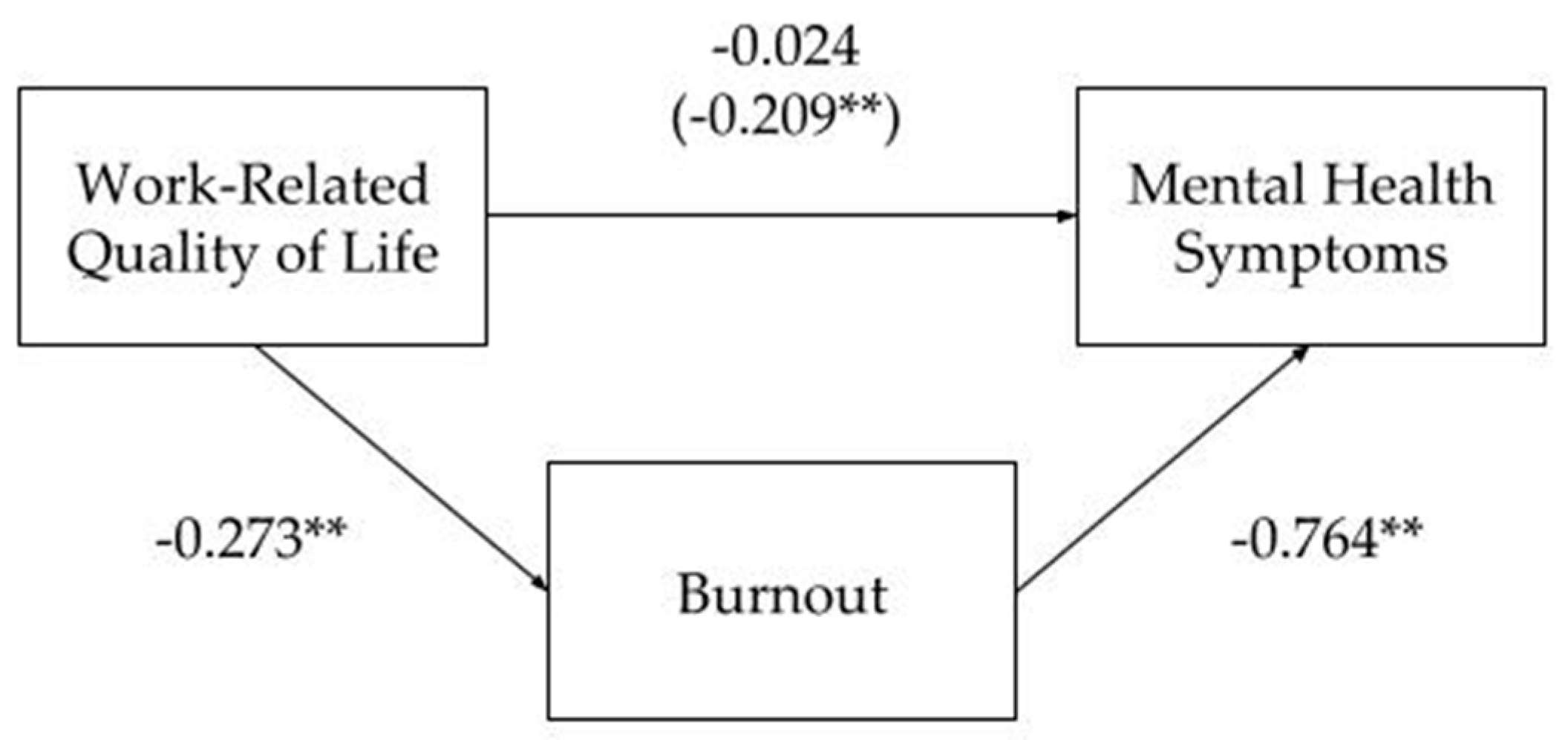
Mediating Effect of Burnout on the Association between Work-Related Quality of Life and Mental Health Symptoms

 ,
,  , , and
, , and 
Abstract
:1. Introduction
1.1. Burnout—Conceptualization/Assessment
1.2. WRQoL Implications and Burnout
1.3. Burnout Consequences and Mental Health Symptoms
1.4. Objectives
2. Materials and Methods
2.1. Measurement Instruments
2.2. Procedures
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Plaisier, I.; Beekman, A.T.F.; de Graaf, R.; Smit, J.; van Dyck, R.; Penninx, B. Work functioning in persons with depressive and anxiety disorders: The role of specific psychopathological characteristics. J. Affect. Disord. 2010, 125, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Schaufeli, W.B. Past performance and future perspectives of burnout research. SA J. Ind. Psychol. 2003, 29, 1–15. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Leiter, M.P.; Maslach, C. Burnout: 35 years of research and practice. Career Dev. Int. 2009, 14, 204–220. [Google Scholar] [CrossRef] [Green Version]
- Schaufeli, W.B.; Desart, S.; De Witte, H. Burnout assessment tool (Bat)—Development, validity, and reliability. Int. J. Environ. Res. Public Health 2020, 17, 9495. [Google Scholar] [CrossRef]
- Bresó, E.; Salanova, M.; Schaufeli, W.B. In search of the “third dimension” of burnout: Efficacy or inefficacy? Appl. Psychol. 2007, 56, 460–478. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; De Witte, H.; Desart, S. User Manual–Burnout Assessment Tool (BAT)–Version 2.0; KU Leuven: Leuven, Belgium, 2019. [Google Scholar]
- Ahmad, S. Paradigms of quality of work life. J. Hum. Values 2013, 19, 73–82. [Google Scholar] [CrossRef] [Green Version]
- Loscocco, K.A.; Roschelle, A.R. Influences on the quality of work and nonwork life: Two decades in review. J. Vocat. Behav. 1991, 39, 182–225. [Google Scholar] [CrossRef]
- Bhende, P.; Mekoth, N.; Ingalhalli, V.; Reddy, Y.V. Quality of Work Life and Work–Life Balance. J. Hum. Values 2020, 26, 256–265. [Google Scholar] [CrossRef]
- Sirgy, M.J.; Efraty, D.; Siegel, P.; Lee, D.J. A new measure of quality of work life (QWL) based on need satisfaction and spillover theories. Soc. Indic. Res. 2001, 55, 241–302. [Google Scholar] [CrossRef]
- Swamy, D.R.; Nanjundeswaraswamy, T.S.; Rashmi, S. Quality of Work Life: Scale Development and Validation. Int. J. Caring Sci. 2015, 8, 281–300. [Google Scholar] [CrossRef]
