 Marta Torra Moreno
Marta Torra Moreno Josefa Canals Sans
Josefa Canals Sans Maria Teresa Colomina Fosch
Maria Teresa Colomina Fosch- 1Jeroni de Moragas Private Fundation, Tarragona, Spain
- 2Jeroni de Moragas Association, Tarragona, Spain
- 3Department of Psychology, Research Center for Behavioral Assessment (CRAMC), Rovira i Virgili University, Tarragona, Spain
- 4Research Group in Neurobehavior and Health (NEUROLAB), Tarragona, Spain
In recent years, digital devices have been progressively introduced in rehabilitation programs and have affected skills training methods used with children and adolescents with intellectual disabilities (ID). The objective of this review is to assess the effects of the use of digital devices on the cognitive functions and behavioral skills in this population, and to acknowledge their potential as a therapeutic tool. Electronic databases were analyzed until February 2020 using search formulas with free terms related to ID and the use of digital systems with children or adolescents. The risk of bias in randomized controlled trials was assessed by means of the modified Cochrane Collaboration tool and the quality level of the non-randomized studies was assessed using the Newcastle-Ottawa Scale. Forty-four studies were analyzed, most of which were categorized as low quality. Of the executive function studies analyzed, 60% reported significant improvements, most commonly related to working memory. Within the cognitive skills, 47% of the studies analyzed reported significant improvements, 30% of them in language. Significant improvements in the social (50%) and behavioral domains (30%) were also reported. These results suggest that digital interventions are effective in improving working memory and academic skills, and positively affect both the social and behavioral domains. Little information has been published regarding the duration of the effects, which could be limited in time. Further research is necessary to assess long-term effectiveness, the influence of comorbidities, and the effects on subjects with severe ID. The inclusion of smartphones and special education centers is also necessary.
Introduction
The Diagnostic and Statistical Manual of the American Psychiatric Association, Fifth Edition (DSM-5) (1), defines the concept of “intellectual disability” (ID) as a “disorder that begins during the developmental period and it includes limitations in intellectual functioning and also adaptive behavior in the conceptual, social and practical domains.” The meta-analysis of McKenzie et al. (2) reported a prevalence of intellectual disability of somewhat <1%, but more recent studies have reported a rate of 1.2% in American children aged 3–17 years (3, 4). Although the prevalence of ID is not the highest among the neurodevelopmental disorders, ID is a chronic disorder that imposes a heavy burden on the family, and is among the top 20 most costly disorders (5, 6). The comorbidity or co-occurrence of mental disorders and neurological illness is common in children and adolescents with ID and affects both their clinical progression and the outcomes of interventions (5, 7–9). The most common co-occurrent mental problems in children are autistic spectrum disorders (ASD), attention-deficit/hyperactivity disorder (ADHD) and behavioral and emotional problems, which are significantly related to the development of different domains of adaptive behavior (5, 9–13). Independently of comorbid disorders, it has been estimated that there are several overlapping cognitive difficulties in ID related to attention (14–16), learning (15–18), memory (15, 18, 19), perceptive and visuospatial skills (17, 20, 21), executive functions (15, 18, 22), processing speed (22), and communication (15, 23–25).
In the field of disability management, functional and psychosocial interventions are used most frequently, but cognitive interventions have also yielded positive results (26–28). Cognitive training refers specifically to repeated practice in a specific domain to obtain both cognitive and behavioral improvement (29). Although there are few evidence-based strategies available, professionals tend to adapt materials to meet the needs of subjects with ID to overcome difficulties in their day-to-day lives (15, 30). Recently, the number of studies describing and evaluating skills training programs (31–33) has been on the rise, coinciding with the exponential development of information and communication technologies (ICT). Browing et al. (34) were pioneers in using computers to assess the effectiveness of community skills training in children with ID. Digital technologies have easy, clear objectives and instructions, and their virtual environment, striking colors, and entertaining music and sounds can make them attractive and useful tools for interventions with subjects with ID. Although the use of these technologies has increased in recent years with benefits reported in aspects like adaptive behaviors and learning, such as communication and socialization in small children with ID, research focusing on skills generalization and technology use is necessary (35). More specifically, virtual reality has been recommended as a means by which to practice or teach cognitive and emotional skills, robots have been suggested as a way to stimulate and engage children with ID, and handheld or multimedia devices have been recommended as learning supports. Digital media using interactive computer software (31, 32, 36–38) and web-based applications expressly designed to train and practice skills through smartphones or tablets (33, 39, 40) have both been used in subjects with ID. These programs have a fixed number of sessions of specific lengths, facilitating the process of recording performance measurements as well as longitudinal follow-up. In addition, these programs allow for both the provision of reward feedback and the adjustment of the difficulty of the task. For years, subjects with ID have been using technology to overcome their motor, communication and visual impairments (41), and these devices have contributed to facilitating their performance of day-to-day activities (42, 43). However, in order to fully take advantage of digital interventions (44–46), people with ID may need longer training periods and easier tasks to obtain the most benefit (47).
Due to the number and diversity of skills training programs available through digital devices for people with ID, it is important to describe which digital interventions and media have been developed, as well as which are the most effective. Programs and devices have been used to support language learning and communication (48, 49), daily living skills, time perception and imagination (42), executive function (50, 51), emotional skills (52) and to reduce behavioral problems (33). Due to the lack of systematic reviews conducted to assess the efficacy of digital interventions in children and adolescents with ID, our review focuses on this specific age group and encompasses all digital technology currently in common use. The aims of this study are (1) to assess the use of digital devices in children and adolescents with ID and the effects derived from their use on cognitive functions (e.g., attention, memory, executive functions and language), academic and behavioral skills, daily routines, and social skills, and (2) to determine whether this methodology can be considered a therapeutic tool for subjects with ID. This systematic review will contribute to bringing to light the hard work done with this specific population and will constitute a step forward for the inclusion of people with ID in society and for the improved quality of life for children and adolescents with ID by offering them modern, effective interventions.
Materials and Methods
Prior to the literature search, we registered with the PROSPERO database (register number CRD42019121219) and created a detailed protocol in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocol (PRISMA-P) (53).
Literature Search Strategy and Information Sources
A systematic literature search of SCOPUS, the Web of Science and PsycINFO was carried out that ended in February 2020. The following search formula was created with the following free terms: (“intellectual disability” OR “mental retardation” OR “neurodevel* retardation” OR “cognitive disability”) AND (“self-help devices” OR “video games” OR “virtual reality” OR “APPS” OR “tablets” OR “Ipad” OR “computer*”) AND (“child” OR “adolescent”).
Study Selection Process and Eligibility Criteria
The systematic review and the selected studies were organized according to the participants, interventions, comparators, outcome measures, and study design (PICOS). Participants were children and adolescents with ID (mild to profound) or with syndromes associated with ID. All studies included therapeutic interventions using digital devices such as virtual reality, computers (including laptops), touch screens, input devices and handheld devices [smartphones, personal digital assistants (PDA), tablets].
Outcome measures obtained using non-standardized or standardized tests were included if the dependent variables were related to either the cognitive, social, emotional or behavioral domains. The study designs included in our analysis were experimental studies, randomized and quasi-experimental (non-randomized or without control group). We included articles published in peer-reviewed journals in English or Spanish.
We excluded studies whose participants were parents or professionals, or had mental illness, traumatic brain injury or sensorial affection. In addition, we excluded studies that did not meet the previously defined PICOS characteristics or which contained poor empirical data. Case studies, reviews, abstracts and communications from scientific meetings and qualitative studies were not considered.
The inclusion of the studies was independently reviewed by two authors. A form with inclusion criteria was designed and reviewed by all authors. In the first round, titles and abstracts of articles were selected in accordance with the form. In the second round, we assessed the full-text articles for their selection based on the inclusion criteria. In some cases, we requested the full text from the authors. Duplicated articles were removed. When necessary, any disagreement was discussed with a third author. We created a PRISMA flow chart to track the studies we included and discarded [(54); Figure 1].
