
Plasma Exosome Profile in ST-Elevation Myocardial Infarction Patients with and without Out-of-Hospital Cardiac Arrest

 , , , , , ,
, , , , , ,  , and
, and
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
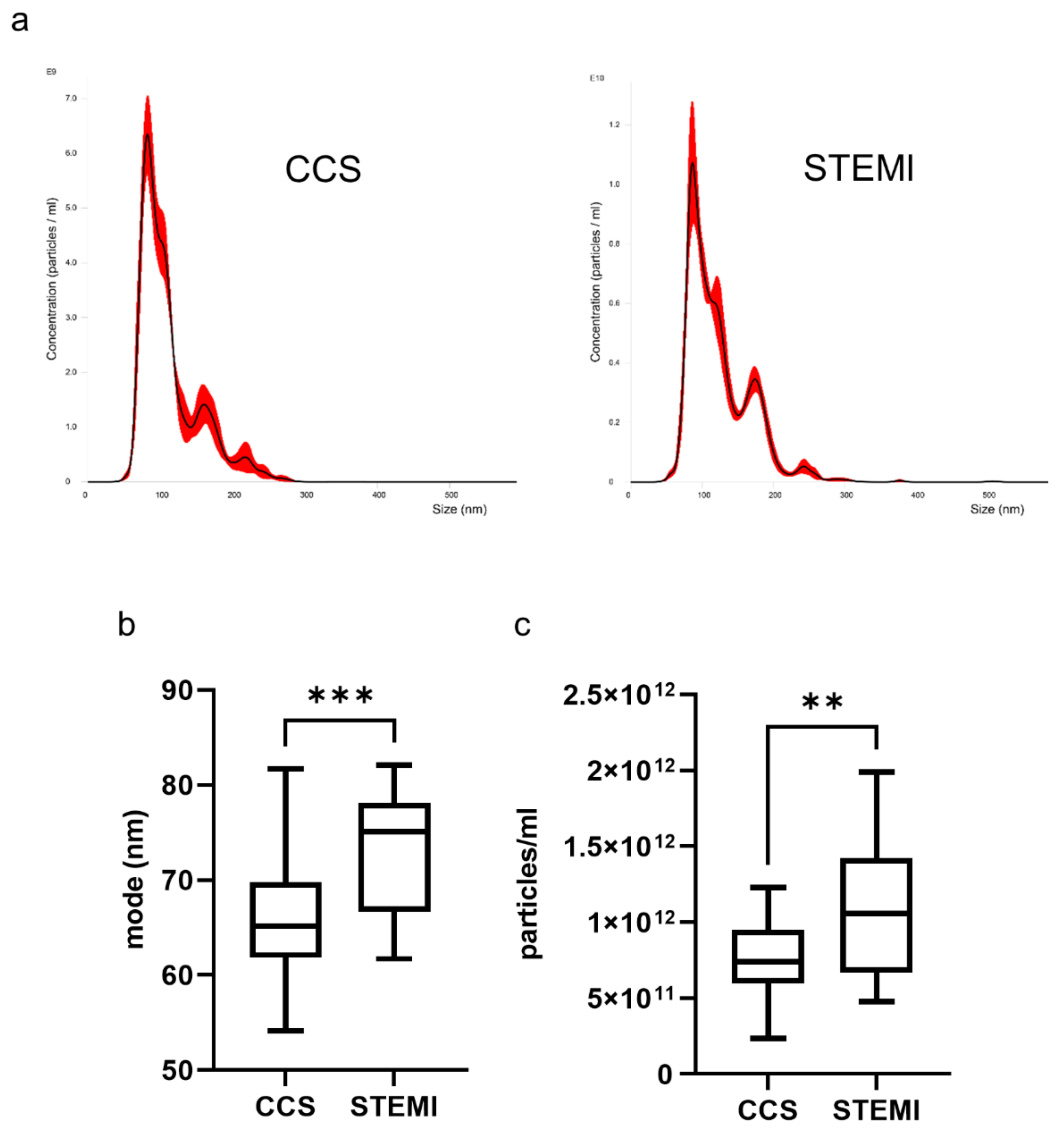
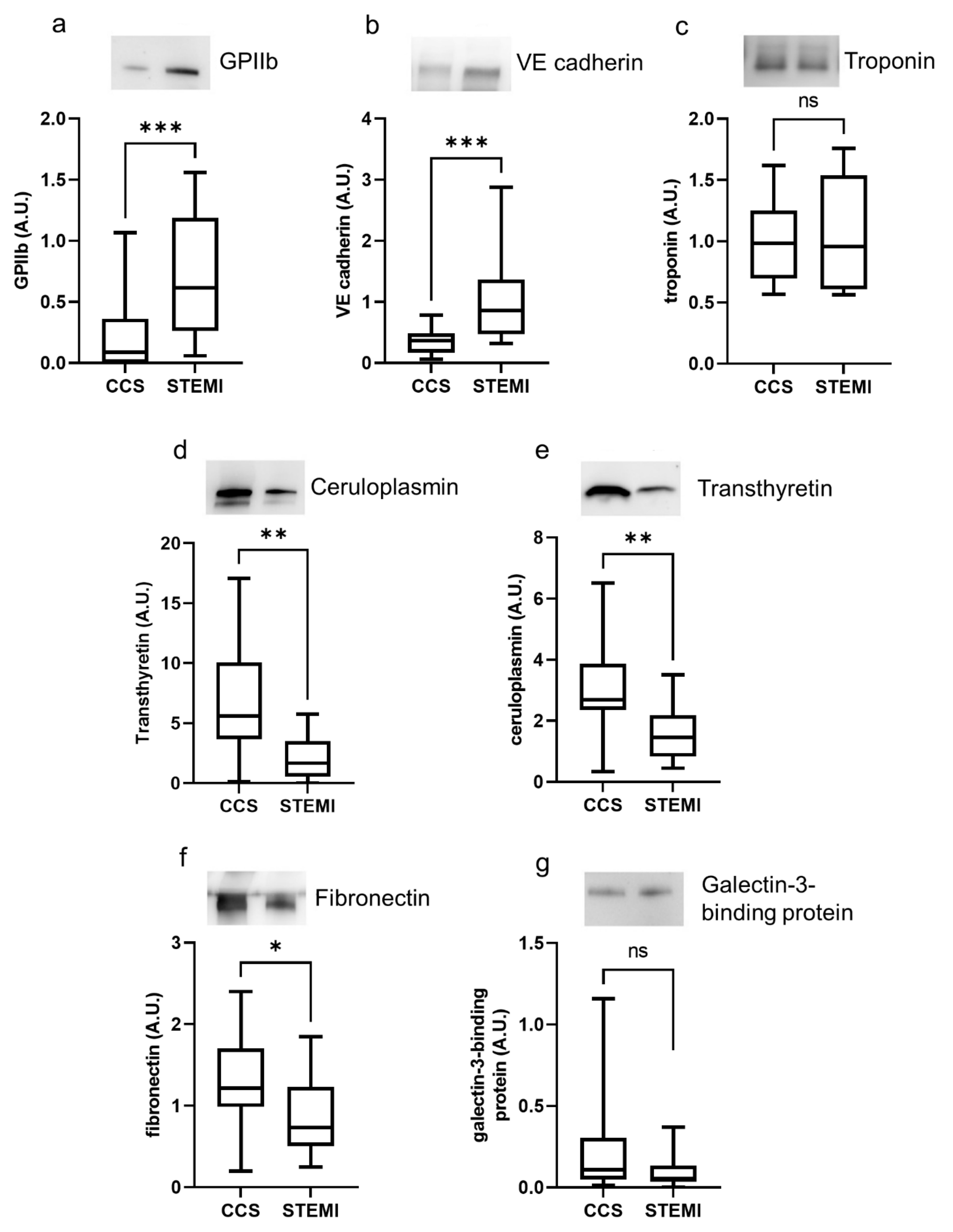
2.2. Exosome Characterization in Uncomplicated STEMI Versus CCS
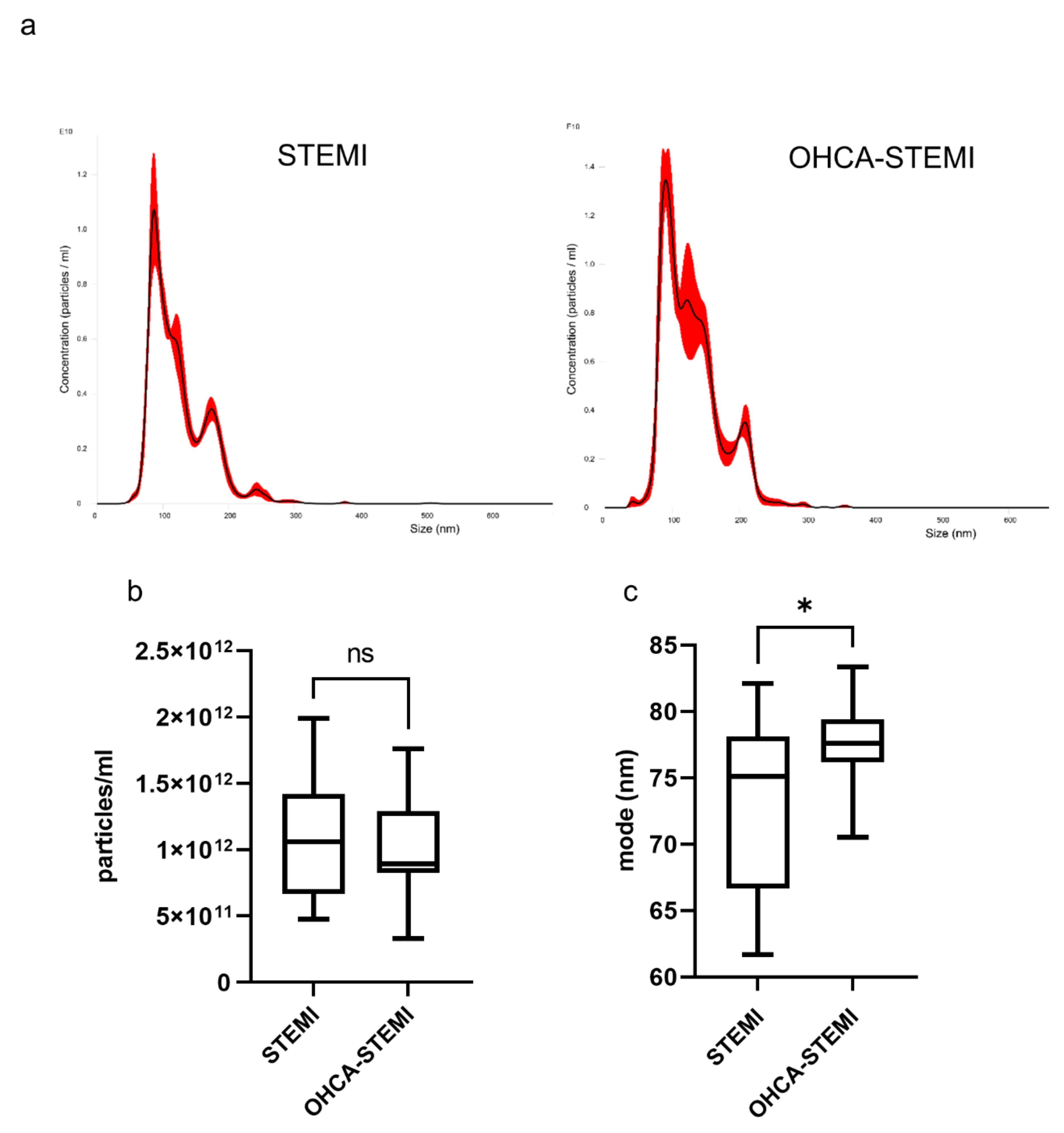
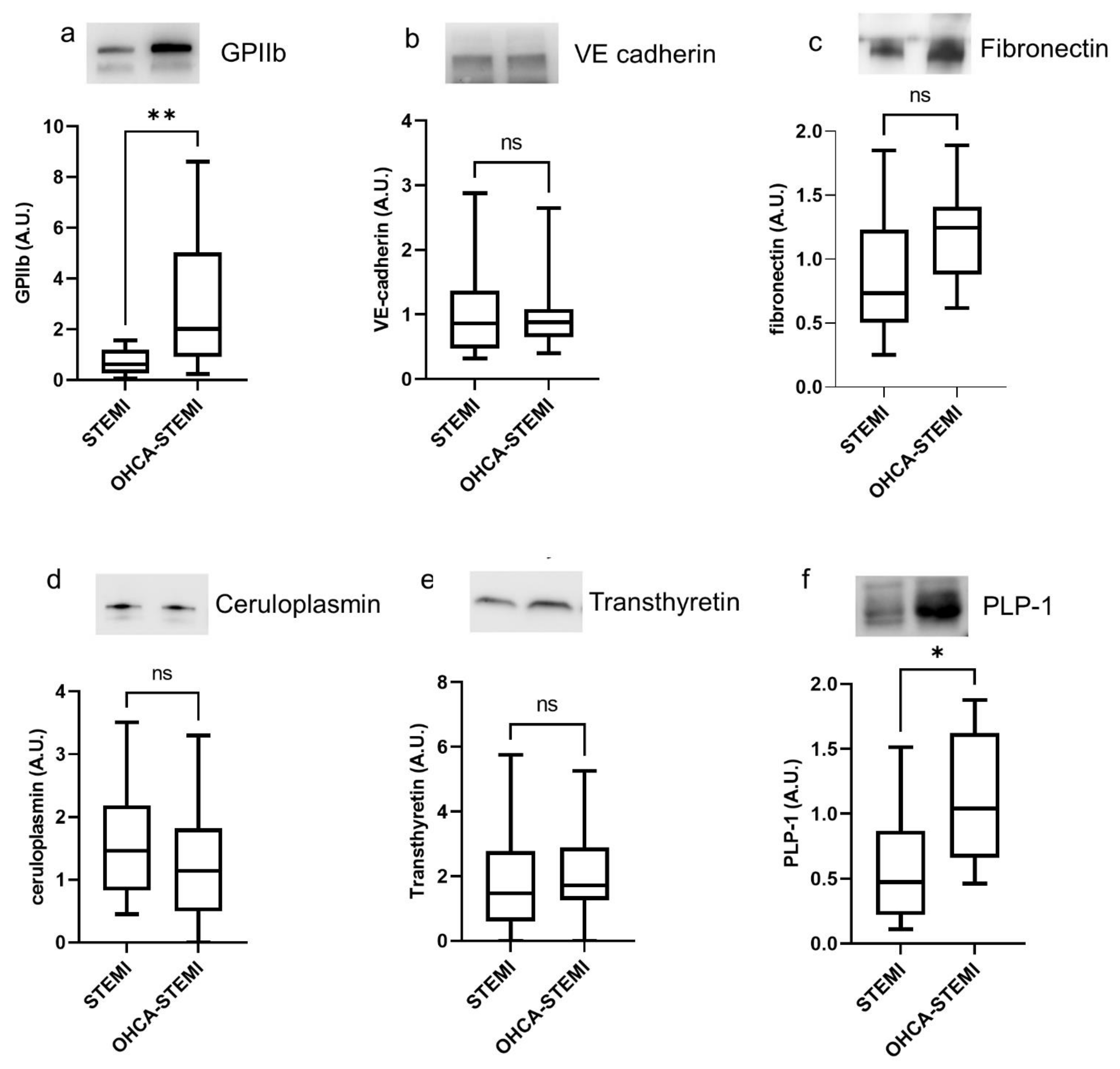
2.3. Exosome Characterization in Uncomplicated STEMI versus OHCA-STEMI
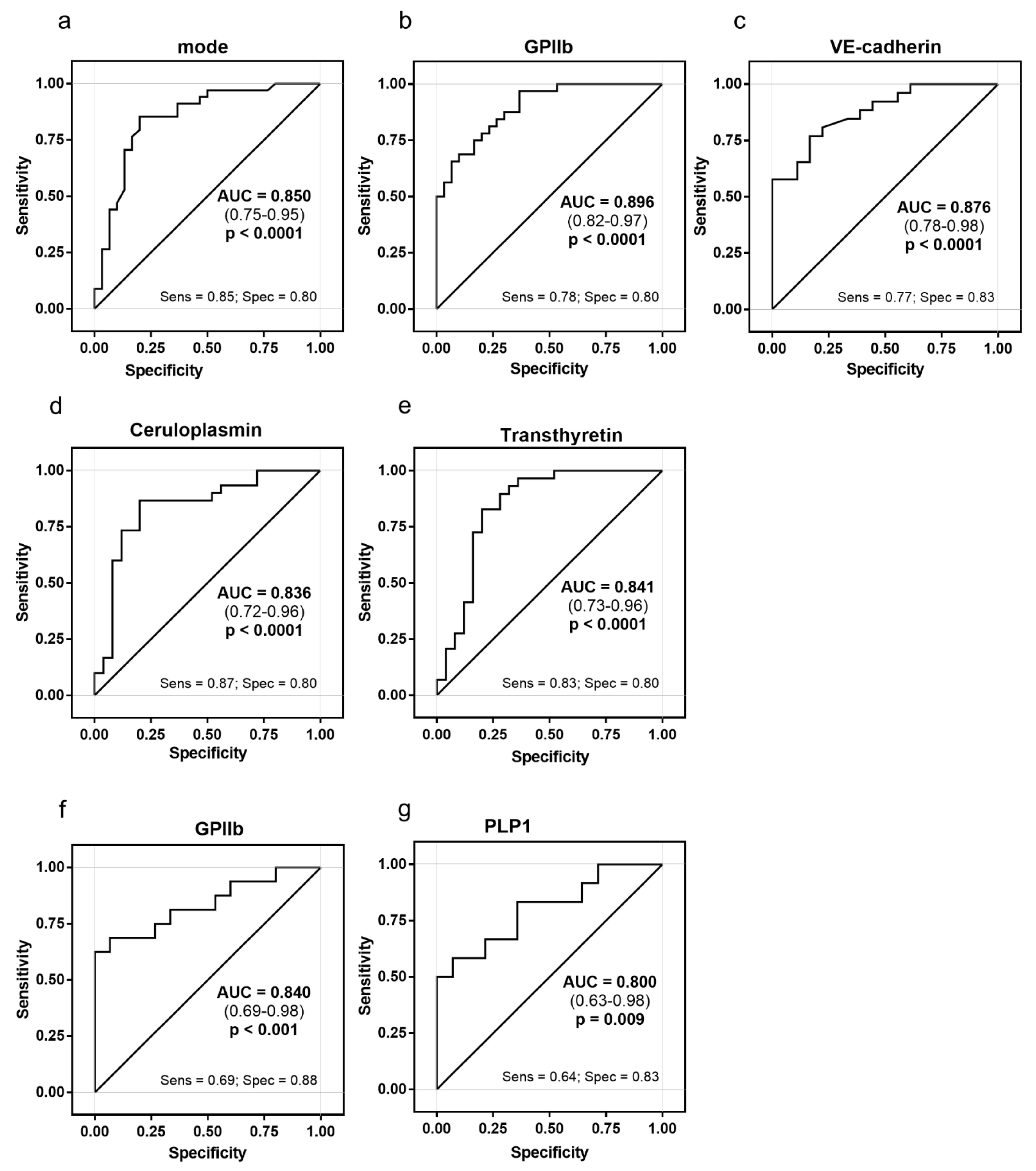
2.4. Exosome Ability to Discriminate between STEMI and CCS
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Study Protocol
4.3. Human Plasma Collection and Exosome Isolation
4.4. Nanoparticle Tracking Analysis (NTA)
4.5. Western Blot Analysis
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef] [Green Version]
- De Maria, G.L.; Garcia-Garcia, H.M.; Scarsini, R.; Finn, A.; Sato, Y.; Virmani, R.; Bhindi, R.; Ciofani, J.L.; Nuche, J.; Ribeiro, H.B.; et al. Novel device-based therapies to improve outcome in ST-segment elevation myocardial infarction. Eur. Heart J. Acute Cardiovasc. Care 2021, zuab012. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, F.; Butrymovich, V.; Kelbæk, H.; Wachtell, K.; Helqvist, S.; Kastrup, J.; Holmvang, L.; Clemmensen, P.; Engstrøm, T.; Grande, P.; et al. Short- and Long-Term Cause of Death in Patients Treated With Primary PCI for STEMI. J. Am. Coll. Cardiol. 2014, 64, 2101–2108. [Google Scholar] [CrossRef] [PubMed]
- Kalluri, R.; LeBleu, V.S. The biology function and biomedical applications of exosomes. Science 2020, 367, eaau6977. [Google Scholar] [CrossRef]
- Zarà, M.; Amadio, P.; Campodonico, J.; Sandrini, L.; Barbieri, S.S. Exosomes in Cardiovascular Diseases. Diagnostics 2020, 10, 943. [Google Scholar] [CrossRef] [PubMed]
- Moreira-Costa, L.; Barros, A.S.; Lourenço, A.P.; Leite-Moreira, A.F.; Nogueira-Ferreira, R.; Thongboonkerd, V.; Vitorino, R. Exosome-Derived Mediators as Potential Biomarkers for Cardiovascular Diseases: A Network Approach. Proteomes 2021, 9, 8. [Google Scholar] [CrossRef] [PubMed]
- Raposo, G.; Stoorvogel, W. Extracellular vesicles: Exosomes, microvesicles, and friends. J. Cell Biol. 2013, 200, 373–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guay, C.; Regazzi, R. Exosomes as new players in metabolic organ cross-talk. Diabetes Obes. Metab. 2017, 19, 137–146. [Google Scholar] [CrossRef]
