepsia. (2014) 55:791–802. doi: 10.1111/epi.12631
34. Russo EB. Taming THC: potential cannabis synergy and phytocannabinoid-terpenoid entourage effects. Br J Pharmacol. (2011) 163:1344–64. doi: 10.1111/j.1476-5381.2011.01238.x
35. Bergamaschi MM, Queiroz RH, Chagas MH, de Oliveira DC, De Martinis BS, Kapczinski F, et al. Cannabidiol reduces the anxiety induced by simulated public speaking in treatment-naïve social phobia patients. Neuropsychopharmacology. (2011) 36:1219–26. doi: 10.1038/npp.2011.6
36. Crippa JA, Derenusson GN, Ferrari TB, Wichert-Ana L, Duran FL, Martin-Santos R, et al. Neural basis of anxiolytic effects of cannabidiol (CBD) in generalized social anxiety disorder: a preliminary report. J Psychopharmacol. (2011) 25:121–30. doi: 10.1177/0269881110379283
37. de Faria SM, de Morais Fabricio D, Tumas V, Castro PC, Ponti MA, Hallak JE, et al. Effects of acute cannabidiol administration on anxiety and tremors induced by a Simulated Public Speaking Test in patients with Parkinson’s disease. J Psychopharmacol. (2020) 34:189–96. doi: 10.1177/0269881119895536
38. Das RK, Kamboj SK, Ramadas M, Yogan K, Gupta V, Redman E, et al. Cannabidiol enhances consolidation of explicit fear extinction in humans. Psychopharmacology. (2013) 226:781–92. doi: 10.1007/s00213-012-2955-y
39. Chagas MH, Zuardi AW, Tumas V, Pena-Pereira MA, Sobreira ET, Bergamaschi MM, et al. Effects of cannabidiol in the treatment of patients with Parkinson’s disease: an exploratory double-blind trial. J Psychopharmacol. (2014) 28:1088–98. doi: 10.1177/0269881114550355
40. Aran A, Harel M, Cassuto H, Polyansky L, Schnapp A, Wattad N, et al. Cannabinoid treatment for autism: a proof-of-concept randomized trial. Mol Autism. (2021) 12:6. doi: 10.1186/s13229-021-00420-2
41. Devinsky O, Cross JH, Laux L, Marsh E, Miller I, Nabbout R, et al. Trial of cannabidiol for drug-resistant seizures in the Dravet syndrome. N Engl J Med. (2017) 376:2011–20. doi: 10.1056/NEJMoa1611618
42. McGuire P, Robson P, Cubala WJ, Vasile D, Morrison PD, Barron R, et al. Cannabidiol (CBD) as an adjunctive therapy in schizophrenia: a multicenter randomized controlled trial. Am J Psychiatry. (2018) 175:225–31. doi: 10.1176/appi.ajp.2017.17030325
43. Katz I, Katz D, Shoenfeld Y, Porat-Katz BS. Clinical evidence for utilizing cannabinoids in the elderly. Isr Med Assoc J. (2017) 19:71–5.
44. Volicer L, Stelly M, Morris J, McLAUGHLIN J, Volicer BJ. Effects of dronabinol on anorexia and disturbed behavior in patients with Alzheimer’s disease. Int J Geriatr Psychiatry. (1997) 12:913–9.