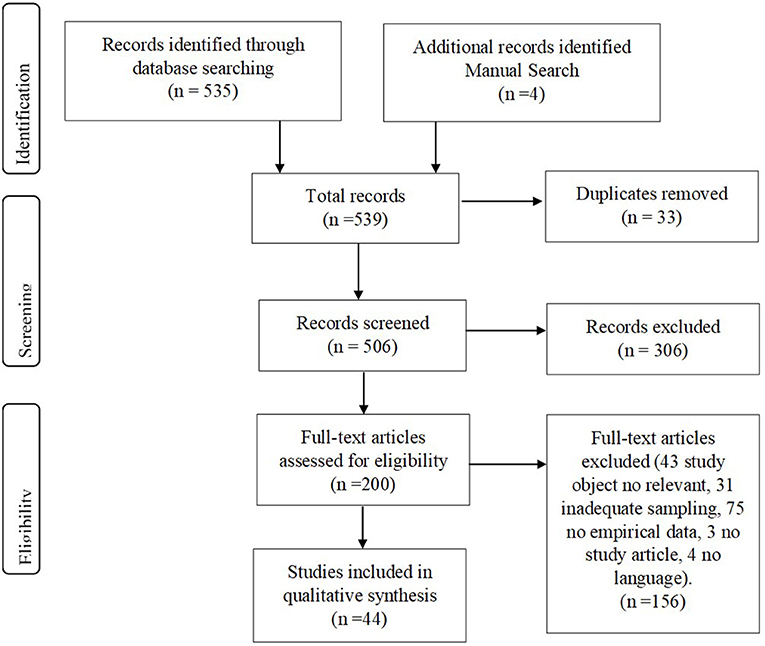
Figure 1. Flow chart for the article selection process.
Risk of Bias Assessment
Three reviewers independently assessed the risk of bias for each study using the modified Cochrane Collaboration tool (55) for randomized controlled trials. Bias was assessed as a judgment (high, low or unclear) for individual elements from five domains (selection, performance, attrition, reporting, and other). We converted this score to a quality assessment, indicating that high risk of bias equals low quality, low risk of bias is equal to high quality and unclear risk of bias is equal to moderate quality. For non-randomized studies, we assessed the quality level using Newcastle-Ottawa Quality Assessment Scale (56). Bias was assessed as a judgement (good, low) for individual elements from three domains (selection, comparability and ascertainment), resulting in a total score. The categorization of the quality assessments is reflected in the summary tables.
Results
Study Characteristics
The flow chart included as Figure 1 illustrates the process of selection for the articles included in this systematic review. First, studies were identified in databases (n = 535) and manual searches (n = 4), and then duplicates were removed (n = 33). The titles and abstracts of the remaining 506 publications were screened to select articles that met the inclusion criteria, and 306 articles were excluded. The remaining 200 full texts were carefully examined. Then the articles that did not report an intervention or that were beyond the scope of this systematic review were excluded (n = 156). In the end, a total of 44 articles were included in this review. The general characteristics are summarized in Table 1, while detailed information for each study is summarized in Tables 2–4.
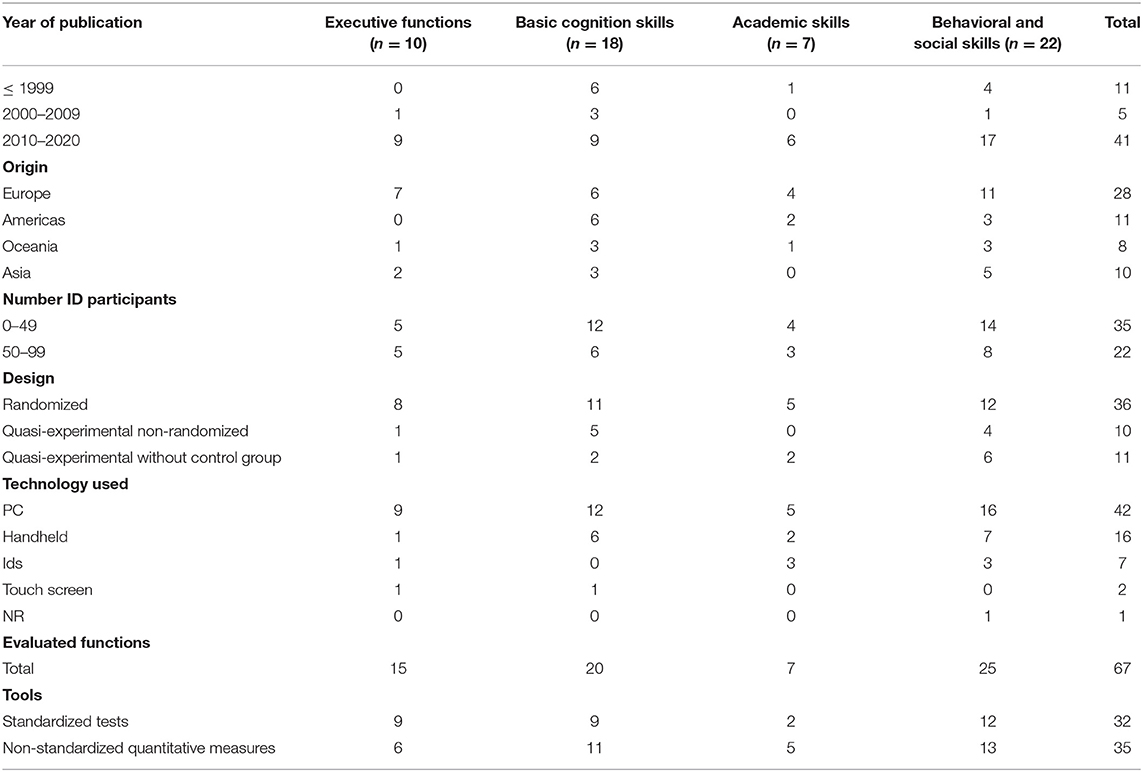
Table 1. Study characteristics according to psychological outcomes.
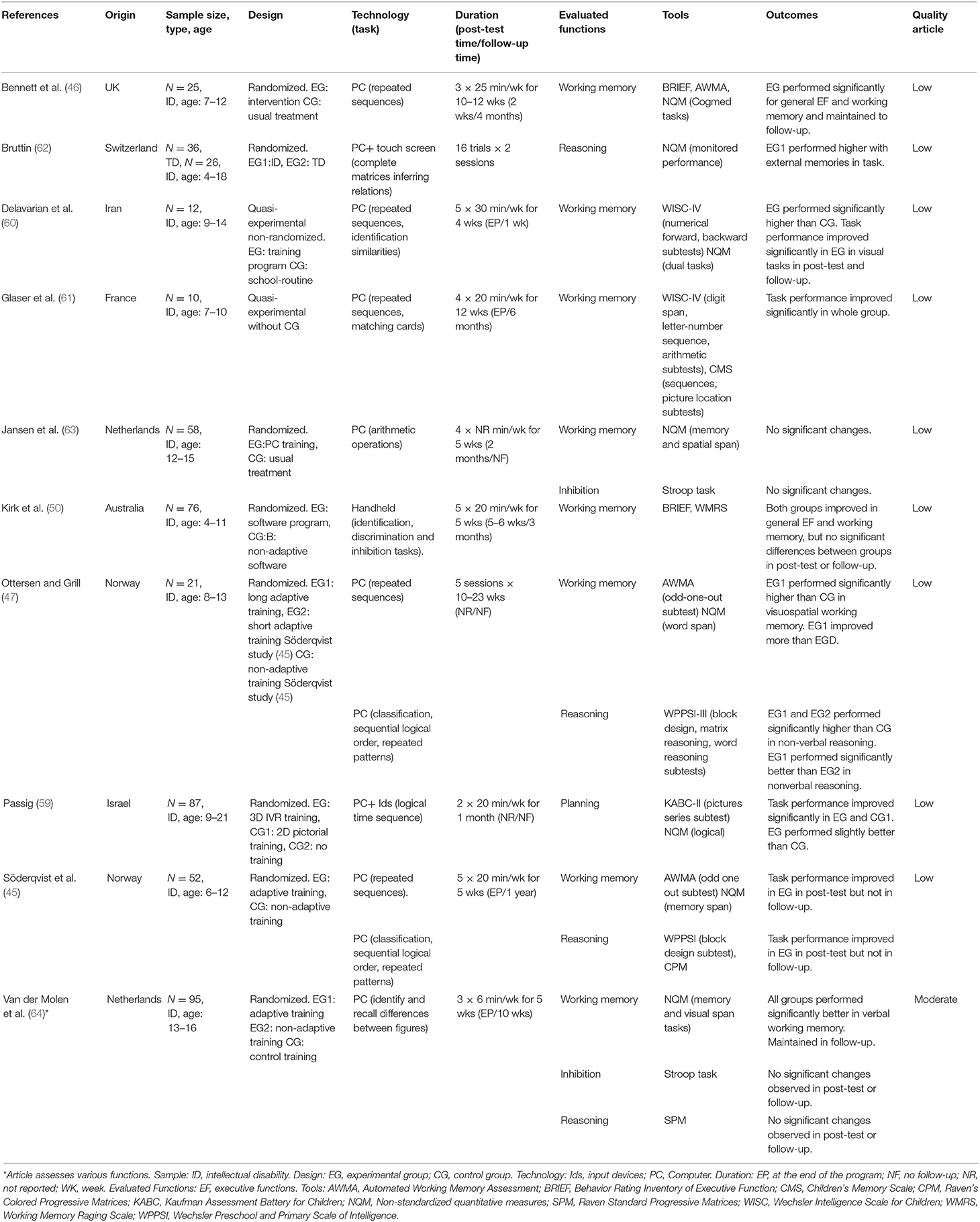
Table 2. Reviewed studies focusing on executive functions.