- Carrozzo, A.; Casieri, V.; Di Silvestre, D.; Brambilla, F.; De Nitto, E.; Sardaro, N.; Papini, G.; Storti, S.; Settanni, G.; Solinas, M.; et al. Plasma exosomes characterization reveals a perioperative protein signature in older patients undergoing different types of on-pump cardiac surgery. Geroscience 2021, 43, 773–789. [Google Scholar] [CrossRef]
- King, H.W.; Michael, M.Z.; Gleadle, J.M. Hypoxic enhancement of exosome release by breast cancer cells. BMC Cancer 2012, 12, 421. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.; Deep, G. Hypoxia in tumor microenvironment regulates exosome biogenesis: Molecular mechanisms and translational opportunities. Cancer Lett. 2020, 479, 23–30. [Google Scholar] [CrossRef]
- Currim, F.; Singh, J.; Shinde, A.; Gohel, D.; Roy, M.; Singh, K.; Shukla, S.; Mane, M.; Vasiyani, H.; Singh, R. Exosome Release Is Modulated by the Mitochondrial-Lysosomal Crosstalk in Parkinson’s Disease Stress Conditions. Mol. Neurobiol. 2021, 58, 1819–1833. [Google Scholar] [CrossRef]
- Zhang, Z.G.; Chopp, M. Exosomes in stroke pathogenesis and therapy. J. Clin. Investig. 2016, 126, 1190–1197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, L.; Mei, S.; Zhang, S.; Qin, Q.; Li, H.; Liao, Y.; Fan, H.; Liu, Z.; Zhu, H. Cardio-renal Exosomes in Myocardial Infarction Serum Regulate Proangiogenic Paracrine Signaling in Adipose Mesenchymal Stem Cells. Theranostics 2020, 10, 1060–1073. [Google Scholar] [CrossRef] [PubMed]
- He, C.; Zheng, S.; Luo, Y.; Wang, B. Exosome Theranostics: Biology and Translational Medicine. Theranostics 2018, 8, 237–255. [Google Scholar] [CrossRef] [PubMed]
- Emanueli, C.; Shearn, A.I.U.; Angelini, G.D.; Sahoo, S. Exosomes and exosomal miRNAs in cardiovascular protection and repair. Vasc. Pharm. 2015, 71, 24–30. [Google Scholar] [CrossRef] [Green Version]
- Henning, R.J. Cardiovascular Exosomes and MicroRNAs in Cardiovascular Physiology and Pathophysiology. J. Cardiovasc. Transl. Res. 2021, 14, 195–212. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Martin, P.; Fogarty, B.; Brown, A.; Schurman, K.; Phipps, R.; Yin, V.P.; Lockman, P.; Bai, S. Exosome delivered anticancer drugs across the blood-brain barrier for brain cancer therapy in Danio rerio. Pharm. Res. 2015, 32, 2003–2014. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.C.; Liu, L.; Ma, F.; Wong, C.W.; Guo, X.E.; Chacko, J.V.; Farhoodi, H.P.; Zhang, S.X.; Zimak, J.; Ségaliny, A.; et al. Elucidation of Exosome Migration across the Blood-Brain Barrier Model In Vitro. Cell Mol. Bioeng. 2016, 9, 509–529. [Google Scholar] [CrossRef]
