 Lulu Yuan
Lulu Yuan Yuqin Gao
Yuqin Gao Bochen Pan
Bochen Pan Junyan Wang
Junyan Wang Yanjie Wang
Yanjie Wang Caixia Gong
Caixia Gong Weiren Wang
Weiren Wang Xiaohan Li2*
Xiaohan Li2*- 1Liaoning Provincial Key Laboratory of Oral Diseases, Department of Nursing, School and Hospital of Stomatology, China Medical University, Shenyang, China
- 2School of Nursing, China Medical University, Shenyang, China
- 3Shengjing Hospital, China Medical University, Shenyang, China
- 4West China School/Hospital of Stomatology, Sichuan University, Chengdu, China
Background: Resilience has become a hot spot in the field of positive psychology to study life-change events. However, there were little information on resilience among the fathers and mothers of patients with cleft lip and/or palate respectively. The present study aimed to explore and compare the level and potential influential factors associated with resilience among fathers/mothers of patients with cleft lip and/or palate in China.
Method: A cross-sectional study was carried out between April 2019 and July 2020 among fathers/mothers of patients with cleft lip and/or palate in two cleft lip and/or palate treatment centers in China. Sixty Nine fathers and 179 mothers of patients with cleft lip and/or palate were interviewed with a questionnaire on demographic variables and the Resilience Scale-14 (RS-14), Herth Hope Index (HHI), Multidimensional Scale of Perceived Social Support (MSPSS), Revised Life Orientation Test (LOT-R), Parenting Stress Index-Short Form (PSI-SF) and Coping Health Inventory for Parents (CHIP). T-test/univariate one-way ANOVA, Pearson's r, hierarchical linear regression analysis were conducted to explore the influential factors of resilience.
Results: Fathers of patients with cleft lip and/or palate had a higher level of resilience (77.77 ± 14.18) than mothers (74.52 ± 14.33) though without significance. Resilience was positively associated with hope, perceived social support, optimism and coping and negatively correlated with parenting stress both in the fathers and the mothers. Hierarchical linear regression analysis showed that hope (β = 0.400, P < 0.01), coping (β = 0.281, P < 0.05), job status, medical payments (β = −0.240, P < 0.05) were found to be associated with resilience among the fathers of patients with CL/P, and all four variables in the model could explain 42.8% of the variance in resilience; Hope (β = 0.225, P < 0.05), perceived social support (β = 0.194, P < 0.05), the age of patients (β = 0.189, P < 0.05) were found to be associated with resilience among the mothers, and all three variables in the model could explain 27.6% of the variance in resilience.
Conclusion: Our study showed that, in China, fathers of patients with cleft lip and/or palate had a higher level of resilience than mothers though without significance. Hope was the only communal variable strongly associated with resilience among both the fathers and the mothers; besides, coping, job status and medical payments were found to be associated with resilience among the fathers; while perceived social support and the age of patients were found to be associated with resilience among the mothers. The results suggest that enhance hope in parents of patients with cleft lip and/or palate might greatly help improve their resilience. Besides, fathers and mothers need specific intervention to prompt their resilience.
Introduction
Cleft lip and/or palate (CL/P) is one of the most common congenital developmental conditions in humans and the most prevalent developmental condition in the craniomaxillofacial region. Global data show that the overall incidence of cleft lip and/or palate in the world is approximately 1/700 (1). China, located in Asia, is a high-incidence area worldwide (2). China's birth surveillance data from 2000 to 2011 showed that cleft lip with or without cleft palate was the third most prevalent condition in infants in the perinatal period in China (3). Its incidence rate was approximately 1.82‰ and increased year by year (4). Cleft lip and/or palate will not only affect the patient's appearance but also adversely affect the patient's functions of pronunciation, chewing, and swallowing (5). With the development of medical treatment, the nasolabial and palate conditions of patients have greatly improved after sequential treatment. Nevertheless, there are still quite a few patients who cannot work and live like unaffected people. One important reason is that the psychological problems of the patients do not always return to normal with the improvement of shape and function (6).
The psychological problems of patients with cleft lip and/or palate are not inherent; they are the result of long-term growth and development. Ecological systems theory states that people are not independent individuals and cannot exist alone without the environment (7). Individual development should come from the interaction between the individual and the environment. The influence of the environment on individual behavior and psychological development cannot ignore. At the same time, ecological systems theory emphasizes that the growth and development of children and adolescents are affected by environmental factors. For children, especially those with chronic diseases, the most important environment comprises parents and family. Previous studies have shown that the normal development of psychological and social behavior among patients with CL/P depends mostly on the psychological state of their parents (8–10). However, parents of patients with CL/P are under more pressure, including “strike syndrome” (11–13), feeding difficulties (14, 15), difficulties seeking medical treatment (16), a lack of disease information (17), a fear of treatment failure (17), heavy financial burden of treatment (18), growth and academic problems of patients (19–22), marriage and family relationships (23, 24), stigma (25, 26), social isolation (27) and decreased quality of life (28, 29). What's more, so far, the majority of related studies are on mothers, only few on fathers. Mothers and fathers experience parenthood differently. Therefore, the psychological state of the fathers and mothers of patients with CL/P, especially the positive psychological resources, requires our attention and exploration.
Resilience is a very important concept in psychology and has been a research subject for many decades. Studies have shown that resilience is positively related to the level of mental health and negatively related to distress (30, 31). Resilience has also been found to be critical to quality of life (32). Surprisingly, however, little information about resilience in fathers and/or mothers of patients with CL/P is currently available. Considering such immense pressure on fathers and/or mothers of patients with CL/P and the importance of their positive mental resources, resilience should be approached from different perspectives, including psychological methods. Therefore, we aim to fill this knowledge gap with the current study. Furthermore, studies focusing on the relationship between resilience and other psychological factors in caregivers have shown that, in addition to demographic and clinical characteristics, hope (33, 34), social support (35, 36), optimism (37, 38), stress (39, 40) and coping (41) were all associated with resilience, but their relationship in fathers and/or mothers of patients with CL/P is unknown. The hypothesis proposes that resilience is positively associated with hope, social support, optimism and coping, and negatively associated with stress among fathers and/or mothers of patients with CL/P. Accordingly, we will test this hypothesis in the current study. We hope that the findings of our study and, in particular, the identification of influential factors of resilience may have potential value and help shed new light on the healthy development and functional balance of patients with CL/P, their parents, and their families.
