 Jonas Leonhardt1
Jonas Leonhardt1 Marcela Winkler2
Marcela Winkler2 Anne Kollikowski3
Anne Kollikowski3 Lisa Schiffmann3Anne Quenzer4
Lisa Schiffmann3Anne Quenzer4 Hermann Einsele1
Hermann Einsele1 Claudia Löffler1,3*
Claudia Löffler1,3*- 1Department of Internal Medicine II, University Hospital of Wuerzburg, Wuerzburg, Germany
- 2Department of Natural and Integrative Medicine, Robert-Bosch-Hospital, Stuttgart, Germany
- 3Comprehensive Cancer Center, University Hospital of Wuerzburg, Wuerzburg, Germany
- 4Department of Gynecology and Obstetrics, University Hospital of Wuerzburg, Wuerzburg, Germany
Introduction: National and international guidelines recommend early integration of evidence-based multimodal interventions and programs, especially with a focus on relaxation techniques and other Mind–Body-based methods to maintain the quality of life of oncology patients, improve treatment tolerability, and promote healthy lifestyle behaviors. Consequently, we aim to understand what drives patients and how they navigate integrative medicine to best advise them. This study aimed to detect possible topics of particular interest to patients and identify the patient groups that could benefit most from further programs. Furthermore, we aimed to investigate if patients are open-minded toward integrative oncology concepts and learn about their motivational level to maintain or change behavior.
Methods: Between August 2019 and October 2020 we surveyed patients undergoing oncological therapy in a university oncological outpatient center using a custom-developed questionnaire based on established Mind–Body Medicine concepts.
Results: We included 294 patients with various cancers. More than half reported problems sleeping through (61%) and 42% felt stressed frequently, invariably rating this as detrimental to their health. Moreover, a slight majority (52%) felt physically limited due to their disease and only 30% performed defined exercise programs. Women were significantly more likely to feel stressed and reported with alarming frequency that they often feel “everything was up to them.” The 40–65-year-olds reported significantly less restful sleep, more stress and were more dissatisfied with their situation. However, this group already used natural remedies most frequently and was most often motivated to use relaxation techniques in the next 6 months. The lower the perceived individual energy level (EL), the less frequently patients did sport, the more frequently they felt their disease impaired their activity, mostly feeling stressed and tense. We also found significant associations between negative emotions/thoughts and the variables “sleep,” “use of relaxation techniques,” “personal stress perception,” and “successful lifestyle modification.”
Conclusion: Mind–Body programs that focus on patient’s individual resources, with tools to explore impairing patterns of self-perception and cognitive biases, can be a valuable resource for oncology patients and should therefore be part of an integrative medical treatment concept.
1. Introduction
Numerous studies prove the sustained interest of Europeans and especially Germans in complementary and alternative medicine (CAM) (Kemppainen et al., 2018; Fjær et al., 2020; Lederer et al., 2021). Patients desire to strengthen personal resources, play an active role in coping with their disease, receive holistic care, and improve the side effects of their therapy (Davidson et al., 2002; Boon et al., 2003; Verhoef et al., 2005; Evans et al., 2007; Huebner et al., 2014; Klafke et al., 2014). In contrast to alternative methods, integrative oncology as a future model of evidence-based complementary medicine stands for a meaningful addition to conventional therapies (Deng et al., 2013; Witt et al., 2017). National and international guidelines recommend early integration of evidence-based multimodal interventions and programs to maintain the quality of life of oncology patients, improve treatment tolerability, and promote healthy lifestyle behaviors (Greenlee et al., 2017; Jeitler et al., 2017; Voiß et al., 2020; Deutsche Krebsgesellschaft, 2021). A focus within these multimodal concepts is on Mind–Body-Medicine (MBM) interventions and techniques. The National Institutes of Health (NIH) describes MBM as a discipline that focuses on the nature of the interactions that link the brain, the body, the mind, and behavior to one another and how emotional, mental, social, spiritual, experiential, and behavioral factors can directly influence health (Esch and Stefano, 2022).
Therefore, we wanted to determine subjectively unmet needs for integrative counseling and treatment services among cancer patients at the Comprehensive Cancer Center of the University Hospital of Wuerzburg. Moreover, we aimed to investigate if patients are open-minded toward integrative oncology concepts and to learn how motivated they are to change behavior. We also wanted to better understand those topics of particular interest to patients and identify those who could benefit most from further programs. We hypothesized that individual mindset at the time of the survey might both influence how stressed and burdened patients feel and affect their motivation to change behavior. Hence, we focused specifically on individual emotional/mental state, as well as inquired about interest in Mind–Body interventions, which we judged to be an appropriate evidence-based resource.
2. Materials and methods
2.1. Participants and recruitment
Patients suffering from a hematological or solid tumor and undergoing outpatient treatment were recruited by an MD student and physicians at the Interdisciplinary Outpatient Departments for Chemotherapy for Internal Medicine and Gynecology of Wuerzburg University Hospital. The patients had to be at least 18 years old. Otherwise, there were no exclusion criteria. After detailed explanation of the questionnaire by an MD student, each patient signed the consent form, and written informed consent regarding data protection. Consent could be withdrawn at any time during and after the survey.
2.2. Data collection
A MD student extracted general patient information (e.g., stage of the disease, medication, clinical course of therapy) from medical records. The number of different medication prescribed daily at the time of the survey was taken into account, whereby the oncological therapy itself was not counted. Medication prescribed more than once a day were only taken into account once in the evaluation. On-demand medication, as well as medication that should be taken less frequently than once a day, were not included in the evaluation.
2.3. Questionnaire
We used a custom-developed questionnaire based on a Mind–Body-Medicine Day Care Clinic program, first published in 2013 and intended to support patients cope with their disease and establish a healthy lifestyle (Paul et al., 2013; Dobos et al., 2015). The Day Care Clinic program combines elements of the MBM Cancer Program of the Benson-Henry Mind/Body Medical Institute at Harvard Medical School, techniques from the Mindfulness-Based Stress Reduction (MBSR) program, as well as defined methods of self-regulation and self-care (Kabat-Zinn, 1982; Kabat-Zinn, 1990; Benson, 1999). It also focusses on the patient’s individual resources, based on the salutogenic model to “guide health promotion” (Mittelmark et al., 2017). Accordingly, relaxation techniques, exercise, cognitive restructuring, nutrition, and social support are important elements.
Patients were asked to provide feedback on the following (* indicates dichotomous items): a.o. sleep*; daily rhythms; perceived energy level on a scale from 0 (lowest imaginable energy level) to 10 (highest imaginable energy-level); use of breathing* and/or relaxation techniques and personal stress perception*; dietary habits; sports activity; use of natural remedies; social support*; thoughts, feelings, and attitudes. In order to better understand the relationship between thoughts, feelings, attitudes and wellbeing, as well as the motivation to develop healthy habits, patients were asked to assess which statements they could identify with from five statements suggesting either a rather optimistic or a rather pessimistic emotional alignment. Regarding health-promoting behavior, we asked how long this could already be maintained and whether and when patients could imagine changing their behavior. The data was collected paper based. Supplementary Table S2 provides detailed information on the set of questions, as well as on missing data.
2.4. Statement of ethics
Patients’ written, informed consent could be withdrawn at any time during and after the survey. The study was approved by the Ethics Committee of the Julius-Maximilian-University Wuerzburg on 15 April 2019 (study number 12/19-me) and performed according to the Declaration of Helsinki.
2.5. Statistical analysis
The results were statistically analyzed using the data processing program IBM SPSS Statistics version 25 for Windows (IBM SPSS Statistics for Windows, 2017). We aimed to include at least 250 patients. Given the explorative nature and novelty of the study, we performed no sample size calculation. However, since the aim of the study was to find out which parameters might be relevant for patients, we decided to use this broad approach in order to estimate effect sizes of associated parameters for future studies.
Besides descriptive statistics analyses for absolute and relative frequencies, observed numbers and means, we determined normal distributions using the Kolmogorov–Smirnov test and visual inspection of histograms. A subgroup analysis compared participants who provided positive statements to those who provided negative statements. Further subgroup analyses compared gender (male, female), and age categories (18–39 years, 40–65 years, and over 65 years old) (see Tables 1–3). The classification of the age categories was based on the model of Sender and Zabokrtsky, especially concerning younger patients (Sender and Zabokrtsky, 2015). To examine if a low energy level might interfere with initiating and maintaining lifestyle modifications, we divided patients into the following groups according to their perceived energy level (EL): low EL (0–3/10), medium EL (4–6/10), and high EL (7–10/10). In all calculations chi-square test was used to detect association and differences. The significance level was set at p < 0.05 for all tests (Bühl, 2019). Effect size was expressed by Phi coefficent (φ) and Cramers V to measure association between two variables. Subgroup analysis calculations primarily used 2 × 2 crosstabs for gender, 2 × 3 crosstabs for age, and 2 × 2 crosstabs for positive and negative statements. In few calculations larger crosstabs were used.
