 Håkan Lars Olsson1*
Håkan Lars Olsson1* Mona Landin Olsson2
Mona Landin Olsson2- 1Departments of Oncology and Cancer Epidemiology, Clinical Sciences, Lund University, Lund, Sweden
- 2Department of Endocrinology, Clinical Sciences, Lund University, Lund, Sweden
Cyclic hormonal stimulation of the breast tissue plays a significant role in breast carcinogenesis. Current risk factor models do not include direct measures of cycle characteristics although the effects of possible surrogates of cycle activity such as age at menarche and menopause, parity, and nursing time have been investigated. Future risk models should also include menstrual cycle length, regularity, number of cycles before first full-term pregnancy, and life-time number of cycles. New risk factor models for pre- and postmenopausal breast cancer are proposed here. Furthermore, there is a need for more long-term, prospective studies investigating menstrual cycle characteristics as data currently available are primarily retrospective and collected at one time-point only.
Background
In the 1990s, our research group pioneered studies on menstrual cycle length, menstrual regularity, and the number of menstrual cycles as risk factors for breast cancer (1, 2). Women who developed breast cancer were more likely to have short, regular cycles, and had more cycles before the first full-term pregnancy than healthy women and those with benign breast disease. As the luteal phase is fixed in time, only the follicular phase may vary, thus exposing women with shorter, and more numerous cycles to higher amounts of progesterone during the luteal phase (3). We and others have also shown a greater number of dividing epithelial cells in the luteal phase than in the follicular phase (4–6). Cell division is generally considered a prerequisite for carcinogenesis and women with short and numerous cycles may therefore have a higher risk of developing cancer as a result of increased cell proliferation. Although progesterone protects against endometrial cancer, it appears to have a different effect in increasing breast cancer risk (7). This was confirmed by recent findings investigating breast cancer type 1 susceptibility protein (BRCA1) carcinogenesis, the roles of progesterone and receptor activator of nuclear factor kappa-B ligand (RANKL), and the therapeutic potential of anti-progestins (8, 9).
Furthermore, several studies regarding the risk of exogenous hormones and breast cancer revealed that the combination of progestins and estrogen increased the risk of breast cancer compared with the effects of estrogen alone (10–13). We also showed that shorter menstrual cycles were associated with the cytochrome P450 17 (CYP17) genotype (14).
A list of studies concerning the menstrual cycle is presented in Table 1 (15–25). These studies indicate that a high number of cycles before the first full-term pregnancy and high life-time menstrual activity (LMA) increased breast cancer risk. Furthermore, a short time interval between menarche and the establishment of regular cycles is another risk factor. In contrast, no relationship was observed between the length of menstrual bleeding and breast cancer (26). Of the studies listed in Table 1 two (16, 20) included only Asian women and one (24) only American African women.
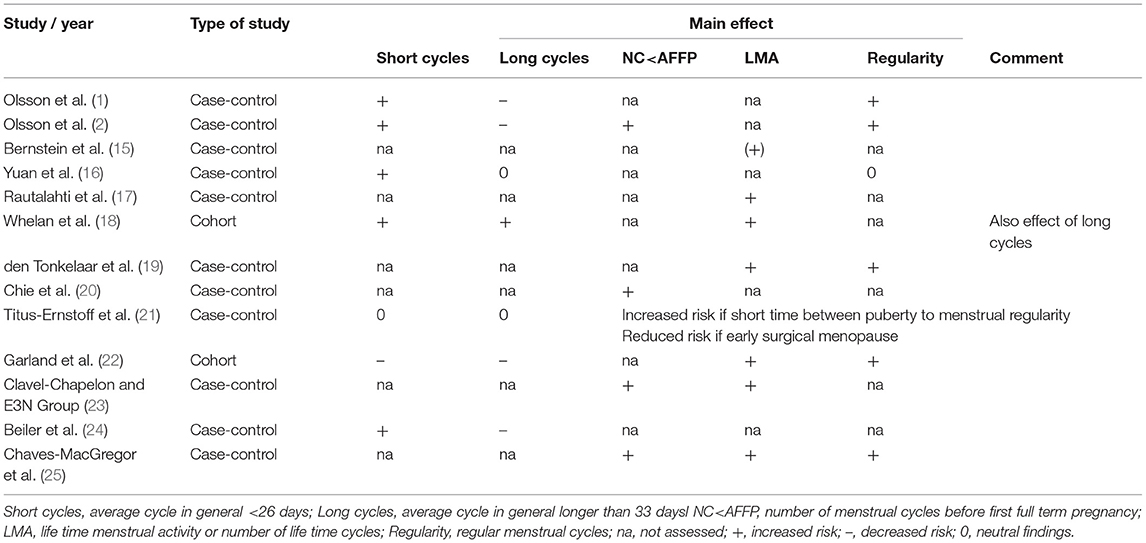
Table 1. Studies of different menstrual cycle characteristics and breast cancer risk.
