Predictive Model for Occlusal Vertical Dimension Determination and Digital Preservation with Three-Dimensional Facial Scanning

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
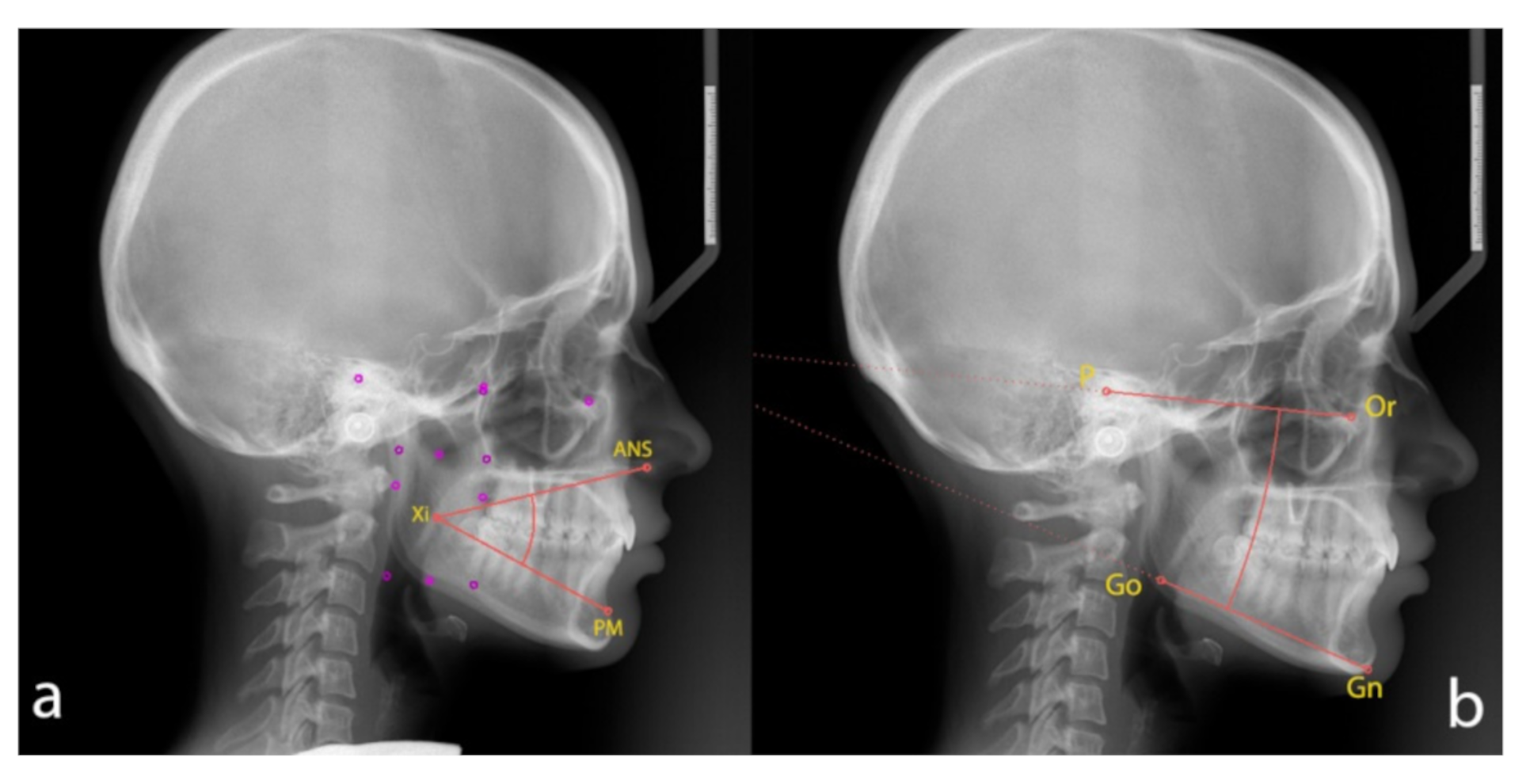
2.1. Cephalometric Analysis
- -
- The lower facial height angle [LFHˆ], between [ANS], [Xi] point and [PM];
- -
- The angle [MLˆFH], between mandibular plane (the plane tangent to the lower edge of the mandibular body, [Gn] and [Go]) and Frankfurt plane ([P] and [Or]).