Executive Functions
As detailed in Table 2, 10 studies assessed the effect of interventions on executive functions, some of them also evaluated reasoning. Following theoretical models from different authors and the methodology of some of the studies (57, 58) reasoning has been included in executive function analyses. Through all the studies, executive functions were assessed in 462 children and adolescents with ID. The majority of these studies were published within the last decade and only one [10%] was published between 2000 and 2009 (59). Sample sizes were small in all of the studies we analyzed (range n = 10 to n = 95). Participant age ranged from 4 to 21. Most of the studies used randomized designs, except two [20%]: a quasi-experimental non-randomized study (60), and a quasi-experimental study without control group design (61). Most of the interventions used personal computers (n = 9) [75%] (45–47, 59–64). There was great variability in the tasks used: repeated sequences (45–47, 60, 61), matrices (62), identification and discrimination (50, 60, 64), classification and ordering (45, 47, 59) repeated patterns, mathing and arithmetic operations (45, 61, 63). Session interventions generally last for a period of between 20 and 30 min or until the completion of a concrete number of tasks or sessions (47, 62). The duration of the interventions ranged from 4 to 23 weeks. Post-test evaluations were generally performed only at the end of the program (45, 60, 61, 64) or at 1 or 2 months (50, 63). Almost half of the studies did not refer to any follow-up monitoring, and the interval of the rest was between 2 months to 1 year (45, 46, 50, 61, 64). The most common function evaluated was working memory (45–47, 50, 60, 61, 63, 64) and reasoning (45, 47, 62, 64). Outcomes measures were obtained by means of behavior tests that assess executive functions such as Behavior Rating Inventory of Executive Function BRIEF and Automated Working Memory Assessment AWMA (45–47, 50), neuropsychological tests applied to children as working memory subtests of Weschler Intelligence Scale (45, 47, 60, 61) and Stroop Task (63, 64). Nine [60%] studies used standardized tests and six [40%] studies used non-standardized quantitative measures. Of the studies analyzed, six [60%] reported significant improvements and the remainder reported some improvements or non-significant changes (45, 50, 62–64). Finally, our assessment of the quality of the studies determined that nine [90%] were low quality and one [10%] was moderate (64).
Basic Cognition Skills
Eighteen studies assessed the effect of interventions on basic cognition skills as their main focus (Table 3). A total of 592 subjects with ID were evaluated in basic cognition skills. Nine [50%] of the studies were published in the past decade, six [33%] were published before 1999 and three [16%] between 2000 and 2009. Sample sizes were usually small (range n = 4 to n = 95). Subject age ranged between 1 and 22. Eleven [61%] studies had a randomized design, the rest were quasi-experimental non-randomized (65–69) and quasi-experimental without control group (70, 71). In terms of the technology used, 12 [63%] of the studies used personal computer devices for their interventions (45, 64–75). Language was the most common function evaluated with 14 [70%] of the studies analyzed (45, 50, 64–72, 74, 76, 77) followed by attention, which were the focus of three [15%] of the studies analyzed (45, 75, 78). There was great heterogeneity regarding the tasks used, with the most common related to concept matching (65, 71, 72, 77), sentence construction, pronunciation, drawing, writing, answering questions (51, 66–70, 72, 74, 76) identification and discrimination tasks (50, 51, 64, 67, 78). In general, the duration of the sessions was between 20 and 30 min. In some studies, the length of the session was adjusted to the completion of the tests (72, 77, 79). Fourteen [77%] of the studies analyzed had a duration of between 1 and 4 months. Eight [44%] of the studies analyzed did not specify when post-test assessments were administered. When this data was available the range varied between immediately after the program and 6 weeks. Regarding follow-up, only a few studies assessed long-term outcomes of between 1 month and 1 year (45, 50, 64, 66, 74, 75, 78). A great number of studies, 11 [55%] to be exact, used non-standardized quantitative measures, the remainder (n = 9) [45%], used standardized tests. Of the studies analyzed, 10 [55%] reported significant benefits [all in language (n = 7)], four [22%] obtained non-significant improvements, and in the remaining, improvements were similar between groups or no improvement was observed (51, 68, 74). Fifteen [83%] studies were categorized as low quality, two [11%] as having moderate quality and one [5%] as high quality.
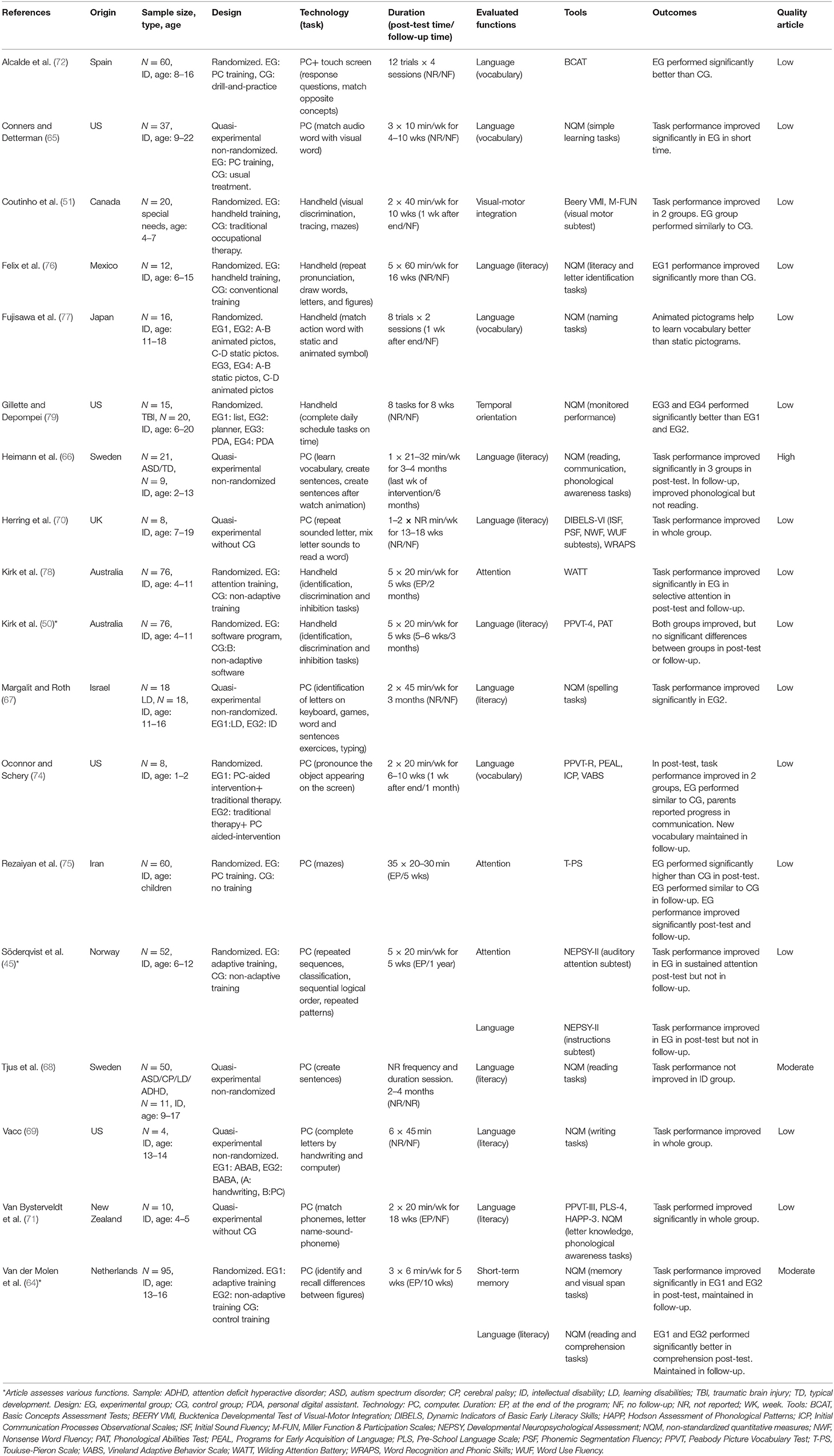
Table 3. Reviewed studies focusing on basic cognitive skills.