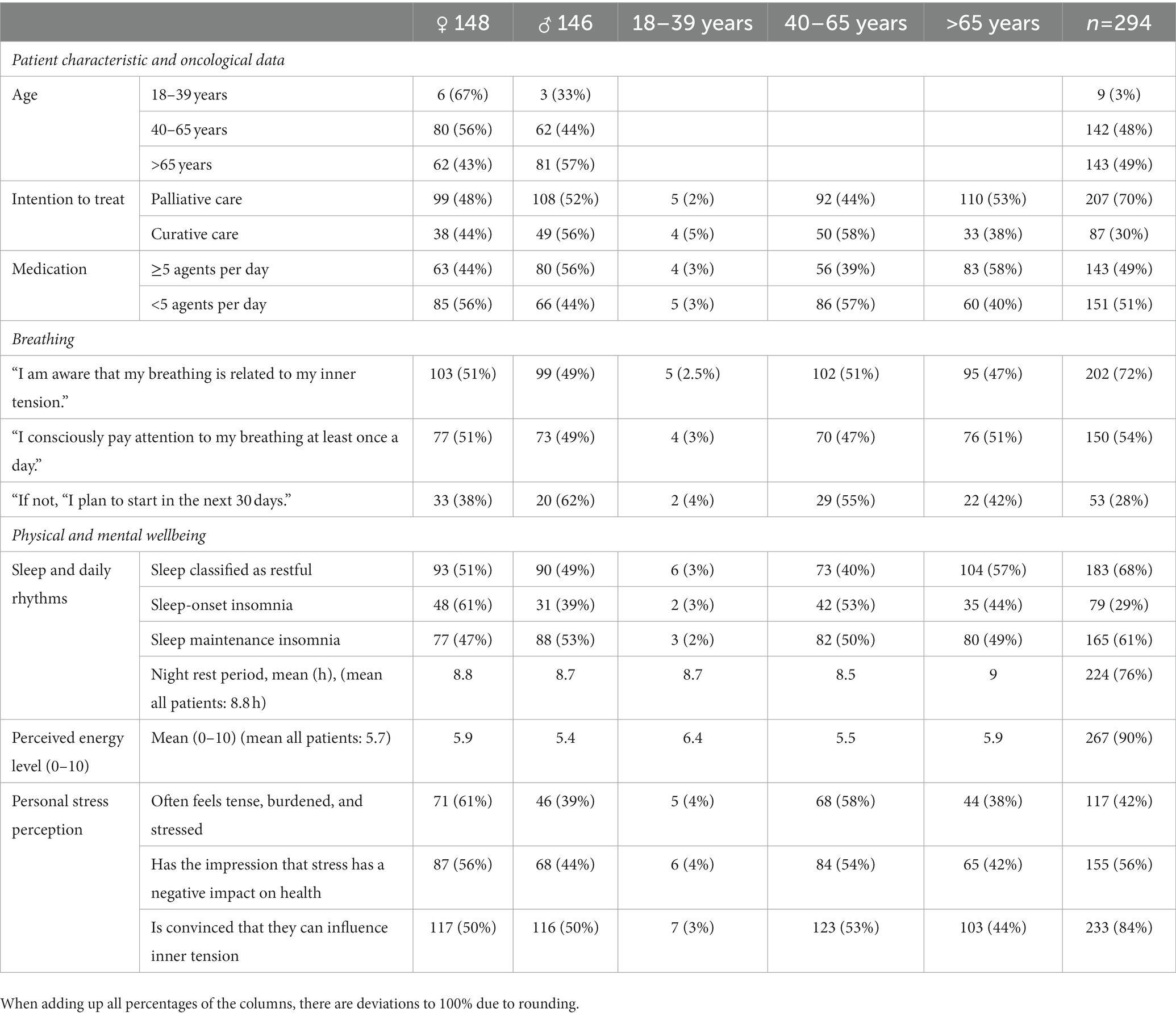
Table 1. Clinical characteristics of patients, oncological data, physical/mental wellbeing.
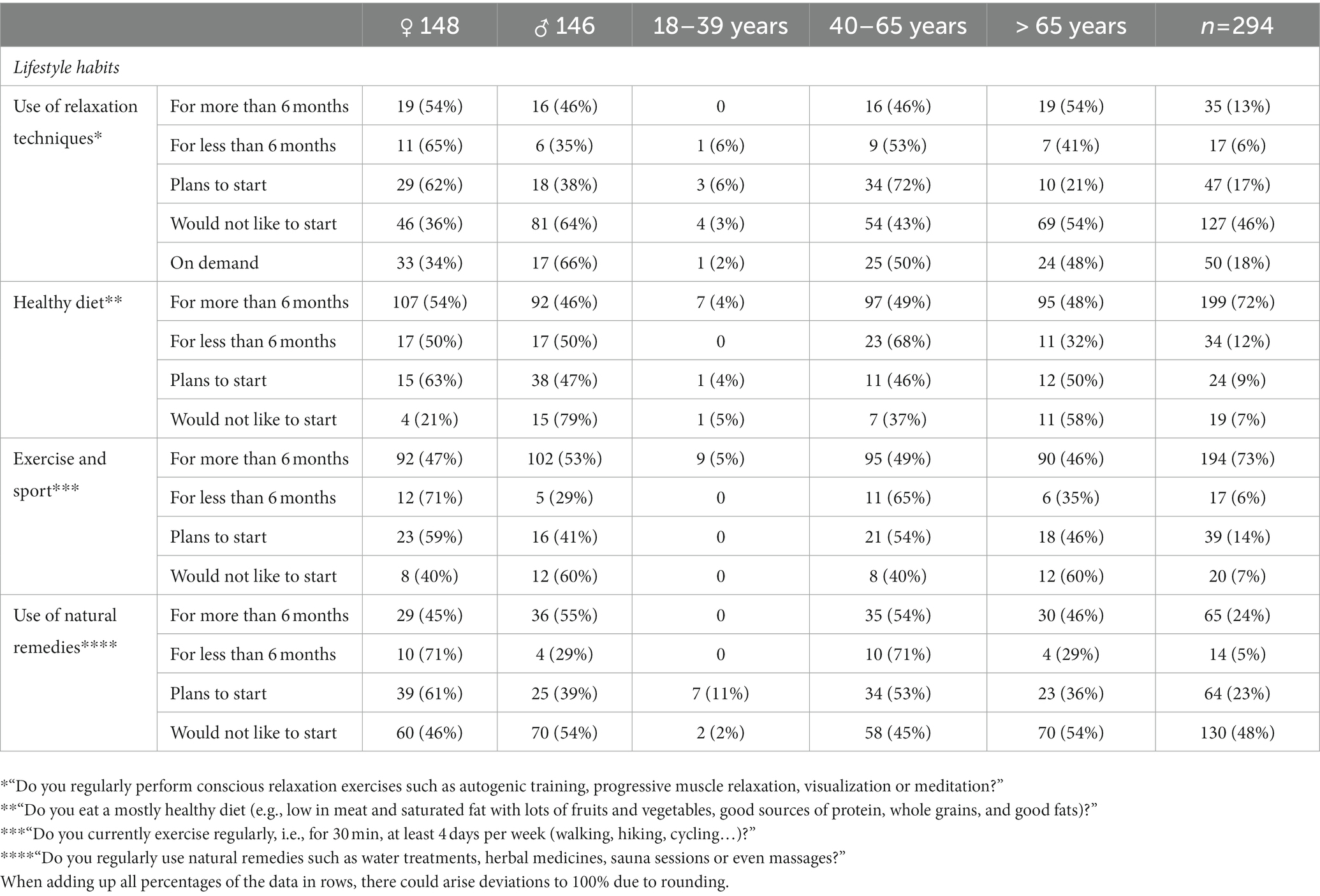
Table 2. Patients’ lifestyle habits: presentation of results comparatively between men and women, and comparatively between different age groups.