- Van Laar, D.; Edwards, J.A.; Easton, S. The Work-Related Quality of Life scale for healthcare workers. J. Adv. Nurs. 2007, 60, 325–333. [Google Scholar] [CrossRef]
- Wang, P.; Chu, P.; Wang, J.; Pan, R.; Sun, Y.; Yan, M.; Jiao, L.; Zhan, X.; Zhang, D. Association Between Job Stress and Organizational Commitment in Three Types of Chinese University Teachers: Mediating Effects of Job Burnout and Job Satisfaction. Front. Psychol. 2020, 11, 1–12. [Google Scholar] [CrossRef]
- Wu, F.; Ren, Z.; Wang, Q.; He, M.; Xiong, W.; Ma, G.; Fan, X.; Guo, X.; Liu, H.; Zhang, X. The relationship between job stress and job burnout: The mediating effects of perceived social support and job satisfaction. Psychol. Health Med. 2021, 26, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Pu, J.; Hou, H.; Ma, R.; Sang, J. The effect of psychological capital between work–family conflict and job burnout in Chinese university teachers: Testing for mediation and moderation. J. Health Psychol. 2016, 22, 1799–1807. [Google Scholar] [CrossRef] [PubMed]
- Kanten, S.; Sadullah, O. An Empirical Research on Relationship Quality of Work Life and Work Engagement. Procedia Soc. Behav. Sci. 2012, 62, 360–366. [Google Scholar] [CrossRef] [Green Version]
- Cheng, L.; Gan, Y. Psychological capital and occupational commitment of Chinese urban preschool teachers mediated by work-related quality of life. Soc. Behav. Personal. 2020, 48, e8905. [Google Scholar] [CrossRef]
- Alrawadieh, Z.; Cetin, G.; Dincer, M.Z.; Dincer, F.I. The impact of emotional dissonance on quality of work life and life satisfaction of tour guides. Serv. Ind. J. 2020, 40, 50–64. [Google Scholar] [CrossRef]
- Tuuli, P.; Karisalmi, S. Impact of working life quality on burnout. Exp. Aging Res. 1999, 25, 441–449. [Google Scholar] [CrossRef]
- Cetrano, G.; Tedeschi, F.; Rabbi, L.; Gosetti, G.; Lora, A.; Lamonaca, D.; Manthorpe, J.; Amaddeo, F. How are compassion fatigue, burnout, and compassion satisfaction affected by quality of working life? Findings from a survey of mental health staff in Italy. BMC Health Serv. Res. 2017, 17, 755. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.Q.; Lv, W.J.; Qian, R.L.; Zhang, Y.H. Job burnout and quality of working life among Chinese nurses: A cross-sectional study. J. Nurs. Manag. 2019, 27, 1835–1844. [Google Scholar] [CrossRef] [PubMed]
