
Recent Advances in Myoelectric Control for Finger Prostheses for Multiple Finger Loss
by
 , , , and
, , , and
Viritpon Srimaneepong
1 ,
,
Artak Heboyan
2 ,
,
Azeem Ul Yaqin Syed
3 ,
,
Hai Anh Trinh
4,5,
Pokpong Amornvit
6 and
Dinesh Rokaya
7,* 1
Department of Prosthodontics, Faculty of Dentistry, Chulalongkorn University, Bangkok 10330, Thailand
2
Department of Prosthodontics, Faculty of Stomatology, Yerevan State Medical University, Str. Koryun 2, Yerevan 0025, Armenia
3
Department of Prosthodontics, Fatima Jinnah Dental College, Karachi 74900, Pakistan
4
Department of Implantology, Ha Noi National Hospital of Odonto-stomatology, Hanoi 100000, Vietnam
5
VNU School of Medicine and Pharmacy, Vietnam National University, Hanoi 10000, Vietnam
6
Maxillofacial Prosthetic Center, Golden Jubilee Medical Center, Mahidol University, Salaya 73170, Thailand
7
Department of Clinical Dentistry, Walailak University International College of Dentistry, Walailak University, Bangkok 10400, Thailand
*
Author to whom correspondence should be addressed.
Appl. Sci. 2021, 11(10), 4464; https://doi.org/10.3390/app11104464
Submission received: 3 April 2021
/
Revised: 20 April 2021
/
Accepted: 3 May 2021
/
Published: 14 May 2021
(This article belongs to the Special Issue Orthopaedic and Rehabilitation Engineering II)
Abstract
:The loss of one or multiple fingers can lead to psychological problems as well as functional impairment. Various options exist for replacement and restoration after hand or finger loss. Prosthetic hand or finger prostheses improve esthetic outcomes and the quality of life for patients. Myoelectrically controlled hand prostheses have been used to attempt to produce different movements. The available articles (original research articles and review articles) on myoelectrically controlled finger/hand prostheses from January 1922 to February 2021 in English were reviewed using MEDLINE/PubMed, Web of Science, and ScienceDirect resources. The articles were searched using the keywords “finger/hand loss”, “finger prosthesis”, “myoelectric control”, and “prostheses” and relevant articles were selected. Myoelectric or electromyography (EMG) signals are read by myoelectrodes and the signals are amplified, from which the muscle’s naturally generated electricity can be measured. The control of the myoelectric (prosthetic) hands or fingers is important for artificial hand or finger movement; however, the precise control of prosthetic hands or fingers remains a problem. Rehabilitation after multiple finger loss is challenging. Implants in finger prostheses after multiple finger loss offer better finger prosthesis retention. This article presents an overview of myoelectric control regarding finger prosthesis for patients with finger implants following multiple finger loss.
1. Introduction
Hands and fingers have a vital role in daily life for various functions and esthetics. The loss of a hand or finger (one or more) may be a result of trauma, disease, or congenital abnormalities. The loss of hands and fingers can lead to psychological problems, functional impairment, and social dysfunction [1]. Various options exist for replacement and restoration after hand and finger loss. For finger loss, the amount of tissue loss, the extent of finger loss (carpel, metacarpal, phalanges), and the number of fingers lost must be considered in treatment planning [2,3]. Prosthetic hand or finger prostheses improve esthetic outcomes and quality of life for patients. Passive hand or finger prostheses are mostly fabricated from silicone retained from adhesive or as implants that are robust and difficult or impossible regarding movement. Such passive devices may be able to perform limited activities [4,5]; however, a bionic hand substantially improves the functional outcome [6].
There has been considerable development in the biomedical field due to the development of engineering and digital technologies [7,8,9,10]. Nowadays, commercial prosthetic hands are becoming advanced and offer a range of individual hand/finger movements. The use of myoelectrical control in hand prostheses to produce different movements is common in the literature [11,12,13]; however, the precise control of prosthetic hands or fingers is still a problem. Although different methods have been proposed to control a prosthetic hand or finger, the expected function is difficult to achieve. Various methods to command a prosthetic hand include a joystick, push buttons, keyboard, vision, speech, electromyography (EMG), electroencephalography (EEG), and electroneurography (ENG). Among all, electromyographical techniques are most commonly used in prosthetics. EMG is also sometimes called surface EMG (sEMG). This article presents an overview of myoelectric control for hand/finger prostheses in the context of multiple finger loss and the use of implants. In the market, various myoelectric hand prostheses are available but feature limited hand movement, control, and control speed. The motor cortex’s output through corticospinal projection is important in producing individuated hand/finger movements. The use of an implant in a finger bone can aid the retention of a myoelectrically controlled finger or hand prosthesis in producing different movements.
2. Methodology
Available articles on myoelectrically controlled finger/hand prostheses were reviewed from January 1922 to February 2021 using the MEDLINE/PubMed, Web of Science, and ScienceDirect resources in English. The articles were searched using the keywords “finger loss”, “hand loss”, “hand prosthesis”, “finger prosthesis”, “prostheses”, “myoelectric control”, “myoelectrically control”, and relevant articles were selected.
The inclusion criteria of the articles included original research articles and review articles in English from January 1922 to February 2021. The exclusion criteria for articles included case reports and editorial and commentary articles.