45. Shelef A, Barak Y, Berger U, Paleacu D, Tadger S, Plopsky I, et al. Safety and efficacy of medical cannabis oil for behavioral and psychological dymptoms of dementia: an-open label, add-on, pilot study. J Alzheimers Dis. (2016) 51:15–9. doi: 10.3233/Jad-150915
46. Bosnjak Kuharic D, Markovic D, Brkovic T, Jeric Kegalj M, Rubic Z, Vuica Vukasovic A, et al. Cannabinoids for the treatment of dementia. Cochrane Database Syst Rev. (2021) 9:CD012820. doi: 10.1002/14651858.CD012820.pub2
47. Hillen JB, Soulsby N, Alderman C, Caughey GE. Safety and effectiveness of cannabinoids for the treatment of neuropsychiatric symptoms in dementia: a systematic review. Ther Adv Drug Saf. (2019) 10:2042098619846993. doi: 10.1177/2042098619846993
48. Schleider LBL, Mechoulam R, Lederman V, Hilou M, Lencovsky O, Betzalel O, et al. Prospective analysis of safety and efficacy of medical cannabis in large unselected population of patients with cancer. Eur J Intern Med. (2018) 49:37–43. doi: 10.1016/j.ejim.2018.01.023
49. Abuhasira R, Schleider LBL, Mechoulam R, Novack V. Epidemiological characteristics, safety and efficacy of medical cannabis in the elderly. Eur J Intern Med. (2018) 49:44–50. doi: 10.1016/j.ejim.2018.01.019
50. Inglet S, Winter B, Yost SE, Entringer S, Lian A, Biksacky M, et al. Clinical data for the use of cannabis-based treatments: a comprehensive review of the literature. Ann Pharmacother. (2020) 54:1109–43. doi: 10.1177/1060028020930189
51. Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ. (2010) 340:c332. doi: 10.1136/bmj.c332
52. Folstein MF, Folstein SE, McHugh PR. Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. (1975) 12:189–98. doi: 10.1016/0022-3956(75)90026-6
53. Iverson GL, Hopp GA, DeWolfe K, Solomons K. Measuring change in psychiatric symptoms using the neuropsychiatric inventory: nursing Home version. Int J Geriatr Psychiatry. (2002) 17:438–43. doi: 10.1002/gps.617
54. Cummings JL, Mega M, Gray K, Rosenbergthompson S, Carusi DA, Gornbein J. The Neuropsychiatric Inventory: comprehensive assessment of psychopathology in dementia. Neurology. (1994) 44:2308–14. doi: 10.1212/Wnl.44.12.2308
55. Wood S, Cummings JL, Hsu MA, Barclay T, Wheatley MV, Yarema KT, et al. The use of the neuropsychiatric inventory in nursing home residents. Characterization and measurement. Am J Geriatr Psychiatry. (2000) 8:75–83. doi: 10.1097/00019442-200002000-00010
56. Dolgin M. Nomenclature and Criteria for Diagnosis of Diseases of the Heart and Great Vessels. Boston, MA: Little, Brown (1994).
57. Dumville JC, Hahn S, Miles JN, Torgerson DJ. The use of unequal randomisation ratios in clinical trials: a review. Contemp Clin Trials. (2006) 27:1–12. doi: 10.1016/j.cct.2005.08.003
58. Bar-Lev Schleider L, Mechoulam R, Saban N, Meiri G, Novack V. Real life experience of medical cannabis treatment in autism: analysis of safety and efficacy. Sci Rep. (2019) 9:200. doi: 10.1038/s41598-018-37570-y
59. Grotenhermen F. The pharmacokinetics and the pharmacodynamics of cannabinoids. Clin Pharmacokinet. (2003) 42:327–60. doi: 10.2165/00003088-200342040-00003
60. Naftali T, Bar-Lev Schleider L, Almog S, Meiri D, Konikoff FM. Oral CBD-rich cannabis induces clinical but not endoscopic response in patients with Crohn’s disease, a randomized controlled trial. J Crohns Colitis. (2021) 15:1799–806. doi: 10.1093/ecco-jcc/jjab069
61. Cohen-Mansfield J. Conceptualization of agitation: results based on the Cohen-Mansfield agitation inventory and the agitation behavior mapping instrument. Int Psychogeriatr. (1997) 8:309–15. doi: 10.1017/S1041610297003530