2.2. Anthropometric Measurements
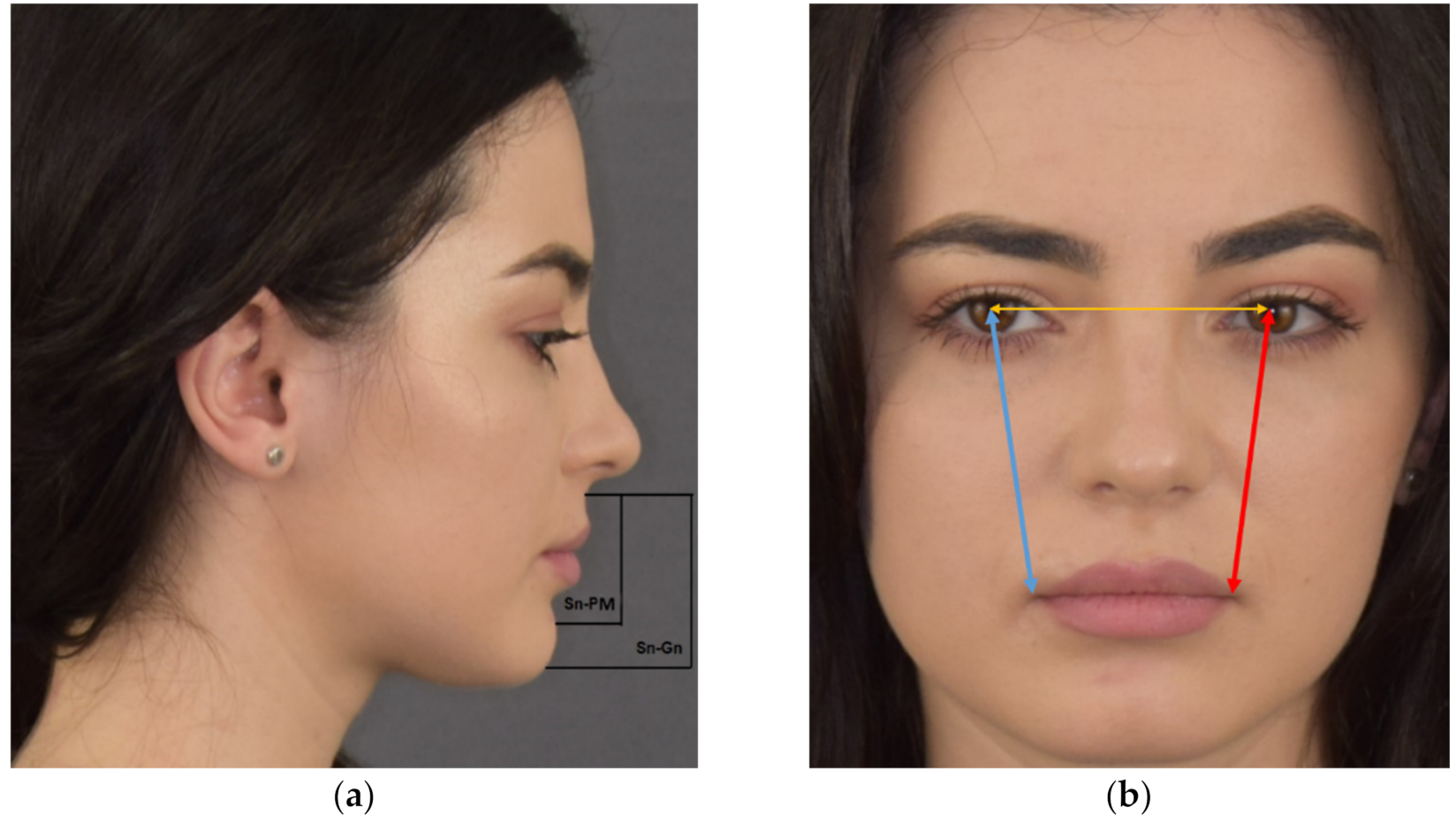
2.2.1. Clinical Anthropometric Measurements
- -
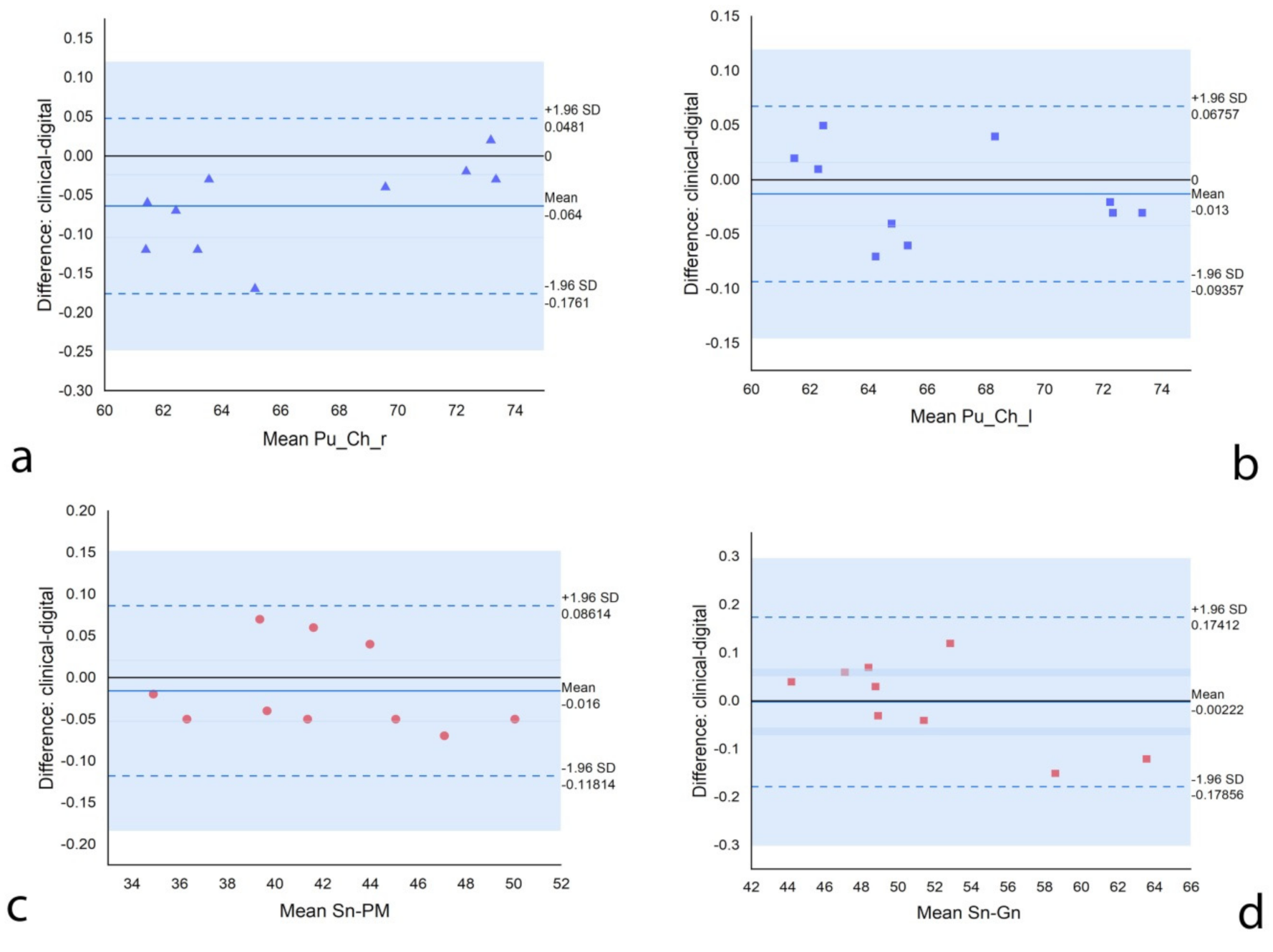
- Subnasion [Sn] and the point on the anterior edge of the symphysis that shows the profile’s change from concave to convex (Prementon [PM]) (Sn–PM);
- -
- Subnasion [Sn] - Gnathion [Gn] (Sn–Gn);
- -
- Right pupil [Pu] to right buccal commissure (chelion [Ch]) (Pu–Ch_r);
- -
- Left pupil to left buccal commissure (Pu–Ch_l).
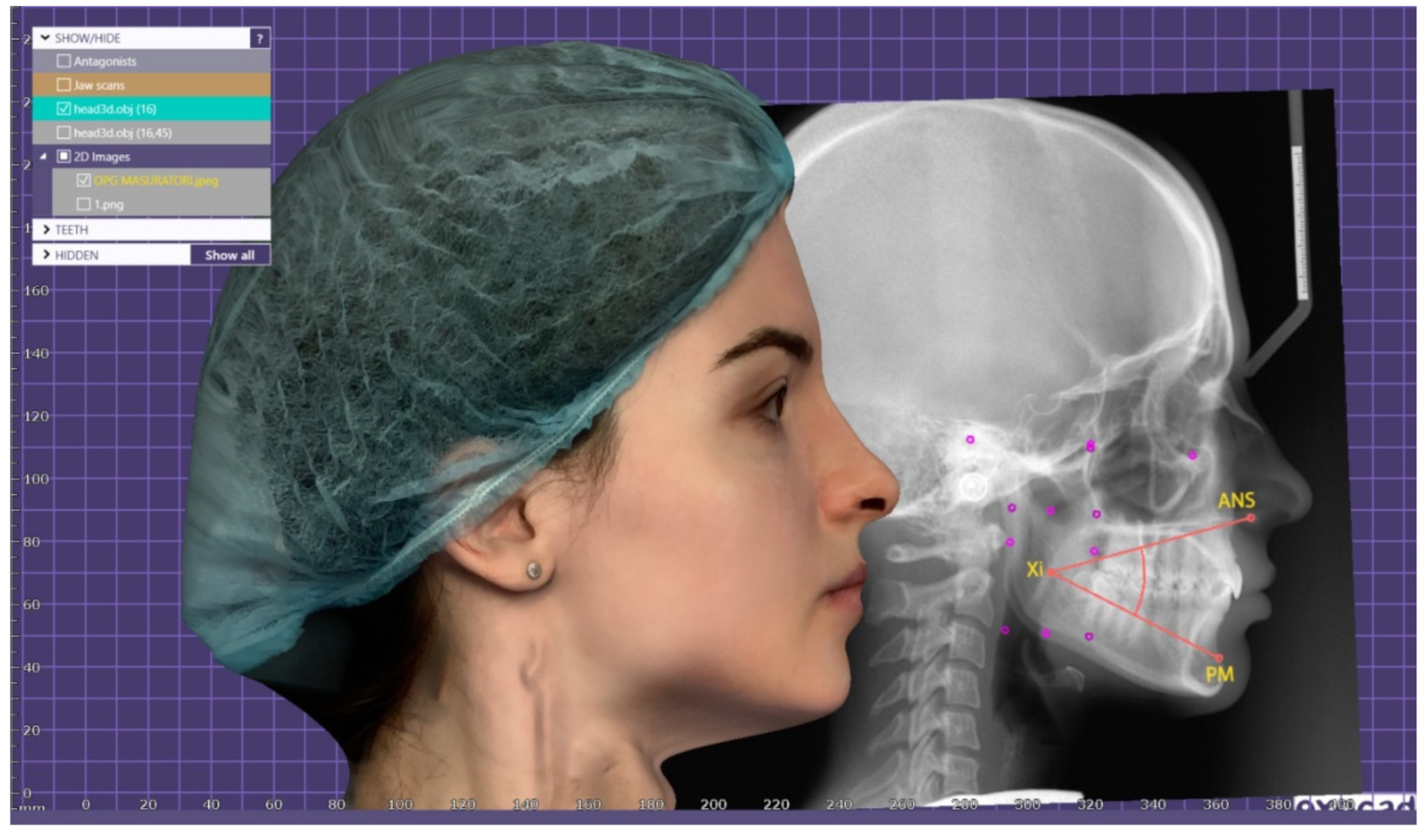
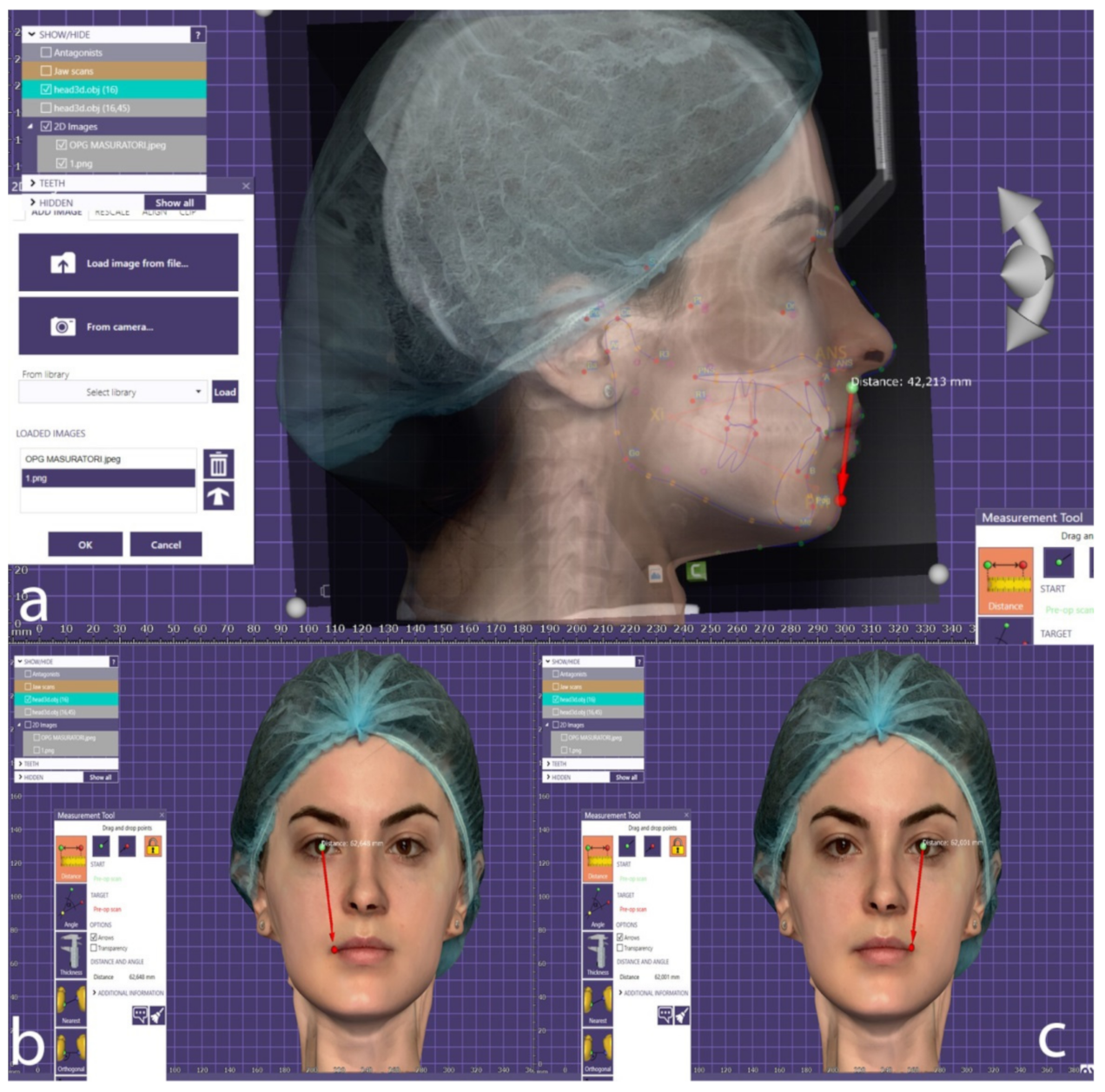
2.2.2. Anthropometric Measurements on Facial Scanning
2.3. Data Analysis
3. Results
3.1. Descriptive Analyses of the Standard Measurements
3.2. Baseline Data of the Participants
3.3. Correlations between Variable
3.4. Calculation of OVD Regression Formula
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Enkling, N.; Enkling-Scholl, J.; Albrecht, D.; Bornstein, M.M.; Schimmel, M. Determination of the occlusal vertical dimension in edentulous patients using lateral cephalograms. J. Oral Rehabil. 2018, 45, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Alhajj, M.N.; Daer, A.A. A proposed linear skeletal distance to predict occlusal vertical dimension: A cephalometric study. J. Prosthet. Dent. 2017, 118, 732–735. [Google Scholar] [CrossRef] [PubMed]
- Abduo, J.; Lyons, K. Clinical considerations for increasing occlusal vertical dimension: A review. Aust. Dent. J. 2012, 57, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Pintilie, I.I.; Cristache, C.-M. Alterations in the Temporomandibular Joints Morphology in Edentulous Patients—Clinical Consequences, Diagnostic Methods and Therapeutic Decisions; Conrad, J., Ed.; Nova Science Publishers: New York, NY, USA, 2020; ISBN 978-1-53617-441-0. [Google Scholar]
- Igic, M.; Krunic, N.; Aleksov, L.; Kostic, M.; Igic, A.; Petrovic, M.; Dacic, S.; Igic, S.; Igic, A. Determination of vertical dimension of occlusion by using the phonetic vowel “O” and “E”. Vojn. Pregl. Med. Pharm. J. Serbia 2015, 72, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Alhajj, M.N.; Khalifa, N.; Abduo, J.; Amran, A.G.; Ismail, I.A. Determination of occlusal vertical dimension for complete dentures patients: An updated review. J. Oral Rehabil. 2017, 44, 896–907. [Google Scholar] [CrossRef]
- Şakar, O. Re-establishing Occlusal Vertical Dimension and Maximal Intercuspal Position in Partially Edentulous Patients. In Removable Partial Dentures; Springer International Publishing: Cham, Switzerland, 2016. [Google Scholar]