Methods
Study Settings
This cross-sectional study was conducted in two cleft lip and/or palate treatment centers in China. Both are provincial regional treatment centers affiliated with medical universities. The first is in northeastern China, and the second is in southwestern China. Data were collected between April 2019 and July 2020. The current research was approved by the Ethical Committee of China Medical University (NO. 2018-27).
Subjects
Respondent inclusion criteria were as follows: (1) Fathers/Mothers of patients with CL/P under 18 years old; (2) agreement to participate in the survey; (3) the capability to understand and complete the questionnaire. The exclusion criteria were as follows: (1) the respondents had other care tasks; (2) the patients had other comorbid serious diseases. The study size was arrived at by using the following formula: The parameters were α = 0.05, Zα = 1.96, σ = 15.39(arrived via the pre-test), and δ = 2; therefore, n = 1.962*15.392/22 = 227.47. Considering that there were invalid questionnaires, the sample size was increased by 10~20%, and the final sample size was 251~273.
Data Collection
The whole process of the study was anonymous and voluntary for the parents. The investigators consisted of four nurses who were trained uniformly by the researcher. At the time of the patient's visit, informed consent was given to their parents. After agreeing to participate, one of the parents filled out a paper version of the questionnaire in a separate, undisturbed space in the hospital, so that the parents would not influence each other in completing the questionnaires. The investigators were responsible for providing explanations for questionnaire items without any inducement. Another trained investigator conducted quality control on the spot and then collected the questionnaires. Epidata software (version 3.1) was used for data entry and double-checking.
Tools
Demographic and clinical characteristics were collected via a general questionnaire. Demographic characteristics consisted of the ages of patients and fathers/mothers, the sex of patients, whether the patient was an only child, developmental status of patients, education level of fathers/mothers, job status of fathers/mothers, religious belief of fathers/mothers, monthly income, residence area, family structure, and medical payments. Clinical variables included patient's type of oral cleft and family history (Whether there is a cleft lip or palate in the family).
Measurement of Resilience
Respondents' resilience was measured with the Resilience Scale-14 (RS-14) (42). The RS-14 includes 14 items, and each item is rated on a 7-point scale, with a total score ranging from 14 to 98. The Chinese version of the RS-14 has been used in previous studies, and the reliability and validity were confirmed (30). Cronbach's alpha coefficient for the total scale of resilience was 0.901 in the present study.
Measurement of Hope
Hope was assessed by the Herth Hope Index (HHI) (43), which contains 3 subscales: temporality and future, positive readiness and expectancy, and interconnectedness. The HHI consists of 12 items, and each item is scored on a 4-point scale. The total HHI score ranges from 12 to 48, and a higher total score reflects a higher level of hope. The Chinese version of the HHI has been found to have good reliability and validity (44). In the current study, Cronbach's α was 0.854.
Measurement of Social Support
The level of perceived social support was assessed by the Chinese version of the Multidimensional Scale of Perceived Social Support (MSPSS) (45), which measures perceived support from three social relationships: fam-ily, friends and significant others (such as relatives and colleagues). The MSPSS includes 12 items rated on a 7-point scale. The total score ranges from 12 to 84, with a higher score indicating higher social support. The scale had good reliability and validity among various Chinese populations (46, 47). In this study, Cronbach's α of the MSPSS was 0.928.
Measurement of Optimism
Optimism was assessed by the 10-item Revised Life Orientation Test (LOT-R), which was designed by Scheier et al. (48). The LOT-R consists of ten items using a 5-point rating system, three of which are for optimism, three of which are for pessimism, and the other four items serve as fillers. A higher score indicates a higher level of optimism. The LOT-R has shown good reliability and validity among various Chinese populations (47). Cronbach's α was 0.600 in the current research.
Measurement of Parenting Stress
Parenting stress was assessed by the Parenting Stress Index-Short Form (PSI-SF) (49), which contains 3 subscales: parent distress, parent-child dysfunctional interaction, and difficult child. The PSI-SF consists of 36 items, and each item is scored using a 5-point scale, with a total score ranging from 36 to 180. Higher scores indicate a higher level of parenting stress. The Chinese version has demonstrated good reliability and validity (50). Cronbach's α was 0.940 in this study.
Measurement of Coping
The Coping Health Inventory for Parents (CHIP) was developed by Mc Cubbin (51) to measure what coping strategies respondents used to maintain normal family life when there was a child with chronic disease in the family. The CHIP is a 45-item scale rated on a 5-point scale, with a total score ranging from 45 to 225. Higher scores indicate a higher level of coping. The scale has been widely used among the Chinese population (52). Cronbach's α was 0.940 in the current study.
Statistical Analyses
Statistical Package for Social Sciences (SPSS 22.0 for Windows) was used to conduct data analyses. Significance for all statistical tests was set at 0.05 (2-tailed). The normality and homogeneity of variances were first tested for each continuous variable. Independent sample T-tests and one-way ANOVA were used to describe distributions of resilience in categorical demographic and clinical variables among fathers and mothers. Pearson's r test was conducted to test the correlations among hope, perceived social support, optimism, parenting stress, coping and resilience. Hierarchical linear regression analyses were conducted to test the study hypotheses. The variables with P < 0.2 in one-way ANOVA/t-test were entered into step 1 of the hierarchical regression analysis as control variables in order to not overfit the regression models (53). Then, the independent variables (hope, perceived social support, optimism, parenting stress, and the coping of the parents) were also entered into step 2 of the hierarchical regression. Variables were entered in the regression analysis at P < 0.05 and removed from the model at P > 0.10. Multicollinearity diagnostic tests were carried out by the Tolerance and variance inflation factor (VIF). Data provided in the regression models included the standardization regression coefficient (β), R2, adjusted R2 (Adj. R2), R2-change and F value.
Results
Descriptive Statistics
In the current study, 262 questionnaires were distributed. Among them, seven participants refused to attend the survey, seven questionnaires were considered invalid. The number of valid questionnaires was 248, yielding an effective response rate of 94.66%.
Among the 248 participants, 69 (27.8%) were fathers, and 179 (72.2%) were mothers. The mean age of the patients was 7.70 years (SD = 5.76, range 0.08–18). In terms of the clinical variables, among all the patients, 53 (21.4%) had cleft lip, 77 (31%) had cleft palate and 118 (47.6%) had both cleft lip with cleft palate. Only 13 (5.2%) patients had a family history of cleft lip and/or palate. The demographic and clinical characteristics and the level of resilience among fathers/mothers of patients with CL/P were described in Table 1.