LMA is calculated for natural cycles using the following variables: age at menopause and menarche, average cycle length, number of pregnancies, and duration of nursing excluding periods of exogenous hormone use. There are however a number of relevant caveats: first, cycle length may vary during reproductive life and studies thus consider the average cycle length. In retrospective studies, there may be a recall bias for cycle length. Furthermore, there are discrepancies regarding the number of cycles counted during exogenous hormonal treatment (27, 28). In addition, there are few high-quality, long-term (life-time) prospective studies investigating cycle length. In this context and in support of the importance of LMA, it is notable that early menopause or castration protect against breast cancer. Other factors such as extreme physical activity and starvation reduce cyclic activity and thus breast cancer risk (29). Finally, the consistency in results regarding cycle length, the number of cycles before the first full-term pregnancy, and LMA indicate that the crude retrospective assessment of menstrual cycles has an important bearing on investigating breast cancer risk.
Benign breast disease is characterized by irregular menstrual cycles and is more common at the end of reproductive life (1). Irregular cycles cause cystic disease in the breasts and ovaries and women with cystic ovarian disease therefore have a lower incidence of breast cancer (30).
We have postulated that women whose breast size is maintained or increased after hormonal exposure may have a higher risk of cancer than those whose breast size decreases upon such exposure (31). However, this hypothesis requires further investigation of the menstrual cycle. Possible assessment of breast density or magnetic resonance imaging (MRI) images without contrast assessing fibroglandular density may be helpful (32).
Finally, the effects of oral contraceptive (OC) use should be investigated. For example, it is unclear whether lengthening menstrual cycles artificially via administration of OCs in women with naturally short cycles decreases cancer risk. Conversely, it is also unclear whether cancer risk increases in women whose naturally long cycles are artificially shortened by the use of OCs.
A number of risk factors have been identified for breast cancer such as age at menarche, age at first full term pregnancy, parity, age at menopause, obesity (postmenopausal risk), number of menstrual cycles, weight gain, hormone replacement therapy, early oral contraceptive use, breast size, preecclampsia, birth weight, nursing, height, breast density, physical activity, night shift work, radiation exposure, tobacco use, alcohol use, family history, mutation carrier of a predisposing gene. Some of the above factors are still under investigation with partly diverging findings such as for tobacco use, breast size and night shift work and others like preecclampsia and high physical activity are protective. Some factors like radiation exposure, reproductive and genetic factors are more important premenopausally, while obesity is more important for older women.
Development of better methods to describe the menstrual cycle more exact is needed. One method is of course to use a calendar recording the start of each menstruation, another way is to record basal body temperature daily, women in the luteal phase have a higher body temperature, or study the cervical mucus. However, it can be difficult to pinpoint ovulation using these methods, especially if your menstrual cycles are irregular. Research in fertility medicine especially in women with irregular menstruations is mainly driven to better time ovulation through ovulation prediction kits either using urine (measuring LH) or saliva (studying ferning patterns in relation to estrogen increase). Again these latter methods are too cumbersome and expensive to be used in large epidemiological risk factor studies and explain their absence in literature.