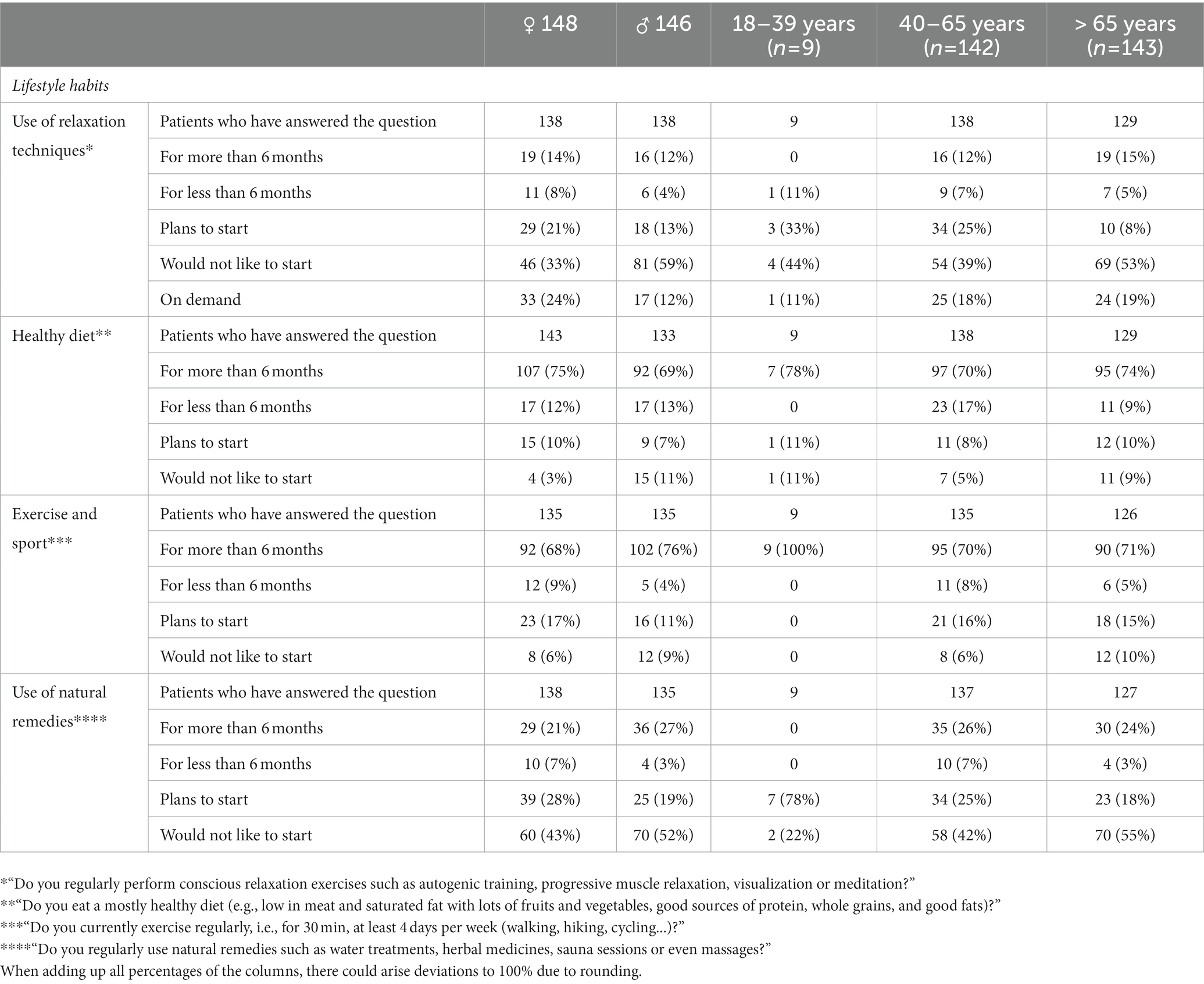
Table 3. Patients’ lifestyle habits: behavior change already implemented or intention to change behavior within each subgroup.
3. Results
3.1. Patient characteristics
A total of 294 patients with approximately equal numbers of women and men were surveyed. The mean age was 63.9 ± 11.9 years. Slightly less than half had hematological, one third gastrointestinal and less than one-fifth had gynecological malignancies (see Supplementary Table S1). Seventy percent (n = 207) were in palliative and 30% (n = 87) in curative therapy with a prospect of cure (Table 1).
3.2. Physical and mental wellbeing and lifestyle habits
Although more than half reported sleep-through disturbances (n = 165; 61%), the majority rated sleep quality as good and restful (n = 183; 68%). However, the perceived average daytime energy level was rated at 5.7 out of 10. Forty-two percent reported feeling tense and stressed frequently, with more than half rating this detrimental to their health. Although the majority reported being conscious of a connection between breathing and inner tension, only half of the patients paid attention to their breathing at least once a day and about one third were motivated to start within the next 30 days (Table 1). The vast majority felt well integrated into their social network of friends and family (n = 276, 96%), were confident they could rely on caregivers in challenging situations (n = 274, 98%) and enjoyed work/daily tasks (n = 244, 87%).
Two thirds (n = 187, 66%) reported they already had successful experiences with lifestyle changes in the past, although more than one third reported they had often quickly fallen back into bad habits (n = 95, 37%). Tables 1–3 illustrate reported mental and physical wellbeing, as well as health behaviors, and summarize the motivation for behavior change regarding various lifestyle habits.
Concerning physical activity, over half reported feeling physically limited due to their disease (n = 146, 52%). Although a total of 78% (n = 211) stated that they were physically active at least 4 days a week for 30 min each, patients notably reported particularly about increased everyday activities (n = 248, 88%) and only 30% (n = 85) stated in an additional question that they performed defined exercise programs. Furthermore, a relevant proportion equated relaxing activities, such as sleeping or reading, with structured relaxation techniques.
3.3. Health-promoting behavior by patient characteristics—thoughts, feelings, and attitudes
Depending on the current emotional/mental mind state, we analyzed differences regarding “sleep,” “personal stress perception,” and “successful lifestyle modification” (Figure 1). Chi-square test with 2 × 2 crosstabs was used. Patients who reported restful sleep were significantly less likely to feel tensed and stressed, less likely to think about their disease, less likely to feel that “life is unfair,” and more likely to enjoy their daily tasks. In addition, patients who felt less stressed were significantly more likely to identify with statements that indicate a more optimistic emotional alignment. In addition, an optimistic attitude was associated with significantly more positive experiences in terms of sustainable lifestyle changes.