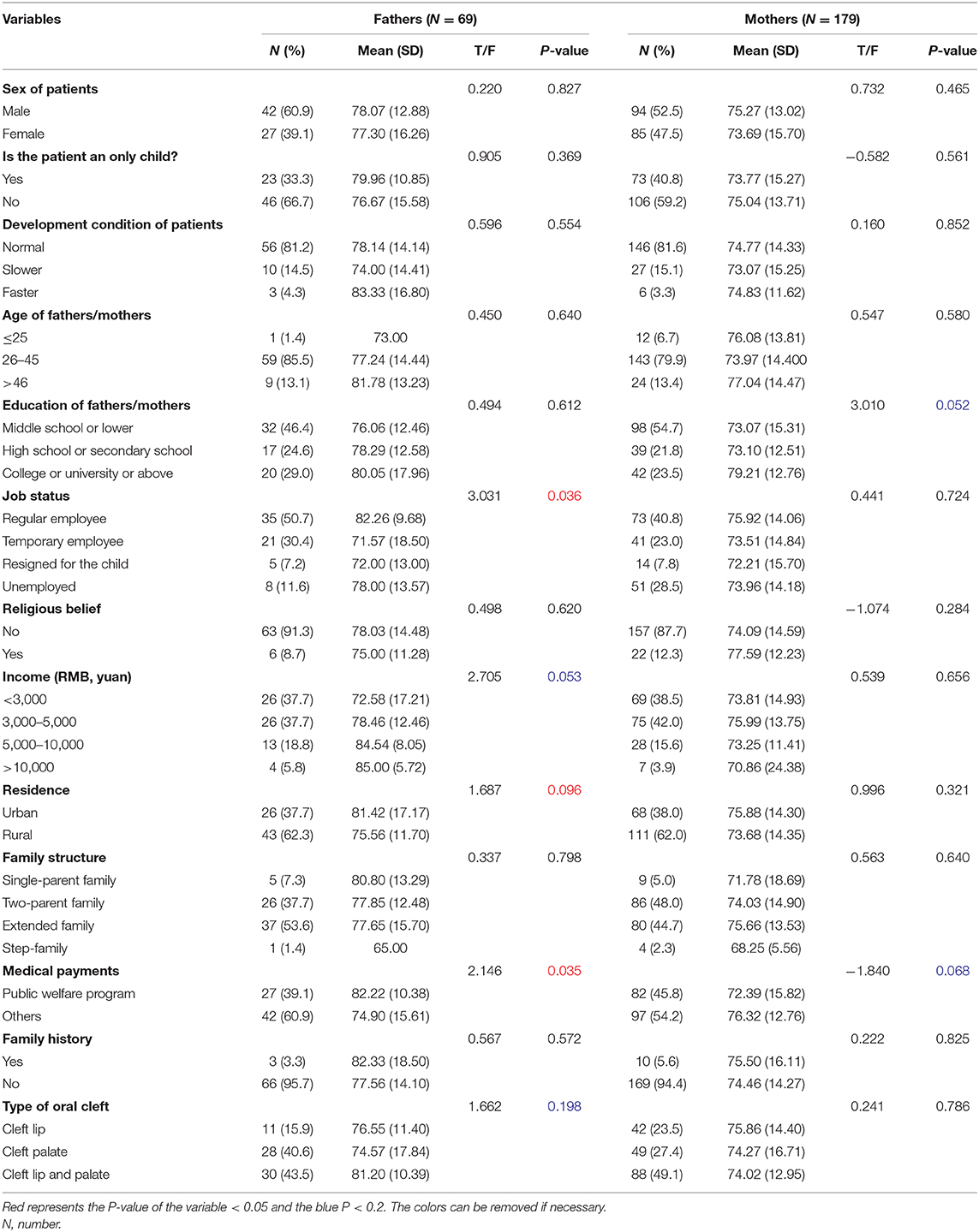
Table 1. Demographic and clinical characteristics and the level of resilience among fathers and mothers of patients with CLP (n = 248).
Resilience Level
Although there was no significant difference in the level of resilience between fathers and mothers of patients with CL/P, the resilience level of fathers was higher than that of mothers, which was were described in Table 2.

Table 2. Level and comparison of resilience between fathers and mothers.
Correlation Among Continuous Variables
The results of the correlation analysis of hope, perceived social support, optimism, parenting stress, and coping with resilience among fathers of patients with CL/P are presented in Table 3. Resilience was positively associated with hope (r = 0.533, p < 0.001), perceived social support (r = 0.325, p < 0.01), optimism (r = 0.261, p < 0.01) and coping (r = 0.462, p < 0.001) and negatively correlated with parenting stress (r = −0.312, p < 0.01).
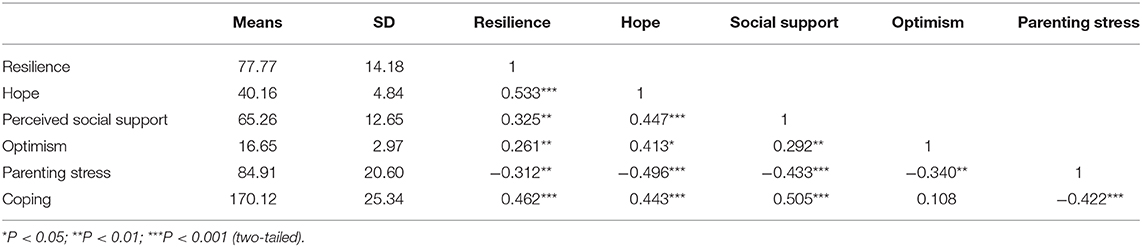
Table 3. Descriptive statistics and correlations in continuous variables among fathers (n = 69).
The results of the correlation analysis of hope, perceived social support, optimism, parenting stress, and coping with resilience among mothers of patients with CL/P are presented in Table 4. Resilience was positively associated with hope (r = 0.448, p < 0.001), perceived social support (r = 0.420, p < 0.01), optimism (r = 0.226, p < 0.01) and coping (r = 0.357, p < 0.001) and negatively correlated with parenting stress (r = −0.382, p < 0.001).