- Banks, W.A.; Sharma, P.; Bullock, K.M.; Hansen, K.M.; Ludwig, N.; Whiteside, T.L. Transport of Extracellular Vesicles across the Blood-Brain Barrier: Brain Pharmacokinetics and Effects of Inflammation. Int. J. Mol. Sci. 2020, 21, 4407. [Google Scholar] [CrossRef]
- Looze, C.; Yui, D.; Leung, L.; Ingham, M.; Kaler, M.; Yao, X.; Wu, W.W.; Shen, R.-F.; Daniels, M.P.; Levine, S.J. Proteomic profiling of human plasma exosomes identifies PPARgamma as an exosome-associated protein. Biochem. Biophys. Res. Commun. 2009, 378, 433–438. [Google Scholar] [CrossRef] [Green Version]
- Reunanen, A.; Knekt, P.; Aaran, R.-K. Serum Ceruloplasmin Level and the Risk of Myocardial Infarction and Stroke. Am. J. Epidemiol. 1992, 136, 1082–1090. [Google Scholar] [CrossRef]
- Fox, P.L.; Mazumder, B.; Ehrenwald, E.; Mukhopadhyay, C.K. Ceruloplasmin and cardiovascular disease. Free. Radic. Biol. Med. 2000, 28, 1735–1744. [Google Scholar] [CrossRef]
- Gleissner, C.A.; Erbel, C.; Linden, F.; Domschke, G.; Akhavanpoor, M.; Helmes, C.M.; Doesch, A.O.; Kleber, M.E.; Katus, H.A.; Maerz, W. Galectin-3 binding protein, coronary artery disease and cardiovascular mortality: Insights from the LURIC study. Atherosclerosis 2017, 260, 121–129. [Google Scholar] [CrossRef]
- Song, K.S.; Kim, H.K.; Shim, W.; Jee, S.H. Plasma fibronectin levels in ischemic heart disease. Atherosclerosis 2001, 154, 449–453. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhou, X.; Krepinsky, J.C.; Wang, C.; Segbo, J.; Zheng, F. Association study between fibronectin and coronary heart disease. Clin. Chem. Lab. Med. (CCLM) 2006, 44, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Valiente-Alandi, I.; Potter Sarah, J.; Salvador Ane, M.; Schafer Allison, E.; Schips, T.; Carrillo-Salinas, F.; Gibson Aaron, M.; Nieman Michelle, L.; Perkins, C.; Sargent Michelle, A.; et al. Inhibiting Fibronectin Attenuates Fibrosis and Improves Cardiac Function in a Model of Heart Failure. Circulation 2018, 138, 1236–1252. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Gautam, V.; Naseem, S. Acute-phase proteins: As diagnostic tool. J. Pharm. Bioallied Sci. 2011, 3, 118–127. [Google Scholar] [CrossRef]
- Gruys, E.; Toussaint, M.J.M.; Niewold, T.A.; Koopmans, S.J. Acute phase reaction and acute phase proteins. J. Zhejiang Univ. Sci. B 2005, 6, 1045–1056. [Google Scholar] [CrossRef] [Green Version]