- Akar, H. The relationships between quality of work life, school alienation, burnout, affective commitment and organizational citizenship: A study on teachers. Eur. J. Educ. Res. 2018, 7, 169–181. [Google Scholar]
- Melamed, S.; Shirom, A.; Toker, S.; Berliner, S.; Shapira, I. Burnout and risk of cardiovascular disease: Evidence, possible causal paths, and promising research directions. Psychol. Bull. 2006, 132, 327–353. [Google Scholar] [CrossRef]
- Maslach, C.; Leiter, M.P. Understanding the burnout experience: Recent research and its implications for psychiatry. World Psychiatry 2016, 15, 103–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alarcon, G.M. A meta-analysis of burnout with job demands, resources, and attitudes. J. Vocat. Behav. 2011, 79, 549–562. [Google Scholar] [CrossRef]
- Kim, H.; Kao, D. A meta-analysis of turnover intention predictors among U.S. child welfare workers. Child. Youth Serv. Rev. 2014, 47, 214–223. [Google Scholar] [CrossRef]
- Ruotsalainen, J.H.; Verbeek, J.H.; Mariné, A.; Serra, C. Preventing occupational stress in healthcare workers. Cochrane Database Syst. Rev. 2015, 4. [Google Scholar] [CrossRef] [PubMed]
- Leitão, J.; Pereira, D.; Gonçalves, Â. Quality of work life and contribution to productivity: Assessing the moderator effects of burnout syndrome. Int. J. Environ. Res. Public Health 2021, 18, 2425. [Google Scholar] [CrossRef] [PubMed]
- Schaufeli, W.B.; Bakker, A.B. Job demands, job resources, and their relationship with burnout and engagement: A multi-sample study. J. Organ. Behav. 2004, 25, 293–315. [Google Scholar] [CrossRef] [Green Version]
- Ahola, K.; Väänänen, A.; Koskinen, A.; Kouvonen, A.; Shirom, A. Burnout as a predictor of all-cause mortality among industrial employees: A 10-year prospective register-linkage study. J. Psychosom. Res. 2010, 69, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Center, C.; Davis, M.R.; Detre, T.P.; Ford, D.E.; Hansbrough, W.B.; Hendin, H.; Laszlo, J.; Litts, D.A.; Mann, J.J.; Mansky, P.A.; et al. Confronting Depression and Suicide in Physicians: A Consensus Statement. J. Am. Med. Assoc. 2003, 289, 3161–3166. [Google Scholar] [CrossRef] [PubMed]
- Eurofound. Burnout in the Workplace: A Review of Data and Policy Responses in the EU; Issue October; 2018; Available online: http://eurofound.link/ef18047 (accessed on 31 March 2021).