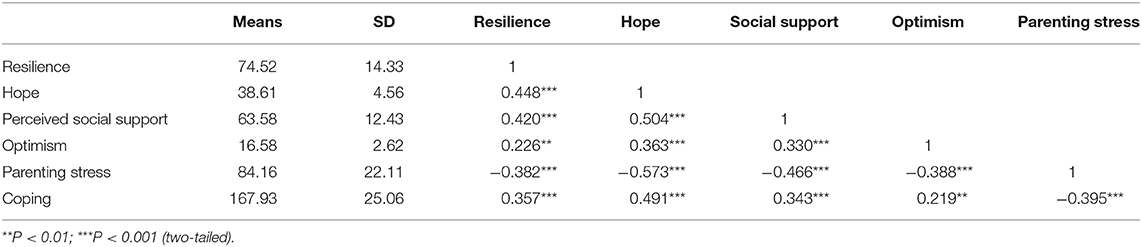
Table 4. Descriptive statistics and correlations in continuous variables among mothers (n = 179).
Hierarchical Linear Regression Analysis
Hierarchical linear regression analysis was conducted to identify the influential factors of resilience among the fathers/mothers of patients with CL/P. Variables that were significantly associated with resilience in the univariate analyses, and variables related to the psychology of parents were included in the multiple regression analysis.
Among fathers, demographic variables (the age of patients, job status, income, residence, medical payments, and type of oral cleft), hope, perceived social support, optimism, parenting stress, and coping were included in the regression analysis. The results of the analysis are shown in Table 5. Hope (β = 0.400, P < 0.01), coping (β = 0.281, P < 0.05), job status, medical payments (β = −0.240, P < 0.05) were found to be associated with resilience among the fathers of patients with CL/P, and all four variables in the model could explain 42.8% of the variance in resilience.
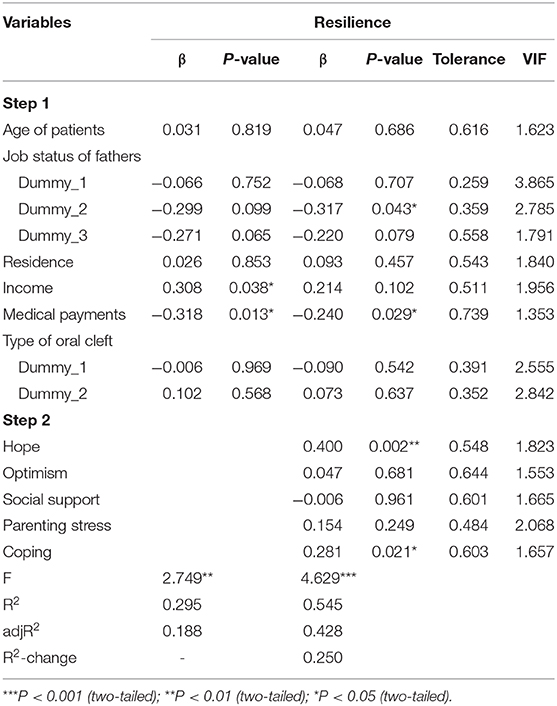
Table 5. Hierarchical linear regression analysis on results of resilience among fathers of patients with CL/P (n = 69).
Among mothers, demographic variables (the age of patients, education, and medical payments), hope, perceived social support, optimism, parenting stress, and coping were included in the regression analysis. The results of the analysis are shown in Table 6. Hope (β = 0.225, P < 0.05), perceived social support (β = 0.194, P < 0.05), the age of patients (β = 0.189, P < 0.05) were found to be associated with resilience among the mothers of patients with CL/P, and all four variables in the model could explain 27.6% of the variance in resilience.
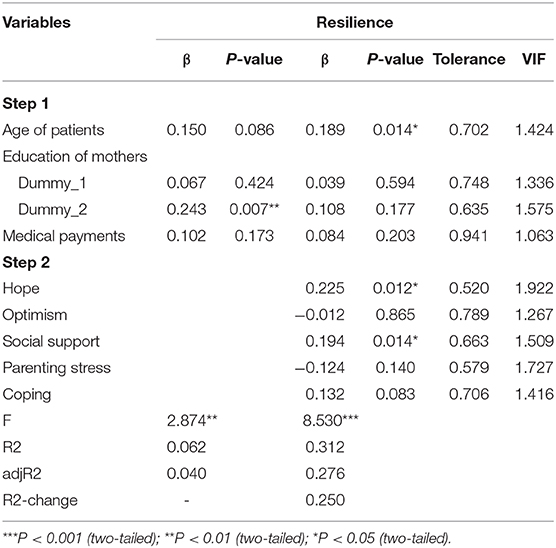
Table 6. Hierarchical linear regression analysis on results of resilience among mothers of patients with CL/P (n = 179).
Discussion
The current study explored the level and influential factors of resilience among fathers and mothers of patients with CL/P.
Resilience Levels Among Fathers and Mothers of Patients With CL/P
The level of resilience in the study was similar to (54) or higher (55) than previous studies of caregivers of children with chronic diseases. Besides, the resilience level of fathers was higher than that of mothers, though there was no significant difference. The finding was significant due to the lack of information available in the literature about resilience in parents of patients with CL/P. This result is explainable. On one hand, resilience emphasizes that individuals can actively respond and adapt well in the face of negative events such as threats, adversity, or pressure (56–58), in which fathers have certain advantage over mothers. As parents accept and work hard on the disease gradually, their resilience level will become higher. On the other hand, CL/P is not a life-threatening disease but a disease with a promising cure. The patient's condition will improve as the treatment progresses. Therefore, in our clinical work, we should pay more special attention to the psychological status of parents of young patients.
At the same time, we noticed that more mothers (179, 72.2%) were recruited in the study than fathers (69, 27.8%). The result came as no surprise to us, because quite many studies have shown the similarly information, both in parents of patients with CL/P (24, 59) and families having a child with chronic conditions (60). This phenomenon resulted from the fact that mothers usually took more responsibilities on child caring in families in China, in comparison with fathers. What's more, more fathers were employed than mothers in this study, similar to other research (12, 61). Besides, mothers had higher levels of parental involvement behaviors than fathers (62).
Factors Associated With Resilience Among Fathers and Mothers of Patients With CL/P
In the current study, hope, coping, job status and medical payments were found to be associated with resilience among the fathers of patients with CL/P. Hope, perceived social support and the age of patients were found to be associated with resilience among the mothers of patients with CL/P.