- Bissasu, M. Pre-extraction records for complete denture fabrication: A literature review. J. Prosthet. Dent. 2004, 91, 55–58. [Google Scholar] [CrossRef]
- Tallgren, A. Changes in adult face height due to ageing, wear and loss of teeth and prosthetic treatment. Acta Odontol. Scand. 1957, 15, 1–122. [Google Scholar]
- Provost, W.A.; Towle, H.J. Determination of physiologic rest position by electronic measurement. J. Prosthet. Dent. 1972, 27, 377–380. [Google Scholar] [CrossRef]
- Shpuntoff, H. Determination of vertical dimension of rest: A comparative study. J. Prosthet. Dent. 1988, 59, 640. [Google Scholar] [CrossRef]
- Freitas de Souza, R.; Marra, J.; Carolina Pero, A.; Antonio Compagnoni, M. Effect of denture fabrication and wear on closest speaking space and interocclusal distance during deglutition. J. Prosthet. Dent. 2007, 97, 381–388. [Google Scholar] [CrossRef]
- Darling, D.W.; Kraus, S.; Glasheen-Wray, M.B. Relationship of head posture and the rest position of the mandible. J. Prosthet. Dent. 1984, 52, 111–115. [Google Scholar] [CrossRef]
- Pansch, J.L.; Callaghan, N.R.; Appleby, R.C. Effects of cast-gold mandibular dentures on the vertical dimension of rest position. J. Prosthet. Dent. 1972, 28, 21–25. [Google Scholar] [CrossRef]
- Woda, A.; Pionchon, P.; Palla, S. Regulation of mandibular postures: Mechanisms and clinical implications. Crit. Rev. Oral Biol. Med. 2001, 12, 166–178. [Google Scholar] [CrossRef]
- Hellsing, G. Functional adaptation to changes in vertical dimension. J. Prosthet. Dent. 1984, 52, 867–870. [Google Scholar] [CrossRef]
- Ballard, C.F. Mandibular posture. Dent. Pract. Dent. Rec. 1967, 17, 377. [Google Scholar]
- Rahn, A.O.; Ivanhoe, J.R.; Plummer, K.D. Textbook of Complete Dentures; PMPH-USA: Raleigh, NC, USA, 2009; ISBN 1607950251. [Google Scholar]
- Abdul-Rassol, M. Facial measurement method for determining occlusal vertical dimension. Al-Taqani 2007, 20, 13–17. [Google Scholar]
- Vinnakota, D.N.; Kanneganti, K.C.; Pulagam, M.; Keerthi, G.K. Determination of vertical dimension of occlusion using lateral profile photographs: A pilot study. J. Indian Prosthodont. Soc. 2016, 16, 323. [Google Scholar] [CrossRef]
- Şakar, O.; Sülün, T.; Kurt, H.; Gençel, B. Reliability and comparison of two facial measurements to detect changes of occlusal vertical dimension in complete denture wearers. Gerodontology 2011, 28, 205–208. [Google Scholar] [CrossRef]