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; 2013; DSM-V; Available online: https://doi-org.db29.linccweb.org/10.1176/appi.books.9780890425596.dsm02 (accessed on 31 March 2021).
- Bianchi, R.; Schonfeld, I.S.; Laurent, E. Burnout-depression overlap: A review. Clin. Psychol. Rev. 2015, 36, 28–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, A.H. Anxiety. In Encyclopedia of Psychology and Religion; Leeming, D.A., Ed.; Springer: Boston, MA, USA, 2014; pp. 95–99. [Google Scholar] [CrossRef]
- Koutsimani, P.; Montgomery, A.; Georganta, K. The relationship between burnout, depression, and anxiety: A systematic review and meta-analysis. Front. Psychol. 2019, 10, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Beer, L.T.; Schaufeli, W.B.; De Witte, H.; Hakanen, J.J.; Shimazu, A.; Glaser, J.; Seubert, C.; Bosak, J.; Sinval, J.; Rudnev, M. Measurement Invariance of the Burnout Assessment Tool (BAT) Across Seven Cross-National Representative Samples. Int. J. Environ. Res. Public Health 2020, 17, 5604. [Google Scholar] [CrossRef] [PubMed]
- Gomes, J.; Silva, C.; Cruz, A. Escala da Qualidade de Vida Relacionada com o Trabalho. In User Manual for the Work-Related Quality of Life (WRQoL) Scale: A Measure of Quality of Working Life; 2018; Available online: http://www.qowl.co.uk/researchers/Escala QVT.pdf (accessed on 31 March 2021).
- Nazaré, B.; Pereira, M.; Canavarro, M.C. Avaliação breve da psicossintomatologia: Análise fatorial confirmatória da versão portuguesa do Brief Symptom Inventory 18 (BSI 18). Anal. Psicol. 2017, 35, 213–230. [Google Scholar] [CrossRef] [Green Version]
- Ruiz-Fernández, M.D.; Pérez-García, E.; Ortega-Galán, Á.M. Quality of Life in Nursing Professionals: Burnout, Fatigue, and Compassion Satisfaction. Int. J. Environ. Res. Public Health 2020, 17, 1253. [Google Scholar] [CrossRef] [Green Version]
- Caponnetto, P.; Magro, R.; Inguscio, L.; Cannella, M.C. Quality of life, work motivation, burn-out and stress perceptions benefits of a stress management program by autogenic training for emergency room staff: A pilot study. Ment. Illn. 2018, 10, 67–70. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, K.; Muller Neff, D.; Pitman, S. Burnout in mental health professionals: A systematic review and meta-analysis of prevalence and determinants. Eur. Psychiatry 2018, 53, 74–99. [Google Scholar] [CrossRef]
- Guan, S.; Xiaerfuding, X.; Ning, L.; Lian, Y.; Jiang, Y.; Liu, J.; Ng, T.B. Effect of Job Strain on Job Burnout, Mental Fatigue and Chronic Diseases among Civil Servants in the Xinjiang Uygur Autonomous Region of China. Int. J. Environ. Res. Public Health 2017, 14, 872. [Google Scholar] [CrossRef] [Green Version]
- Farré, L.; Fawaz, Y.; Gonzalez, L.; Graves, J. How the COVID-19 Lockdown Affected Gender Inequality in Paid and Unpaid Work in Spain; IZA Discussion Paper Series; 2020; Available online: https://ssrn.com/abstract=3643198 (accessed on 31 March 2021).