Academic Skills
As detailed in Table 4, seven studies assessed the effect of interventions on academic skills adding a total of 264 subjects evaluated. Most of them, concretely six [86%] studies were published between 2010 and 2020 and one study [14%] was published before 1999. Sample sizes were small in all studies analyzed (range n = 3 to n = 95). Participant age ranged between 3 and 23 years. Regarding design of the studies, most of them (n = 5) [71%] were randomized design and two [28%] were quasi-experimental without control group (80, 81). Respecting technology used in the interventions, half of the studies (n = 5) [50%] used personal computer (63, 64, 73, 80, 82), some of them also used input devices (n = 3) [30%]; and the remaining two [20%], used handheld (78, 81). Concerning evaluated functions, mathematics was the most common (n = 6) [85%] (50, 63, 64, 80–82). Regarding the tasks used, existed a great heterogeneity. The most common were related to arithmetic operations (63, 80), matching or response questions (81, 82) and identification and classification (50, 64, 73). In general, the duration of the sessions was between 10 and 30 min. Most of the studies (n = 6) [85%] had a duration ranged between 1 and 4 months. Four [57%] studies specify post-test assessments, from just at the end of the intervention to 2 months. Only three [42%] studies conducted long-term assessment, they were ranged between 10 weeks and 3 months (50, 64, 80). In reference to assessment tools, the majority of the studies analyzed used non-standardized quantitative measures (n = 5) [71%], and the rest (n = 2) [28%], used standardized tests. The outcomes reported from the studies analyzed, two [29%] showed significant improvements (64, 82) and the rest (n = 5) [71%] reported some improvements or non-significant changes. Six [85%] studies were categorized as low quality and one [15%], as moderate quality.
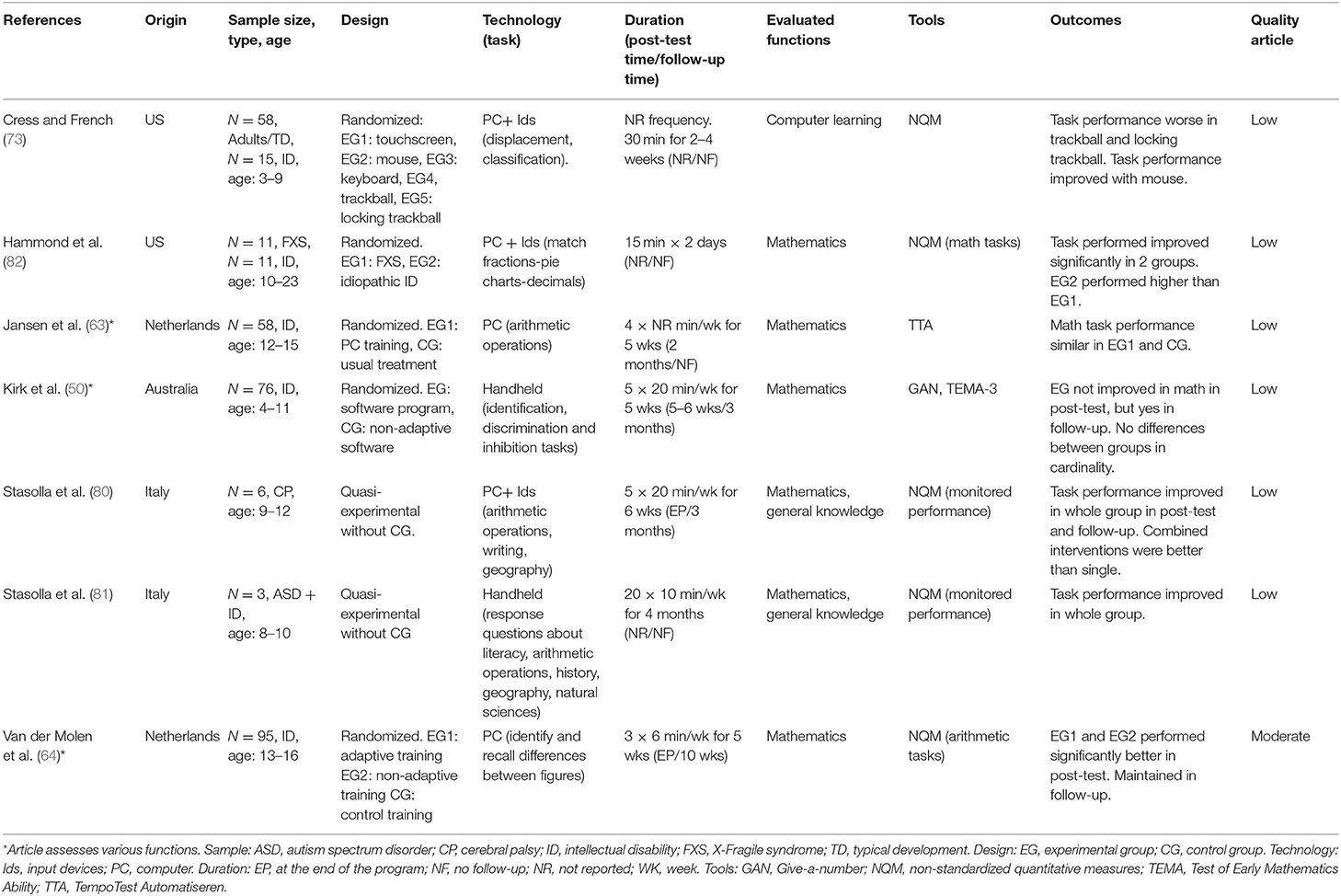
Table 4. Reviewed studies focusing on academic skills.
Behavioral and Social Skills
The studies that assessed the effect of interventions on behavioral and social skills are described in Table 5. Through all the studies, 759 children and adolescent with ID were assessed. Again, most of these studies were published in the last decade (n = 17) [77%]. Sample sizes were mostly small (range n = 3 to n = 87) and the age ranges were between 4 and 31 years old. In terms of the design of the studies analyzed, 12 [54%] had a randomized design, six [27%] a quasi-experimental design without CG (34, 61, 80, 81, 83, 84) and four [18%] a quasi-experimental non-randomized design (85–88). The most common devices used were personal computers (34, 45, 61, 80, 83–85, 87–94) and handheld devices (50, 52, 78, 81, 84, 94, 95). The most commonly evaluated functions were behavioral (45, 50, 52, 78, 80, 81, 86–88, 90, 92) and social skills (34, 61, 83–85, 87, 93–95). The most common tasks proposed were matching (45, 52, 61, 83, 85, 87, 94), combination with real life tasks (52, 84, 89, 92, 95) and sequences (45, 83, 88, 90). Sessions had a general duration of between 20–30 min and 55–90 min. Generally, the duration of the interventions was between 2 and 4 months. Time to post-test was absent in nine [40%] the studies, only at the end of the program in eight [36%] studies, and between 1 week and 3 months post program in five [22%]. Most of these studies did not include any follow-up. Non-standardized quantitative measures (n = 13) [52%] and standardized tests (n = 12) [48%] were used about equally. The outcomes of the interventions reported indicate that almost half resulted in significant benefits (n = 10) [45%], and the remainder obtained no significant improvements (n = 11) [50%], or non-significant changes (n = 1) [5%]. Of the significant benefits reported, nine [50%] studies correspond to social skills and three [30%] to behavioral skills. Seventeen [77%] of the studies were categorized as low quality, four [18%] as moderate and one [5%] as high.