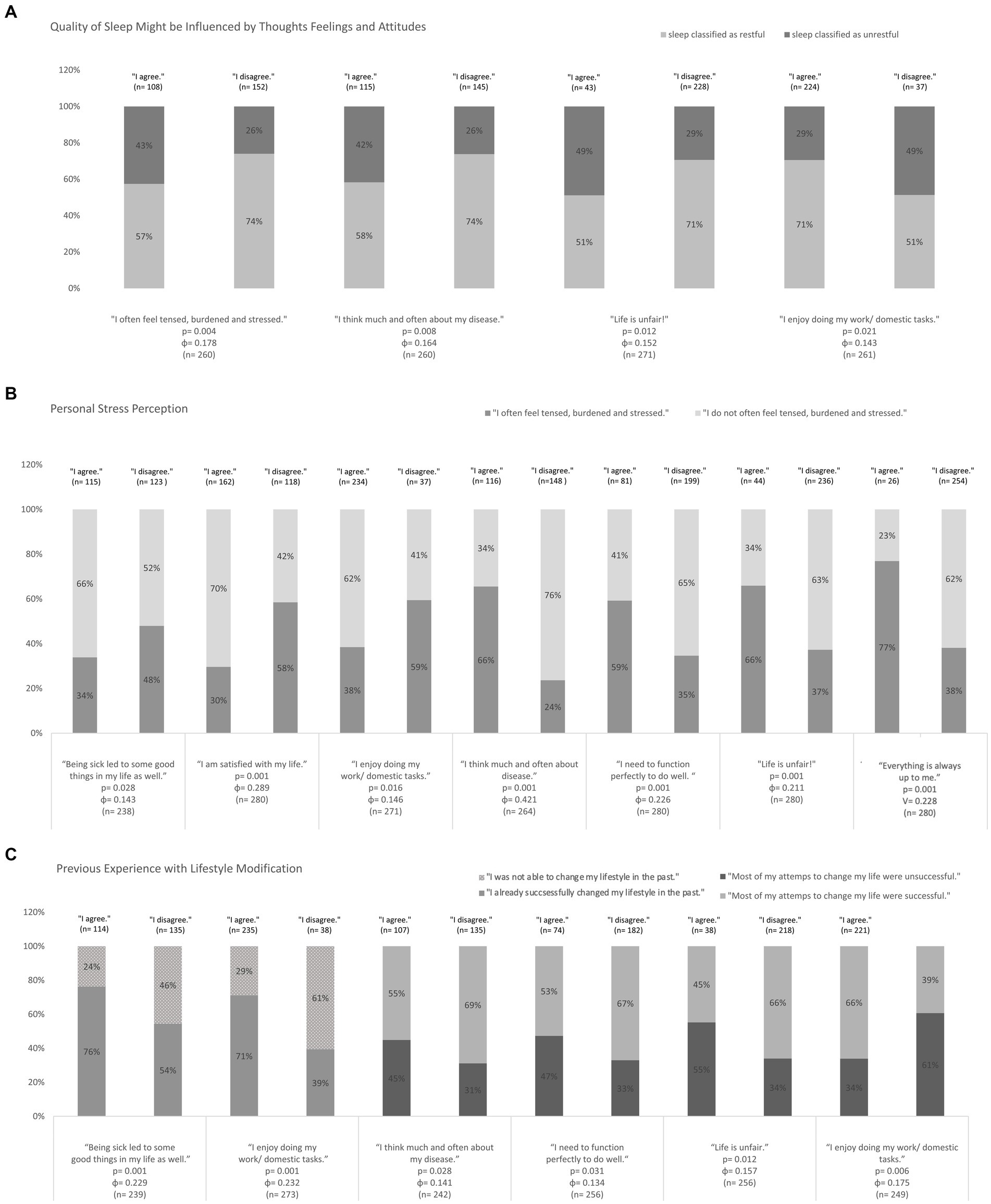
Figure 1. Influence of individual mindset on the variables of (A) sleep, (B) stress perception, and (C) experience with lifestyle modifications. Chi-square test were used, p-values and Phi-coefficient is given in the Diagramm (n indicates the number of patients, who have answered the question, respectively).
3.4. Health-promoting behavior by patient characteristics—gender and age
Significant findings were also achieved when looking at gender and age (Tables 1–3; Figure 2) using Chi-square tests. To analyze gender differences, we primarily used 2 × 2 crosstabs, regarding age we primarily used 2 × 3 crosstabs. We found a significant association between gender and use of relaxation techniques [x2(5) = 20.8, p < 0.001, V = 0.274]. Women were significantly more likely to feel stressed, more often concerned about their wellbeing regarding most lifestyle habits and more motivated to change behavior. They were significantly more interested in paying more attention to their breathing at least once a day in the next 30 days [x2(1) = 5.0, p = 0.025, ɸ = 0.163]. Furthermore, women were already twice as likely to use relaxation techniques and even three times as likely to use a relaxation technique in the next 30 days. However, significantly more women picked negative statements such as to “I think much and often about my disease” [1.4 times as often, x2(1) = 4.2, p = 0.041, ɸ = 0.123], “I always end up doing everything” [12 times as often, x2(1) = 20.1, p < 0.001, ɸ = 0.261] and “life is unfair” [twice as often, x2(1) = 7.8, p = 0.005, ɸ = 0,163]. More women than men could identify with the statement “sadness and pain are part of life, but there are always good times to follow” [1.3 times, x2(1) = 6.6, p = 0.01, ɸ = 0.151]. Regarding the variable age, we found significant differences concerning “sleep” [x2(2) = 12.2, p = 0.002, V = 0.212], “use of relaxation techniques” [x2(10) = 24.6, p = 0.002, V = 0.211], “exercise into daily activities” [x2(2) = 6.7, p = 0.038, V = 0.152] and “use of natural remedies” [x2(8) = 22.1, p = 0.007, V = 0.285]. The 40-65-year-olds reported significantly less restful sleep, more stress and were more dissatisfied with their own situation compared to the other age groups. This group already used natural remedies most frequently and was most often motivated to use relaxation techniques in the next 6 months. The older the patients, the less frequently they reported regular physical activity. The younger the patients, the more frequently they stated, “I always end up doing everything.”
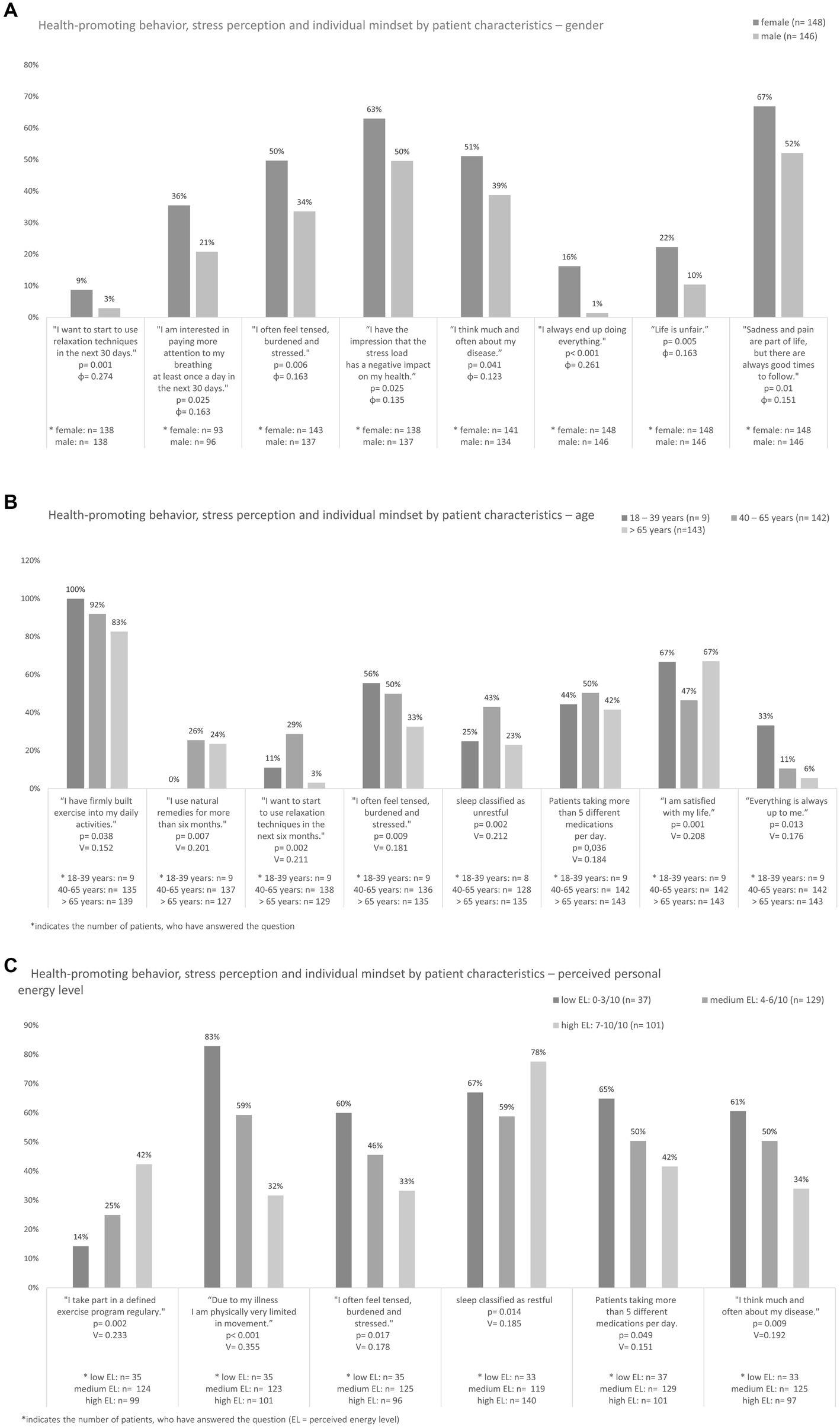
Figure 2. Health-promoting behavior by patient characteristics of (A) gender, (B) age, and (C) perceived personal energy level. Chi-square test was used, p-values and Cramers V or Phi-coefficient given in the Diagramm.