- Alhajj, M.N.; Khalifa, N.; Amran, A. Eye-rima oris distance and its relation to the vertical dimension of occlusion measured by two methods: Anthropometric study in a sample of Yemeni dental students. Eur. J. Dent. 2016, 10, 29. [Google Scholar] [CrossRef]
- Akhma, N.E.; Sumarsongko, T.; Rikmasari, R. Correlation between the occlusal vertical dimension and the pupil rima oris distance among Sundanese population. Padjadjaran J. Dent. 2017, 29. [Google Scholar] [CrossRef] [Green Version]
- Nagpal, A.; Parkash, H.; Bhargava, A.; Chittaranjan, B. Reliability of different facial measurements for determination of vertical dimension of occlusion in edentulous using accepted facial dimensions recorded from dentulous subjects. J. Indian Prosthodont. Soc. 2014, 14, 233–242. [Google Scholar] [CrossRef] [PubMed]
- Muhammad Irfan, M.; Muhammad, A.M.K. Determination of occlusal vertical dimension in a section of Pakistani population using craniofacial measurements. J. Univ. Med. Dent. Coll. 2015, 6, 1–5. [Google Scholar]
- Basnet, B.B.; Parajuli, P.K.; Singh, R.K.; Suwal, P.; Shrestha, P.; Baral, D. An anthropometric study to evaluate the correlation between the occlusal vertical dimension and length of the thumb. Clin. Cosmet. Investig. Dent. 2015, 7, 33. [Google Scholar] [CrossRef] [Green Version]
- Ladda, R.; Bhandari, A.J.; Kasat, V.O.; Angadi, G.S. A new technique to determine vertical dimension of occlusion from anthropometric measurements of fingers. Indian J. Dent. Res. 2013, 24, 316. [Google Scholar] [CrossRef]
- Bhandari Aruna, J.; Ladda, R.; Bhandari Akshay, J. Correlation between vertical dimension of occlusion and length of little finger. Pravara Med. Rev. 2012, 4, 10–14. [Google Scholar]
- Ladda, R.; Kasat, V.O.; Bhandari, A.J. A new technique to determine vertical dimension of occlusion from anthropometric measurement of interpupillary distance. J. Clin. Exp. Dent. 2014, 6, e395. [Google Scholar] [CrossRef]
- Darvell, B.W.; Spratley, M.H. The inapplicability of formulae to determine vertical dimension. Aust. Dent. J. 1979, 24, 48–51. [Google Scholar] [CrossRef] [PubMed]
- Alhajj, M.N.; Musaad, N.J.; Ismail, I.A. Correlation between Finger Length and Occlusal Vertical Dimension in Adult Sudanese Women. Bull. Tokyo Dent. Coll. 2016, 57, 215–221. [Google Scholar] [CrossRef] [Green Version]
- Delić, Z.; Šimunović-Šoškić, M.; Perinić-Gržić, R.; Vukovojac, S.; Rajić, Z.; Kuna, T.; Kuna, T. Evaluation of craniometric methods for determination of vertical dimension of occlusion. Coll. Antropol. 2000, 24, 31–35. [Google Scholar]
