New Therapeutics in HER2-Positive Advanced Breast Cancer: Towards a Change in Clinical Practices?

 ,
, 
Abstract
:1. Introduction
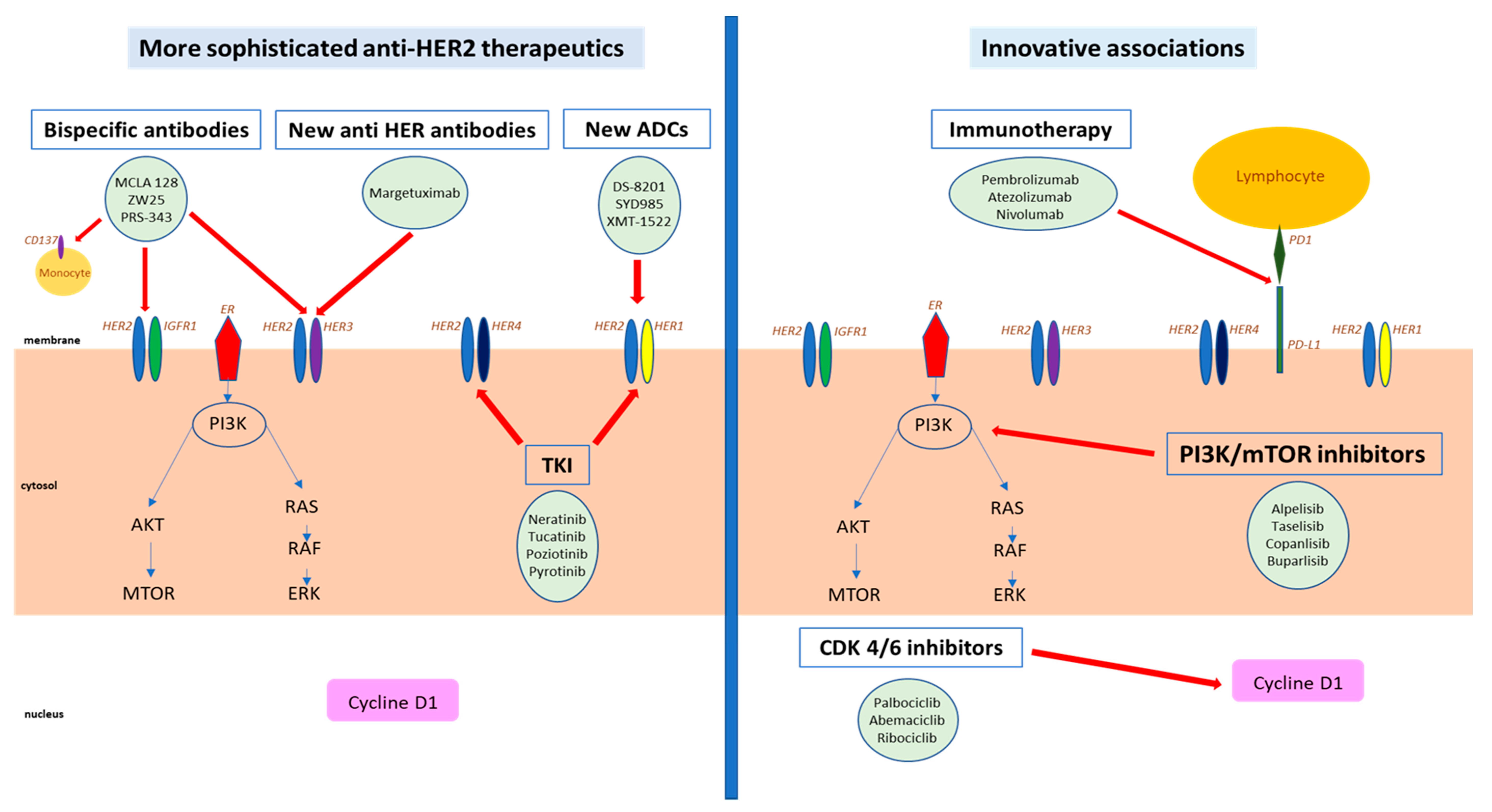
- The drugs that directly target HER2, include novel anti-HER antibodies characterized with an increased affinity, antibody-drug conjugates (ADC), bispecific antibodies, as well as more potent or more specific HER2 tyrosine kinase inhibitors (TKI), and targeted radio-immunotherapy.
- The drugs that indirectly target HER2 include novel therapeutics modulating HER2-connected pathways, which may synergize with direct anti-HER2 targeting through innovative associations, such as immune check point inhibitors (ICIs), cell cycle inhibitors, and PI3K inhibitors.