62. Cohen-mansfield J, Marx MS, Rosenthal AS. A description of agitation in a nursing home. J Gerontol. (1989) 44:M77–84. doi: 10.1093/geronj/44.3.M77
63. Rabinowitz J, Davidson M, De Deyn PP, Katz I, Brodaty H, Cohen-Mansfield J. Factor analysis of the Cohen-Mansfield agitation inventory in three large samples of nursing home patients with dementia and behavioral disturbance. Am J Geriatr Psychiatry. (2005) 13:991–8. doi: 10.1176/appi.ajgp.13.11.991
64. Weiner MF, Tractenberg RE, Jin S, Gamst A, Thomas RG, Koss E, et al. Assessing Alzheimer’s disease patients with the Cohen-Mansfield agitation inventory: scoring and clinical implications. J Psychiatr Res. (2002) 36:19–25. doi: 10.1016/S0022-3956(01)00047-4
65. Zuidema SU, Buursema AL, Gerritsen MGJM, Oosterwal KC, Smits MMM, Koopmans RTCM, et al. Assessing neuropsychiatric symptoms in nursing home patients with dementia: reliability and reliable change index of the neuropsychiatric inventory and the cohen-mansfield agitation inventory. Int J Geriatr Psychiatry. (2011) 26:127–34. doi: 10.1002/gps.2499
66. van den Elsen GA, Ahmed AI, Verkes RJ, Kramers C, Feuth T, Rosenberg PB, et al. Tetrahydrocannabinol for neuropsychiatric symptoms in dementia: a randomized controlled trial. Neurology. (2015) 84:2338–46. doi: 10.1212/WNL.0000000000001675
67. Herrmann N, Ruthirakuhan M, Gallagher D, Verhoeff N, Kiss A, Black SE, et al. Randomized placebo-controlled trial of Nabilone for agitation in Alzheimer’s disease. Am J Geriatr Psychiatry. (2019) 27:1161–73. doi: 10.1016/j.jagp.2019.05.002
68. Borenstein M, Rothstein H, Cohen J. Power and Precision: A Computer Program of Statistical Power Analyses and Confidence Intervals. Mahwah, NJ: Lawrence Erlbaum Associates, Inc (1997).
69. Shannon S, Lewis N, Lee H, Hughes S. Cannabidiol in anxiety and sleep: a large case series. Perm J. (2019) 23:18–041. doi: 10.7812/tpp/18-041
70. van den Elsen GAH, Ahmed AIA, Verkes RJ, Feuth T, van der Marck MA, Olde Rikkert MGM. Tetrahydrocannabinol in behavioral disturbances in dementia: a crossover randomized controlled trial. Am J Geriatr Psychiatry. (2015) 23:1214–24. doi: 10.1016/j.jagp.2015.07.011
71. Walther S, Schüpbach B, Seifritz E, Homan P, Strik W. Randomized, controlled crossover trial of dronabinol, 2.5 mg, for agitation in 2 patients with dementia. J Clin Psychopharmacol. (2011) 31:256–8. doi: 10.1097/JCP.0b013e31820e861c
72. Poleg S, Kourieh E, Ruban A, Shapira G, Shomron N, Barak B, et al. Behavioral aspects and neurobiological properties underlying medical cannabis treatment in Shank3 mouse model of autism spectrum disorder. Transl Psychiatry. (2021) 11:524. doi: 10.1038/s41398-021-01612-3
73. Gallily R, Yekhtin Z, Hanus L. Overcoming the bell-shaped dose-response of cannabidiol by using cannabis extract enriched in cannabidiol. Pharm Pharmacol. (2015) 6:75–85. doi: 10.4236/pp.2015.62010
74. Mühlbauer V, Möhler R, Dichter MN, Zuidema SU, Köpke S, Luijendijk HJ. Antipsychotics for agitation and psychosis in people with Alzheimer’s disease and vascular dementia. Cochrane Database Syst Rev. (2021) 12:CD013304. doi: 10.1002/14651858.CD013304.pub2
75. Auchus AP, Bissey-Black C. Pilot study of haloperidol, fluoxetine, and placebo for agitation in Alzheimer’s disease. J Neuropsychiatry Clin Neurosci. (1997) 9:591–3. doi: 10.1176/jnp.9.4.591
76. Teri L, Logsdon RG, Peskind E, Raskind M, Weiner MF, Tractenberg RE, et al. Treatment of agitation in AD: a randomized, placebo-controlled clinical trial. Neurology. (2000) 55:1271–8. doi: 10.1212/wnl.55.9.1271
77. Grossberg GT, Kohegyi E, Mergel V, Josiassen MK, Meulien D, Hobart M, et al. Efficacy and safety of brexpiprazole for the treatment of agitation in Alzheimer’s dementia: two 12-week, randomized, double-blind, placebo-controlled trials. Am J Geriatr Psychiatry. (2020) 28:383–400. doi: 10.1016/j.jagp.2019.09.009