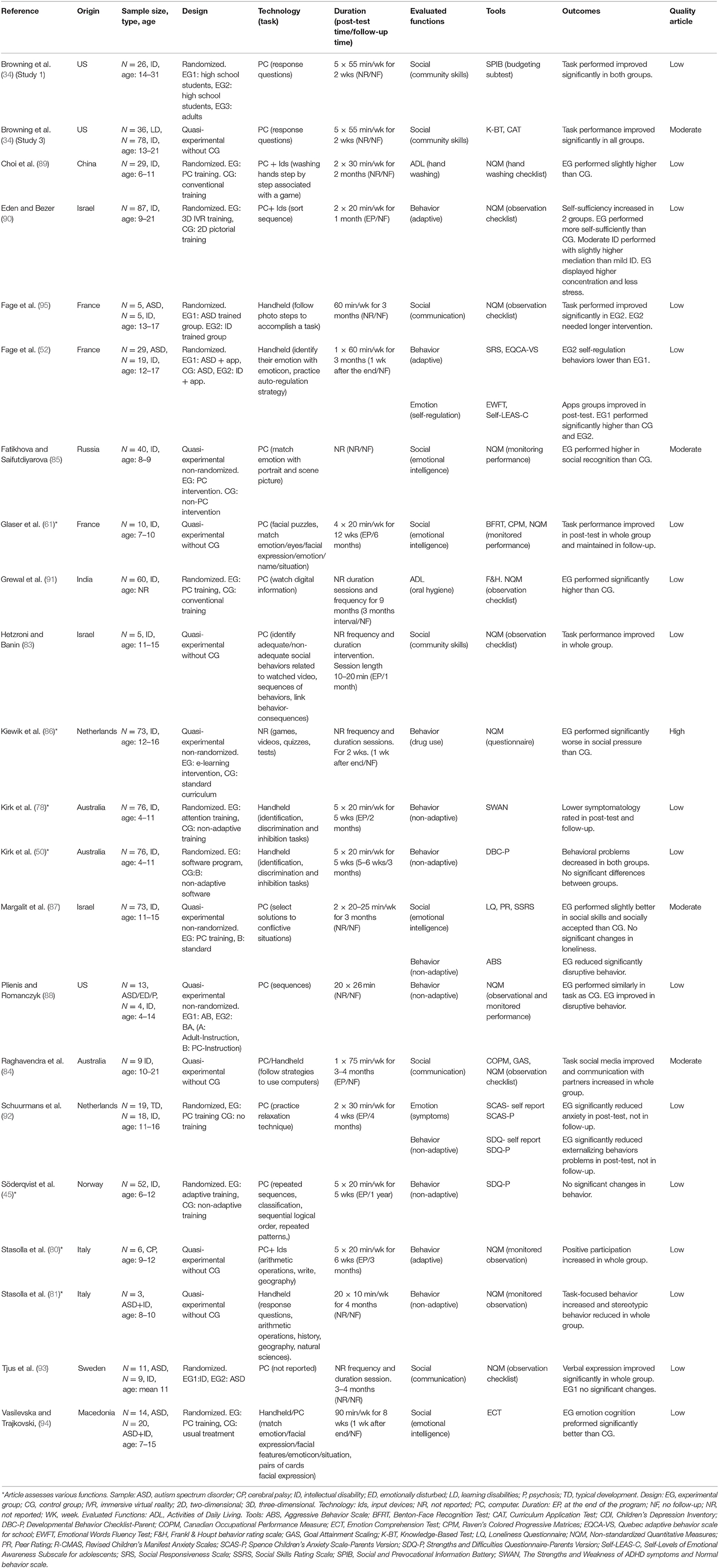
Table 5. Reviewed studies focusing on behavioral and social skills.
Discussion
Summary of Main Findings
The main objective of this review was to assess the effects of digital interventions on trained skills in children and adolescents with ID. In general, the available evidence suggests that interventions undertaken with digital devices are potentially beneficial in executive function (e.g., working memory, reasoning and planning), basic cognition (as language and attention) and academic (concretely mathematics) training as well as in the social and behavioral domains. The increasing number of studies assessing the effectiveness of digital devices in the last years is noteworthy. Some studies assessed several functions at the same time, in these cases we included the same study in each of our function categories: executive functions, basic cognition skills, and behavioral and social skills (50, 63, 64). Kirk et al. (50) concluded that attention training did not improve other skills, like receptive vocabulary, phonological abilities, or cardinality. This observation suggests a possible line of research that would focus on more deeply exploring the connection between training in one skill and benefits in others.
More than a half the studies we analyzed used randomized designs, albeit most of them evaluated a small number of participants. Studies were very heterogeneous in terms of the age range, tasks and devices used. Computers were the most frequently used device in the studies, followed by handheld devices. However, we noted a lack of studies comparing the same task administered on different devices. In fact, the choice of device seemed to be adapted to the subjects' requirements. Interestingly, it has been suggested that subjects with ID perform better using a mouse than a touch screen (73), which could be attributable to motor difficulties.
Numerous tasks (mazes, puzzles, matching, discrimination, and sequences) were developed to train different functions. Although most studies used games, some used videos depicting different scenes and situations to train social skills (83, 86, 91). Several authors indicated that in order to obtain beneficial effects the tasks must include positive reinforcement, immediate feedback, and frequent repetition (45, 46, 61, 96).
Because the lengths of the sessions and the duration of the interventions varied from study to study, we did not have enough data to draw a conclusion in this regard. Two studies described positive outcomes in the social and behavioral domains after a short intervention of 2 weeks (34, 86). These studies did not include a follow-up assessment and there was not sufficient data to evaluate long-term effectiveness. We found a wide range of duration, from 4 to 27 weeks in which the effectiveness of the intervention could be demonstrated. Ottersen and Grill (47) replicated the research conducted by Söderqvist et al. (45), but they extended the length of the interventions and then compared the results of the two studies. Comparing short vs. long interventions, they concluded that progress was more constant and stable in working memory and nonverbal reasoning in long interventions.
Several studies did not specify the time at which the post-test evaluation was conducted, some did it immediately at the end of the program, while others assessed it between 1 week and 1 year after the training program ended. In general, all of the studies reported improvements when the subjects were evaluated within 1 week of training (60, 61, 64, 66, 71, 75, 78, 86, 92, 94). Only few studies included a follow-up step to assess long-term effects. Improved or maintained skills were reported at 1 and 4 months (46, 60, 64, 74, 75, 78), 5 months, (75) and at 6 months (66). A 1-year follow-up assessment did not find any effects (45), suggesting that effects could be limited in time and that a repeated intervention would be necessary to maintain the improvements achieved.
Several studies comparing digital training with traditional (or typical) interventions suggest that digital methods may be more effective than traditional ones (45–47, 50, 51, 60, 62–65, 72, 76, 86, 89, 91, 94). ID severity is an important factor to take into account, as intelligence level may limit outcomes, and subjects with moderate and severe ID will require greater support to achieve the requirements of the tasks (82). However, many authors did not specify the severity of their subjects' ID, while others combined mild and moderate ID but did not make comparisons between ID severities. Only Passig (59) observed that subjects with mild ID performed better than those with moderate ID. On the other hand, a great number of studies with subjects with mild ID reported benefits (34, 46, 62–64, 67, 72, 75, 78, 81, 85, 87, 89, 95), but few studies reported positive results in the moderate and severe ID population (65, 69, 70, 76). More studies and larger samples comparing task achievement between ID severities are needed. The majority of the studies did not specify the presence or absence of medical or psychiatric comorbidities in children with ID, but when described, the most common were genetic disorders such as Down's, Fragile X (FXS) or Williams syndromes. This is an important issue because comorbidities may add task-specific challenges. For example some difficulties were observed when training spatial knowledge in individuals with Down's syndrome using a virtual environment (96). In some cases, cerebral palsy (CP), ASD, ADHD, and motor and sensory impairment were also present. These comorbidities may interfere with task performance and the outcome of the intervention and should be noted in the results of the studies.
It is important to emphasize that new technologies do not replace the work of professionals (80), but they can help in combined interventions. Furthermore, future research is needed to assess the usefulness of other handheld devices, such as smartphones, for educational purposes. New technologies are powerful tools that can also impact the everyday lives of people with ID. The extended use of handheld devices may have beneficial effects on social and relationship skills through the construction of social networks (84) or, on the other hand, such use may have detrimental effects by increasing the risk of cyberbullying aimed at adolescents with ID (97). However, neither handheld devices nor social skills have received much attention in subjects with ID.
In agreement with a previous systematic review conducted by den Brok and Sterkenburg (42) including the ID population at all ages, we conclude that there is evidence to support the effectiveness of digital interventions in some daily living, cognitive, academic and social skills domains. However, we did not find evidence supporting long-lasting beneficial effects lasting more than a few months after the cessation of the training sessions. Moreover, to our knowledge, no research has been published that evaluates the effects of repeated interventions on long-term outcomes. In this regard, more follow-up studies are needed to examine the beneficial effects of long-term and repeated interventions.
Limitations and Future Directions for Research
The main limitation of this review is related to the low quality of the studies analyzed, in part due to their small sample sizes. Our conclusions must be taken with caution, because monitoring the use of digital devices at home was not described and the complex characteristics of the sample could have influenced the study designs. The use of non-standardized tests and assessments rated by parents or teachers (e.g., BRIEF, ABC) was very common, and these carry a potential risk of bias due to the subjective component (46).
For future lines of research, it would be interesting to conduct studies in special education centers were training variables in training programs may be easier to control than at home. It is also necessary observe effects in subjects with severe and profound ID. It is important to consider longer follow-up assessments and longer interventions (e.g., 6 and 12 months) due to the lack of studies that make use of these longer formats, and because the improvements reported are probably not permanent (50, 78). The influence of the type of disorder giving rise to the intellectual disability as well as the most effective digital devices for use in these types of interventions should also be explored.
Despite the limitations described at the methodological level, the data analyzed suggest that digital interventions have potential as a therapeutic tool to benefit working memory, academic skills, and the social and behavioral domains in children and adolescents with ID.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Author Contributions
Designed form, data collection, and the inclusion analysis of the studies was independently reviewed by MC and MT. When it was necessary, any disagreement was discussed with JC. All authors contributed to the study conception and design, contributed to quality analysis, commented on previous versions of the manuscript, read, and approved the final manuscript.