2. Novel Anti-HER2 Antibodies
2.1. Antibody-Drug Conjugates
2.1.1. Trastuzumab-Deruxtecan
Mechanism of Action
Clinical Outcomes
2.1.2. Trastuzumab Duocarmazine
Mechanism of Action
Clinical Outcomes
2.1.3. Other Antibody-Drug Conjugates
2.2. Margetuximab (MGAH22)
2.2.1. Mechanism of Action
2.2.2. Clinical Outcomes
2.3. Bispecific Antibodies
2.3.1. Zenocutuzumab (MCLA 128)
Mechanism of Action
Clinical Outcomes
- HER2-positive MBC failing 2–4 prior HER2 therapies (including T-DM1): doublet with MCLA-128 and trastuzumab, or triplet with MCLA-128, trastuzumab, and vinorelbine.
- HR+/HER2-low expression MBC failing ≥1 prior endocrine therapy + CDK4-6 inhibitor: MCLA-128 and endocrine therapy.
2.3.2. Azymetric (ZW25)
Mechanism of Action
Clinical Outcomes
- First-in-human, three-part trial: ZW25 alone and combined with selected chemotherapy agents (capecitabine, vinorelbine, or paclitaxel) in patients with HER2-expressing MBC (cohort 4–6) (NCT02892123).
- Phase II trial: ZW25 with palbociclib plus fulvestrant in patients with HER2-positive/HR-positive ABC (NCT04224272)
- Phase I/II trial: ZW25 in combination with docetaxel in patient with HER2-positive BC, tislelizumab and chemotherapy in patients with HER2+ gastroesophageal adenocarcinoma (NCT04276493).
2.3.3. PRS-343
Mechanism of Action
Clinical Outcomes
2.3.4. Other Bispecific Antibodies
2.4. More Potent or More Specific HER2 TKI
2.4.1. Neratinib
Mechanism of Action
Clinical Outcomes
2.4.2. Tucatinib (ONT-380)
Mechanism of Action
Clinical Outcomes
2.4.3. Pyrotinib
Mechanism of Action
Clinical Outcomes
2.4.4. Poziotinib (NOV120101)
Mechanism of Action
Clinical Outcomes
2.5. Targeted Radio-Immunotherapy
2.5.1. Mechanism of Action
2.5.2. Clinical Outcomes
3. Innovative Associations Co-Targeting HER2 and Connected Pathways
3.1. Immunotherapy
3.1.1. Rational for Inhibiting Immune Checkpoint in HER2-Positive
3.1.2. Clinical Outcome
Pembrolizumab
Atezolizumab
Nivolumab
3.2. Cell Cycle Inhibitors
3.2.1. Rational for Inhibiting Cell Cycle via CDK4/6 Inhibitors in HER2-Positive BC
3.2.2. Clinical Outcomes
3.3. PI3K/mTOR Inhibitors
3.3.1. Rational for Targeting the PI3K/AKT/mTOR Pathway in HER2-Positive BC
3.3.2. Clinical Outcomes
mTOR Inhibitors
PI3K Inhibitors
4. Perspective of Integration of Novel Anti-HER2 Therapeutics in Clinical Practice
- The changing landscape in systemic treatment at the early stage, since it may increasingly incorporate pertuzumab and trastuzumab emtansine, both being major components of therapeutic management in the advanced setting, with documented major overall survival gain. Thus, pertuzumab-trastuzumab combo, which improves pathological complete response rate in the neoadjuvant setting [100], was recently confirmed to increase disease-free survival in node-positive disease, whatever the expression of hormone receptors, when administered in the adjuvant setting [101]. In addition, trastuzumab emtansine, when used in the post-neoadjuvant setting in the presence of residual invasive disease, increased significantly survival outcome. Accordingly, those patients relapsing after being exposed to these drugs may require alternative therapeutic algorithm, and potential early introduction of most recent drugs with efficacy after pertuzumab and trastuzumab emtansine exposure.
- The clinical presentation of the disease balanced with the toxicity profile of emerging drugs. Thus, because of its outstanding activity but also its potential for significant chemo-like toxicities, including potentially severe pulmonary toxicity, trastuzumab-deruxtecan could be predominantly proposed to patients with aggressive diseases but keeping a good performance status with a satisfactory respiratory function. In contrast, tucatinib in combination with trastuzumab and capecitabine could be first offered to more fragile patients and/or with more indolent diseases. In addition, regarding to the highly significant improvement in OS for patients with brain metastases, this combination may be preferred in this subgroup. Even though the neratinib-capecitabine combination may have significant activity in CNS disease, the high level of digestive toxicity, notably diarrheas, and the marginal clinical benefit registered to date, clearly make it an inferior option to consider in this setting.