- Hessvik, N.P.; Llorente, A. Current knowledge on exosome biogenesis and release. Cell Mol. Life Sci. 2018, 75, 193–208. [Google Scholar] [CrossRef] [Green Version]
- Zhao, C.; Wang, H.; Xiong, C.; Liu, Y. Hypoxic glioblastoma release exosomal VEGF-A induce the permeability of blood-brain barrier. Biochem. Biophys. Res. Commun. 2018, 502, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Gidlöf, O.; Evander, M.; Rezeli, M.; Marko-Varga, G.; Laurell, T.; Erlinge, D. Proteomic profiling of extracellular vesicles reveals additional diagnostic biomarkers for myocardial infarction compared to plasma alone. Sci. Rep. 2019, 9, 8991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrachina, M.N.; Calderón-Cruz, B.; Fernandez-Rocca, L.; García, Á. Application of Extracellular Vesicles Proteomics to Cardiovascular Disease: Guidelines, Data Analysis, and Future Perspectives. Proteomics 2019, 19, 1800247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deftu, A.T.; Radu, B.M.; Cretoiu, D.; Deftu, A.F.; Cretoiu, S.M.; Xiao, J. Exosomes as intercellular communication messengers for cardiovascular and cerebrovascular diseases. In Exosomes; Edelstein, L., Smythies, J., Quesenberry, P., Noble, D., Eds.; Academic Press: Cambridge, MA, USA, 2020; Chapter 9; pp. 199–238. [Google Scholar] [CrossRef]
- Gawaz, M. Role of platelets in coronary thrombosis and reperfusion of ischemic myocardium. Cardiovasc. Res. 2004, 61, 498–511. [Google Scholar] [CrossRef] [PubMed]
- Falque, H.; Bochaton, T.; Bernelin, H.; Paccalet, A.; Da Silva, C.C.; Baetz, D.; Bonnefoy-Cudraz, E.; Mewton, N.; Ovize, M. Endothelial activation and infarct size at the acute phase of myocardial infarction. Arch. Cardiovasc. Dis. Suppl. 2018, 10, 178. [Google Scholar] [CrossRef]
- Frossard, M.; Fuchs, I.; Leitner, J.M.; Hsieh, K.; Vlcek, M.; Losert, H.; Domanovits, H.; Schreiber, W.; Laggner, A.N.; Jilma, B. Platelet Function Predicts Myocardial Damage in Patients With Acute Myocardial Infarction. Circulation 2004, 110, 1392–1397. [Google Scholar] [CrossRef] [Green Version]
- Moccetti, F.; Brown, E.; Xie, A.; Packwood, W.; Qi, Y.; Ruggeri, Z.; Shentu, W.; Chen, J.; López, J.A.; Lindner, J.R. Myocardial Infarction Produces Sustained Proinflammatory Endothelial Activation in Remote Arteries. J. Am. Coll. Cardiol. 2018, 72, 1015–1026. [Google Scholar] [CrossRef]