3.5. Health-promoting behavior by patient characteristics—perceived personal energy level
We found significant associations between the perceived personal energy level and the variables “sleep,” “exercise,” “personal stress perception” and “feeling, thoughts and attitudes” (Figure 2). Chi-square test and 2 × 3 crosstabs were primarily used. The higher the EL, the more often patients reported restful sleep [x2(2) = 8.6, p = 0.014, V = 0.185]. Moreover, patients with high EL were two times less likely to think about their disease [x2(2) = 9.4, p = 0.009, V = 0.192] and two times more likely to report being satisfied with their situation [x2(2) = 11.4, p = 0.003, V = 0.207]. The lower the EL, the less frequently patients were active in sports [x2(2) = 13.8, p = 0.002, V = 0.223], the more frequently they felt their disease impaired their activity [x2(2) = 32.7, p < 0.001, V = 0.355], and also felt stressed and tense most of the time [x2(2) = 8.1, p = 0.017, V = 0.178]. This patient group with the lower EL was significantly more likely to rely on more than 5 medications per day [x2(2) = 6.0, p = 0.049, V = 0.151].
4. Discussion
4.1. Physical and mental wellbeing and lifestyle habits: we should use the full potential of relaxation techniques such as breathing exercises
Two out of 5 patients reported feeling stressed regularly. This matches results of other studies that demonstrated an average up to 52% of patients feel limited by increased disease-associated stress (Zabora et al., 2001; Mehnert et al., 2018).
In the first months after a cancer diagnosis, studies have shown that both chronic and episodic stress are independent predictors of the increase in distressing physical symptoms such as pain and fatigue (Harris et al., 2017). Additionally, stress levels appear to be the strongest predictor of quality of life 2 years after diagnosis (Härtl et al., 2010). It is all the more striking that almost half of the patients do not yet use any relaxation techniques and reported no current interest in starting promptly, although 56% reported stress could have a negative effect on their health.
Oppegaard et al. (2021) could demonstrate impressively that anxiety profiles are associated with stress, resilience and symptom severity in outpatients receiving chemotherapy. A recent study examining the effects of a group-based integrative oncology program to build resilience and improve quality of life in cancer patients revealed that patients with anxiety and low initial resilience benefited most (Savaş et al., 2022). Regarding relaxation methods, breathing exercises play an important role as they are easy to learn and available ubiquitously. There is convincing evidence that concentrative breathing exercises contribute to improved stress regulation and can reduce anxiety (Jerath et al., 2015; Soni and Muniyandi, 2019). A majority (74%) was aware of the connection between breathing and inner tension, with only one third reporting they would like to focus more on their own breathing in the future. Especially informal quick exercise sessions, such as mindful awareness of breathing together with easy-to-follow explanations about the connections between breathing, stress, and physical wellbeing, should be in an integrative treatment program. Moreover, patients need to know that relaxing activities such as sleeping or even reading are not the same as structured relaxation techniques. Not to forget, it is important to encourage patients to discuss the use relaxation techniques/mind–body-based interventions with their care providers. Patients might not give information about use of mind–body medicine out of fear of physician criticism (Davis et al., 2012). On the other hand, the attitude of the physician could also have an influence on the attitude of the patients. There exists first evidence, that physician’s lifestyle might influence the prescription of healthy habits to breast cancer patients (Cangussú et al., 2022).
In addition, these results show that there is a considerable need not only for multimodal group services, but also for intensive psycho-oncological support in individual settings.
4.2. Patients need to perform more defined exercise programs
Our results showed that 52% of the respondents felt physically limited, despite regular physical activity which is recommended as being at least 30 min of moderate to intense aerobic activity three times a week and 20–30 min of resistance training twice a week (Campbell et al., 2019). Any kind of physical activity in everyday life also including defined exercise programs is important, especially to achieve the most important goal: avoiding physical inactivity (Campbell et al., 2019). But it seems that the duration and intensity of physical activity should have been higher for these patients to reduce physical limitation, especially since only 30% reported doing defined physical activity programs. Our results also showed patients with a low EL less likely to be physically active and more likely to feel impaired, stressed, and tense. In contrast, patients with a higher EL reported sleeping better, were more satisfied, and thought less about their illness. Therefore, patients should be directed to practice defined supervised physical activity programs to address specific needs and physical problems (Schmitz et al., 2019; Depenbusch et al., 2020). Oncologists play a significant role as the interface with the patient and should therefore regularly assess the patients’ current physical activity, advise them on their current and desired physical activity and communicate the importance of regular exercise. If this is not possible due to time constraints, they should at least refer patients to appropriate physical activity programs and/or exercise therapy professionals (Schmitz et al., 2019). A recent study has shown that physical exercise counseling in cancer patients has an impact on their physical activity and, depending on previous activity levels, directly related to higher physical activity after diagnosis (Depenbusch et al., 2020). In addition, compelling evidence exists for supervised exercise therapy compared to unsupervised interventions (Buffart et al., 2017). In conclusion, the least physicians can do is follow the so-called “call-to-action” (Schmitz et al., 2019).
4.3. Health-promoting behavior by patient characteristics—thoughts, feelings, and attitudes might influence health-promoting behavior
More than two-thirds of patients had reported positive experiences with lifestyle modifications, but 37% indicated they had often quickly fallen back into bad habits.
Behavior change is easier to maintain if achievable goals are chosen and the person is confident they have good resources to achieve them. Life experiences and personal core values can influence how people react in difficult situations and particularly how patients come to terms with their disease (Savioni and Triberti, 2020; Sevild et al., 2020). We therefore hypothesized that individual mindset at the time of the survey may have influenced how stressed and burdened patients felt and their motivation to change their behavior (Bandura, 1982; Ashford et al., 2010). Patients indicating a more optimistic emotional alignment were significantly more likely to report successful and sustainable lifestyle modifications compared to patients with a presumably more pessimistic mindset. Moreover, patients who felt pleasure in their daily tasks and reported thinking less often about their disease were significantly less likely to feel life was unfair and to experience sleep disturbances (Roberts and Duong, 2014; Wang et al., 2015; Scott et al., 2021). Although we found an association between patients’ satisfaction with their own situation and their perceived stress level, this patient group was also significantly more likely to report already regularly practicing relaxation techniques including perceptions and patterns of evaluation. Mindfulness, for example, means non-judgmental awareness of the present moment. Studies have demonstrated the effect of regular relaxation and mindfulness practice on stress, satisfaction and gratitude (Hoffman et al., 2012; Cramer et al., 2013; Love et al., 2019; Norelli et al., 2022). Additionally, there is convincing evidence that mindfulness-based interventions and especially integrative day-care programs focusing on MBM may benefit patients with anxiety and depressiveness (Witt et al., 2015; Haller et al., 2017; Jin et al., 2019; Li et al., 2019; Parmentier et al., 2019). Since approximately one third of cancer patients suffers from depressiveness, Mind–Body procedures should be encouraged early, especially for patients who are more likely to identify with pessimistic thoughts (Krebber et al., 2014). In addition, it also makes sense to use the resource of psycho-oncological counseling even more, e.g., focusing on cognitive biases and behavioral therapy approaches.
4.4. Gender-specific differences require adapted support
As observed in other studies, women were significantly more motivated to change their lifestyle habits (Verhoef et al., 2005; Voiß et al., 2019). However, another important finding was that especially women felt stressed significantly more often and were also concerned that this could have a negative impact on their health. Other studies provide similar results (Bergerot et al., 2015; Fischer et al., 2022). Women were also able to identify significantly more often with rather pessimistic statements and reported with alarming frequency that they often feel “everything was up to them.” Other studies also show that, e.g., breast cancer patients feel insufficiently supported in their social networks and that younger female patients particularly suffered more frequently from depression and anxiety (Linden et al., 2012). We therefore hypothesize that this patient group could particularly benefit from interventions oriented toward behavioral therapy, supporting the cultivation of a positive mindset, but also from socio-medical counseling (Salakari et al., 2017; Sousa Rodrigues Guedes et al., 2020; Zainal et al., 2021). Evidence for both single interventions and multimodal programs continues to grow (Latte-Naor and Mao, 2019). However, we assume that particularly women could especially benefit from multimodal approaches, e.g., a day clinic, as they are confronted with special challenges due to their different roles: family, work and society. Moreover, these results indicate the importance of psycho-oncological interventions that focus on individual resources, behavioral change and support patients to take care of themselves and their limits (e.g., with mindfulness-based strategies). An expansion of supportive integrative medical services could thus have a positive impact both on individuals themselves and on their environment.