Funding
This work was supported by Industrial Doctorate from Generalitat de Catalunya reference number 2019 DI 72.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Abbreviations
ABC, Aberrant Behavior Checklist; ADHD, Attention-Deficit/Hyperactivity Disorder; ASD, Autistic Spectrum Disorder; APA, American Psychiatric Association; AWMA, Automated Working Memory Assessment; BRIEF, Behavior Rating Inventory of Executive Function; CP, Cerebral Palsy; DSM-5, Diagnostic and Statistical Manual Fifth Edition; FXS, Fragile X Syndrome; ICT, Information and Communication Technologies; ID, Intellectual Disability; PDA: Personal Digital Assistant; PICOS, Participants, Interventions, Comparators, Outcome measures, Study design; PRISMA-P, Preferred Reporting Items for Systematic Review and Meta-Analysis Protocol.
Footnotes
1. ^Indicated what studies are included in the review, as the reviewer suggested.
References
1. American Psychiatric Association (APA). Manual Diagnóstico y Estadístico de los Trastornos Mentales DSM-V. Barcelona: Editorial Panamericana (2013).
2. McKenzie K, Milton M, Smith G, Oullette-Kuntz H. Systematic review of the prevalence and incidence of intellectual disabilities: current trends and issues. Curr Dev Disord Rep. (2016) 3:104–15. doi: 10.1007/s40474-016-0085-7
3. Zablotsky B, Black LI, Blumberg SJ. Estimated prevalence of children with diagnosed developmental disabilities in the United States, 2014-2016. NCHS Data Brief. (2017) 291:1–8.
4. Zablotsky B, Maenner MJ, Blumberg SJ. Geographic disparities in treatment for children with autism spectrum disorder. Acad Pediatr. (2019) 19:740–7. doi: 10.1016/j.acap.2019.02.013
5. Munir K. The co-occurrence of mental disorders in children and adolescents with intellectual disability/intellectual developmental disorder. Curr Opin Psychiatry. (2016) 29:95–102. doi: 10.1097/YCO.0000000000000236
6. Pikakshi VK, Goyal S, Thakral A, Baniya G. Comorbidities among children with intellectual disability presenting for disability certification at a tertiary care center and assessment of burden in mothers of these children. J Mental Health Hum Behav. (2018) 23:108. doi: 10.4103/jmhhb.jmhhb_5_19
7. Einfeld SL, Piccinin AM, Mackinnon A, Hofer SM, Taffe J, Gray KM, et al. Psychopathology in young people with intellectual disability. JAMA. (2006) 296:1981–9. doi: 10.1001/jama.296.16.1981
8. Uzun A, Sari SA, Mercan C. Sociodemographic characteristics, risk factors, and prevalence of comorbidity among children and adolescents with intellectual disability: a cross-sectional study. J Ment Health Res Intellect Disabil. (2020) 13:66–85. doi: 10.1080/19315864.2020.1727590
9. Flanigan L, Climie EA, Christina Gray C, Fernández C. ADHD in individuals with intellectual disability. In: Matson DJL, editor. Handbook of Intellectual Disabilities, Autism and Child Psychopathology. Calgary, AB (2019). p. 917–36. doi: 10.1007/978-3-030-20843-1_48
10. Emerson E. Prevalence of psychiatric disorders in children and adolescents with and without intellectual disability. J Intellect Disabil Res. (2003) 47:51–8. doi: 10.1046/j.1365-2788.2003.00464.x
11. Gligorović M, Buha Ðurović N. Inhibitory control and adaptive behaviour in children with mild intellectual disability. J Intellect Disability Res: JIDR. (2014) 58:233–42. doi: 10.1111/jir.12000
12. Kurzius-Spencer M, Pettygrove S, Christensen D, Pedersen AL, Cunniff C, Meaney FJ, et al. Behavioral problems in children with autism spectrum disorder with and without co-occurring intellectual disability. Res. Autism Spectr Disord. (2018) 56:61–71. doi: 10.1016/j.rasd.2018.09.002
13. Dekker MC, Koot HM, Van Der Ende J, Verhulst FC. Emotional and behavioral problems in children and adolescents with and without intellectual disability. J Child Psychol Psychiatry Allied Discipl. (2002) 43:1087–98. doi: 10.1111/1469-7610.00235
14. Neece CL, Baker BL, Blacher J, Crnic KA. Attention-deficit/hyperactivity disorder among children with and without intellectual disability: an examination across time. J Intellect Disabil Res: JIDR. (2011) 55:623–35. doi: 10.1111/j.1365-2788.2011.01416.x
15. Hronis A, Roberts L, Kneebone II. A review of cognitive impairments in children with intellectual disabilities: Implications for cognitive behaviour therapy. Br J Clin Psychol. (2017) 56:189–207. doi: 10.1111/bjc.12133
16. D'Souza H, Karmiloff-Smith A. Neurodevelopmental Disorders. Wiley Interdisciplinary Reviews: Cognitive Science. London: Wiley-Blackwell (2017). doi: 10.1002/wcs.1398
17. Vicari S, Verucci L, Carlesimo GA. Implicit memory is independent from IQ and age but not from etiology: evidence from down and williams syndromes. J Intellect Disabil Res. (2007) 51:932–41. doi: 10.1111/j.1365-2788.2007.01003.x
18. Bexkens A, Jansen BR, Van der Molen MW, Huizenga HM. Cool decision-making in adolescents with behavior disorder and/or mild-to-borderline intellectual disability. J Abnorm Child Psychol. (2016) 44:357–67. doi: 10.1007/s10802-015-9996-8
19. Purser HRM, Jarrold C. Impaired verbal short-term memory in down syndrome reflects a capacity limitation rather than atypically rapid forgetting. J Exp Child Psychol. (2005) 91:1–23. doi: 10.1016/j.jecp.2005.01.002
20. Rais M, Binder DK, Razak KA, Ethell IM. Sensory Processing Phenotypes in Fragile X Syndrome. SAGE Publications Inc. (2018). doi: 10.1177/1759091418801092
21. Di Blasi FD, Elia F, Buono S, Ramakers GJA, Di Nuovo. SF. Relationships between visual-motor and cognitive abilities in intellectual disabilities. Percept Mot Skills. (2007) 104:763–72. doi: 10.2466/pms.104.3.763-772
22. Schuiringa H, van Nieuwenhuijzen M, Orobio de Castro B, Matthys W. Executive functions and processing speed in children with mild to borderline intellectual disabilities and externalizing behavior problems. Child Neuropsychol. (2017) 23:442–62. doi: 10.1080/09297049.2015.1135421
23. Marrus N, Hall L. Intellectual disability and language disorder. Child Adolesc Psychiatr Clin N Am. (2017) 26:539–54. doi: 10.1016/j.chc.2017.03.001
24. Jones FW, Long K, Finlay WML. Assessing the reading comprehension of adults with learning disabilities. J Intellect Disabil Res. (2006) 50:410–8. doi: 10.1111/j.1365-2788.2006.00787.x
25. Van Wingerden E, Segers E, van Balkom H, Verhoeven L. Foundations of reading comprehension in children with intellectual disabilities. Res Dev Disabil. (2016) 60:211–22. doi: 10.1016/j.ridd.2016.10.015
26. Danielsson H, Zottarel V, Palmqvist L, Lanfranchi S. The effectiveness of working memory training with individuals with intellectual disabilities - a meta-analytic review. Front Psychol. (2015) 6:1230. doi: 10.3389/fpsyg.2015.01230
27. Lanfranchi S, Pulina F, Carretti B, Mammarella IC. Training spatial-simultaneous working memory in individuals with down syndrome. Res Dev Disabil. (2017) 64:118–29. doi: 10.1016/j.ridd.2017.03.012
28. Verberg FLM, Helmond P, Overbeek G. Study protocol: A randomized controlled trial testing the effectiveness of an online mindset intervention in adolescents with intellectual disabilities. BMC Psychiatry. (2018) 18:377. doi: 10.1186/s12888-018-1939-9
29. Kirk HE, Gray K, Riby DM, Cornish KM. Cognitive training as a resolution for early executive function difficulties in children with intellectual disabilities. Res Dev Disabil. (2015) 38:145–60. doi: 10.1016/j.ridd.2014.12.026
30. Man J, Kangas M. Best practice principles when working with individuals with intellectual disability and comorbid mental health concerns. Qual Health Res. (2019) 30:560–71. doi: 10.1177/1049732319858326
31. Favre E, Peyroux E, Babinet MN, Poisson A, Demily C. Computer-based cognitive remediation program for the treatment of behavioral problems in children with intellectual disability: the ≪COGNITUS & MOI≫ study protocol for a randomized controlled trial. BMC Psychiatry. (2018) 18:235. doi: 10.1186/s12888-018-1810-z