- Delić, Z.; Vukovojac, S.; Gržić, R.; Maričić, D.; Kovač, Z.; Kovačević, D. Evaluation of craniometric methods for determination of vertical dimension of occlusion—Part 2. Coll. Antropol. 2003, 27, 191–194. [Google Scholar]
- Thompson, J.R. The rest position of the mandible and its significance to dental science. J. Am. Dent. Assoc. 1946. [Google Scholar] [CrossRef]
- Slavicek, R. Die Bedeutung der skelettalen Diagnose für den zahnlosen Patienten. In Schwerpunkte in der Totalprothetik; Quintessenz Verlags-GmbH: Berlin, Germany, 1986; pp. 73–98. [Google Scholar]
- Brzoza, D.; Barrera, N.; Contasti, G.; Hernández, A. Predicting vertical dimension with cephalograms, for edentulous patients. Gerodontology 2005, 22, 98–103. [Google Scholar] [CrossRef]
- Orthlieb, J.D.; Laurent, M.; Laplanche, O. Cephalometric estimation of Vertical Dimension of Occlusion. J. Oral Rehabil. 2000, 27, 802–807. [Google Scholar] [CrossRef]
- Pagano, S.; Moretti, M.; Marsili, R.; Ricci, A.; Barraco, G.; Cianetti, S. Evaluation of the accuracy of four digital methods by linear and volumetric analysis of dental impressions. Materials 2019, 12, 1958. [Google Scholar] [CrossRef] [Green Version]
- Revilla-León, M.; Raney, L.; Piedra-Cascón, W.; Barrington, J.; Zandinejad, A.; Özcan, M. Digital workflow for an esthetic rehabilitation using a facial and intraoral scanner and an additive manufactured silicone index: A dental technique. J. Prosthet. Dent. 2020, 123, 564–570. [Google Scholar] [CrossRef]
- Lo Russo, L.; Di Gioia, C.; Salamini, A.; Guida, L. Integrating intraoral, perioral, and facial scans into the design of digital dentures. J. Prosthet. Dent. 2020, 123, 584–588. [Google Scholar] [CrossRef] [PubMed]
- Dindaroǧlu, F.; Kutlu, P.; Duran, G.S.; Görgülü, S.; Aslan, E. Accuracy and reliability of 3D stereophotogrammetry: A comparison to direct anthropometry and 2D photogrammetry. Angle Orthod. 2016, 86, 487–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Bassetti, N. The Vertical Dimension in Prosthesis and Orthognathodontics: Integration between Function and Aesthetics; Smeraldi, C., Ed.; EDRA: Milano, Italy, 2016; ISBN 978-88-214-3959-9. [Google Scholar]
- Toma, A.M.; Zhurov, A.; Playle, R.; Ong, E.; Richmond, S. Reproducibility of facial soft tissue landmarks on 3D laser-scanned facial images. Orthod. Craniofacial Res. 2009, 12, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Granata, S.; Giberti, L.; Vigolo, P.; Stellini, E.; Di Fiore, A. Incorporating a facial scanner into the digital workflow: A dental technique. J. Prosthet. Dent. 2019, 123, 781–785. [Google Scholar] [CrossRef]