According to the results of logistic regression analysis, hope was the only communal variable strongly associated with resilience among both fathers and mothers of patients with CL/P, which was similar to the results in previous studies on the resilience of caregivers of children with chronic diseases (63, 64). Hope has been confirmed to be related to almost all health outcomes (65). It is part of the psychological capitals of caregivers. Hope is an important resilience factor when caregivers cope with the care pressure of patients, which can help caregivers alleviate negative psychological distress. Lloyd's research found that as an influential factor of mental resilience, a low level of hope could predict the anxiety and depression level of parents of children with intellectual disabilities (34). In addition, hope is an important influencing factor in the development of caregivers' resilience. In a longitudinal study, hopefulness was found to be capable of predicting resilience among hereditary colorectal cancer patients (66). Therefore, enhancing the level of hope may become an important strategy to increase the level of resilience among both fathers and mothers of patients with CL/P in China.
In addition to hope, we found that coping was another positive psychological resource for the resilience among fathers of patients with CL/P. There were rare studies on resilience of fathers. Fortunately, this result was consistent with previous findings on the psychological conditions among caregivers and mothers of patients with CL/P (67, 68). Active coping strategies are the behaviors taken by caregivers under the condition of good psychological adjustment, and the implementation of active coping strategies, in turn, will help to improve the psychological condition of themselves. Then, a virtuous circle forms, and the growth of parents' psychological capital is prompted. Nadia Hasanzadeh's study on mothers of patients with CL/P confirmed this and further pointed out that positive coping strategies not only help improve the mother's psychological status but also benefit the mother's parent-child behavior (68). Therefore, active coping strategies should be valued, and we suggest that in clinical care, clinicians and nurses should help fathers of patients with CL/P develop active coping plans to adjust their psychological pressure and relieve negative emotions.
In this study, we also found that perceived social support made a positive contribution to the resilience of mothers of patients with CL/P. The positive effect of social support has been confirmed in many studies, both studies on the resilience of caregivers with chronic diseases (35, 69) and studies on psychological conditions of caregivers of patients with CL/P (12, 67, 70). Perceived social support is a part of the positive psychological capital of almost all patients and caregivers. People with higher levels of perceived social support have more resources they can use to care for the patients, which lightens the burden of care and psychological burden. The level of resilience and psychological status are naturally improved. However, it is worth noting the results of two qualitative studies (35, 36). Their findings showed that the support of family and friends was not always sufficient to promote the psychological resilience of caregivers, and the support function helped to enhance resilience only when it was considered to match the needs. Therefore, the specific role of perceived social support needs further study and discussion.
On the other hand, it is interesting to note that some of the demographic variables have been demonstrated specifically associated with the resilience of parents of patients with CL/P.
First, we found that job status and medical payments were of great significance for the resilience of the fathers. In the study, fathers with regular employee had the highest level of resilience than other status. Regular employee meant a stable income. Besides, fathers of patients with public welfare program had higher level of resilience than others. Having public welfare program could be interpreted as less financial pressure. In other words, these two variables related to the fathers' resilience suggests that the fathers bear more economic pressure in the treatment of children. This is in line with the role of fathers in most Chinese families.
Finally, it was not surprising to find that the age of patients was an important factor for the resilience of the mothers. This has been confirmed not only in the study of the resilience of caregivers of children with chronic diseases (71) but also in the study of the psychological conditions of caregivers of patients with CL/P (28). In the study, the age of patients was associated with resilience of the mothers, not the fathers, possibly for the primary caregivers for CL/P was often the mothers. The resilience of mothers increases with the age of patients. It is a good phenomenon, mainly because as the patient grows up and the treatment progresses, the mothers can take care of their children more easily. However, one problem that we cannot ignore is the patient's psychological and developmental problems. The improvement of clinical symptoms does not mean the complete end of the child's treatment. In clinical practice, we have also found that many parents of patients with CL/P pay too much attention to the improvement of their children's appearance and function while ignoring their children's performance in interpersonal communication, personality development and school achievement and attribute the patients' inadaptability in these aspects only to different personalities and characteristics. Previous studies have also found similar problems (72–74). In summary, although the burden of life care and medical care for parents is reduced as patients with CL/P grow up, we should still remind parents and provide parents with relevant professional services to promote the healthy growth of patients' psychology and society.
However, the current study results were partially inconsistent with our hypothesis in that optimism and parenting stress showed no significant relations neither with fathers nor mothers. Therefore, further research is still needed to explore the exact mechanism of the two variables.
Strength and Limitations
The current study aimed to identify the potential influencing factors associated with resilience in fathers and mothers of patients with CL/P. In this respect, our study has added some new information. The results provided evidence that hope was the only communal variable strongly associated with resilience among both the fathers and the mothers; coping, job status and medical payments were found to be associated with resilience among the fathers; while perceived social support and the age of patients were found to be associated with resilience among the mothers. In addition, our study provided clinical information for the definition of resilience. The results of our study showed that the age of patients was a vital factor for the resilience of the mothers. This result indicated that resilience may be a developable quality for dealing with adversity.
Due to the cross-sectional design, the causal relationship could not be confirmed. Future studies should be carried out to assess whether interventions could improve the level of resilience among fathers and mothers of patients with CL/P. In addition, we focused only on the associations of resilience with hope, optimism, parenting stress, coping and perceived social support; other factors that may be important to consider for resilience were not included. Besides, the long number of questions may represent a limitation for the quality of response. Moreover, a larger sample is needed to improve the representativeness. Despite some limitations, our study provided important new information on resilience in parents of patients with CL/P, and it had useful theoretical and clinical implications.
Conclusions
Our study showed that, in China, fathers of patients with CL/P had a higher level of resilience than mothers though without significance. Hope was the only communal variable strongly associated with resilience among both fathers and mothers of patients with CL/P; besides, coping, job status and medical payments were found to be associated with resilience among the fathers; while perceived social support and the age of patients were found to be associated with resilience among the mothers of patients with CL/P.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Committee on Human Experimentation of China Medical University (2018-27). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
LY and XL were responsible for conception and design of the study. YG gave directions to the study. LY, JW, YW, and CG performed data extraction. LY did the data analysis and wrote the manuscript. BP and WW contributed to the revision of the manuscript. All authors have reviewed the manuscript and given final approval of the version to be published.
Funding
This study was funded by the project of Education Department of Liaoning Province (LJKR0281) and the project of College of Nursing, China Medical University (2017HL-17). The funding bodes played no role in the design of study, collection, analysis and interpretation of data, or in writing the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank all our patients who were willing to take part in the study. We would also like to thank colleagues at the Maxillofacial Surgery Department of School and Hospital of Stomatology of China Medical University and West China School/ Hospital of Stomatology Sichuan University for their help with data collection. Finally, we would like to thank Education Department of Liaoning Province and College of Nursing for the funding of this study.