32. de Mello Monteiro CB, da Silva TD, de Abreu LC, Fregni F, de Araujo LV, Ferreira HIB, et al. Short-term motor learning through non-immersive virtual reality task in individuals with down syndrome. BMC Neurol. (2017) 17:71. doi: 10.1186/s12883-017-0852-z
33. Kim M, Blair KSC, Lim K. Using tablet assisted Social StoriesTM to improve classroom behavior for adolescents with intellectual disabilities. Res Dev Disabil. (2014) 35:2241–51. doi: 10.1016/j.ridd.2014.05.011
34. *Browning P, Nave G, White WA, Barkin PZ. Interactive video as an instructional technology for handicapped learners: a development and research program. Austr New Zealand J Deve Disabil. (1985) 11:123–8. doi: 10.3109/13668258508998630
35. Burns CO, Lemon J, Granpeesheh D, Dixon DR. Interventions for daily living skills in individuals with intellectual disability: a 50-year systematic review. Adv Neurodevelop Disord. (2019) 3:235–45. doi: 10.1007/s41252-019-00114-0
36. Siberski J, Shatil E, Siberski C, Eckroth-Bucher M, French A, Horton S, et al. Computer-based cognitive training for individuals with intellectual and developmental disabilities: pilot study. Am J Alzheimer's Dis Other Dement. (2015) 30:41–8. doi: 10.1177/1533317514539376
37. Vereenooghe L, Gega L, Reynolds S, Langdon PE. Using computers to teach people with intellectual disabilities to perform some of the tasks used within cognitive behavioural therapy: a randomised experiment. Behav Res Ther. (2016) 76:13–23. doi: 10.1016/j.brat.2015.11.002
38. Cooney P, Jackman C, Coyle D, O'Reilly G. Computerised cognitive-behavioural therapy for adults with intellectual disability: randomised controlled trial. Br J Psychiatry. (2017) 211:95–102. doi: 10.1192/bjp.bp.117.198630
39. Van den Bosch KA, Andringa TC, Post WJ, Ruijssenaars WAJJM, Vlaskamp C. The relationship between soundscapes and challenging behavior: a small-scale intervention study in a healthcare organization for individuals with severe or profound intellectual disabilities. Build Acoustics. (2018) 25:123–35. doi: 10.1177/1351010X18775022
40. Lancioni GE, Singh NN, O'Reilly MF, Sigafoos J, Alberti G, Perilli V, et al. An upgraded smartphone-based program for leisure and communication of people with intellectual and other disabilities. Front Public Health. (2018) 6:234. doi: 10.3389/fpubh.2018.00234
41. Raspa M, Fitzgerald T, Furberg RD, Wylie A, Moultrie R, DeRamus M, et al. Mobile technology use and skills among individuals with fragile X syndrome: implications for healthcare decision making. J Intellect Disabil Res: JIDR. (2018) 62:821–32. doi: 10.1111/jir.12537
42. den Brok WL, Sterkenburg PS. Self-controlled technologies to support skill attainment in persons with an autism spectrum disorder and/or an intellectual disability: a systematic literature review. Disabil Rehabil Assist Technol. (2014) 10:1–10. doi: 10.3109/17483107.2014.921248
43. Palmer SB, Wehmeyer ML, Davies DK, Stock SE. Family members' reports of the technology use of family members with intellectual and developmental disabilities. J Intellect Disabil Res. (2012) 56:402–14. doi: 10.1111/j.1365-2788.2011.01489.x
44. Klingberg T. Training and plasticity of working memory. Trends Cogn Sci. (2010) 14:317–32. doi: 10.1016/j.tics.2010.05.002
45. *Söderqvist S, Nutley SB, Ottersen J, Grill KM, Klingberg T. Computerized training of non-vrbal reasoning and working memory in children with intellectual disability. Front Hum Neurosci Vol. (2012) 6:271. doi: 10.3389/fnhum.2012.00271
46. *Bennett S, Buckley S, Holmes J. Computerized memory training leads to sustained improvement in visuospatial short-term memory skills in children with down syndrome. Am J Intellect Dev Disabil Vol. (2013) 118:179–92. doi: 10.1352/1944-7558-118.3.179
47. *Ottersen J, Grill KM. Benefits of extending and adjusting the level of difficulty on computerized cognitive training for children with intellectual disabilities. Front Psychol. (2015) 6:1233. doi: 10.3389/fpsyg.2015.01233
48. Boyle S, McCoy A, McNaughton D, Light J. Using digital texts in interactive reading activities for children with language delays and disorders: a review of the research literature and pilot study. Semin Speech Lang. (2017) 38:263–75. doi: 10.1055/s-0037-1604274
49. Barbosa RTA, de Oliveira ASB, de Lima Antão JYF, Crocetta TB, Guarnieri R, Antunes TPC, et al. Augmentative and alternative communication in children with down's syndrome: a systematic review. BMC Pediatr. (2018) 18:160. doi: 10.1186/s12887-018-1144-5
50. *Kirk H, Gray K, Ellis K, Taffe J, Cornish K. Impact of attention training on academic achievement, executive functioning, and behavior: a randomized controlled trial. Am J Intellect Dev Disabil. (2017) 122:97–117. doi: 10.1352/1944-7558-122.2.97
51. *Coutinho F, Bosisio ME, Brown E, Rishikof S, Skaf E, Zhang X, et al. Effectiveness of iPad apps on visual-motor skills among children with special needs between 4y0m−7y11m. Disabil Rehabilit Assistive Technol. (2016) 12:402–10. doi: 10.1080/17483107.2016.1185648
52. *Fage C, Consel C, Etchegoyhen K, Amestoy A, Bouvard M, Mazon C, et al. An emotion regulation app for school inclusion of children with ASD: design principles and evaluation. Comp Educ. (2019) 131:1–21. doi: 10.1016/j.compedu.2018.12.003
53. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Rev Espanola Nutr Hum Dietet. (2015) 20:148–60. doi: 10.1186/2046-4053-4-1
54. Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
55. Higgins JPT, Green S, (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration (2011). Available online at: www.cochrane-handbook.org
56. Wells G, Shea B, O'Connell D, Peterson J, Welch V, Losos M, et al. The Ottawa Hospital. Ottawa, ON: Research Institute (2019). Available online at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp
57. Diamond A. Executive functions. Annu Rev Psychol. (2013) 64:135–68. doi: 10.1146/annurev-psych-113011-143750
58. Demetriou EA, DeMayo MM, Guastella AJ. Executive function in autism spectrum disorder: history, theoretical models, empirical findings, and potential as an endophenotype. Front Psychiatry. (2019) 10:753. doi: 10.3389/fpsyt.2019.00753
59. *Passig D. Improving the sequential time perception of teenagers with mild to moderate mental retardation with 3D Immersive Virtual Reality (IVR). J Educ Comput Res. (2009) 40:263–80. doi: 10.2190/EC.40.3.a
60. *Delavarian M, Bokharaeian B, Towhidkhah F, Gharibzadeh S. Computer-based working memory training in children with mild intellectual disability. Early Child Dev Care. (2015) 185:66–74. doi: 10.1080/03004430.2014.903941
61. *Glaser B, Lothe A, Chabloz M, Dukes D, Pasca C, Redoute J, et al. Candidate socioemotional remediation program for individuals with intellectual disability. Am J Intellect Develop Disabil. (2012) 117:368–83. doi: 10.1352/1944-7558-117.5.368
62. *Bruttin CD. Computerised assessment of an analogical reasoning test: Effects of external memory strategies and their positive outcomes in young children and adolescents with intellectual disability. Educ Child Psychol. (2011) 28:18–32.
63. *Jansen BRJ, De Lange E, Van der Molen MJ. Math practice and its influence on math skills and executive functions in adolescents with mild to borderline intellectual disability. Res Dev Disabil. (2013) 34:1815–24. doi: 10.1016/j.ridd.2013.02.022
64. *Van der Molen MJ, Van Luit JEH, Van der Molen MW, Klugkist I, Jongmans MJ. Effectiveness of a computerised working memory training in adolescents with mild to borderline intellectual disabilities. J Intellect Disabil Res. (2010) 54:433–47. doi: 10.1111/j.1365-2788.2010.01285.x
65. *Conners FA, Detterman DK. Information-processing correlates of computer-assisted word learning by mentally retarded students. Am J Mental Defic. (1987) 91:606–12.