78. Rosenberg PB, Drye LT, Porsteinsson AP, Pollock BG, Devanand DP, Frangakis C, et al. Change in agitation in Alzheimer’s disease in the placebo arm of a nine-week controlled trial. Int Psychogeriatr. (2015) 27:2059–67. doi: 10.1017/S1041610215001106
79. Hersch EC, Falzgraf S. Management of the behavioral and psychological symptoms of dementia. Clin Interv Aging. (2007) 2:611–21. doi: 10.2147/cia.s1698
80. Marcinkowska M, Śniecikowska J, Fajkis N, Paśko P, Franczyk W, Kołaczkowski M. Management of dementia-related psychosis, agitation and aggression: a review of the pharmacology and clinical effects of potential drug candidates. CNS Drugs. (2020) 34:243–68. doi: 10.1007/s40263-020-00707-7
81. Pisanti S, Malfitano AM, Ciaglia E, Lamberti A, Ranieri R, Cuomo G, et al. Cannabidiol: state of the art and new challenges for therapeutic applications. Pharmacol Ther. (2017) 175:133–50. doi: 10.1016/j.pharmthera.2017.02.041
82. Ibeas Bih C, Chen T, Nunn AV, Bazelot M, Dallas M, Whalley BJ. Molecular targets of cannabidiol in neurological disorders. Neurotherapeutics. (2015) 12:699–730. doi: 10.1007/s13311-015-0377-3
83. Elsaid S, Kloiber S, Le Foll B. Effects of cannabidiol (CBD) in neuropsychiatric disorders: a review of pre-clinical and clinical findings. Prog Mol Biol Transl Sci. (2019) 167:25–75. doi: 10.1016/bs.pmbts.2019.06.005
84. García-Gutiérrez MS, Navarrete F, Gasparyan A, Austrich-Olivares A, Sala F, Manzanares J. Cannabidiol: a potential new alternative for the treatment of anxiety, depression, and psychotic disorders. Biomolecules. (2020) 10:1575. doi: 10.3390/biom10111575
85. Martín-Moreno AM, Brera B, Spuch C, Carro E, García-García L, Delgado M, et al. Prolonged oral cannabinoid administration prevents neuroinflammation, lowers β-amyloid levels and improves cognitive performance in Tg APP 2576 mice. J Neuroinflammation. (2012) 9:8. doi: 10.1186/1742-2094-9-8
86. Bhattacharyya S, Fusar-Poli P, Borgwardt S, Martin-Santos R, Nosarti C, O’Carroll C, et al. Modulation of mediotemporal and ventrostriatal function in humans by Delta9-tetrahydrocannabinol: a neural basis for the effects of Cannabis sativa on learning and psychosis. Arch Gen Psychiatry. (2009) 66:442–51.
87. Berman JS, Symonds C, Birch R. Efficacy of two cannabis based medicinal extracts for relief of central neuropathic pain from brachial plexus avulsion: results of a randomised controlled trial. Pain. (2004) 112:299–306. doi: 10.1016/j.pain.2004.09.013
88. Ware MA, Wang T, Shapiro S, Robinson A, Ducruet T, Huynh T, et al. Smoked cannabis for chronic neuropathic pain: a randomized controlled trial. CMAJ. (2010) 182:E694–701. doi: 10.1503/cmaj.091414
89. Ware MA, Fitzcharles MA, Joseph L, Shir Y. The effects of nabilone on sleep in fibromyalgia: results of a randomized controlled trial. Anesth Analg. (2010) 110:604–10. doi: 10.1213/ANE.0b013e3181c76f70
90. Cameron C, Watson D, Robinson J. Use of a synthetic cannabinoid in a correctional population for posttraumatic stress disorder-related insomnia and nightmares, chronic pain, harm reduction, and other indications: a retrospective evaluation. J Clin Psychopharmacol. (2014) 34:559–64. doi: 10.1097/jcp.0000000000000180
91. Gorelick DA, Goodwin RS, Schwilke E, Schroeder JR, Schwope DM, Kelly DL, et al. Around-the-clock oral THC effects on sleep in male chronic daily cannabis smokers. Am J Addict. (2013) 22:510–4. doi: 10.1111/j.1521-0391.2013.12003.x