Conclusion and Proposal
The characteristics and number of menstrual cycles before the first full-term pregnancy, LMA, and menstrual regularity require further investigation as part of epidemiological studies of breast cancer, as other risk factors such as age at menarche and menopause, parity, and nursing are only surrogates for cyclic hormonal exposure. Menstrual cycle characteristics should be included in risk factor models of breast cancer. Current models such as Gail, Tyrer-Cusick, Rosner Colditz BCRAT, BCPRO, and BOADICEA only include family history, germline mutation status, breast density, polygenic risk scores, and surrogates of cycle activity such as age at menarche, age at first full-term pregnancy (AFFP), parity, nursing, and age at menopause (33–39). The BOADICEA and Tyrer-Cusick models appear to be the most informative (39). Parity and AFFP may exert independent effects on differentiation of the breast epithelium, and are indirectly related to menstrual cycle activity. However, cyclic hormonal stimulation of the breast tissue, which is probably the most important hormonal factor contributing to breast cancer, is not directly investigated in such models. Proposed revised risk factor models for pre- and postmenopausal breast cancer are listed in Table 2. Only surrogates such as age at menarche, AFFP, parity, and nursing have been included in previous studies. Prospective life-time studies on menstrual cycle activity are encouraged, as current studies primarily include retrospective data collected at one time-point and often use average measures of menstrual factors. Studies covering longer time periods should include other factors of importance for the menstrual cycle such as physical activity, obesity, psychological stress, and intercurrent diseases such as osteoporosis (29).
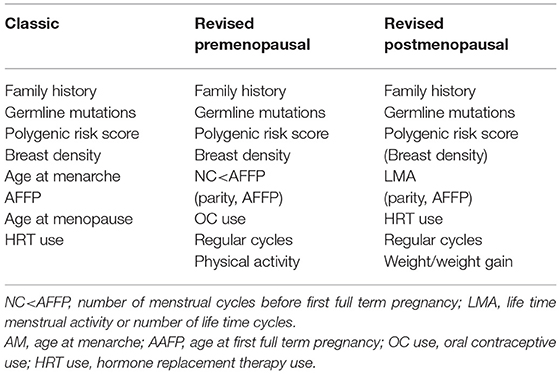
Table 2. Revised risk factor models for breast cancer taking the menstrual cycle into account.
Author Contributions
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
Funding
This work was supported by grants from the Swedish Cancer Society, the Berta Kamprad Foundation, and local hospital funds.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Olsson H, Landin-Olsson M, Gullberg B. Retrospective assessment of menstrual cycle length in patients with breast cancer, in patients with benign breast disease, and in women without breast disease. J Natl Cancer Inst. (1983) 70:17–20.
2. Olsson H, Ranstam J, Landin-Olsson M. The number of menstrual cycles prior to the first full-term pregnancy: an important risk factor of breast cancer? Acta Radiol Oncol. (1987) 26:387–9. doi: 10.3109/02841868709104365
3. Atashgaran V, Wrin J, Barry SC, Dasari P, Ingman WV. Dissecting the biology of menstrual cycle-associated breast cancer risk. Front Oncol. (2016) 6:267. doi: 10.3389/fonc.2016.00267
4. Ferguson D, Anderson T. Morphological evaluation of cell turnover in relation to the menstrual cycle in the “resting” human breast. Br J Cancer. (1981) 44:177. doi: 10.1038/bjc.1981.168
5. Olsson H, Jernstrom H, Alm P, Kreipe H, Ingvar C, Jonsson PE, et al. Proliferation of the breast epithelium in relation to menstrual cycle phase, hormonal use, and reproductive factors. Breast Cancer Res Treat. (1996) 40:187–96. doi: 10.1007/BF01806214
6. Huh SJ, Oh H, Peterson MA, Almendro V, Hu R, Bowden M, et al. The proliferative activity of mammary epithelial cells in normal tissue predicts breast cancer risk in premenopausal women. Cancer Res. (2016) 76:1926–34. doi: 10.1158/0008-5472.CAN-15-1927
7. Brisken C. Progesterone signalling in breast cancer: a neglected hormone coming into the limelight. Nat Rev Cancer. (2013) 13:385–96. doi: 10.1038/nrc3518