3. Signals and Finger Motor Function
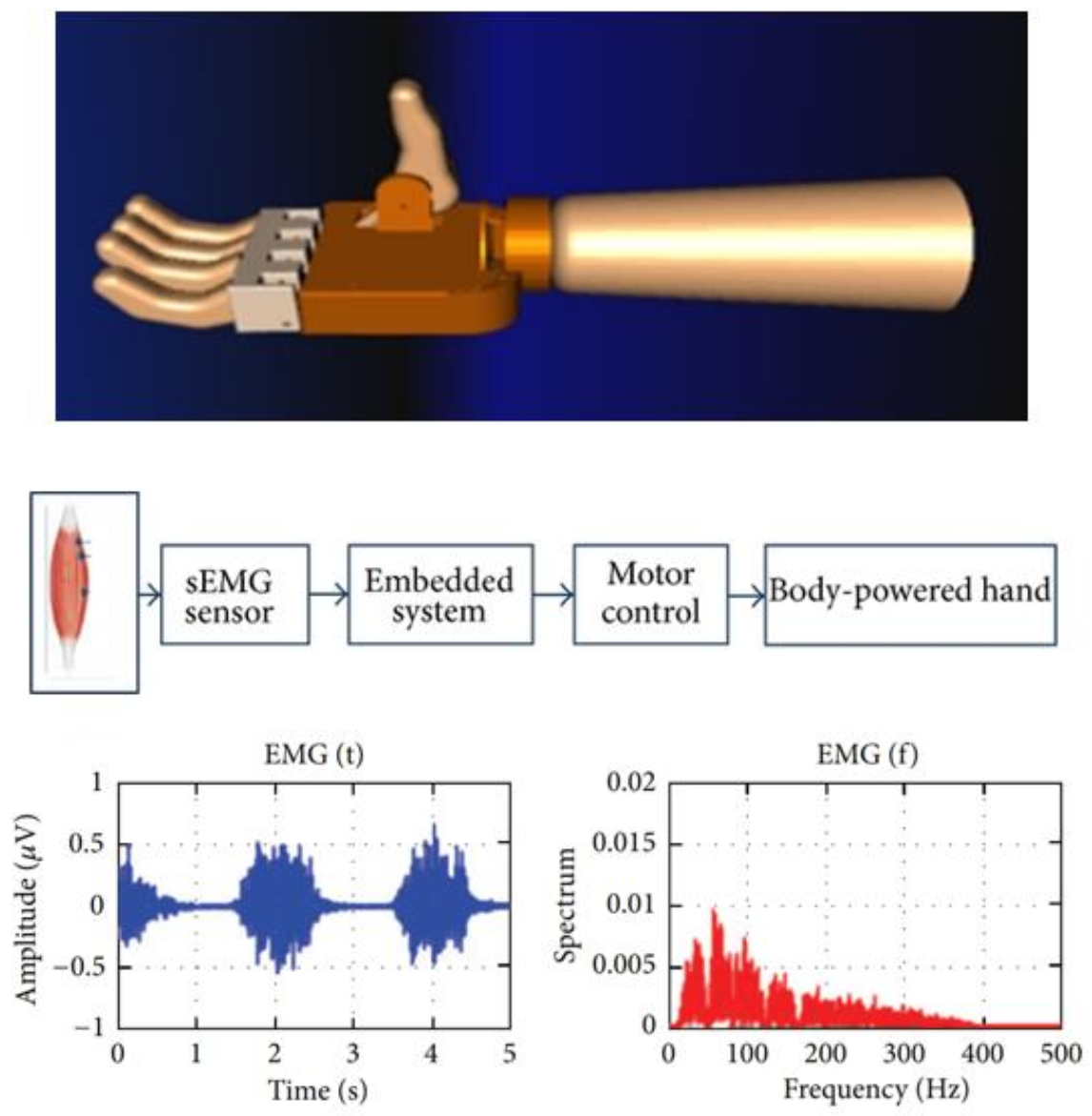
Signals are important for the control of the myoelectrical (prosthetic) hands or fingers. Figure 1 shows a myoelectrically controlled hand prosthesis (designed in computer software), a design to collect EMG signals, and the generated signals [14].
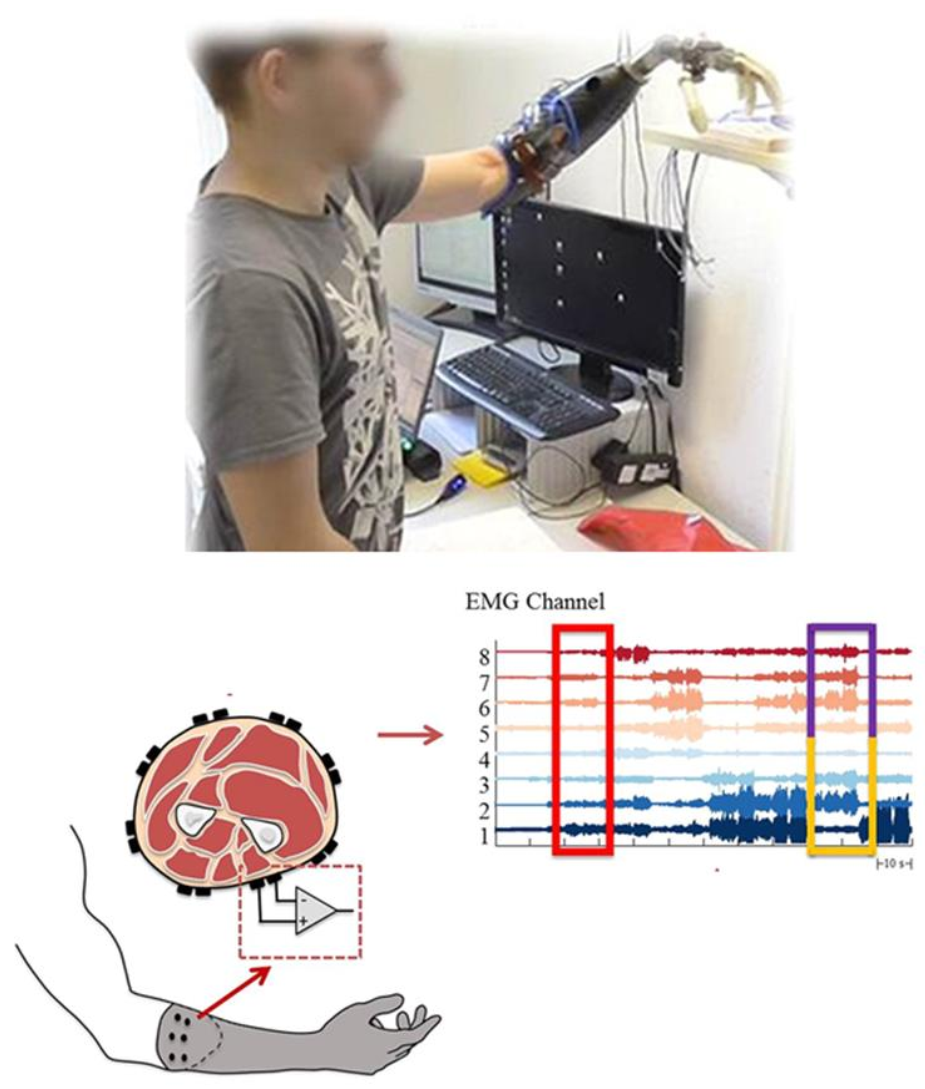
The motor and sensory components of the hand provide an individual with high functionality and elegant behavior through a complex integrated system [15]. Human hands can perform numerous actions, varying from handling heavy objects to fine digital movements while directly connecting with the brain. It would ideal if similar movements can be performed by prosthetic hands and fingers. An intelligent interface that controls prosthetic hands and fingers can suggest movement by interpreting a muscle’s electrical activity via the surface EMG signal [16,17]. Figure 2 shows a myoelectrically controlled hand prosthesis, the generation of signals, and EMG channels [6]. The myoelectric activities of the residual limb for the phantom limb movements (PLM) may help for pattern recognition in the context of myoelectrical control [17].
Finger movements require specific stimulation of a group of muscles [18]. Such stimulation is principally controlled by the motor cortex through the corticospinal tract. The motor cortex’s output operates via corticospinal projection, which is important for the movements of the finger. Normally, an action potential propagates and activates a motor neuron which in turn activates the muscle fibers. When the depolarization of the postsynaptic membrane of muscle fiber takes place, the depolarization spreads along the fiber supplemented by the movement of ions and generates an electromagnetic field [19]. Myoelectric or EMG signals are read by microelectrodes and the signals are amplified, from which the muscle’s naturally generated electricity can be measured [16]. The signals are assigned to control the movement of the prosthesis after processing. Specific EMG pulse sequences are linked to a specific movement of the prosthesis. The predefined movements are controlled by specific signals [20].