References
1. Dixon MJ, Marazita ML, Beaty TH, Murray JC. Cleft lip and palate: understanding genetic and environmental influences. Nat Rev Genet. (2011) 12:167–78. doi: 10.1038/nrg2933
2. Chang WJ, See LC, Lo LJ. Time trend of incidence rates of cleft lip/palate in Taiwan from 1994 to 2013. Biomed J. (2016) 39:150–4. doi: 10.1016/j.bj.2015.10.003
3. Ministry Ministry of Health PRC. Report on Prevention And Treatment Of Birth Defects In China. (2012). Available online at: http://www.gov.cn/gzdt/att/att/site1/20120912/1c6f6506c7f811bacf9301.pdf
4. Zhao RH. Epidemiological analysis of congenital cleft lip and palate. Chin Pract Med. (2011) 6:223–4. doi: 10.3969/j.issn.1673-7555.2011.16.183
5. Zhang JN, Song FQ, Zhou SN, Zheng H, Peng LY, Zhang Q, et al. Analysis of single-nucleotide polymorphism of Sonic hedgehog signaling pathway in non-syndromic cleft lip and/or palate in the Chinese population. Beijing Da Xue Xue Bao Yi Xue Ban. (2019) 51:556–63. doi: 10.19723/j.issn.1671-167X.2019.03.027
6. Shi B, Zheng Q. It is necessary to do psychological intervention for patients with cleft lip and palate. Hua Xi Kou Qiang Yi Xue Za Zhi. (2010) 28:345–7. doi: 10.3969/j.issn.1000-1182.2010.04.001
7. Liu J, Meng HM. Understanding on the ecological system theory of bronfenbrenner developmental psychology. Chin J Health Psychol. (2009) 17:250–2. doi: 10.13342/j.cnki.cjhp.2009.02.045
8. Field T, Healy B, Goldstein S, Perry S, Bendell D, Schanberg S, et al. Infants of depressed mothers show “depressed” behavior even with nondepressed adults. Child Dev. (1988) 59:1569–79. doi: 10.2307/1130671
9. Weng GZ, Xu L, Liao CX. Status quo of research on psychological state of parents of children with cheilopalatognathus. Chin Nurs Res. (2009) 23:2920–1. doi: 10.3969/j.issn.1009-6493.2009.32.003
10. Sank JR, Berk NW, Cooper ME, Marazita ML. Perceived social support of mothers of children with clefts. Cleft Palate Craniofac J. (2003) 40:165–71. doi: 10.1597/1545-1569_2003_040_0165_pssomo_2.0.co_2
11. O'Hanlon K, Camic PM, Shearer J. Factors associated with parental adaptation to having a child with a cleft lip and/or palate: the impact of parental diagnosis. Cleft Palate Craniofac J. (2012) 49:718–29. doi: 10.1597/10-018
12. Ueki S, Fujita Y, Kitao M, Kumagai Y, Ike M, Niinomi K, et al. Resilience and difficulties of parents of children with a cleft lip and palate. Jpn J Nurs Sci. (2019) 16:232–7. doi: 10.1111/jjns.12231
13. Nur Yilmaz RB, Germec Cakan D, Turkyilmaz Uyar E. Maternal and paternal well-being during nasoalveolar molding and primary surgery periods. J Craniofac Surg. (2019) 30:2227–32. doi: 10.1097/SCS.0000000000006028
14. Britton KF, McDonald SH, Welbury RR. An investigation into infant feeding in children born with a cleft lip and/or palate in the West of Scotland. Eur Arch Paediatr Dent. (2011) 12:250–5. doi: 10.1007/BF03262817
15. Marques I, Garla L, Neto J, Silva M, Graciano M, Moorhead J, et al. Longitudinal study of growth of children with unilateral cleft-lip palate from birth to two years of age. Cleft Palate Craniofac J. (2009) 46:603–9. doi: 10.1597/08-105.1
16. Bennett KG, Ranganathan K, Patterson AK, Baker MK, Vercler CJ, Kasten SJ, et al. Caregiver-reported outcomes and barriers to care among patients with cleft lip and palate. Plast Reconstr Surg. (2018) 142:884e−91. doi: 10.1097/PRS.0000000000004987
17. Crerand CE, Rosenberg J, Magee L, Stein MB, Wilson-Genderson M, Broder HL. Parent-Reported Family Functioning among Children with Cleft Lip/Palate. Cleft Palate Craniofac J. (2015) 52:651–9. doi: 10.1597/14-050
18. Bluestone CD. Studies in otitis media: children's hospital of Pittsburgh-university of pittsburgh progress report−2004. Laryngoscope. (2004) 114:1–26. doi: 10.1097/01.mlg.0000148223.45374.ec
19. Bruneel L, Bettens K, Van Lierde K. The relationship between health-related quality of life and speech in patients with cleft palate. Int J Pediatr Otorhinolaryngol. (2019) 120:112–7. doi: 10.1016/j.ijporl.2019.02.018
20. Roberts RM, Mathias JL, Wheaton P. Cognitive functioning in children and adults with nonsyndromal cleft lip and/or palate: a meta-analysis. J Pediatr Psychol. (2012) 37:786–97. doi: 10.1093/jpepsy/jss052
21. Cavalheiro MG, Lamônica DAC, de Vasconsellos Hage SR, Maximino LP. Child development skills and language in toddlers with cleft lip and palate. Int J Pediatr Otorhinolaryngol. (2019) 116:18–21. doi: 10.1016/j.ijporl.2018.10.011
22. Persson M, Becker M, Svensson H. Academic achievement in individuals with cleft: a population-based register study. Cleft Palate Craniofac J. (2012) 49:153–9. doi: 10.1597/09-047
23. Speltz ML, Morton K, Goodell EW, Clarren SK. Psychological functioning of children with craniofacial anomalies and their mothers: follow-up from late infancy to school entry. Cleft Palate Craniofac J. (1993) 30:482–9. doi: 10.1597/1545-1569_1993_030_0482_pfocwc_2.3.co_2
24. Sischo L, Clouston SA, Phillips C, Broder HL. Caregiver responses to early cleft palate care: a mixed method approach. Health Psychol. (2016) 35:474–82. doi: 10.1037/hea0000262
25. Gyimah SO. Cultural background and infant survival in Ghana. Ethn Health. (2006) 11:101–20. doi: 10.1080/13557850500460314
26. Loh J, Ascoli M. Cross-cultural attitudes and perceptions towards cleft lip and palate deformities. World Cult Psychiatry Res Rev. (2011) 6:127–34.