4.5. There is need for programs tailored to the needs of different age groups
This study demonstrated that more than half of the patients were affected by sleep-through disturbance. This matches results recently published by Voiss et al. for cancer survivors with up to 60% suffering from sleep problems and studies focusing on patients under treatment which found insomnia symptoms in up to 59% of cancer patients (Palesh et al., 2010; Savard et al., 2011; Voiss et al., 2019). In our study, the group aged 40–65 was most frequently affected by sleep disorders. Strikingly this age group also reported feeling stressed and dissatisfied with their own situation much more often. We also found an association between sleep disturbances and perceived personal energy level. It is comprehensible that poor nighttime sleep could be related to reduce wellbeing during the day, from increased feelings of stress up to increased susceptibility to depression. Several studies (Savard et al., 2011; Irwin et al., 2013; Lee et al., 2022) have already demonstrated this.
On the other hand, this age group reported the greatest motivation to learn a relaxation technique in the next 6 months and most frequently used self-care strategies and natural remedies for symptom relief. We hypothesize that the group of 40–65-year-olds might be affected in a special way due to, e.g., financial worries, future career and family responsibilities. Being confronted with a life-threatening disease in the most productive years of their lives could be a strong motivation to leaving no stone unturned to work toward the most positive further course possible. To our knowledge, there are some well-evaluated programs that include this age group (Faller et al., 2013), but none that are tailored to address the specific problems of this highly motivated age group in a personalized way.
4.6. Limitations of the study
The results must nevertheless be interpreted carefully. First, due to restrictions during the pandemic, we did not succeed in recruiting a representative patient population with respect to the frequencies of the entities as originally planned. Therefore, the distribution of disease sites of the participants is not representative of cancer incidence across sites. Thus, the findings are only representative of the groups sample and generalizability is limited.
Second, we used a custom-developed questionnaire based on a German Mind–Body Medicine Day Care Clinic program. This questionnaire was not validated. Third, the study question was very ambitious and this was at the same time a limitation of the study, as parameters relevant for patients were mixed with parameters relevant for the provider. However, the study approach was deliberately chosen to be very open and multifaceted, as this study may be understood from a clinical perspective as a screening for not yet sufficiently addressed needs of patients to become aware and thus has an exploratory character. For this reason, no hypotheses were formed, so that the subgroup analyses, for which a case number calculation based on hypotheses would actually be desirable, must be interpreted with caution and the results from this should only serve as an initial orientation for follow-up studies.
Agreement on pessimistic or optimistic thoughts does provide a mood picture. However, we cannot exclude the possibility that some patients were perhaps suffering, e.g., from an undiagnosed anxiety disorder or depression. Therefore, the statements used can only be understood as screening, and patients with a more pessimistic response behavior should be tested for psychological comorbidities using standardized instruments. Furthermore, the statements represent snapshots and, depending on the current individual situation, the results may also fluctuate in the short term so that longitudinal assessments should be more reliable for follow-up studies and in routine practice. Follow-up studies should optimally include more patients aged <39 years. Furthermore, a better differentiation must be made between patients with chronic course and patients with limited survival in the large group of palliative patients since these two groups are likely to differ significantly in symptom burden and needs.
Some patients abandoned the questionnaire, explaining it was too time-consuming. The effort required to complete the questionnaire may have led to more open-minded patients agreeing to participate. No data was collected on this. Furthermore, the impact of patients answering questions according to the principle of social desirability remains unclear.
4.7. Conclusion
To conclude, interventions and programs focusing on Mind–Body techniques, patient’s individual resources, with tools to explore impairing patterns of self-perception and cognitive biases, can be a valuable resource for oncology patients and should therefore be part of an integrative medical treatment concept. Especially for women and patients aged between 40 and 65 appropriately tailored programs would be reasonable regarding their special stress situation. Due to the demonstrated relations between a patient’s thoughts, feelings, and attitudes on the one hand and motivation for behavior change on the other hand, patients can also benefit from the sustainable implementation of a healthy lifestyle.
Data availability statement
The original contributions presented in the study are included in the article/ Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethics Committee of the Julius-Maximilian-University Wuerzburg on 15 April 2019 (study number 12/19-me). The patients/participants provided their written informed consent to participate in this study.
Author contributions
CL and HE contributed to the study concept. JL, MW, LS, and AK contributed to the methodology. JL and CL were responsible for the formal analysis, drafted the manuscript, and carried out the investigation. MW, AK, LS, AQ, and HE critically reviewed and edited the manuscript. JL contributed to the data curation and visualization of the data. HE contributed to the supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This publication was supported by the Open Access Publication Fund of the University of Wuerzburg.
Acknowledgments
Statistical support was provided by the Statistical Consulting Office, Institute of Epidemiology and Biometrics, Julius Maximilian University of Würzburg. We sincerely thank Elizabeth Morris for editing and proofreading to again significantly improve our manuscript. We would also like to thank Dr. Sascha Schäuble from the Leibniz-HKI in Jena for his advice and support in the statistical analysis and presentation.
Conflict of interest
CL: lecture fees from Celgene GmbH, Roche GmbH, Novartis Pharma GmbH, BMS GmbH & Co. KGaA, Mundipharma GmbH Co. KG, Merck KGaA.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2023.1140693/full#supplementary-material
References
Ashford, S., Edmunds, J., and French, D. P. (2010). What is the best way to change self-efficacy to promote lifestyle and recreational physical activity? A systematic review with meta-analysis. Br. J. Health Psychol. 15, 265–288. doi: 10.1348/135910709X461752
Bandura, A. (1982). Self-efficacy mechanism in human agency. Am. Psychol. 37, 122–147. doi: 10.1037/0003-066X.37.2.122
Bergerot, C. D., Clark, K. L., Nonino, A., Waliany, S., Buso, M. M., and Loscalzo, M. (2015). Course of distress, anxiety, and depression in hematological cancer patients: association between gender and grade of neoplasm. Palliat. Support. Care 13, 115–123. doi: 10.1017/S1478951513000849
Boon, H., Brown, J. B., Gavin, A., and Westlake, K. (2003). Men with prostate cancer: making decisions about complementary/alternative medicine. Med. Decis. Mak. 23, 471–479. doi: 10.1177/0272989X03259815
Buffart, L. M., Kalter, J., Sweegers, M. G., Courneya, K. S., Newton, R. U., Aaronson, N. K., et al. (2017). Effects and moderators of exercise on quality of life and physical function in patients with cancer: an individual patient data meta-analysis of 34 RCTs. Cancer Treat. Rev. 52, 91–104. doi: 10.1016/j.ctrv.2016.11.010
Bühl, A. SPSS: Einführung in die moderne Datenanalyse ab SPSS 25. 16., aktualisierte Auflage. Hallbergmoos: Pearson; (2019). (Pearson Studium - Scientific Tools).
Campbell, K. L., Winters-Stone, K. M., Wiskemann, J., May, A. M., Schwartz, A. L., Courneya, K. S., et al. (2019). Exercise guidelines for Cancer survivors: consensus statement from international multidisciplinary roundtable. Med. Sci. Sports Exerc. 51, 2375–2390. doi: 10.1249/MSS.0000000000002116
Cangussú, R., Mascarenhas, E., Rebelatto, T. F., Zaffaroni, F., de Jesus, R. G., Filho, P. R. N., et al. (2022). Influence of physician's lifestyle on the prescription of healthy habits to breast cancer patients (LACOG 1218). Support Care Cancer 30, 4399–4406. doi: 10.1007/s00520-022-06864-3
Cramer, H., Lauche, R., Langhorst, J., Dobos, G., and Paul, A. (2013). Characteristics of patients with internal diseases who use relaxation techniques as a coping strategy. Complement. Ther. Med. 21, 481–486. doi: 10.1016/j.ctim.2013.08.001
Davidson, J. R., MacLean, A. W., Brundage, M. D., and Schulze, K. (2002). Sleep disturbance in cancer patients. Soc. Sci. Med. 54, 1309–1321. doi: 10.1016/S0277-9536(01)00043-0
Davis, E. L., Oh, B., Butow, P. N., Mullan, B. A., and Clarke, S. (2012). Cancer patient disclosure and patient-doctor communication of complementary and alternative medicine use: a systematic review. Oncologist 17, 1475–1481. doi: 10.1634/theoncologist.2012-0223
Deng, G. E., Rausch, S. M., Jones, L. W., Gulati, A., Kumar, N. B., Greenlee, H., et al. (2013). Complementary therapies and integrative medicine in lung cancer. Chest 143, e420S–e436S. doi: 10.1378/chest.12-2364
Depenbusch, J., Haussmann, A., Tsiouris, A., Schmidt, L., Wiskemann, J., Ungar, N., et al. (2020). The association between physicians' exercise counseling and physical activity in patients with cancer: which roles do patients' satisfaction and previous physical activity levels play? Psychooncology 29, 1856–1863. doi: 10.1002/pon.5506
Deutsche Krebsgesellschaft. S3-Leitline Komplementärmedizin in der Behandlung von onkologischen patienten (2021). Available at: https://www.awmf.org/leitlinien/detail/ll/032-055OL.html.