The effectiveness of prosthetic hands can be assessed by user performance when performing functional tasks. Chadwell et al. [21] compared the upper limb activity between myoelectric prosthesis users and normal adults and found that temporal patterns in upper limb activity were present. It was also found that prosthesis users were greatly reliant on their intact limbs for daily activities. There was no significant correlation between the kinematic and the gaze-related performance between myoelectric prosthesis users and normal adults.
Access to the neural control information for an arm is lost during amputation. Hence, improving the function of hands or finger prosthesis poses a challenge. Various invasive methods have been proposed to generate proper signals for myoelectrical prostheses, such as peripheral nerve signal transmission [22], motor cortex [23], or targeted muscle reinnervation (TMR) [24] methods. In TMR, the muscle of the amputee is reinnervated with the residual nerves of the amputated limb. Following the reinnervation, the target muscles produce EMG signals, and these signals can control the prosthetic hand/arm and have promising results [25]. Engdahl et al. [26] studied four types of control for a prosthetic hand (TMR, myoelectric, cortical interfaces, and peripheral nerve interfaces) in upper-limb amputees and found that the participants showed a maximum positive response for the myoelectrical interface, while they showed the least interest for the cortical interface. More skillful individual and combined finger control has not yet been gained [27]. Khushaba et al. [27] investigated the accuracy of individual and combined finger movements using surface EMG signals using Bayesian data fusion in postprocessing for the proper classification of EMG data belonging to different movements. Similarly, Isaković et al. [28] purposed a feedback interface for a myoelectric prosthesis with multiple degrees of freedom that allows proprioceptive and sensory information (i.e., the grasping force). In this method, nine subjects performed a sequential algorithm in a time comparable to that reported when performed by experts and found that amplitudes can be significantly streamlined to a quarter of initial time without reducing the outcome when using prior knowledge in setting the baseline stimulation.
Atzori et al. [20] studied the natural control of robotic hands via sEMG using healthy subjects and amputees. A neural network was used to evaluate the effects of the pre-processing, layer architecture, data augmentation, and optimization. The results show that convolutional neural networks with simple architecture can produce precise results comparable to the average classical classification methods. They also show that several factors (pre-processing, net architecture, and parameters for optimization) are important for the analysis of sEMG data. More accuracy for computer vision and object recognition tasks is seen with larger networks.
Recently, multimodal data acquisition has been applied for the EMG-based detection of hand/finger movement [20,29,30,31]. Accelerometers can be combined with EMG electrodes to produce excellent capabilities to recognize hand movements [32]. Similarly, convolutional neural networks and deep learning have revolutionized machine learning, computer vision, and speech recognition. Deep learning is used in deep neural network applications and reinforcement learning to maximize the performance of a machine or software agent by itself making errors [33]. The neural networks have been applied to EMG hand movement recognition. The highest accuracy can be seen when combined convolutional neural networks with the retrained network. Table 1 shows the summary of developments in myoelectric finger prostheses and research outcomes.
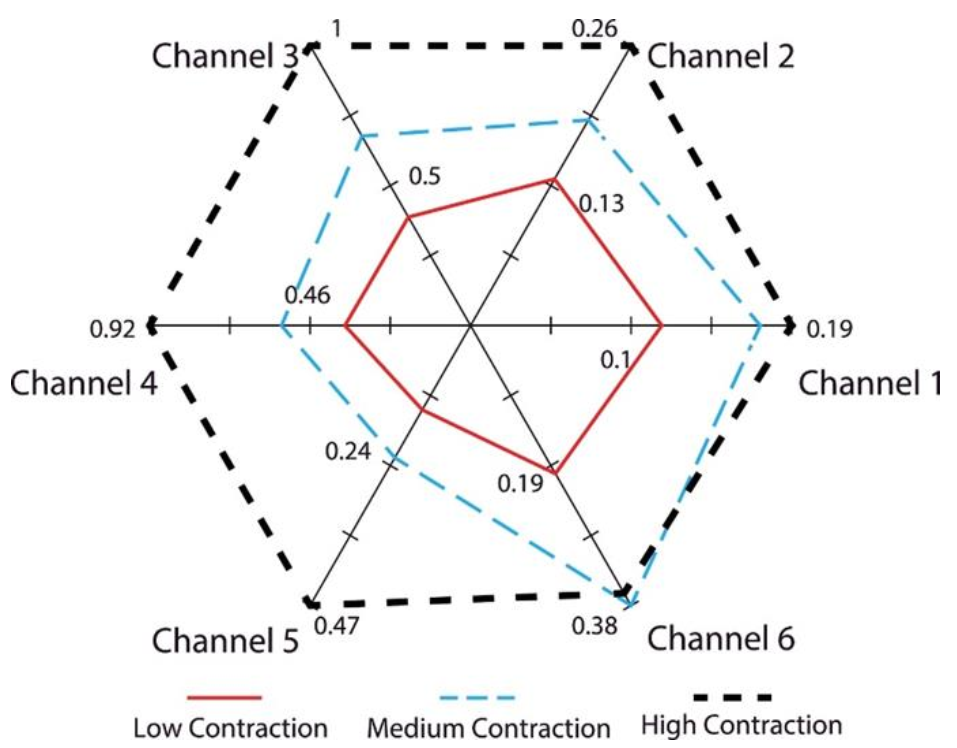
Furthermore, EMG-driven prosthesis performance is influenced by various factors, such as electrode position shifting, varying muscle contraction levels, forearm orientation, and limb position [16]. In addition, Khushaba et al. [16] investigated the combined effect of forearm orientation and muscle contraction levels on the generalizability of EMG pattern recognition. They first verified whether the subjects could produce EMG activity in all different classes of movement at three muscular contraction levels (low, medium, and high) by analyzing the RMS of EMG activity across all channels, orientations, and movements. Figure 3 shows the representative radar plot of the EMG signals RMS values collected from one subject performing wrist flexion (C4) when the wrist was fully pronated. The RMS values from the different channels were then grouped in separate columns for each force level, thereby constructing an RMS matrix. They found a significant difference (p = 0.003) between the means of the different force levels. They also mentioned that multiple factors can influence the accuracy of EMG pattern recognition.