8. Hu H, Wang J, Gupta A, Shidfar A, Branstetter D, Lee O, et al. RANKL expression in normal and malignant breast tissue responds to progesterone and is up-regulated during the luteal phase. Breast Cancer Res Treat. (2014) 146:515–23. doi: 10.1007/s10549-014-3049-9
9. Tanos T, Sflomos G, Echeverria PC, Ayyanan A, Gutierrez M, Delaloye J-F, et al. Progesterone/RANKL is a major regulatory axis in the human breast. Sci Transl Med. (2013) 5:182. doi: 10.1126/scitranslmed.3005654
10. Rossouw JE, Anderson GL, Prentice RL, LaCroix AZ, Kooperberg C, Stefanick ML, et al. Writing Group for the Women's Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women's Health Initiative randomized controlled trial. J Am Med Assoc. (2002) 288:321–33. doi: 10.1001/jama.288.3.321
11. Olsson HL, Ingvar C, Bladstrom A. Hormone replacement therapy containing progestins and given continuously increases breast carcinoma risk in Sweden. Cancer. (2003) 97:1387–92. doi: 10.1002/cncr.11205
12. Beral V, Million Women Study Collaborators. Breast cancer and hormone-replacement therapy in the Million Women Study. Lancet. (2003) 362:419–27. doi: 10.1016/S0140-6736(03)14596-5
13. Anderson GL, Limacher M, Assaf AR, Bassford T, Beresford SA, Black H, et al. Women's health initiative steering committee. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women's Health Initiative randomized controlled trial. J Am Med Assoc. (2004) 291:701–12. doi: 10.1001/jama.291.14.1701
14. Henningson M, Johansson U, Borg A, Olsson H, Jernstrom H. CYP17 genotype is associated with short menstrual cycles, early oral contraceptive use and BRCA mutation status in young healthy women. Mol Hum Reprod. (2007) 13:231–6. doi: 10.1093/molehr/gam004
15. Bernstein L, Ross RK, Lobo RA, Hanisch R, Krailo MD, Henderson BE. The effects of moderate physical activity on menstrual cycle patterns in adolescence: implications for breast cancer prevention. Br J Cancer. (1987) 55:681–5. doi: 10.1038/bjc.1987.139
16. Yuan JM, Yu MC, Ross RK, Gao YT, Henderson BE. Risk factors for breast cancer in Chinese women in Shanghai. Cancer Res. (1988) 49:1949–53.
17. Rautalahti M, Albanes D, Virtamo J, Palmgren J, Haukka J, Heinonen OP. Lifetime menstrual activity – Indicator of breast cancer risk. Eur J Epidemiol. (1993) 9:17–25. doi: 10.1007/BF00463085
18. Whelan EA, Sandler DP, Root JL, Smith KR, Weinberg CR. Menstrual cycle patterns and risk of breast cancer. Am J Epidemiol. (1994) 140:1081–90. doi: 10.1093/oxfordjournals.aje.a117208
19. den Tonkelaar I, de Waard F. Regularity and length of menstrual cycles in women aged 41-46 in relation to breast cancer risk: results from the DOM-project. Breast Cancer Res Treat. (1996) 38:253–8. doi: 10.1007/BF01806143
20. Chie W, Fu C, Lee W, Li C, Huang C, Chang K, et al. Ages at different reproductive events, numbers of menstrual cycles in between and breast cancer risk. Oncol Rep. (1997) 4:1039–43. doi: 10.3892/or.4.5.1039
21. Titus-Ernztoff L, Lonenecker MP, Newcomb PA, Dain B, Greenberg ER, Mittendorf R, et al. Menstrual factors in relation to breast cancer risk. Cancer Epidemiol Biomark Prev. (1998) 7:783–9.
22. Garland M, Hunter DJ, Colditz GA, Manson JE, Stampfer MJ, Spiegelman D, et al. Menstrual cycle characteristics and history of ovulatory infertility in relation in breast cancer risk in a large cohort of US women. Am J Epidemiol. (1998) 147:636–43. doi: 10.1093/oxfordjournals.aje.a009504
23. Clavel-Chapelon F, E3N Group. Cumulative number of menstrual cycles and breast cancer risk: results from the E3N cohort study of French women. Cancer Cause Control. (2002) 13:831–8. doi: 10.1023/A:1020684821837
24. Beiler JS, Zhu K, Hunter S, Payne-Wilks K, Roland CL, Chinchilli VM. A case-control study of menstrual factors in relation to breast cancer risk in African-American women. J Natl Med Assoc. (2003) 95:930–8.