66. *Heimann M, Nelson KE, Tjus T, Gillberg C. Increasing reading and communication skills in children with autism through an interactive multimedia computer program. J Autism Dev Disord. (1995) 25:459–80. doi: 10.1007/BF02178294
67. *Margalit M, Roth YB. Strategic keyboard training and spelling improvement among children with learning disabilities and mental retardation. Educ Psychol. (1989) 9:321–9. doi: 10.1080/0144341890090404
68. *Tjus T, Heimann M, Nelson K. Reading acquisition by implementing a multimedia intervention strategy for fifty children with autism or other learning and communication disabilities. J Cognit Behav Psychother. (2004) 4:203–21.
69. *Vacc NN. Word processor versus handwriting: a comparative study of writing samples produced by mildly mentally handicapped students. Except Child. (1987) 54:156–65. doi: 10.1177/001440298705400209
70. *Herring E, Grindle C, Kovshoff H. Teaching early reading skills to children with severe intellectual disabilities using headsprout early reading. J Appl Res Intellect Disabil. (2019) 32:1138–48. doi: 10.1111/jar.12603
71. *Van Bysterveldt AK, Gillon G, Foster-Cohen S. Integrated speech and phonological awareness intervention for pre-school children with down syndrome. Int J Lang Commun Disord. (2010) 45:320–35. doi: 10.3109/13682820903003514
72. *Alcalde C, Navarro JI, Marchena E, Ruiz G. Acquisition of basic concepts by children with intellectual disabilities using a computer-assisted learning approach. Psychol. Rep. (1998) 82:1051–6. doi: 10.2466/pr0.1998.82.3.1051
73. *Cress CJ, French GJ. The relationship between cognitive load measurements and estimates of computer input control skills. Assist Technol. (1994) 6:54–66. doi: 10.1080/10400435.1994.10132227
74. *Oconnor L, Schery TK. A comparison of microcomputer-aided and traditional language therapy for developing communication-skills in nonoral toddlers. J Speech Hear Disord. (1986) 51:356–61. doi: 10.1044/jshd.5104.356
75. *Rezaiyan A, Mohammadi E, Fallah PA. Effect of computer game intervention on the attention capacity of mentally retarded children. Int J Nurs Pract. (2007) 13:284–8. doi: 10.1111/j.1440-172X.2007.00639.x
76. *Felix VG, Mena LJ, Ostos R, Maestre GE. A pilot study of the use of emerging computer technologies to improve the effectiveness of reading and writing therapies in children with down syndrome. Br J Educat Technol. (2017) 48:611–24. doi: 10.1111/bjet.12426
77. *Fujisawa K, Inoue T, Yamana Y, Hayashi H. The effect of animation on learning action symbols by individuals with intellectual disabilities. Augment Alternat Commun. (2011) 27:53–60. doi: 10.3109/07434618.2011.553245
78. *Kirk HE, Gray KM, Ellis K, Taffe J, Cornish KM. Computerised attention training for children with intellectual and developmental disabilities: a randomised controlled trial. J Child Psychol Psychiatry. (2016) 57:1380–9. doi: 10.1111/jcpp.12615
79. *Gillette Y, Depompei R. Do PDAs enhance the organization and memory skills of students with cognitive disabilities? Psychol Sch. (2008) 45:665–77. doi: 10.1002/pits.20316
80. *Stasolla F, Damiani R, Perilli V, D'Amico F, Caffò AO, Stella A, et al. Computer and microswitch-based programs to improve academic activities by six children with cerebral palsy. Res Dev Disabilit. (2015) 45–46:1–13. doi: 10.1016/j.ridd.2015.07.005
81. *Stasolla F, Perilli V, Boccasini A, Caffò AO, Damiani R, Albano V. Enhancing academic performance of three boys with autism spectrum disorders and intellectual disabilities through a computer-based program. Life Span Disabil. (2016) 19:153–83.
82. *Hammond JL, Hirt M, Hall SS. Effects of computerized match-to-sample training on emergent fraction-decimal relations in individuals with fragile X syndrome. Res Dev Disabil. (2012) 33:1–11. doi: 10.1016/j.ridd.2011.08.021
83. *Hetzroni OE, Banin I. The effect of educational software, video modelling and group discussion on social-skill acquisition among students with mild intellectual disabilities. J Appl Res Intellect Disabil. (2016) 30:757–73. doi: 10.1111/jar.12271
84. *Raghavendra P, Hutchinson C, Grace E, Wood D, Newman L. “I like talking to people on the computer”: Outcomes of a home-based intervention to develop social media skills in youth with disabilities living in rural communities. Res Dev Disabil. (2018) 76:110–23. doi: 10.1016/j.ridd.2018.02.012
85. *Fatikhova LF, Saifutdiyarova EF. Computer technology in the development of emotional intelligence of children with intellectual disabilities. Rev Eur Stud. (2015) 7:130–5. doi: 10.5539/res.v7n1p130
86. *Kiewik M, VanDerNagel JEL, Engels RCME, DeJong CA. The efficacy of an e-learning prevention program for substance use among adolescents with intellectual disabilities: a pilot study. Res Dev Disabil. (2016) 63:160–6. doi: 10.1016/j.ridd.2016.09.021
87. *Margalit M. Effects of social skills training for students with an intellectual disability. Int J Disabil Dev Educ. (1995) 42:75–85. doi: 10.1080/0156655950420108
88. *Plienis AJ, Romanczyk RG. Analyses of performance, behavior, and predictors for severely disturbed children: a comparison of adult vs computer instruction. Analy Intervent Dev Disabil. (1985) 5:345–56. doi: 10.1016/0270-4684(85)90004-7
89. *Choi KS, Wong PK, Chung WY. Using computer-assisted method to teach children with intellectual disabilities handwashing skills. Disabil Rehabilit Assist Technol. (2012) 7:507–16. doi: 10.3109/17483107.2011.652998
90. *Eden S, Bezer M. Three-dimensions vs. two-dimensions intervention programs: The effect on the mediation level and behavioural aspects of children with intellectual disability. Eur J Spec Needs Educ. (2011) 26:337–53. doi: 10.1080/08856257.2011.593827
91. *Grewal N, Sethi T, Grewal S. Widening horizons through alternative and augmentative communication systems for managing children with special health care needs in a pediatric dental setup. Special Care Dentistr. (2015) 35:114–9. doi: 10.1111/scd.12099
92. *Schuurmans AAT, Nijhof KS, Engels RCME, Granic I. Using a videogame intervention to reduce anxiety and externalizing problems among youths in residential care: an initial randomized controlled trial. J Psychopathol Behav Assess. (2018) 40:344–54. doi: 10.1007/s10862-017-9638-2
93. *Tjus T, Heimann M, Nelson KE. Interaction patterns between children and their teachers when using a specific multimedia and communication strategy: observations from children with autism and mixed intellectual disabilities. Autism. (2001) 5:175–87. doi: 10.1177/1362361301005002007
94. *Vasilevska Petrovska I, Trajkovski V. Effects of a computer-based intervention on emotion understanding in children with autism spectrum conditions. J Autism Dev Disord. (2019) 49:4244–55. doi: 10.1007/s10803-019-04135-5
95. *Fage C, Pommereau L, Consel C, Balland E, Sauzeon H. Tablet-based activity schedule in mainstream environment for children with autism and children with ID. ACM Trans Access Comput. (2016) 8. doi: 10.1145/2854156
96. Courbois Y, Farran EK, Lemahieu A, Blades M, Mengue-Topio H, Sockeel P. Wayfinding behaviour in down syndrome: a study with virtual environments. Res Dev Disabil. (2013) 34:1825–31. doi: 10.1016/j.ridd.2013.02.023
Keywords: intellectual disability, cognitive intervention, behavioral intervention, digital devices, computer, handheld, systematic review
Citation: Torra Moreno M, Canals Sans J and Colomina Fosch MT (2021) Behavioral and Cognitive Interventions With Digital Devices in Subjects With Intellectual Disability: A Systematic Review. Front. Psychiatry 12:647399. doi: 10.3389/fpsyt.2021.647399
Received: 04 January 2021; Accepted: 17 March 2021;
Published: 13 April 2021.
Edited by:
Kerim Munir, Boston Children's Hospital, United StatesReviewed by:
Haris Memisevic, University of Sarajevo, Bosnia and HerzegovinaCaridad López-Granero, University of Zaragoza, Spain
Copyright © 2021 Torra Moreno, Canals Sans and Colomina Fosch. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria Teresa Colomina Fosch, mariateresa.colomina@urv.cat
†ORCID: Marta Torra Moreno orcid.org/0000-0003-0622-4593
Josefa Canals Sans orcid.org/0000-0002-6209-9558
Maria Teresa Colomina Fosch orcid.org/0000-0002-5619-4874