4. Cosmetic Gloves for Myoelectric Prosthetic Hand or Fingers
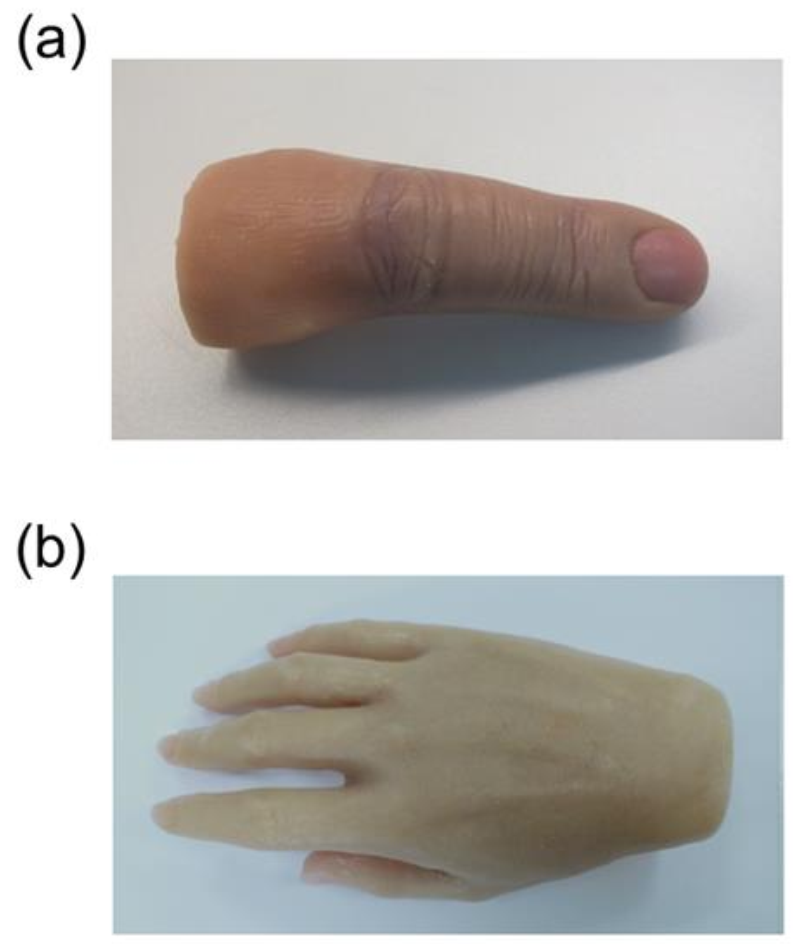
Humiliation arising from the use of a prosthetic finger or hand has been considerably reduced because of esthetic improvements. Coverings and gloves have been developed to approximate natural skin tones and they allow visualization of the metallic infrastructure beneath. There are different passive prosthetic gloves available for finger/hand rehabilitation such as electrically powered, activity-specific, body-powered, and hybrid models. A body-powered glove is durable as it is directly driven by body parts (joints and wrist). The cosmetic gloves for myoelectric prosthetic hands can be made from various superelastic rubbers, such as silicone rubber (TSG silicone), a thermoplastic styrene elastomer (TSE), or polyvinyl chloride (PVC) for a realistic appearance and support for flexible motion. Figure 4 shows the silicone prosthesis for finger and hand finger rehabilitation.
Yabuki et al. [48] compared TSE, TSG silicone, and PVC gloves for myoelectric prosthetic hands. They found that the differences were small and showed a similar range of motion. The flexible TSE resulted in easy fitting with the lowest fitting time and was hard to break and featured convenient elasticity. Both TSG silicone and TSE gloves showed similar results for grasping objects in pick-and-place experiments. Furthermore, TSG resin is a thermoset material and can be processed at room temperature. Therefore, the TSG silicone material was more suitable for implementing a sensor.
Similarly, Sareen et al. [49] fabricated a prosthetic glove prototype from polylactic acid using 3D printing for hand rehabilitation. The best design prototype was a half-ring servomotor-operated design which is easily adjustable with varying patient finger dimensions. The prototype could produce finger movements using strings attached to servomotors. In addition, this device could be integrated with force-sensitive resistors and controllers for different disability levels; however, the durability of the coverings requires diligent care and adds further costs to the prosthesis.
5. Osseointegrated Implant Retained Myoelectric Prosthesis
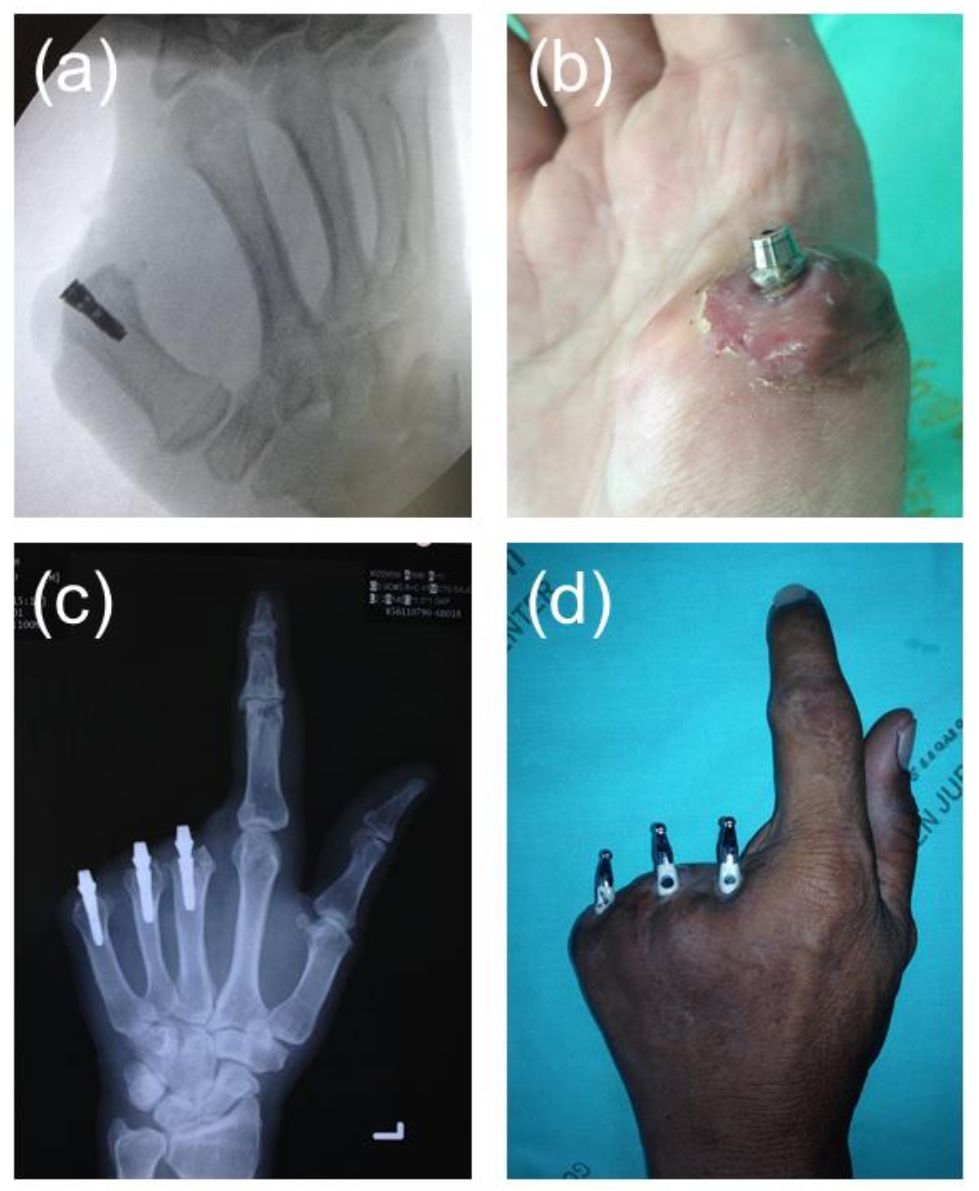
Retention is one of the key factors in the success of a myoelectric finger prosthesis for functions such as grasping, carrying, and holding [50]. A friction or adhesive-retained finger prosthesis cannot provide adequate retention. Bone-anchored osseointegration was originally investigated by the Swedish dentist Per-Ingvar Brånemark [51]. An osseointegrated implant retained finger prosthesis offers better retention and helps in different functions [52,53]. Figure 5 shows implants in a finger bone used for the retention of finger prostheses. In two cases, dental implants were placed in the finger bone to retain the silicone prosthesis. In case 1 (Figure 5a,b), a single implant of 5 mm in diameter × 17 mm in length (Osseo Speed, Astra Tech, Molndal, Sweden) was placed in the bone inside the medullary canal with an insertion torque of 40 Ncm for the thumb for single finger loss, whereas in case 2 (Figure 5c,d), three implants of the same size and same insertion were placed on each middle, ring, and little finger thumb for multiple finger loss. Radiographs were taken to verify the position of the implant. Customized metal abutments were fabricated to aid the retention of the silicone prostheses. The mode of retention of the silicone prostheses was friction retained with the metal abutment.