25. Chavez-MacGregor M, Elias SG, Onland-Moret NC, van der Schouw YT, Van Gils CH, Monninkhof E, et al. Postmenopausal breast cancer risk and cumulative number of menstrual cycles. Cancer Epidemiol Biomark Prev. (2005) 14:799–804. doi: 10.1158/1055-9965.EPI-04-0465
26. Butler LM, Potischman NA, Newman B, Millikan RC, Brogan D, Gammon MD, et al. Menstrual risk factors and early-onset breast cancer. Cancer Cause Control. (2000) 11:451–8. doi: 10.1023/A:1008956524669
27. Gorrindo T, Lu Y, Pincus S, Riley A, Simon JA, Singer BH, et al. Lifelong menstrual histories are typically erratic and trending: a taxonomy. Menopause. (2007) 14:74–88. doi: 10.1097/01.gme.0000227853.19979.7f
28. Small CM, Manatunga AK, Marcus M. Validity of self-reported menstrual cycle length. Ann Epidemiol. (2007) 17:163–70. doi: 10.1016/j.annepidem.2006.05.005
29. Harlow SD, Ephross SA. Epidemiology of menstruation and its relevance to women's health. Epidemiol Rev. (1995) 17:265–86. doi: 10.1093/oxfordjournals.epirev.a036193
30. Bosetti C, Scotti L, Negri E, Talamini R, Levi F, Franceschi S, et al. Benign ovarian cysts and breast cancer risk. Int J Cancer. (2006) 119:1679–82. doi: 10.1002/ijc.22016
31. Olsson H. Risk for malignant tumors after oral contraceptive use: is it related to organ size while taking the pill? Med Oncol Tumor Pharmacother. (1990) 7:61–4.
32. Grubstein A, Rapson Y, Benzaquen O, Rozenblatt S, Gadiel I, Atar E, et al. Comparison of background parenchymal enhancement and fibroglandular density at breast magnetic resonance imaging between BRCA gene mutation carriers and non-carriers. Clin Imaging. (2018) 51:347–51. doi: 10.1016/j.clinimag.2018.06.010
33. Gail MH, Brinton LA, Byar DP, Corle DK, Green SB, Schairer C, et al. Projecting individualized probabilities of developing breast cancer for white females who are being examined annually. J Natl Cancer Inst. (1989) 81:1879–86. doi: 10.1093/jnci/81.24.1879
34. Tyrer J, Duffy SW, Cuzick JA. Breast cancer prediction model incorporating familial and personal risk factors. Stat Med. (2004) 23:1111–30. doi: 10.1002/sim.1668
35. Rosner B, Colditz GA. Nurses' Health Study: log-incidence mathematical model of breast cancer incidence. J Natl Cancer Inst. (1996) 88:359–64. doi: 10.1093/jnci/88.6.359
36. Pharoah PD, Antoniou AC, Easton DF, Ponder BA. Polygenes, risk prediction, and targeted prevention of breast cancer. N Engl J Med. (2008) 358:2796–803. doi: 10.1056/NEJMsa0708739
37. Brentnall AR, Cuzick J, Buist DSM, Bowles EJA. Long-term accuracy of breast cancer risk assessment combining classic risk factors and breast density. JAMA Oncol. (2018) 4:e180174. doi: 10.1001/jamaoncol.2018.0174
38. Lee A, Mavaddat N, Wilcox AN, Cunningham AP, Carver T, Hartley S, et al. BOADICEA: a comprehensive breast cancer risk prediction model incorporating genetic and nongenetic risk factors. Genet Med. (2019) 21:1708–18. doi: 10.1038/s41436-018-0406-9
Keywords: breast cancer, menstrual cycle, risk, retrospective, prospective
Citation: Olsson HL and Olsson ML (2020) The Menstrual Cycle and Risk of Breast Cancer: A Review. Front. Oncol. 10:21. doi: 10.3389/fonc.2020.00021
Received: 19 August 2019; Accepted: 08 January 2020;
Published: 24 January 2020.
Edited by:
Mary Beth Terry, Columbia University, United StatesReviewed by:
Azin Nahvijou, Tehran University of Medical Science, IranAhmadreza Niavarani, Tehran University of Medical Sciences, Iran
Jasmine A. McDonald, Columbia University, United States
Copyright © 2020 Olsson and Olsson. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Håkan Lars Olsson, hakan.olsson@med.lu.se