- Greve, A.M.; Christoffersen, M.; Frikke-Schmidt, R.; Nordestgaard, B.G.; Tybjærg-Hansen, A. Association of Low Plasma Transthyretin Concentration With Risk of Heart Failure in the General Population. JAMA Cardiol. 2021, 6, 258–266. [Google Scholar] [CrossRef]
- Kharb, R.; Sharma, A.; Chaddar, M.K.; Yadav, R.; Agnihotri, P.; Kar, A.; Biswas, S. Plasma Proteome Profiling of Coronary Artery Disease Patients: Downregulation of Transthyretin—An Important Event. Mediat. Inflamm. 2020, 2020, 3429541. [Google Scholar] [CrossRef]
- Singh, T.K. Serum ceruloplasmin in acute myocardial infarction. Acta Cardiol. 1992, 47, 321–329. [Google Scholar]
- Brunetti, N.D.; Pellegrino, P.L.; Correale, M.; De Gennaro, L.; Cuculo, A.; Di Biase, M. Acute phase proteins and systolic dysfunction in subjects with acute myocardial infarction. J. Thromb. Thrombolysis 2008, 26, 196–202. [Google Scholar] [CrossRef]
- Gabay, C.; Kushner, I. Acute-Phase Proteins and Other Systemic Responses to Inflammation. N. Engl. J. Med. 1999, 340, 448–454. [Google Scholar] [CrossRef]
- Gitlin, J.D. Transcriptional regulation of ceruloplasmin gene expression during inflammation. J. Biol. Chem. 1988, 263, 6281–6287. [Google Scholar] [CrossRef]
- Myron Johnson, A.; Merlini, G.; Sheldon, J.; Ichihara, K. Clinical indications for plasma protein assays: Transthyretin (prealbumin) in inflammation and malnutrition. International Federation of Clinical Chemistry and Laboratory Medicine (IFCC): IFCC Scientific Division Committee on Plasma Proteins (C-PP). Clin. Chem. Lab. Med. 2007, 45, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Karam, N.; Bataille, S.; Marijon, E.; Tafflet, M.; Benamer, H.; Caussin, C.; Garot, P.; Juliard, J.-M.; Pires, V.; Boche, T.; et al. Incidence, Mortality, and Outcome-Predictors of Sudden Cardiac Arrest Complicating Myocardial Infarction Prior to Hospital Admission. Circ. Cardiovasc. Interv. 2019, 12, e007081. [Google Scholar] [CrossRef]
- Negovsky, V.A. Postresuscitation disease. Crit. Care Med. 1988, 16, 942–946. [Google Scholar] [CrossRef]
- Ji, Q.; Ji, Y.; Peng, J.; Zhou, X.; Chen, X.; Zhao, H.; Xu, T.; Chen, L.; Xu, Y. Increased Brain-Specific MiR-9 and MiR-124 in the Serum Exosomes of Acute Ischemic Stroke Patients. PLoS ONE 2016, 11, e0163645. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Song, Y.; Huang, J.; Qu, M.; Zhang, Y.; Geng, J.; Zhang, Z.; Liu, J.; Yang, G.-Y. Increased Circulating Exosomal miRNA-223 Is Associated with Acute Ischemic Stroke. Front. Neurol. 2017, 8, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, D.-B.; Liu, J.-L.; Wang, W.; Li, R.-Y.; Yu, D.-J.; Lan, X.-Y.; Li, J.-P. Plasma Exosomal miR-422a and miR-125b-2-3p Serve as Biomarkers for Ischemic Stroke. Curr. Neurovascular Res. 2017, 14, 330–337. [Google Scholar] [CrossRef]