27. Bonsu AB, Dzomeku VM, Apiribu F, Obiri-Yeboah S, Asamoah B, Mensah KB, et al. Having a child with orofacial cleft: initial reaction and psychosocial experiences of Ghanaian mothers. Int J Afr Nurs Sci. (2018) 8:132–40. doi: 10.1016/j.ijans.2018.05.003
28. Aslan BI, Gulsen A, Tirank SB, Findikcioglu K, Uzuner FD, Tutar H, et al. Family functions and life quality of parents of children with cleft lip and palate. J Craniofac Surg. (2018) 29:1614–8. doi: 10.1097/SCS.0000000000004611
29. Awoyale T, Onajole AT, Ogunnowo BE, Adeyemo WL, Wanyonyi KL, Butali A. Quality of life of family caregivers of children with orofacial clefts in Nigeria: a mixed-method study. Oral Dis. (2016) 22:116–22. doi: 10.1111/odi.12379
30. Gao Y, Yuan L, Pan B, Wang L. Resilience and associated factors among Chinese patients diagnosed with oral cancer. BMC Cancer. (2019) 19:447. doi: 10.1186/s12885-019-5679-0
31. Rosenberg AR, Wolfe J, Bradford MC, Shaffer ML, Yi-Frazier JP, Curtis JR, et al. Resilience and psychosocial outcomes in parents of children with cancer. Pediatr Blood Cancer. (2014) 61:552–7. doi: 10.1002/pbc.24854
32. Cho EA, Oh HE. Effects of laughter therapy on depression, quality of life, resilience and immune responses in breast cancer survivors. J Korean Acad Nurs. (2011) 41:285–93. doi: 10.4040/jkan.2011.41.3.285
33. Duggleby WD, Williams A, Holstlander L, Thomas R, Cooper D, Hallstrom LK, et al. Hope of rural women caregivers of persons with advanced cancer: guilt, self-efficacy and mental health. Rural Remote Health. (2014) 14:2561. doi: 10.22605/RRH2561
34. Lloyd TJ, Hastings R. Hope as a psychological resilience factor in mothers and fathers of children with intellectual disabilities. J Intellect Disabil Res. (2009) 53:957–68. doi: 10.1111/j.1365-2788.2009.01206.x
35. Donnellan WJ, Bennett KM, Soulsby LK. What are the factors that facilitate or hinder resilience in older spousal dementia carers? a qualitative study. Aging Ment Health. (2015) 19:932–9. doi: 10.1080/13607863.2014.977771
36. Donnellan WJ, Bennett KM, Soulsby LK. Family close but friends closer: exploring social support and resilience in older spousal dementia carers. Aging Ment Health. (2017) 21:1222–8. doi: 10.1080/13607863.2016.1209734
37. Peer JW, Hillman SB. Stress and resilience for parents of children with intellectual and developmental disabilities: a review of key factors and recommendations for practitioners. J Policy Pract Intellect Disabil. (2014) 11:92–8. doi: 10.1111/jppi.12072
38. Gardner J, Harmon T. Exploring resilience from a parent's perspective:a qualitative study of six resilient mothers of children with an intellectual disability. Aust Soc Work. (2002) 55:60–8. doi: 10.1080/03124070208411672
39. Ekas N, Whitman TL. Autism symptom topography and maternal socioemotional functioning. Am J Intellect Dev Disabil. (2010) 115:234–49. doi: 10.1352/1944-7558-115.3.234
40. Sarrionandia A, Ramos-Díaz E, Fernández-Lasarte O. Resilience as a mediator of emotional intelligence and perceived stress: a cross-country study. Front Psychol. (2018) 9:2653. doi: 10.3389/fpsyg.2018.02653
41. Ruiz-Robledillo N, De Andrés-García S, Pérez-Blasco J, González-Bono E, Moya-Albiol L. Highly resilient coping entails better perceived health, high social support and low morning cortisol levels in parents of children with autism spectrum disorder. Res Dev Disabil. (2014) 35:686–95. doi: 10.1016/j.ridd.2013.12.007
42. Wagnild GM, Young HM. Development and psychometric evaluation of the Resilience Scale. J Nurs Meas. (1993) 1:165–78.
43. Herth K. Development and refinement of an instrument to measure hope. Sch Inq Nurs Pract. (1991) 5:39–51.
44. Wang YH. Study on feasibility of Chinese version of herth hope index for cancer patients. J Chin Nurs Res. (2010) 24:20–1. doi: 10.3969/j.issn.1009-6493.2010.01.008
45. Dahlem NW, Zimet GD, Walker RR. The Multidimensional Scale of Perceived Social Support: a confirmation study. J Clin Psychol. (1991) 47:756–61. doi: 10.1002/1097-4679(199111)47:6<756::aid-jclp2270470605>3.0.co;2-l
46. Liu L, Yang YL, Wang ZY, Wu H, Wang Y, Wang L. Prevalence and positive correlates of posttraumatic stress disorder symptoms among Chinese patients with hematological malignancies: a cross-sectional study. PLoS ONE. (2015) 10:e0145103. doi: 10.1371/journal.pone.0145103
47. Yang YL, Liu L, Li MY, Shi M, Wang L. Psychological disorders and psychosocial resources of patients with newly diagnosed bladder and kidney cancer: a cross-sectional study. PLoS ONE. (2016) 11:e0155607. doi: 10.1371/journal.pone.0155607
48. Scheier MF, Carver CS, Bridges MW. Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): a reevaluation of the life orientation test. J Pers Soc Psychol. (1994) 67:1063–78. doi: 10.1037/0022-3514.67.6.1063
49. Abidin RR. Parenting Stress Index-Professional Manual 3rd Ed. Lutz FL: Psychological Assessment Resource (1995).
50. Ren WX. A Study On The Relationship Among Parental Stress, Coping Strategies And Parent-Child Relationship Satisfaction Of Mothers. Taiwan: National Taiwan Normal University (1995).