- Lavorgna, L.; Cervino, G.; Fiorillo, L.; Di Leo, G.; Troiano, G.; Ortensi, M.; Galantucci, L.; Cicciù, M. Reliability of a virtual prosthodontic project realized through a 2d and 3d photographic acquisition: An experimental study on the accuracy of different digital systems. Int. J. Environ. Res. Public Health 2019, 16, 5139. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.J.; Xiong, Y.X.; Wang, Y. Three-dimensional accuracy of facial scan for facial deformities in clinics: A new evaluation method for facial scanner accuracy. PLoS ONE 2017, 12, e0169402. [Google Scholar] [CrossRef] [PubMed]
- Valletta, R.; Pango, A.; Tortora, G.; Rongo, R.; Simeon, V.; Spagnuolo, G.; D’Antò, V. Association between gingival biotype and facial typology through cephalometric evaluation and three-dimensional facial scanning. Appl. Sci. 2019, 9, 5057. [Google Scholar] [CrossRef] [Green Version]
- You, Y.; Shen, Y.; Zhang, G.; Xing, X. Real-time and high-resolution 3D face measurement via a smart active optical sensor. Sensors 2017, 17, 734. [Google Scholar] [CrossRef] [Green Version]
- Amornvit, P.; Sanohkan, S. The accuracy of digital face scans obtained from 3D scanners: An in vitro study. Int. J. Environ. Res. Public Health 2019, 16, 5061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrario, V.F.; Sforza, C.; Dellavia, C.; Tartaglia, G.M.; Sozzi, D.; Carù, A. A quantitative three-dimensional assessment of abnormal variations in facial soft tissues of adult patients with cleft lip and palate. Cleft Palate-Craniofacial J. 2003, 40, 544–549. [Google Scholar] [CrossRef]
- Majeed, M.I.; Haralur, S.B.; Khan, M.F.; Al Ahmari, M.A.; Al Shahrani, N.F.; Shaik, S. An anthropometric study of cranio-facial measurements and their correlation with vertical dimension of occlusion among Saudi Arabian subpopulations. Open Access Maced. J. Med. Sci. 2018, 6, 680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ercan, I.; Ozdemir, S.T.; Etoz, A.; Sigirli, D.; Tubbs, R.S.; Loukas, M.; Guney, I. Facial asymmetry in young healthy subjects evaluated by statistical shape analysis. J. Anat. 2008, 213, 663–669. [Google Scholar] [CrossRef]
- Chou, T.M.; Moore, D.J.; Young, L.; Glaros, A.G. A diagnostic craniometric method for determining occlusal vertical dimension. J. Prosthet. Dent. 1994, 71, 568–574. [Google Scholar] [CrossRef]
- Hayakawa, I. Principles and Practices of Complete Dentures: Creating the Mental Image of a Denture; Quintessence: Chicago, IL, USA, 1999; ISBN 4874176070. [Google Scholar]