- The evaluation of available or emerging biomarkers. While additional molecular information might better orient prescription in a near future, the presence of HER2 overexpression/amplification remains the only validated biomarker for efficacy of anti-HER2 therapeutics. Thus, the levels of HER2 mRNA or protein did not predict efficacy of either dual blockade or trastuzumab emtansine, but was identified as a prognostic factor, a lower HER2 expression being associated with worse outcome [102]. In addition, the presence of heterogeneity in HER2 expression was recently associated with lower efficacy of trastuzumab emtansine [103,104]. However, both of these features might be less relevant for predicting efficacy of novel ADCs, in which a bystander effect is suspected and activity in a low-HER2 context is demonstrated [105]. Another potential important biomarker in HER2-positive ABC is the expression of hormone receptors, identifying the so-called “triple-positive” breast cancer. This luminal HER2-positive subtype, possibly better approximated by PAM50 gene expression signature, might be particularly sensitive to endocrine therapy-based with or without CDK4/6 inhibitors approaches [106,107]. Other molecular alterations with potential therapeutic interest include those associated with PI3K pathway, including PIK3CA mutations and/or PTEN loss and/or AKT1 mutation, which might guide the future use of PI3K/mTOR/AKT inhibitors in this subtype [93]. Finally, PD-L1 expression as well as presence of TILs could identify HER2-positive ABC with potential sensitivity to ICIs [78,79].
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Owens, M.A.; Horten, B.C.; Da Silva, M.M. HER2 amplification ratios by fluorescence in situ hybridization and correlation with immunohistochemistry in a cohort of 6556, cancer tissues. Clin. Breast Cancer 2004, 5, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Baselga, J.; Cortés, J.; Kim, S.-B.; Im, S.-A.; Hegg, R.; Im, Y.-H. Pertuzumab plus Trastuzumab plus Docetaxel for Metastatic Breast Cancer. N. Engl. J. Med. 2012, 366, 109–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swain, S.M.; Kim, S.-B.; Cortés, J.; Ro, J.; Semiglazov, V.; Campone, M. Pertuzumab, trastuzumab, and docetaxel for HER2-Positive metastatic breast cancer (CLEOPATRA study): Overall survival results from a randomised, Double-Blind, Placebo-Controlled, phase 3 study. Lancet Oncol. 2013, 14, 461–471. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, F.; Senkus, E.; Costa, A.; Papadopoulos, E.; Aapro, M.; André, F. 4th ESO–ESMO International Consensus Guidelines for Advanced Breast Cancer (ABC 4). Ann. Oncol. 2018, 29, 1634–1657. [Google Scholar] [CrossRef] [PubMed]
- Blackwell, K.L.; Miles, D.; Gianni, L.; Krop, I.E.; Welslau, M.; Baselga, J. Primary results from EMILIA, a phase III study of trastuzumab emtansine (T-DM1) versus capecitabine (X) and lapatinib (L) in HER2-positive locally advanced or metastatic breast cancer (MBC) previously treated with trastuzumab (T) and a taxane. J. Clin. Oncol. 2012, 30, LBA1. [Google Scholar] [CrossRef]
- Alley, S.C.; Okeley, N.M.; Senter, P.D. Antibody–Drug conjugates: Targeted drug delivery for cancer. Curr. Opin. Chem. Biol. 2010, 14, 529–537. [Google Scholar] [CrossRef]
- Sievers, E.L.; Senter, P.D. Antibody-Drug conjugates in cancer therapy. Annu. Rev. Med. 2013, 64, 15–29. [Google Scholar] [CrossRef]
- FDA Approval: Ado-Trastuzumab Emtansine for the Treatment of Patients with HER2-Positive Metastatic Breast Cancer|Clinical Cancer Research [Internet]. Available online: https://clincancerres.aacrjournals.org/content/20/17/4436.short (accessed on 12 April 2020).