Finger bone implants also help to reduce the prosthesis failure rate [54]. In addition, osseointegrated implants improve functionality, durability, and freedom of movement in the prosthesis, as well supporting vibrotactile and pressure feedback secondary to osseoperception [55,56,57,58]. Osseointegration considers many complications and restrictions inherent to socket-based prostheses, particularly among patients with compromised soft tissue envelopes (e.g., decreased tissue compliance, history of skin grafting, persistent ulceration, or wounds, underlying heterotopic bone, painful neuromas) or a short residual limb [59]. It also eliminates issues related to socket fit and signal transduction between the myositis and the electrodes, improving the efficiency of these devices.
Excellent development in osseointegration arises from the incorporation of motosensory devices into the implant itself [59]. An example of such a device is e-OPRA (Integrum, Sweden), which contains a bidirectional interface using electrodes integrated with the device to improve control of the osseointegrated prosthesis. Currently, clinical trials are being conducted on the e-OPRA device in the USA and are expected to complete by January in 2023 [55]. It has been shown that promising results with more reliability and precision for implanted electrodes than surface electrodes can be found among transhumeral amputees [60,61]. Mastinu et al. [62] studied grip control and motor coordination in three transhumeral amputees with the e-OPRA device. The synergy between bone-anchored devices, advanced neuromuscular interfaces, and targeted muscle reinnervation can significantly improve the sensory and motor function of advanced prostheses.
The main limitation of the above techniques for finger prostheses is that they cannot permit active pronation, supination, flexion, and extension. The use of an implant in the finger bone can aid the retention of myoelectrically controlled finger prostheses regarding finger movements.
6. Discussion
There has been a significant improvement in finger and hand prostheses from passive hooks and shoulder harnesses to myoelectrically controlled prostheses [34,43,45,46]. At present, there are various myoelectrically controlled commercial prosthetic hands in the markets and they offer a range of individual hand/finger movements [11,12,13]. Some commonly used models include the i-Limb, Vincent Hand, i-Limb Pulse, SensorHand, BeBionic, BeBionic V2, and Michelangelo models [43,44,45,46,47]. Still, the precise control of prosthetic hands or fingers is a problem.
The myoelectric activities of the residual limb for phantom limb movements help for the pattern recognition regarding myoelectric control and intelligent interfaces can control prosthetic hands and fingers, which can suggest finger and hand movement. The signals are assigned to control the movement of the finger/hand prosthesis. The muscle’s electrical activity can be interpreted by the sEMG signal [16,17]. Several factors (pre-processing, net architecture, and parameters for optimization) are important for the analysis of sEMG data. More accuracy on computer vision and object recognition tasks is seen with larger networks [20].
Osseointegrated implants in retained finger prosthesis offer better retention and help in different functions [52]. In addition, osseointegrated implants improve functionality, durability, and freedom of movement in the prosthesis, as well vibrotactile and pressure feedback secondary to osseoperception [54,55,56,57]. An example of this is grip control and motor coordination in three transhumeral amputees with the e-OPRA device [60]. The synergy between bone-anchored devices, advanced neuromuscular interfaces, and targeted muscle reinnervation can significantly improve the sensory and motor function of advanced prostheses.
7. Future Perspectives in Myoelectric Prosthesis
Currently, although myoelectrical prosthetic fingers/hands in the market feature advanced mechanics, the control methods are still rudimentary in most cases. Most myoelectrical hand prostheses lack somatosensory feedback and 100% control robustness, cannot provide sufficient control speed, and are incapable of reproducing various hand movements [20,28]. Hence, they are not sufficient for many real-life applications. The main reason for the lacking robustness is the motion artifacts which typically occur in the low-frequency range [63]. Real-time motion artifact suppression algorithms can be used on an ultra-low-power microcontroller to achieve high robustness.
All myoelectrical control-based prosthetic hands may not have similar operations and exhibit variations in sensing input, deciphering signals, and actuating prosthetic hands [64,65]. The factors that influence myoelectrical fingers/hand prostheses are the shape of the first layer of the network, initial weights of the layers, data augmentation procedures, and the learning rate [20]. The EMG architecture can be made more complex and can be trained with EMG data to produce higher accuracy. Further research and development are necessary for precise control of various prosthetic hand movements with sufficient speed and robust control.
8. Conclusions
Motor cortex output through corticospinal projection is important in producing individuated finger movements. In the market, various myoelectrical hand prostheses are available but feature limited hand movement, control, and control speed. The use of a finger bone implant can aid the retention of myoelectrically controlled finger or hand prostheses regarding the production of different movements. Further research and development are necessary for the precise control of various prosthetic hand movements with sufficient speed and robust control.