- Slavicek, R.; Tajima, K.; Sudmann, V. Importance of skeletal location of maxilla to determine the vertical dimension of occlusion. Int. J. Stomatol. Occlusion Med. 2010, 3, 159–164. [Google Scholar] [CrossRef]
- Rickets, R.M. Orthodontic Diagnosis and Planning-Their Roles in Preventive and Rehabilitative Dentristy; Rocky Mountain Orthodontics: Denver, CO, USA, 1982; Volume 1. [Google Scholar]
- Yamashita, S.; Shimizu, M.; Katada, H. A Newly Proposed Method to Predict Optimum Occlusal Vertical Dimension. J. Prosthodont 2015, 24, 287–290. [Google Scholar] [CrossRef]
- Edwards, C.L.; Richards, M.W.; Billy, E.I.; Neilans, L.C. Using computerized cephalometrics to analyze the vertical dimension of occlusion. Int. J. Prosthodont. 1993, 6, 371–376. [Google Scholar]
- Cristache, C.M.; Totu, E.E.; Iorgulescu, G.; Pantazi, A.; Dorobantu, D.; Nechifor, A.C.; Isildak, I.; Burlibasa, M.; Nechifor, G.; Enachescu, M. Eighteen Months Follow-Up with Patient-Centered Outcomes Assessment of Complete Dentures Manufactured Using a Hybrid Nanocomposite and Additive CAD/CAM Protocol. J. Clin. Med. 2020, 9, 324. [Google Scholar] [CrossRef] [Green Version]
- Bondevik, O. Growth changes in the cranial base and the face: A longitudinal cephalometric study of linear and angular changes in adult norwegians. Eur. J. Orthod. 1995, 17, 525–532. [Google Scholar] [CrossRef]
- Rivera-Morales, W.C.; Mohl, N.D. Relationship of occlusal vertical dimension to the health of the masticatory system. J. Prosthet. Dent. 1991, 65, 547–553. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Min. | Max. | Mean (±SD) |
|---|---|---|---|
| Sn–PM in OVD (mm) | 29 | 63 | 50.20 (±9.06) |
| Sn–PM in RVD (mm) | 31 | 67 | 52.33 (±10.39) |
| Sn–Gn in OVD (mm) OVD | 44 | 73 | 62.47 (±6.77) |
| Sn–Gn in RVD (mm) RVD | 48 | 76 | 66.07 (±6,84) |
| Pu–Ch_r (mm) | 63 | 78 | 70.07 (±3.92) |
| Pu–Ch_l (mm) | 66 | 76 | 71.40 (±3.02) |
| LFHˆ | 34.66° | 51.04° | 42.31° (±4.29) |
| MLˆFH | 11.33° | 34.36° | 22.15° (±6.35) |
| Facial Profile | Number of Subjects (N) | Mean LFHˆ (±SD) | Reference (±Accepted Variation) | Mean Difference | p Value |
|---|---|---|---|---|---|
| Brachyfacial | 48 | 39.06° (±4.29°) | 44° (±2.5°) | −4.94 | 0.758 |
| Mesofacial | 60 | 42.91° (±2.16°) | 49° (±2.5°) | −6.09 | 0.990 |
| Dolichofacial | 42 | 45.48° (±4.70°) | 54° (±2.5°) | −8.52 | 0.692 |
| Sn–PM OVD | Sn–PM RVD | OVD | RVD | Pu–Ch_r | Pu–Ch_l | LFHˆ | MLˆFH | ||
|---|---|---|---|---|---|---|---|---|---|
| Sn–PM OVD | Pearson Correlation | 1 | 0.967 ** | 0.751 ** | 0.809 ** | 0.648 ** | 0.352 | 0.400 | 0.172 |