- Reichelt, M.; Makovi, K.; Sargsyan, A. The impact of COVID-19 on gender inequality in the labor market and gender-role attitudes. Eur. Soc. 2020, 1–18. [Google Scholar] [CrossRef]
- Lyonette, C.; Crompton, R.; Wall, K. Gender, Occupational Class and Work–Life Conflict: A comparison between Britain and Portugal. Community Work Fam. 2007, 10, 283–308. [Google Scholar] [CrossRef]
- International Labour Organization. ILO Monitor: COVID-19 and the World of Work, 7th ed.; Updated Estimates and Analysis; 2021; Available online: https://www.ilo.org/brasilia/noticias/WCMS_767317/lang--pt/index.htm (accessed on 31 March 2021).
- Comisión Económica para América Latina y el Caribe. Mujeres Económicos Cambiantes. 2019. Available online: https://repositorio.cepal.org/bitstream/handle/11362/45032/S1900723_es.pdf?sequence=4&isAllowed=y (accessed on 31 March 2021).
- Lyttelton, T.; Zang, E.; Musick, K. Gender Differences in Telecommuting and Implications for Inequality at Home and Work. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Del Boca, D.; Oggero, N.; Profeta, P.; Rossi, M. Women’s and men’s work, housework and childcare, before and during COVID-19. Rev. Econ. Househ. 2020, 18, 1001–1017. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.P.; Martin, D.; Nagaria, Z.; Verceles, A.C.; Jobe, S.L.; Wickwire, E.M. Mental Health Consequences of Shift Work: An Updated Review. Curr. Psychiatry Rep. 2020, 22, 7. [Google Scholar] [CrossRef] [PubMed]
- Rivera, A.S.; Akanbi, M.; O’Dwyer, L.C.; McHugh, M. Shift work and long work hours and their association with chronic health conditions: A systematic review of systematic reviews with meta-analyses. PLoS ONE 2020, 15, e0231037. [Google Scholar] [CrossRef] [PubMed]
- Amâncio, L.; Santos, M.H. Gender Equality and Modernity in Portugal. An Analysis on the Obstacles to Gender Equality in Highly Qualified Professions. Soc. Sci. 2021, 10, 162. [Google Scholar] [CrossRef]
- Ungureanu, B.S.; Vladut, C.; Bende, F.; Sandru, V.; Tocia, C.; Turcu-Stiolica, R.-A.; Groza, A.; Balan, G.G.; Turcu-Stiolica, A. Impact of the COVID-19 Pandemic on Health-Related Quality of Life, Anxiety, and Training Among Young Gastroenterologists in Romania. Front. Psychol. 2020, 11. [Google Scholar] [CrossRef]
- Turcu-Stiolica, A.; Bogdan, M.; Subtirelu, M.-S.; Meca, A.-D.; Taerel, A.-E.; Iaru, I.; Kamusheva, M.; Petrova, G. Influence of COVID-19 on Health-Related Quality of Life and the Perception of Being Vaccinated to Prevent COVID-19: An Approach for Community Pharmacists from Romania and Bulgaria. J. Clin. Med. 2021, 10, 864. [Google Scholar] [CrossRef]
- Bartosiewicz, A.; Łuszczki, E.; Dereń, K. Personalized Nursing: How Life Satisfaction and Occupational Burnout Influence New Competences of Polish Nurses. J. Pers. Med. 2020, 10, 48. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| N | % | ||
|---|---|---|---|