Author Contributions
Conceptualization, D.R., P.A. and V.S.; methodology, D.R.; software, D.R.; validation, D.R., V.S. and P.A.; formal analysis, D.R.; investigation, D.R.; resources, D.R. and P.A.; data curation, D.R.; writing—original draft preparation, D.R., A.H., A.U.Y.S. and H.A.T.; writing—review and editing, D.R., V.S., A.H., H.A.T. and A.U.Y.S.; visualization, V.S., A.H., A.U.Y.S. and H.A.T.; supervision, P.A. and V.S.; project administration, D.R. and V.S.; funding acquisition, V.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Aydin, C.; Nemli, S.K.; Yilmaz, H. Esthetic, functional, and prosthetic outcomes with implant-retained finger prostheses. Prosthet. Orthot. Int. 2013, 37, 168–174. [Google Scholar] [CrossRef]
- Aydin, C.; Karakoca, S.; Yilmaz, H. Implant-retained digital prostheses with custom-designed attachments: A clinical report. J. Prosthet. Dent. 2007, 97, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Manurangsee, P.; Isariyawut, C.; Chatuthong, V.; Mekraksawanit, S. Osseointegrated finger prosthesis: An alternative method for finger reconstruction. J. Hand Surg. 2000, 25, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Thongpulsawasdi, N.; Amornvit, P.; Rokaya, D.; Keawcharoen, K. Adhesive vs Implant Retained Fingers Prosthesis: A Comparative Study on Esthetic and Functional Outcome. World Appl. Sci. J. 2014, 29, 1015–1019. [Google Scholar]
- Rokaya, D.; Kitisubkanchana, J.; Wonglamsam, A.; Santiwong, P.; Srithavaj, T.; Humagain, M. Nepalese Esthetic Dental (NED) Proportion in Nepalese Population. Kathmandu Univ. Med. J. 2015, 13, 244–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aszmann, O.C.; Vujaklija, I.; Roche, A.D.; Salminger, S.; Herceg, M.; Sturma, A.; Hruby, L.A.; Pittermann, A.; Hofer, C.; Amsuess, S.; et al. Elective amputation and bionic substitution restore functional hand use after critical soft tissue injuries. Sci. Rep. 2016, 6, 34960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humagain, M.; Rokaya, D. Integrating Digital Technologies in Dentistry to Enhance the Clinical Success. Kathmandu Univ. Med. J. 2019, 17, 256–257. [Google Scholar]
- Chang, Y.S. Advances in technology are changing the future of medicine. Asia Pac. Allergy 2016, 6, 137–138. [Google Scholar] [CrossRef] [Green Version]
- Adam, N.R.; Wieder, R.; Ghosh, D. Data science, learning, and applications to biomedical and health sciences. Ann. N. Y. Acad. Sci. 2017, 1387, 5–11. [Google Scholar] [CrossRef] [Green Version]
- Avetisyan, A.; Markaryan, M.; Rokaya, D.; Tovani-Palone, M.R.; Zafar, M.S.; Khurshid, Z.; Vardanyan, A.; Heboyan, A. Characteristics of Periodontal Tissues in Prosthetic Treatment with Fixed Dental Prostheses. Molecules 2021, 26, 1331. [Google Scholar] [CrossRef]
- Weir, R.; Grahn, E.; Duff, S. A new externally powered, myoelectrically controlled prosthesis for persons with partial-hand amputations at the metacarpals. J. Prosthet. Orthot. 2001, 13, 26–31. [Google Scholar] [CrossRef]
- Agnew, P.J. Functional effectiveness of a myo-electric prosthesis compared with a functional split-hook prosthesis: A single subject experiment. Prosthet. Orthot. Int. 1981, 5, 92–96. [Google Scholar] [CrossRef] [Green Version]
- Pistohl, T.; Cipriani, C.; Jackson, A.; Nazarpour, K. Abstract and proportional myoelectric control for multi-fingered hand prostheses. Ann. Biomed. Eng. 2013, 41, 2687–2698. [Google Scholar] [CrossRef] [Green Version]
- Salem, F.H.A.; Mohamed, K.S.; Mohamed, S.B.K.; Gehani, A.A.E. The development of body-powered prosthetic hand controlled by EMG signals using DSP processor with virtual prosthesis implementation. Conf. Pap. Eng. 2013, 598945. [Google Scholar] [CrossRef] [Green Version]
- Montagnani, F.; Controzzi, M.; Cipriani, C. Independent long fingers are not essential for a grasping hand. Sci. Rep. 2016, 6, 35545. [Google Scholar] [CrossRef] [Green Version]
- Khushaba, R.N.; Al-Timemy, A.; Kodagoda, S.; Nazarpour, K. Combined influence of forearm orientation and muscular contraction on EMG pattern recognition. Expert Syst. Appl. 2016, 61, 154–161. [Google Scholar] [CrossRef] [Green Version]
- Touillet, A.; Peultier-Celli, L.; Nicol, C.; Jarrassé, N.; Loiret, I.; Martinet, N.; Paysant, J.; De Graaf, J.B. Characteristics of phantom upper limb mobility encourage phantom-mobility-based prosthesis control. Sci. Rep. 2018, 8, 15459. [Google Scholar] [CrossRef]
- Schieber, M.H.; Lang, C.E.; Reilly, K.T.; McNulty, P.; Sirigu, A. Selective activation of human finger muscles after stroke or amputation. Adv. Exp. Med. Biol. 2009, 629, 559–575. [Google Scholar]
- Wang, N.; Lao, K.; Zhang, X. Design and myoelectric control of an anthropomorphic prosthetic hand. J. Bionic Eng. 2017, 14, 47–59. [Google Scholar] [CrossRef]
- Atzori, M.; Cognolato, M.; Müller, H. Deep learning with convolutional neural networks applied to electromyography data: A resource for the classification of movements for prosthetic hands. Front. Neurorobot. 2016, 10, 9. [Google Scholar] [CrossRef] [Green Version]
- Chadwell, A.; Kenney, L.; Granat, M.H.; Thies, S.; Head, J.; Galpin, A.; Baker, R.; Kulkarni, J. Upper limb activity in myoelectric prosthesis users is biased towards the intact limb and appears unrelated to goal-directed task performance. Sci. Rep. 2018, 8, 11084. [Google Scholar] [CrossRef]
- Urbanchek, M.G.; Baghmanli, Z.; Moon, J.D.; Sugg, K.B.; Langhals, N.B.; Cederna, P.S. Quantification of regenerative peripheral interface signal transmission. Plast. Reconstr. Surg. 2012, 130, 55–56. [Google Scholar] [CrossRef] [Green Version]
- Chestek, C.A.; Gilja, V.; Nuyujukian, P.; Foster, J.D.; Fan, J.M.; Kaufman, M.T.; Churchland, M.M.; Rivera-Alvidrez, Z.; Cunningham, J.P.; Ryu, S.I.; et al. Long-term stability of neural prosthetic control signals from silicon cortical arrays in rhesus macaque motor cortex. J. Neural Eng. 2011, 8, 045005. [Google Scholar] [CrossRef] [Green Version]
- Kuiken, T.A.; Li, G.; Lock, B.A.; Lipschutz, R.D.; Miller, L.A.; Stubblefield, K.A.; Englehart, K.B. Targeted muscle reinnervation for real-time myoelectric control of multifunction artificial arms. JAMA 2009, 301, 619–628. [Google Scholar] [CrossRef] [Green Version]
- Atzori, M.; Müller, H. Control capabilities of myoelectric robotic prostheses by hand amputees: A scientific research and market overview. Front. Neurosci. 2015, 9, 162. [Google Scholar] [CrossRef]
- Engdahl, S.M.; Christie, B.P.; Kelly, B.; Davis, A.; Chestek, C.A.; Gates, D.H. Surveying the interest of individuals with upper limb loss in novel prosthetic control techniques. J. NeuroEng. Rehabil. 2015, 12, 53. [Google Scholar] [CrossRef] [Green Version]
- Khushaba, R.N.; Kodagoda, S.; Takruri, M.; Dissanayake, G. Toward improved control of prosthetic fingers using surface electromyogram (EMG) signals. Exp. Syst. Appl. 2012, 39, 10731–10738. [Google Scholar] [CrossRef]