- Wang, W.; Li, D.B.; Li, R.Y.; Zhou, X.; Yu, D.J.; Lan, X.Y.; Li, J.P.; Liu, J.L. Diagnosis of Hyperacute and Acute Ischaemic Stroke: The Potential Utility of Exosomal MicroRNA-21-5p and MicroRNA-30a-5p. Cerebrovasc. Dis. 2018, 45, 204–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kucharzewska, P.; Christianson, H.C.; Welch, J.E.; Svensson, K.J.; Fredlund, E.; Ringnér, M.; Mörgelin, M.; Bourseau-Guilmain, E.; Bengzon, J.; Belting, M. Exosomes reflect the hypoxic status of glioma cells and mediate hypoxia-dependent activation of vascular cells during tumor development. Proc. Natl. Acad. Sci. USA 2013, 110, 7312–7317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krämer-Albers, E.-M.; Bretz, N.; Tenzer, S.; Winterstein, C.; Möbius, W.; Berger, H.; Nave, K.-A.; Schild, H.; Trotter, J. Oligodendrocytes secrete exosomes containing major myelin and stress-protective proteins: Trophic support for axons? Proteom. Clin. Appl. 2007, 1, 1446–1461. [Google Scholar] [CrossRef]
- Frühbeis, C.; Fröhlich, D.; Kuo, W.P.; Amphornrat, J.; Thilemann, S.; Saab, A.S.; Kirchhoff, F.; Möbius, W.; Goebbels, S.; Nave, K.-A.; et al. Neurotransmitter-triggered transfer of exosomes mediates oligodendrocyte-neuron communication. PLoS Biol. 2013, 11, e1001604. [Google Scholar] [CrossRef] [Green Version]
- Fröhlich, D.; Kuo, W.P.; Frühbeis, C.; Sun, J.-J.; Zehendner, C.M.; Luhmann, H.J.; Pinto, S.; Toedling, J.; Trotter, J.; Krämer-Albers, E.-M. Multifaceted effects of oligodendroglial exosomes on neurons: Impact on neuronal firing rate, signal transduction and gene regulation. Philos. Trans. R. Soc. Lond. Ser. B Biol. Sci. 2014, 369, 20130510. [Google Scholar] [CrossRef] [PubMed]
- Kaur, C.; Ling, E.A. Blood Brain Barrier in Hypoxic-Ischemic Conditions. Curr. Neurovascular Res. 2008, 5, 71–81. [Google Scholar] [CrossRef]
- Dougherty, J.H.; Levy, D.E.; Weksler, B.B. Experimental cerebral ischemia produces platelet aggregates. Neurology 1979, 29, 1460–1465. [Google Scholar] [CrossRef] [PubMed]
- Zeller, J.A.; Tschoepe, D.; Kessler, C. Circulating Platelets Show Increased Activation in Patients with Acute Cerebral Ischemia. Thromb. Haemost. 1999, 81, 373–377. [Google Scholar] [PubMed]