51. Mccubbin HI, Mccubbin MA, Patterson JM, Elizabeth Cauble A, Wilson LR, Warwick WCHIP. Coping health inventory for parents:an assessment of parental coping patterns in the care of the chronically ill child. J Marriage Fam Couns. (1983) 45:359–70. doi: 10.2307/351514
52. Li Y, Wei M. Study of application of the chinese version of CHIP for parents of children with chronic disease. Chin J Nurs. (2007) 42:972–5.
53. Babyak MA. What you see may not be what you get: a brief, nontechnical introduction to overfitting in regression-type models. Psychosom Med. (2004) 66:411–21. doi: 10.1097/00006842-200405000-00021
54. Liu PP, Yin P, Zhu YH, Zhang S, Sheng GM. The correlation of family resilience with sleep quality and depression of parents of children with epilepsy. J Pediatr Nurs. (2021) 56:e49–454. doi: 10.1016/j.pedn.2020.07.016
55. Ye ZJ, Qiu HZ, Li PF, Liang MZ, Wang SN, Quan XM. Resilience model for parents of children with cancer in mainland China-an exploratory study. Eur J Oncol Nurs. (2017) 27:9–16. doi: 10.1016/j.ejon.2017.01.002
56. Connor KM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. (2003) 18:76–82. doi: 10.1002/da.10113
57. Haase JE, Heiney SP, Ruccione KS, Stutzer C. Research triangulation to derive meaning-based quality-of-life theory: adolescent resilience model and instrument development. Int J Cancer Suppl. (1999) 12:125–31. doi: 10.1002/(sici)1097-0215(1999)83:12+<125::aid-ijc22>3.0.co;2-7
58. Richardson GE. The metatheory of resilience and resiliency. J Clin Psychol. (2002) 58:307–21. doi: 10.1002/jclp.10020
59. Nelson P, Glenny AM, Kirk S, Caress AL. Parents' experiences of caring for a child with a cleft lip and/or palate: a review of the literature. Child Care Health Dev. (2012) 38:6–20. doi: 10.1111/j.1365-2214.2011.01244.x
60. Theule J, Cheung K, Aberdeen K. Children's ADHD interventions and parenting stress: a meta-analysis. J Child Fam Stud. (2018) 27:2744–56. doi: 10.1007/s10826-018-1137-x
61. Bourke-Taylor HM, Lee D-CA, Tirlea L, Joyce K, Morgan P, Haines TP. Interventions to improve the mental health of mothers of children with a disability: systematic review, meta-analysis and description of interventions. J Autism Dev Disord. (2021) 51:3690–706. doi: 10.1007/s10803-020-04826-4
62. Zaidman-Zait A, Most T, Tarrasch R, Haddad E. Mothers' and fathers' involvement in intervention programs for deaf and hard of hearing children. Disabil Rehabil. (2018) 40:1301–9. doi: 10.1080/09638288.2017.1297491
63. Mednick L, Cogen F, Henderson C, Rohrbeck CA, Kitessa D, Streisand R. Hope more, worry less: hope as a potential resilience factor in mothers of very young children with type 1 diabetes. Child Health Care. (2007) 36:385–96. doi: 10.1080/02739610701601403
64. Horton TV, Wallander JL. Hope and social support as resilience factors against psychological distress of mothers who care for children with chronic physical conditions. Rehabil Psychol. (2001) 46:382–99. doi: 10.1037/0090-5550.46.4.382
65. Wang WL, Zhou YQ, Chai NN, Li GH, Liu DW. Mediation and moderation analyses: exploring the complex pathways between hope and quality of life among patients with schizophrenia. BMC Psychiatry. (2020) 20:22. doi: 10.1186/s12888-020-2436-5
66. Ho SM, Ho JW, Bonanno GA, Chu AT, Chan EM. Hopefulness predicts resilience after hereditary colorectal cancer genetic testing: a prospective outcome trajectories study. BMC cancer. (2010) 10:279. doi: 10.1186/1471-2407-10-279
67. Baker SR, Owens J, Stern M, Willmot D. Coping strategies and social support in the family impact of cleft lip and palate and parents' adjustment and psychological distress. Cleft Palate Craniofac J. (2009) 46:229–36. doi: 10.1597/08-075.1
68. Hasanzadeh N, Khoda MO, Jahanbin A, Vatankhah M. Coping strategies and psychological distress among mothers of patients with nonsyndromic cleft lip and palate and the family impact of this disorder. J Craniofac Surg. (2014) 25:441–5. doi: 10.1097/SCS.0000000000000483
69. Yu T. Influencing Factors and Intervention of Psychological Resilience of Parents of Autistic Children. Suzhou: Suzhou University (2017).
70. King G, Cathers T, Brown E, Specht JA, Willoughby C, Polgar JM, et al. Turning points and protective processes in the lives of people with chronic disabilities. Qual Health Res. (2003) 13:184–206. doi: 10.1177/1049732302239598
71. Hartley SL, Barker ET, Seltzer MM, Greenberg JS, Floyd FJ. Marital satisfaction and parenting experiences of mothers and fathers of adolescents and adults with autism. Am J Intellect Dev Disabil. (2011) 116:81–95. doi: 10.1352/1944-7558-116.1.81
72. Wehby GL, Collett BR, Barron S, Romitti P, Ansley T. Children with oral clefts are at greater risk for persistent low achievement in school than classmates. Arch Dis Child. (2015) 100:1148–54. doi: 10.1136/archdischild-2015-308358
73. Collett BR, Speltz ML. Social-emotional development of infants and young children with orofacial clefts. Infants Young Child. (2006) 19:262–91. doi: 10.1097/00001163-200610000-00002
Keywords: cleft lip and/or palate, fathers, mothers, resilience, positive psychology
Citation: Yuan L, Gao Y, Pan B, Wang J, Wang Y, Gong C, Wang W and Li X (2022) Resilience and Related Factors: A Comparison of Fathers and Mothers of Patients With Cleft Lip and/or Palate in China. Front. Psychiatry 12:791555. doi: 10.3389/fpsyt.2021.791555
Received: 08 October 2021; Accepted: 20 December 2021;
Published: 13 January 2022.
Edited by:
Delin Sun, Duke University, United StatesReviewed by:
Rosa Helena Wanderley Lacerda, Federal University of Paraíba, BrazilGopalkumar Rakesh, Duke University, United States
Copyright © 2022 Yuan, Gao, Pan, Wang, Wang, Gong, Wang and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lulu Yuan, 18040229859@sina.cn; Xiaohan Li, xhli@cmu.edu.cn