92. Woodward MR, Harper DG, Stolyar A, Forester BP, Ellison JM. Dronabinol for the treatment of agitation and aggressive behavior in acutely hospitalized severely demented patients with noncognitive behavioral symptoms. Am J Geriatr Psychiatry. (2014) 22:415–9. doi: 10.1016/j.jagp.2012.11.022
93. Blake DR, Robson P, Ho M, Jubb RW, McCabe CS. Preliminary assessment of the efficacy, tolerability and safety of a cannabis-based medicine (Sativex) in the treatment of pain caused by rheumatoid arthritis. Rheumatology (Oxford). (2006) 45:50–2. doi: 10.1093/rheumatology/kei183
94. Serpell M, Ratcliffe S, Hovorka J, Schofield M, Taylor L, Lauder H, et al. A double-blind, randomized, placebo-controlled, parallel group study of THC/CBD spray in peripheral neuropathic pain treatment. Eur J Pain. (2014) 18:999–1012. doi: 10.1002/j.1532-2149.2013.00445.x
95. Rog DJ, Nurmikko TJ, Friede T, Young CA. Randomized, controlled trial of cannabis-based medicine in central pain in multiple sclerosis. Neurology. (2005) 65:812–9. doi: 10.1212/01.wnl.0000176753.45410.8b
96. Linares IMP, Guimaraes FS, Eckeli A, Crippa ACS, Zuardi AW, Souza JDS, et al. No acute effects of cannabidiol on the sleep-wake cycle of healthy subjects: a randomized, double-blind, placebo-controlled, crossover study. Front Pharmacol. (2018) 9:315. doi: 10.3389/fphar.2018.00315
97. Tzadok M, Uliel-Siboni S, Linder I, Kramer U, Epstein O, Menascu S, et al. CBD-enriched medical cannabis for intractable pediatric epilepsy: The current Israeli experience. Seizure. (2016) 35:41–4. doi: 10.1016/j.seizure.2016.01.004
98. Arout CA, Haney M, Herrmann ES, Bedi G, Cooper ZD. A placebo-controlled investigation of the analgesic effects, abuse liability, safety and tolerability of a range of oral cannabidiol doses in healthy humans. Br J Clin Pharmacol. (2022) 88:347–55. doi: 10.1111/bcp.14973
99. Peters EN, Mosesova I, MacNair L, Vandrey R, Land MH, Ware MA, et al. Safety, pharmacokinetics and pharmacodynamics of spectrum yellow oil in healthy participants. J Anal Toxicol. (2022) 46:393–407. doi: 10.1093/jat/bkab026
100. Aran A, Cassuto H, Lubotzky A, Wattad N, Hazan E. Brief report: cannabidiol-rich cannabis in children with autism spectrum disorder and severe behavioral problems-a retrospective feasibility study. J Autism Dev Disord. (2019) 49:1284–8. doi: 10.1007/s10803-018-3808-2
101. Barchel D, Stolar O, De-Haan T, Ziv-Baran T, Saban N, Fuchs DO, et al. Oral cannabidiol use in children with autism spectrum disorder to treat related symptoms and co-morbidities. Front Pharmacol. (2019) 9:1521. doi: 10.3389/Fphar.2018.01521
102. Libzon S, Schleider LB, Saban N, Levit L, Tamari Y, Linder I, et al. Medical cannabis for pediatric moderate to severe complex motor disorders. J Child Neurol. (2018) 33:565–71. doi: 10.1177/0883073818773028
Keywords: medical cannabis, cannabidiol, dementia, behavioral disturbances, agitation, randomized controlled trial (RCT), neuropsychiatric symptoms
Citation: Hermush V, Ore L, Stern N, Mizrahi N, Fried M, Krivoshey M, Staghon E, Lederman VE and Bar-Lev Schleider L (2022) Effects of rich cannabidiol oil on behavioral disturbances in patients with dementia: A placebo controlled randomized clinical trial. Front. Med. 9:951889. doi: 10.3389/fmed.2022.951889
Received: 24 May 2022; Accepted: 15 August 2022;
Published: 06 September 2022.
Edited by:
Esther-Lee Marcus, Herzog Hospital, IsraelReviewed by:
Reuven Or, Hadassah Medical Center, IsraelDamiana Scuteri, University of Calabria, Italy
Copyright © 2022 Hermush, Ore, Stern, Mizrahi, Fried, Krivoshey, Staghon, Lederman and Bar-Lev Schleider. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vered Hermush, vhermush@laniado.org.il