Dobos, G., Overhamm, T., Büssing, A., Ostermann, T., Langhorst, J., Kümmel, S., et al. (2015). Integrating mindfulness in supportive cancer care: a cohort study on a mindfulness-based day care clinic for cancer survivors. Support Care Cancer 23, 2945–2955. doi: 10.1007/s00520-015-2660-6
Esch, T., and Stefano, G. B. (2022). The BERN framework of mind-body medicine: integrating self-care, health promotion, resilience, and applied neuroscience. Front. Integr. Neurosci. 16:913573. doi: 10.3389/fnint.2022.913573
Evans, M. A., Shaw, A. R. G., Sharp, D. J., Thompson, E. A., Falk, S., Turton, P., et al. (2007). Men with cancer: is their use of complementary and alternative medicine a response to needs unmet by conventional care? Eur. J. Cancer Care 16, 517–525. doi: 10.1111/j.1365-2354.2007.00786.x
Faller, H., Schuler, M., Richard, M., Heckl, U., Weis, J., and Küffner, R. (2013). Effects of psycho-oncologic interventions on emotional distress and quality of life in adult patients with cancer: systematic review and meta-analysis. J. Clin. Oncol. 31, 782–793. doi: 10.1200/JCO.2011.40.8922
Fischer, J., Knop, S., Danhof, S., Einsele, H., Keller, D., and Löffler, C. (2022). The influence of baseline characteristics, treatment and depression on health-related quality of life in patients with multiple myeloma: a prospective observational study. BMC Cancer 22:1032. doi: 10.1186/s12885-022-10101-9
Fjær, E. L., Landet, E. R., McNamara, C. L., and Eikemo, T. A. (2020). The use of complementary and alternative medicine (CAM) in Europe. BMC Complement Med Ther 20:108. doi: 10.1186/s12906-020-02903-w
Greenlee, H., DuPont-Reyes, M. J., Balneaves, L. G., Carlson, L. E., Cohen, M. R., Deng, G., et al. (2017). Clinical practice guidelines on the evidence-based use of integrative therapies during and after breast cancer treatment. CA Cancer J. Clin. 67, 194–232. doi: 10.3322/caac.21397
Haller, H., Winkler, M. M., Klose, P., Dobos, G., Kümmel, S., and Cramer, H. (2017). Mindfulness-based interventions for women with breast cancer: an updated systematic review and meta-analysis. Acta Oncol. 56, 1665–1676. doi: 10.1080/0284186X.2017.1342862
Harris, L. N., Bauer, M. R., Wiley, J. F., Hammen, C., Krull, J. L., Crespi, C. M., et al. (2017). Chronic and episodic stress predict physical symptom bother following breast cancer diagnosis. J. Behav. Med. 40, 875–885. doi: 10.1007/s10865-017-9855-x
Härtl, K., Engel, J., Herschbach, P., Reinecker, H., Sommer, H., and Friese, K. (2010). Personality traits and psychosocial stress: quality of life over 2 years following breast cancer diagnosis and psychological impact factors. Psychooncology 19, 160–169. doi: 10.1002/pon.1536
Hoffman, C. J., Ersser, S. J., Hopkinson, J. B., Nicholls, P. G., Harrington, J. E., and Thomas, P. W. (2012). Effectiveness of mindfulness-based stress reduction in mood, breast- and endocrine-related quality of life, and well-being in stage 0 to III breast cancer: a randomized, controlled trial. J. Clin. Oncol. 30, 1335–1342. doi: 10.1200/JCO.2010.34.0331
Huebner, J., Micke, O., Muecke, R., Buentzel, J., Prott, F. J., Kleeberg, U., et al. (2014). User rate of complementary and alternative medicine (CAM) of patients visiting a counseling facility for CAM of a German comprehensive cancer center. Anticancer Res. 34, 943–948.
Irwin, M. R., Olmstead, R. E., Ganz, P. A., and Haque, R. (2013). Sleep disturbance, inflammation and depression risk in cancer survivors. Brain Behav. Immun. 30, S58–S67. doi: 10.1016/j.bbi.2012.05.002
Jeitler, M., Jaspers, J., von Scheidt, C., Koch, B., Michalsen, A., Steckhan, N., et al. (2017). Mind-body medicine and lifestyle modification in supportive cancer care: a cohort study on a day care clinic program for cancer patients. Psychooncology 26, 2127–2134. doi: 10.1002/pon.4433
Jerath, R., Crawford, M. W., Barnes, V. A., and Harden, K. (2015). Self-regulation of breathing as a primary treatment for anxiety. Appl. Psychophysiol. Biofeedback 40, 107–115. doi: 10.1007/s10484-015-9279-8
Jin, X., Wang, L., Liu, S., Zhu, L., Loprinzi, P. D., and Fan, X. (2019). The impact of mind-body exercises on motor function, depressive symptoms, and quality of life in Parkinson's disease: a systematic review and meta-analysis. Int. J. Environ. Res. Public Health 17:31. doi: 10.3390/ijerph17010031
Kabat-Zinn, J. (1982). An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: theoretical considerations and preliminary results. Gen. Hosp. Psychiatry 4, 33–47. doi: 10.1016/0163-8343(82)90026-3
Kabat-Zinn, J. Full catastrophe living: Using the wisdom of your body and mind to face stress, pain, and illness. New York, NY: Delta Trade Paperback/Bantam Dell (1990).
Kemppainen, L. M., Kemppainen, T. T., Reippainen, J. A., Salmenniemi, S. T., and Vuolanto, P. H. (2018). Use of complementary and alternative medicine in Europe: health-related and sociodemographic determinants. Scand. J. Public Health 46, 448–455. doi: 10.1177/1403494817733869
Klafke, N., Eliott, J. A., Olver, I. N., and Wittert, G. A. (2014). Australian men with cancer practice complementary therapies (CTs) as a coping strategy. Psychooncology 23, 1236–1242. doi: 10.1002/pon.3550
Krebber, A. M. H., Buffart, L. M., Kleijn, G., Riepma, I. C., Bree, R., Leemans, C. R., et al. (2014). Prevalence of depression in cancer patients: a meta-analysis of diagnostic interviews and self-report instruments. Psychooncology 23, 121–130. doi: 10.1002/pon.3409
Latte-Naor, S., and Mao, J. J. (2019). Putting integrative oncology into practice: concepts and approaches. J. Oncol. Pract. 15, 7–14. doi: 10.1200/JOP.18.00554
Lederer, A.-K., Baginski, A., Raab, L., Joos, S., Valentini, J., Klocke, C., et al. (2021). Complementary medicine in Germany: a multi-centre cross-sectional survey on the usage by and the needs of patients hospitalized in university medical centers. BMC Complement Med Ther 21:285. doi: 10.1186/s12906-021-03460-6
Lee, S., Ryu, S., Lee, G. E., Kawachi, I., Morey, B. N., and Slopen, N. (2022). The association of acculturative stress with self-reported sleep disturbance and sleep duration among Asian Americans. Sleep 45:zsab298. doi: 10.1093/sleep/zsab298
Li, Z., Liu, S., Wang, L., and Smith, L. (2019). Mind-body exercise for anxiety and depression in COPD patients: a systematic review and meta-analysis. Int. J. Environ. Res. Public Health 17:22. doi: 10.3390/ijerph17010022
Linden, W., Vodermaier, A., Mackenzie, R., and Greig, D. (2012). Anxiety and depression after cancer diagnosis: prevalence rates by cancer type, gender, and age. J. Affect. Disord. 141, 343–351. doi: 10.1016/j.jad.2012.03.025
Love, M. F., Sharrief, A., Chaoul, A., Savitz, S., and Beauchamp, J. E. S. (2019). Mind-body interventions, psychological stressors, and quality of life in stroke survivors. Stroke 50, 434–440. doi: 10.1161/STROKEAHA.118.021150
Mehnert, A., Hartung, T. J., Friedrich, M., Vehling, S., Brähler, E., Härter, M., et al. (2018). One in two cancer patients is significantly distressed: prevalence and indicators of distress. Psychooncology 27, 75–82. doi: 10.1002/pon.4464
Mittelmark, M. B., Lindström, B., Bauer, G. F., Espnes, G. A., Pelikan, J. M., Eriksson, M., et al. (2017). “Aaron Antonovsky’s development of salutogenesis, 1979 to 1994,” in The handbook of salutogenesis. eds. M. B. Mittelmark, S. Sagy and M. Eriksson (Cham: Springer), 25–40.