| p value | - | 0.000 | 0.001 | 0.000 | 0.009 | 0.198 | 0.141 | 0.539 | |
| Sn–PM RVD | Pearson Correlation | 0.967 ** | 1 | 0.851 ** | 0.907 ** | 0.687 * | 0.344 | 0.414 | 0.096 |
| p value | 0.00 | - | 0.000 | 0.000 | 0.005 | 0.210 | 0.125 | 0.735 | |
| OVD | Pearson Correlation | 0.751 ** | 0.851 ** | 1 | 0.960 ** | 0.785 ** | 0.448 | 0.518 * | 0.005 |
| p value | 0.001 | 0.000 | - | 0.000 | 0.001 | 0.094 | 0.048 | 0.985 | |
| RVD | Pearson Correlation | 0.809 ** | 0.907 ** | 0.960** | 1 | 0.778 ** | 0.331 | 0.565 * | 0.057 |
| p value | 0.000 | 0.000 | 0.000 | - | 0.001 | 0.229 | 0.028 | 0.839 | |
| Pu–Ch_r | Pearson Correlation | 0.648 ** | 0.687 ** | 0.785 ** | 0.778 ** | 1 | 0.650 ** | 0.405 | 0.102 |
| p value | 0.009 | 0.005 | 0.001 | 0.001 | - | 0.009 | 0.135 | 0.717 | |
| Pu–Ch_l | Pearson Correlation | 0.352 | 0.344 | 0.448 | 0.331 | 0.650 ** | 1 | 0.100 | 0.148 |
| p value | 0.198 | 0.210 | 0.094 | 0.229 | 0.009 | - | 0.723 | 0.599 | |
| LFHˆ | Pearson Correlation | 0.399 | 0.414 | 0.518 * | 0.565 * | 0.405 | 0.100 | 1 | 0.611 * |
| p value | 0.141 | 0.125 | 0.048 | 0.028 | 0.135 | 0.723 | - | 0.016 | |
| MLˆFH | Pearson Correlation | 0.172 | 0.096 | 0.005 | 0.057 | 0.102 | 0.148 | 0.611 * | 1 |
| p value | 0.539 | 0.735 | 0.985 | 0.839 | 0.717 | 0.599 | 0.016 | - | |
| Correlation | R2 | Regression Formula |
|---|---|---|
| OVD–RVD | 0.9221 | y = 0.9505x − 0.3316. |
| OVD–Sn–PM RVD | 0.7235 | y = 0.5543x + 33.461 |
| OVD–Sn–PM OVD | 0.5638 | y = 0.5613x + 34.289 |
| OVD–Pu–Ch_r | 0.6162 | y = 1.3564x – 32.571 |
| OVD–LFHˆ | 0.2678 | y = 0.3284x + 21.794 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oancea, L.; Burlibasa, M.; Petre, A.E.; Panaitescu, E.; Cristache, C.M. Predictive Model for Occlusal Vertical Dimension Determination and Digital Preservation with Three-Dimensional Facial Scanning. Appl. Sci. 2020, 10, 7890. https://doi.org/10.3390/app10217890
Oancea L, Burlibasa M, Petre AE, Panaitescu E, Cristache CM. Predictive Model for Occlusal Vertical Dimension Determination and Digital Preservation with Three-Dimensional Facial Scanning. Applied Sciences. 2020; 10(21):7890. https://doi.org/10.3390/app10217890
Chicago/Turabian StyleOancea, Luminita, Mihai Burlibasa, Alexandru Eugen Petre, Eugenia Panaitescu, and Corina Marilena Cristache. 2020. "Predictive Model for Occlusal Vertical Dimension Determination and Digital Preservation with Three-Dimensional Facial Scanning" Applied Sciences 10, no. 21: 7890. https://doi.org/10.3390/app10217890