- Weidman, J.L.; Shook, D.C.; Hilberath, J.N. Cardiac Resuscitation and Coagulation. Anesthesiology 2014, 120, 1009–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spiel, A.O.; Frossard, M.; Mayr, F.B.; Kliegel, A.; Janata, A.; Uray, T.; Wandaller, C.; Sterz, F.; Jilma, B. Pronounced platelet hyperfunction in patients with cardiac arrest achieving restoration of spontaneous circulation. Crit. Care Med. 2009, 37, 975–979. [Google Scholar] [CrossRef] [PubMed]
- Théry, C.; Witwer, K.W.; Aikawa, E.; Alcaraz, M.J.; Anderson, J.D.; Andriantsitohaina, R.; Antoniou, A.; Arab, T.; Archer, F.; Atkin-Smith, G.K.; et al. Minimal information for studies of extracellular vesicles 2018 (MISEV2018): A position statement of the International Society for Extracellular Vesicles and update of the MISEV2014 guidelines. J. Extracell. Vesicles 2018, 7, 1535750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torti, M.; Manganaro, D.; Visconte, C.; Zarà, M.; Canino, J.; Vismara, M.; Canobbio, I.; Guidetti, G.F. Stimulation of mTORC2 by integrin αIIbβ3 is required for PI3Kβ-dependent activation of Akt but is dispensable for platelet spreading on fibrinogen. Platelets 2020, 31, 521–529. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | CCS (n = 32) | STEMI (n = 18) | OHCA-STEMI (n = 17) | P-ANOVA | * p Value CCS vs. STEMI | * p Value STEMI vs. OHCA-STEMI |
|---|---|---|---|---|---|---|
| Demographic and clinical characteristics | ||||||
| Age, years | 64.1 ± 8.1 | 67.2 ± 10.8 | 58.5 ± 10.5 | 0.03 | 0.42 | 0.02 |
| BMI, Kg/m2 | 26.0 ± 3.0 | 26.5 ± 3.3 | 27.1 ± 4.4 | 0.71 | 0.70 | 1.00 |
| RBC, 106/μL | 4.8 ± 0.4 | 4.0 ± 0.9 | 4.5 ± 0.8 | 0.0003 | 0.0001 | 0.03 |
| WBC, 103/μL | 7.7 ± 1.9 | 11.6 ± 1.9 | 13.0 ± 4.1 | <0.0001 | <0.0001 | 0.37 |
| PLT, 103/μL | 236.6 ± 44.3 | 242.4 ± 53.7 | 247.1 ± 61.3 | 0.053 | 0.08 | 1.00 |
| Hemoglobin (g/dL) | 14.6 ± 1.2 | 13.3 ± 2.0 | 14.2 ± 1.8 | 0.01 | 0.007 | 0.08 |
| Total cholesterol, mg/dL | 159.9 ± 30.4 | 172.4 ± 42.9 | 171.4 ± 43.2 | 0.32 | 0.22 | 0.55 |
| HDL cholesterol, mg/dL | 46.4 ± 10.4 | 41.5 ± 8.8 | 39.7 ± 9.4 | 0.10 | 0.12 | 1.00 |
| LDL cholesterol, mg/dL | 90.4 ± 28.6 | 106.1 ± 39.2 | 113.7 ± 31.9 | 0.08 | 0.09 | 0.98 |
| Triglycerides, mmol/L | 71.0 ± 63.4 | 128.8 ± 60.6 | 136.6 ± 72.8 | 0.29 | 0.26 | 0.96 |
| Glycemia, mg/dL | 109.4 ± 15.6 | 181.9 ± 102.3 | 206.8 ± 122.5 | <0.0001 | 0.001 | 0.30 |
| Creatinine, mg/dL | 1.5 ± 0.2 | 1.1 ± 0.3 | 1.1 ± 0.3 | 0.18 | 0.99 | 0.18 |