Norelli, S. K., Long, A., and Krepps, J. M. (2022). StatPearls: relaxation techniques. Treasure Island, FL: StatPearls Publishing.
Oppegaard, K., Harris, C. S., Shin, J., Paul, S. M., Cooper, B. A., Levine, J. D., et al. (2021). Anxiety profiles are associated with stress, resilience and symptom severity in outpatients receiving chemotherapy. Support Care Cancer 29, 7825–7836. doi: 10.1007/s00520-021-06372-w
Palesh, O. G., Roscoe, J. A., Mustian, K. M., Roth, T., Savard, J., Ancoli-Israel, S., et al. (2010). Prevalence, demographics, and psychological associations of sleep disruption in patients with cancer: University of Rochester Cancer Center-Community Clinical Oncology Program. J. Clin. Oncol. 28, 292–298. doi: 10.1200/JCO.2009.22.5011
Parmentier, F. B. R., García-Toro, M., García-Campayo, J., Yañez, A. M., Andrés, P., and Gili, M. (2019). Mindfulness and symptoms of depression and anxiety in the general population: the mediating roles of worry, rumination, reappraisal and suppression. Front. Psychol. 10:506. doi: 10.3389/fpsyg.2019.00506
Paul, A., Cramer, H., Lauche, R., Altner, N., Langhorst, J., and Dobos, G. J. (2013). An oncology mind-body medicine day care clinic: concept and case presentation. Integr. Cancer Ther. 12, 503–507. doi: 10.1177/1534735412473639
Roberts, R. E., and Duong, H. T. (2014). The prospective association between sleep deprivation and depression among adolescents. Sleep 37, 239–244. doi: 10.5665/sleep.3388
Salakari, M., Pylkkänen, L., Sillanmäki, L., Nurminen, R., Rautava, P., Koskenvuo, M., et al. (2017). Social support and breast cancer: a comparatory study of breast cancer survivors, women with mental depression, women with hypertension and healthy female controls. Breast 35, 85–90. doi: 10.1016/j.breast.2017.06.017
Savard, J., Ivers, H., Villa, J., Caplette-Gingras, A., and Morin, C. M. (2011). Natural course of insomnia comorbid with cancer: an 18-month longitudinal study. J. Clin. Oncol. 29, 3580–3586. doi: 10.1200/JCO.2010.33.2247
Savaş, B. B., Märtens, B., Cramer, H., Voiss, P., Longolius, J., Weiser, A., et al. (2022). Effects of an interdisciplinary integrative oncology group-based program to strengthen resilience and improve quality of life in cancer patients: results of a prospective longitudinal single-center study. Integr. Cancer Ther. 21:153473542210817. doi: 10.1177/15347354221081770
Savioni, L., and Triberti, S. (2020). Cognitive biases in chronic illness and their impact on patients' commitment. Front. Psychol. 11:579455. doi: 10.3389/fpsyg.2020.579455
Schmitz, K. H., Campbell, A. M., Stuiver, M. M., Pinto, B. M., Schwartz, A. L., Morris, G. S., et al. (2019). Exercise is medicine in oncology: engaging clinicians to help patients move through cancer. CA Cancer J. Clin. 69, 468–484. doi: 10.3322/caac.21579
Scott, A. J., Webb, T. L., Martyn-St James, M., Rowse, G., and Weich, S. (2021). Improving sleep quality leads to better mental health: a meta-analysis of randomised controlled trials. Sleep Med. Rev. 60:101556. doi: 10.1016/j.smrv.2021.101556
Sender, L., and Zabokrtsky, K. B. (2015). Adolescent and young adult patients with cancer: a milieu of unique features. Nat. Rev. Clin. Oncol. 12, 465–480. doi: 10.1038/nrclinonc.2015.92
Sevild, C. H., Niemiec, C. P., Bru, L. E., Dyrstad, S. M., and Husebø, A. M. L. (2020). Initiation and maintenance of lifestyle changes among participants in a healthy life centre: a qualitative study. BMC Public Health 20:1006. doi: 10.1186/s12889-020-09111-8
Soni, R., and Muniyandi, M. (2019). Breath rate variability: a novel measure to study the meditation effects. Int J Yoga 12, 45–54. doi: 10.4103/ijoy.IJOY_27_17
Sousa Rodrigues Guedes, T., da Silva Barros C, C. P., Dantas de Oliveira, N. P., Martins Holanda, A., Albuquerque Reis, M., Silva BL, R. E., et al. (2020). Social support in the healthcare of women submitted to breast cancer treatment. Women Health 60, 899–911. doi: 10.1080/03630242.2020.1767263
Verhoef, M. J., Balneaves, L. G., Boon, H. S., and Vroegindewey, A. (2005). Reasons for and characteristics associated with complementary and alternative medicine use among adult cancer patients: a systematic review. Integr. Cancer Ther. 4, 274–286. doi: 10.1177/1534735405282361
Voiß, P., Höxtermann, M. D., Dobos, G., and Cramer, H. (2020). Mind-body medicine use by women diagnosed with breast cancer: results of a nationally representative survey. Support Care Cancer 28, 1077–1082. doi: 10.1007/s00520-019-04914-x
Voiß, P., Höxtermann, M. D., Dobos, G., and Cramer, H. (2019). The use of mind-body medicine among US individuals with sleep problems: analysis of the 2017 National Health Interview Survey data. Sleep Med. 56, 151–156. doi: 10.1016/j.sleep.2019.01.008
Voiss, P., Höxtermann, M. D., Dobos, G., and Cramer, H. (2019). Cancer, sleep problems, and mind-body medicine use: results of the 2017 National Health Interview Survey. Cancer 125, 4490–4497. doi: 10.1002/cncr.32469
Wang, Y.-Q., Li, R., Zhang, M.-Q., Zhang, Z., Qu, W.-M., and Huang, Z.-L. (2015). The neurobiological mechanisms and treatments of REM sleep disturbances in depression. Curr. Neuropharmacol. 13, 543–553. doi: 10.2174/1570159X13666150310002540
Witt, C. M., Außerer, O., Baier, S., Heidegger, H., Icke, K., Mayr, O., et al. (2015). Effectiveness of an additional individualized multi-component complementary medicine treatment on health-related quality of life in breast cancer patients: a pragmatic randomized trial. Breast Cancer Res. Treat. 149, 449–460. doi: 10.1007/s10549-014-3249-3
Witt, C. M., Balneaves, L. G., Cardoso, M. J., Cohen, L., Greenlee, H., Johnstone, P., et al. (2017). A comprehensive definition for integrative oncology. J. Natl. Cancer Inst. Monogr. 2017:7. doi: 10.1093/jncimonographs/lgx012
Zabora, J., BrintzenhofeSzoc, K., Curbow, B., Hooker, C., and Piantadosi, S. (2001). The prevalence of psychological distress by cancer site. Psychooncology 10, 19–28. doi: 10.1002/1099-1611(200101/02)10:1<19::AID-PON501>3.0.CO;2-6
Keywords: lifestyle habits, symptom burden, individual mind state, motivational level, stress
Citation: Leonhardt J, Winkler M, Kollikowski A, Schiffmann L, Quenzer A, Einsele H and Löffler C (2023) Mind–body-medicine in oncology—from patient needs to tailored programs and interventions: a cross-sectional study. Front. Psychol. 14:1140693. doi: 10.3389/fpsyg.2023.1140693
Edited by:
Michael Jeitler, Charité University Medicine Berlin, GermanyReviewed by:
Christina Sauer, Heidelberg University Hospital, GermanyUte Goerling, Charité University Medicine Berlin, GermanyCopyright © 2023 Leonhardt, Winkler, Kollikowski, Schiffmann, Quenzer, Einsele and Löffler. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Claudia Löffler, Loeffler_C@ukw.de