| Gender | Women | 526 | 62.5 |
| Men | 315 | 37.5 | |
| Marital Status | Single | 383 | 45.6 |
| Married | 271 | 32.2 | |
| De facto union | 121 | 14.4 | |
| Divorced/Separated | 59 | 7 | |
| Widower | 7 | 0.8 | |
| Educational Attainment | Up to 12 years of school | 304 | 36.2 |
| Undergraduate degree | 240 | 28.5 | |
| Postgraduate degree | 297 | 35.3 | |
| Place of residence | Small rural | 131 | 15.6 |
| Big rural | 96 | 11.4 | |
| Small urban | 383 | 45.5 | |
| Big urban | 231 | 27.5 | |
| Socioeconomic Status | Low | 33 | 3.9 |
| Middle-Low | 178 | 21 | |
| Middle | 490 | 58.3 | |
| Middle-High | 137 | 16.3 | |
| High | 4 | 0.5 | |
| Professional Status | Working student | 98 | 11.7 |
| Self-employed | 115 | 13.7 | |
| Employed | 628 | 74.6 | |
| Shift work | Yes | 170 | 20.2 |
| No | 671 | 79.8 | |
| Nature of the Organization | Public | 316 | 37.6 |
| Private | 461 | 54.8 | |
| Other | 64 | 7.6 | |
| Sector of Activity | Primary (agriculture, feedstock, fishing, etc.) | 32 | 3.8 |
| Secondary (industry) | 106 | 12.6 | |
| Tertiary (commerce, services, education, etc.) | 703 | 83.6 |
| Gender | M(SD) | t(df) | p | ||
|---|---|---|---|---|---|
| Burnout | Exhaustion | Men | 2.47(0.68) | −4.847(756) | 0.000 ** |
| Women | 2.70(0.61) | ||||
| Mental distance | Men | 1.81(0.75) | −363(752) | 0.717 | |
| Women | 1.83(0.69) | ||||
| Emotional impairment | Men | 2.21(0.70) | −2.169(755) | 0.030 * | |
| Women | 2.31(0.60) | ||||
| Cognitive impairment | Men | 2.15(0.72) | −4.173(761) | 0.000 ** | |
| Women | 2.36(0.67) | ||||
| Overall Burnout | Men | 2.16(0.60) | −3.505(763) | 0.000 ** | |
| Women | 2.30(0.51) | ||||
| Overall WRQoL | Men | 3.61(0.97) | 2.390(749) | 0.017 ** | |
| Women | 3.44(0.96) | ||||
| Mental Health | Somatization Symptoms | Men | 0.44(0.56) | −3.882(698) | 0.000 ** |
| Women | 0.62(0.62) | ||||
| Depression Symptoms | Men | 0.78(0.84) | −1.759(696) | 0.079 | |
| Women | 0.88(0.75) | ||||
| Anxiety Symptoms | Men | 0.75(0.67) | −3.974(697) | 0.000 ** | |
| Women | 0.96(0.70) | ||||
| Overall Mental Health Symptoms | Men | 0.66(0.61) | −3.484(698) | 0.001 * | |
| Women | 0.82(0.61) |
| Shift Work | M(SD) | t(df) | p | ||
|---|---|---|---|---|---|
| Burnout | Exhaustion | Yes | 2.67(0.70) | 1.132(773) | 0.258 |
| No | 2.60(0.64) | ||||
| Mental distance | Yes | 1.89(0.81) | 1.098(769) | 0.273 | |
| No | 1.82(0.79) | ||||
| Emotional impairment | Yes | 2.27(0.69) | −0.069(772) | 0.945 | |
| No | 2.27(0.63) | ||||
| Cognitive impairment | Yes | 2.34(0.79) | 1.014(778) | 0.311 | |
| No | 2.27(0.68) | ||||
| Overall Burnout | Yes | 2.29(0.61) | 1.031(780) | 0.303 | |
| No | 2.24(0.54) | ||||
| Overall WRQoL | Yes | 3.38(1.02) | −1.688(766) | 0.092 | |
| No | 3.53(0.95) | ||||
| Mental Health | Somatization Symptoms | Yes | 0.74(0.70) | 4.131(708) | 0.000 ** |
| No | 0.51(0.56) | ||||