- Isaković, M.; Malešević, J.; Keller, T.; Kostić, M.; Štrbac, M. Optimization of semiautomated calibration algorithm of multichannel electrotactile feedback for myoelectric hand prosthesis. Appl. Bionics Biomech. 2019, 9298758. [Google Scholar] [CrossRef] [PubMed]
- Došen, S.; Cipriani, C.; Kostić, M.; Controzzi, M.; Carrozza, M.C.; Popović, D.B. Cognitive vision system for control of dexterous prosthetic hands: Experimental evaluation. J. NeuroEng. Rehabil. 2010, 7, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Light, C.M.; Chappell, P.H.; Hudgins, B.; Engelhart, K. Intelligent multifunction myoelectric control of hand prostheses. J. Med. Eng. Technol. 2002, 26, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Cotton, D.P.J.; Cranny, A.; Chappell, P.H.; White, N.M.; Beeby, S.P. Control strategies for a multiple degree of freedom prosthetic hand. Meas. Control. 2007, 40, 24–27. [Google Scholar] [CrossRef] [Green Version]
- Gijsberts, A.; Atzori, M.; Castellini, C.; Müller, H.; Caputo, B. Movement error rate for evaluation of machine learning methods for sEMG-based hand movement classification. IEEE Trans. Neural. Syst. Rehabil. Eng. 2014, 22, 735–744. [Google Scholar] [CrossRef]
- Mnih, V.; Kavukcuoglu, K.; Silver, D.; Rusu, A.A.; Veness, J.; Bellemare, M.G.; Graves, A.; Riedmiller, M.; Fidjeland, A.K.; Ostrovski, G.; et al. Human-level control through deep reinforcement learning. Nature 2015, 518, 529–533. [Google Scholar] [CrossRef]
- Lange, F. Lehrbuch der Orthopädie; Gustav Fischer: New York, NY, USA, 1922. [Google Scholar]
- Weiner, N. Cybernetics, or Control and Communication in the Animal and the Machine; Wiley: New York, NY, USA, 1948. [Google Scholar]
- Reiter, R. Eine neue Elektrokunsthand. Grenzgeb Med. 1968, 4, 133–135. [Google Scholar]
- Sherman, E.D. A Russian bioelectric-controlled prosthesis: Report of a research team from the Rehabilitation Institute of Montreal. Can. Med. Assoc. J. 1964, 91, 1268–1270. [Google Scholar]
- Scott, R.N.; Tucker, F.R. Surgical implications of myoelectric control. Clin. Orthop. Relat. Res. 1968, 61, 248–260. [Google Scholar] [CrossRef]
- Dunfield, V.A.; Scott, R.N. A surgically implanted myotelemetry unit. In Proceedings of the 3rd Canadian Medical and Biological Engineering Conference, Halifax, NS, Canada, 9–11 September 1970; p. 32. [Google Scholar]
- Herberts, P.; Petersen, I. Possibilities for control of powered devices by myoelectric signals. Scand. J. Rehabil. Med. 1970, 2, 164–170. [Google Scholar]
- Englehart, K.B.; Hudgins, B. A robust, real-time control scheme for multifunction myoelectric control. IEEE Trans. Biomed. Eng. 2003, 50, 848–854. [Google Scholar] [CrossRef]
- Belter, J.T.; Segil, J.L.; Dollar, A.M.; Weir, R.F. Mechanical design and performance specifications of anthropomorphic prosthetic hands: A review. J. Rehabil. Res. Dev. 2013, 50, 599–618. [Google Scholar] [CrossRef]
- Touch Bionics. Available online: http://www.touchbionics.com/ (accessed on 25 March 2021).
- Vincent Hand. Available online: http://handprothese.de/vincent-hand/ (accessed on 25 March 2021).
- SensorHand Speed. Available online: http://www.ottobock.com/cps/rde/xchg/ob_com_en/hs.xsl/3652.html (accessed on 25 March 2021).
- RSL Steeper. Available online: http://rslsteeper.com/ (accessed on 25 March 2021).
- Michelangelo Prosthetic Hand. Available online: https://www.ottobockus.com/prosthetics/upper-limb-prosthetics/solution-overview/michelangelo-prosthetic-hand/ (accessed on 25 March 2021).
- Yabuki, Y.; Tanahashi, K.; Mouri, Y.; Murai, Y.; Togo, S.; Kato, R.; Jiang, Y.; Yokoi, H. Development of new cosmetic gloves for myoelectric prosthetic hand using superelastic rubber. Rob. Auton. Syst. 2019, 111, 31–43. [Google Scholar] [CrossRef]
- Sareen, A.; Singh, A.; Sinha, A.; Arya, A.; Arya, A.; Sapra, G.; Kumar, R.; Kumar, P.; Singh, D. Design and fabrication of prosthetic glove for hand rehabilitation. Mater. Today Proc. 2020, 28, 1612–1615. [Google Scholar] [CrossRef]
- Lundborg, G.; Brånemark, P.I.; Rosén, B. Osseointegrated thumb prostheses: A concept for fixation of digit prosthetic devices. J. Hand Surg. 1996, 21, 216–221. [Google Scholar] [CrossRef]
- Brånemark, P.I.; Hansson, B.O.; Adell, R.; Breine, U.; Lindström, J.; Hallén, O.; Ohman, A. Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-year period. Scand. J. Plast. Reconstr. Surg. 1977, 16, 1–132. [Google Scholar]
- Amornvit, P.; Rokaya, D.; Keawcharoen, K.; Raucharernporn, S.; Thongpulsawasdi, N. One- vs two stage surgery technique for implant placement in finger prosthesis. J. Clin. Diagn. Res. 2013, 7, 1956–1968. [Google Scholar]
- Amornvit, P.; Rokaya, D.; Keawcharoen, K.; Raucharernporn, S.; Thongpulsawasdi, N.; Alam, M.K. One-Stage Surgery Technique for Implant Placement in Finger Prosthesis: A Clinical Note. Int. Med. J. 2015, 22, 309–312. [Google Scholar]
- Rahyussalim, J.; Marsetio, A.F.; Saleh, I.; Kurniawati, T.; Whulanza, Y. The needs of current implant technology in orthopaedic prosthesis biomaterials application to reduce prosthesis failure rate. J. Nanomater. 2016, 5386924. [Google Scholar] [CrossRef] [Green Version]
- Hagberg, K.; Brånemark, R.; Gunterberg, B.; Rydevik, B. Osseointegrated trans-femoral amputation prostheses: Prospective results of general and condition-specific quality of life in 18 patients at 2-year follow-up. Prosthet. Orthot. Int. 2008, 32, 29–41. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, R.; Brånemark, R.; Olmarker, K.; Rydevik, B.; Van Steenberghe, D.; Brånemark, P.I. Evaluation of the psychophysical detection threshold level for vibrotactile and pressure stimulation of prosthetic limbs using bone anchorage or soft tissue support. Prosthet. Orthot. Int. 2000, 24, 133–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jönsson, S.; Caine-Winterberger, K.; Brånemark, R. Osseointegration amputation prostheses on the upper limbs: Methods, prosthetics and rehabilitation. Prosthet. Orthot. Int. 2011, 35, 190–200. [Google Scholar] [CrossRef] [Green Version]
- Lundborg, G.; Waites, A.; Björkman, A.; Rosén, B.; Larsson, E.-M. Functional magnetic resonance imaging shows cortical activation on sensory stimulation of an osseointegrated prosthetic thumb. Scand. J. Plast. Reconstr. Surg. Hand Surg. 2006, 40, 234–239. [Google Scholar] [CrossRef]
- Bates, T.J.; Fergason, J.R.; Pierrie, S.N. Technological Advances in Prosthesis Design and Rehabilitation Following Upper Extremity Limb Loss. Curr. Rev. Musculoskelet. Med. 2020, 13, 485–493. [Google Scholar] [CrossRef] [PubMed]
- e-OPRA Implant System for Lower Limb Amputees. Available online: https://clinicaltrials.gov/ct2/show/NCT03720171 (accessed on 12 March 2021).