| CRP, mg/L | 0.7 (0.5–2.3) | 2.8 (1.7–3.8) | 2.2 (0.9;4.4) | 0.04 | 0.03 | 0.59 |
| hs Tnl max, μg/L | / | 16.3 (12.9–99.6) | 80.3 (35.6–1742.7) | 0.26 | / | 0.26 |
| Time-to-Pres (h) | / | 3.36 ± 2.2 | 5.24 ± 7.38 | 0.33 | / | 0.33 |
| anterior AMI, n (%) | / | 10 (55.6%) | 10 (58.8%) | 0.78 | / | 0.78 |
| Smokers, n (%) | 6 (71.9%) | 7 (38.9%) | 6 (35.3%) | 0.84 | 0.98 | 0.79 |
| Diabetes, n (%) | 6 (19.4%) | 6 (33.3%) | 5 (29.4%) | 0.54 | 0.51 | 0.99 |
| Hypertension, n (%) | 23 (71.9%) | 12 (66.7%) | 9 (52.9%) | 0.66 | 0.66 | 1.00 |
| Familiarity, n (%) | 4 (22.2%) | 4 (22.2%) | 2 (11.8%) | 0.01 | 0.11 | 0.43 |
| Dyslipidemia, n (%) | 20 (62.5%) | 9 (50%) | 5 (29.4%) | 0.15 | 0.49 | 0.62 |
| Pharmacological treatments | ||||||
| ACE inhibitors, n (%) | 21 (67.7%) | 5 (27.8%) | 8 (47.1%) | 0.02 | 0.008 | 0.20 |
| Statin, n (%) | 23 (74.2%) | 2 (11.1%) | 3 (17.6%) | <0.0001 | <0.0001 | 0.74 |
| β-blockers, n (%) | 19 (61.3%) | 4 (22.2%) | 4 (23.5%) | 0.006 | 0.007 | 0.83 |
| Ca channel blockers, n (%) | 5 (16.1%) | 1 (5.6%) | 1 (5.9%) | 0.39 | 0.46 | 0.99 |
| Hypoglycemics, n (%) | 4 (12.9%) | 5 (27.8%) | 2 (11.8%) | 0.44 | 0.36 | 0.49 |
| Thienopyridine, n (%) | 11 (35.5%) | 0 (0%) | 1 (5.9%) | 0.002 | 0.003 | 0.76 |
| Aspirin, n (%) | 27 (87.1%) | 3 (16.7%) | 3 (17.6%) | <0.0001 | <0.0001 | 0.78 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zarà, M.; Campodonico, J.; Cosentino, N.; Biondi, M.L.; Amadio, P.; Milanesi, G.; Assanelli, E.; Cerri, S.; Biggiogera, M.; Sandrini, L.; et al. Plasma Exosome Profile in ST-Elevation Myocardial Infarction Patients with and without Out-of-Hospital Cardiac Arrest. Int. J. Mol. Sci. 2021, 22, 8065. https://doi.org/10.3390/ijms22158065
Zarà M, Campodonico J, Cosentino N, Biondi ML, Amadio P, Milanesi G, Assanelli E, Cerri S, Biggiogera M, Sandrini L, et al. Plasma Exosome Profile in ST-Elevation Myocardial Infarction Patients with and without Out-of-Hospital Cardiac Arrest. International Journal of Molecular Sciences. 2021; 22(15):8065. https://doi.org/10.3390/ijms22158065
Chicago/Turabian StyleZarà, Marta, Jeness Campodonico, Nicola Cosentino, Maria Luisa Biondi, Patrizia Amadio, Gloria Milanesi, Emilio Assanelli, Silvia Cerri, Marco Biggiogera, Leonardo Sandrini, and et al. 2021. "Plasma Exosome Profile in ST-Elevation Myocardial Infarction Patients with and without Out-of-Hospital Cardiac Arrest" International Journal of Molecular Sciences 22, no. 15: 8065. https://doi.org/10.3390/ijms22158065