| Depression Symptoms | Yes | 1.01(0.85) | 2.878(706) | 0.004 * | |
| No | 0.80(0.77) | ||||
| Anxiety Symptoms | Yes | 1.06(0.81) | 3.544(707) | 0.000 ** | |
| No | 0.84(0.66) | ||||
| Overall Mental Health Symptoms | Yes | 0.94(0.72) | 3.905(708) | 0.000 ** | |
| No | 0.71(0.58) |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1-Exhaustion | ||||||||||
| 2-Mental distance | 0.545 ** | |||||||||
| 3-Emotional impairment | 0.588 ** | 0.505 ** | ||||||||
| 4-Cognitive impairment | 0.602 ** | 0.491 ** | 0.562 ** | |||||||
| 5-Overall Burnout | 0.836 ** | 0.791 ** | 0.807 ** | 0.822 ** | ||||||
| 6-Overall WRQoL | −0.369 ** | −0.529 ** | −0.286 ** | −0.282 ** | −0.450 ** | |||||
| 7-Somatization Symptoms | 0.464 ** | 0.293 ** | 0.362 ** | 0.460 ** | 0.483 ** | −0.188 ** | ||||
| 8-Depression Symptoms | 0.589 ** | 0.562 ** | 0.521 ** | 0.642 ** | 0.711 ** | −0.428 ** | 0.580 ** | |||
| 9-Anxiety Symptoms | 0.564 ** | 0.413 ** | 0.495 ** | 0.655 ** | 0.653 ** | −0.309 ** | 0.700 ** | 0.766 ** | ||
| 10-Overall Mental Health Symptoms | 0.610 ** | 0.483 ** | 0.525 ** | 0.662 ** | 0.700 ** | −0.359 ** | 0.833 ** | 0.900 ** | 0.928 ** |
| Model I | Model II | Model III | |||||||
|---|---|---|---|---|---|---|---|---|---|
| B | SE B | β | B | SE B | β | B | SE B | β | |
| Age | −0.006 | 0.002 | −0.112 * | −0.005 | 0.002 | −0.091 * | −0.004 | 0.001 | −0.074 * |
| Gender | 0.172 | 0.048 | 0.136 ** | 0.142 | 0.046 | 0.112 * | 0.031 | 0.034 | 0.025 |
| Workload | 0.001 | 0.002 | 0.014 | 0.000 | 0.002 | 0.003 | −0.001 | 0.001 | −0.017 |
| Shift | −0.195 | 0.061 | −0.124 * | −0.179 | 0.058 | −0.115 * | −0.147 | 0.042 | −0.094 * |
| WRQoL | −0.227 | 0.024 | −0.349 ** | −0.046 | 0.021 | −0.071 * | |||
| Exhaustion | 0.239 | 0.036 | 0.253 ** | ||||||
| Mental distance | 0.049 | 0.031 | 0.057 | ||||||
| Emotional impairment | 0.056 | 0.035 | 0.059 | ||||||
| Cognitive impairment | 0.372 | 0.032 | 0.427 ** | ||||||
| 0.054 | 0.174 | 0.560 | |||||||
| F | 9.059 ** | 26.860 ** | 89.399 ** | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pereira, H.; Feher, G.; Tibold, A.; Costa, V.; Monteiro, S.; Esgalhado, G. Mediating Effect of Burnout on the Association between Work-Related Quality of Life and Mental Health Symptoms. Brain Sci. 2021, 11, 813. https://doi.org/10.3390/brainsci11060813
Pereira H, Feher G, Tibold A, Costa V, Monteiro S, Esgalhado G. Mediating Effect of Burnout on the Association between Work-Related Quality of Life and Mental Health Symptoms. Brain Sciences. 2021; 11(6):813. https://doi.org/10.3390/brainsci11060813
Chicago/Turabian StylePereira, Henrique, Gergely Feher, Antal Tibold, Vítor Costa, Samuel Monteiro, and Graça Esgalhado. 2021. "Mediating Effect of Burnout on the Association between Work-Related Quality of Life and Mental Health Symptoms" Brain Sciences 11, no. 6: 813. https://doi.org/10.3390/brainsci11060813