- Ortiz-Catalan, M.; Hakansson, B.; Branemark, R. An osseointegrated human-machine gateway for long-term sensory feedback and motor control of artificial limbs. Sci. Transl. Med. 2014, 6, 257re6. [Google Scholar] [CrossRef] [PubMed]
- Mastinu, E.; Clemente, F.; Sassu, P.; Aszmann, O.; Brånemark, R.; Håkansson, B.; Controzzi, M.; Cipriani, C.; Ortiz-Catalan, M. Grip control and motor coordination with implanted and surface electrodes while grasping with an osseointegrated prosthetic hand. J. Neuroeng. Rehabil. 2019, 16, 49. [Google Scholar] [CrossRef] [PubMed]
- Roche, D.; Rehbaum, H.; Farina, D.; Aszmann, O.C. Prosthetic myoelectric control strategies: A clinical perspective. Curr. Surg. Rep. 2014, 2, 44. [Google Scholar] [CrossRef]
- Geethanjali, P. Myoelectric control of prosthetic hands: State-of-the-art review. Med. Devices 2016, 9, 247–255. [Google Scholar] [CrossRef] [Green Version]
- Igual, C.; Pardo, L.A., Jr.; Hahne, J.M.; Igual, J. Myoelectric Control for Upper Limb Prostheses. Electronics 2019, 8, 1244. [Google Scholar] [CrossRef]
Figure 1.
Myoelectrically controlled hand prosthesis designed in computer software, a design to collect the electromyography (EMG) signals, and sample generated signals [14].
Figure 1.
Myoelectrically controlled hand prosthesis designed in computer software, a design to collect the electromyography (EMG) signals, and sample generated signals [14].

Figure 2.
Active myoelectrically controlled hand prosthesis, generation of signals, and signals in the electromyography (EMG) [10].
Figure 2.
Active myoelectrically controlled hand prosthesis, generation of signals, and signals in the electromyography (EMG) [10].

Figure 3.
The results of root mean square (RMS) of the electromyogram (EMG) signals from six channels through flexion of the wrist at three different levels [16].
Figure 3.
The results of root mean square (RMS) of the electromyogram (EMG) signals from six channels through flexion of the wrist at three different levels [16].

Figure 4.
Rehabilitation of finger and hand defects using silicone prostheses: (a) finger prosthesis and (b) hand prosthesis.
Figure 4.
Rehabilitation of finger and hand defects using silicone prostheses: (a) finger prosthesis and (b) hand prosthesis.

Figure 5.
Implants placed in finger bones for the retention of finger prostheses: (a,c) implants in finger bones in an X-ray and (b,d) implants in finger bone clinically.
Figure 5.
Implants placed in finger bones for the retention of finger prostheses: (a,c) implants in finger bones in an X-ray and (b,d) implants in finger bone clinically.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Summary on the developments in myoelectric finger prostheses.
| Year | Developments | Study |
|---|---|---|
| 1922 | Passive hooks and shoulder harness were designed by Weimar. | [34] |
| 1948 | The concept of the prosthesis ideally should replace not only mechanical function but also cutaneous and kinesthetic sensation. | [35] |
| 1948 | Myoelectric control was first implemented by Reinhold Reiter, a physics student at Munich University and patent application. | [36] |
| 1968 | The first commercial myoelectric hands were available from the middle of the 1960s. | [37] |
| 1968 | The concept of natural appearance during function “dynamic cosmesis” which contributes to the complexity of design both in terms of segmental trajectories and in terms of mechanical noise is highlighted. | [38] |
| 1970 onwards | Various advancements in the Myoelectric control prostheses through research and training systems. Availability of advanced commercial limb prostheses, such as the i-Limb from Touch Bionics, BeBionic from RSL Steeper, and Michelangelo by Ottobock. | [11,14,19,20,21,24,39,40,41,42] |
Table 2.
Various myoelectric hand/finger prostheses details.
| Developed Year | Name | Producer | Size | Number of Joints | Degree of Freedom | Joint Coupling Method | Study |
|---|---|---|---|---|---|---|---|
| 2009 | i-Limb | Touch Bionics | 180–18-mm-long, 80–75-mm-wide, 35–41-mm-thick | 11 | 6 | Tendron linking MCP to PIP | [43] |
| 2010 | Vincent Hand | Vincent Systems | - | 11 | 6 | Linkage spanning MCP to PIP | [44] |
| 2010 | i-Limb Pulse | Touch Bionics | 180–182-mm-long, 80–75-mm-wide, 35–45-mm-thick | 11 | 6 | Tendron linking MCP to PIP | [43] |
| 2011 | SensorHand | Otto Bock | Glove sizes | 2 | 1 | DC Motor Worm Gear | [45] |
| 2011 | BeBionic | RSL Steeper | 198-mm-long, 90-mm-wide, 50-mm-thick | 11 | 6 | DC Motor Worm Gear | [46] |
| 2011 | BeBionic V2 | RSL Steeper | 190–200-mm-long, 84–92-mm-wide, 50-mm-thick | 11 | 6 | DC Motor Lead Screw | [46] |
| 2012 | Michelangelo | Otto Bock | - | 6 | 2 | - | [47] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Srimaneepong, V.; Heboyan, A.; Syed, A.U.Y.; Trinh, H.A.; Amornvit, P.; Rokaya, D. Recent Advances in Myoelectric Control for Finger Prostheses for Multiple Finger Loss. Appl. Sci. 2021, 11, 4464. https://doi.org/10.3390/app11104464
AMA Style
Srimaneepong V, Heboyan A, Syed AUY, Trinh HA, Amornvit P, Rokaya D. Recent Advances in Myoelectric Control for Finger Prostheses for Multiple Finger Loss. Applied Sciences. 2021; 11(10):4464. https://doi.org/10.3390/app11104464
Chicago/Turabian StyleSrimaneepong, Viritpon, Artak Heboyan, Azeem Ul Yaqin Syed, Hai Anh Trinh, Pokpong Amornvit, and Dinesh Rokaya. 2021. "Recent Advances in Myoelectric Control for Finger Prostheses for Multiple Finger Loss" Applied Sciences 11, no. 10: 4464. https://doi.org/10.3390/app11104464
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.