- Beck, A.; Goetsch, L.; Dumontet, C.; Corvaïa, N. Strategies and challenges for the next generation of Antibody–Drug conjugates. Nat. Rev. Drug Discov. 2017, 16, 315–337. [Google Scholar] [CrossRef]
- Iwata, H.; Tamura, K.; Doi, T.; Tsurutani, J.; Modi, S.; Park, H. Trastuzumab deruxtecan (DS-8201a) in subjects with HER2-expressing solid tumors: Long-Term results of a large phase 1 study with multiple expansion cohorts. J. Clin. Oncol. 2018, 20, 2501. [Google Scholar] [CrossRef]
- Lewis, P.G.D.; Li, G.; Dugger, D.L.; Crocker, L.M.; Parsons, K.L.; Mai, E. Targeting HER2-Positive breast cancer with trastuzumab-DM1, an Antibody-Cytotoxic drug conjugate. Cancer Res. 2008, 15, 9280–9290. [Google Scholar] [CrossRef] [Green Version]
- Doi, T.; Shitara, K.; Naito, Y.; Shimomura, A.; Fujiwara, Y.; Yonemori, K. Safety, pharmacokinetics, and antitumour activity of trastuzumab deruxtecan (DS-8201), a HER2-Targeting Antibody–Drug conjugate, in patients with advanced breast and gastric or Gastro-Oesophageal tumours: A phase 1 Dose-Escalation study. Lancet Oncol. 2017, 18, 1512–1522. [Google Scholar] [CrossRef]
- Tamura, K.; Tsurutani, J.; Takahashi, S.; Iwata, H.; Krop, I.E.; Redfern, C. Trastuzumab deruxtecan (DS-8201a) in patients with advanced HER2-Positive breast cancer previously treated with trastuzumab emtansine: A Dose-Expansion, phase 1 study. Lancet Oncol. 2019, 20, 816–826. [Google Scholar] [CrossRef]
- Keam, S.J. Trastuzumab deruxtecan: First approval. Drugs 2020, 80, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Modi, S.; Saura, C.; Yamashita, T.; Park, Y.H.; Kim, S.-B.; Tamura, K. Trastuzumab deruxtecan in previously treated Her2-Positive breast cancer. N. Engl. J. Med. 2020, 382, 610–621. [Google Scholar] [CrossRef] [PubMed]
- André, F.; Shahidi, J.; Lee, C.; Wang, K.; Krop, I.E. Abstract OT2-07-02: Trastuzumab deruxtecan (DS-8201a) vs. investigator’s choice of treatment in subjects with HER2-Positive, unresectable and/or metastatic breast cancer who previously received T-DM1: A randomized, phase 3 study. Cancer Res. 2019, 15, OT2-07. [Google Scholar]
- Verma, S.; Shahidi, J.; Lee, C.; Wang, K.; Cortes, J. Abstract OT2-07-03: Trastuzumab deruxtecan (DS-8201a) vs. Ado-Trastuzumab emtansine (T-DM1) for subjects with HER2-Positive, unresectable and/or metastatic breast cancer who previously received trastuzumab and a taxane: A phase 3, randomized study. Cancer Res. 2019, 15, OT2-07. [Google Scholar]
- Bartsch, R.; Bergen, E. ASCO 2018: Highlights in HER2-positive metastatic breast cancer. Memo–Mag. Eur. Med. Oncol. 2018, 11, 280–283. [Google Scholar] [CrossRef] [Green Version]
- Herpen, C.M.V.; Banerji, U.; Mommers, E.C.; Koper, N.P.; Goedings, P.; Lopez, J. 333 Phase I Dose-Escalation trial with the DNA-Alkylating Anti-HER2 Antibody-Drug conjugate SYD985. Eur. J. Cancer 2015, 51, S65. [Google Scholar] [CrossRef]
- Saura, C.; Thistlethwaite, F.; Banerji, U.; Lord, S.; Moreno, V.; MacPherson, I. A phase I expansion cohorts study of SYD985 in heavily pretreated patients with HER2-Positive or HER2-Low metastatic breast cancer. J. Clin. Oncol. 2018, 36, 1014. [Google Scholar] [CrossRef]
- Banerji, U.; van Herpen, C.M.L.; Saura, C.; Thistlethwaite, F.; Lord, S.; Moreno, V. Trastuzumab duocarmazine in locally advanced and metastatic solid tumours and HER2-Expressing breast cancer: A phase 1 Dose-Escalation and Dose-Expansion study. Lancet Oncol. 2019, 20, 1124–1135. [Google Scholar] [CrossRef] [Green Version]
- Yurkovetskiy, A.; Gumerov, D.; Ter-Ovanesyan, E.; Conlon, P.; Devit, M.; Bu, C. Abstract 48: Non-Clinical pharmacokinetics of XMT-1522, a HER2 targeting Auristatin-Based antibody drug conjugate. Cancer Res. 2017, 77, 48. [Google Scholar]
- Barok, M.; Le Joncour, V.; Martins, A.; Isola, J.; Salmikangas, M.; Laakkonen, P. ARX788, a novel Anti-HER2 Antibody-Drug conjugate, shows Anti-Tumor effects in preclinical models of trastuzumab Emtansine-Resistant HER2-Positive breast cancer and gastric cancer. Cancer Lett. 2020, 473, 156–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, X.; Zhang, J.; Ji, D.; Xia, G.; Ji, Y.; Xiong, G. Abstract P1-18-16: A phase 1 study of ARX788, a HER2-targeting Antibody-Drug conjugate, in patients with metastatic HER2-Positive breast cancer. Cancer Res. 2020, 80, P1-18-16. [Google Scholar]
- Rajasekaran, N.; Chester, C.; Yonezawa, A.; Zhao, X.; Kohrt, H.E. Enhancement of Antibody-Dependent cell mediated cytotoxicity: A new era in cancer treatment. Immunotargets Ther. 2015, 4, 91–100. [Google Scholar]
- Iannello, A.; Ahmad, A. Role of Antibody-Dependent Cell-Mediated cytotoxicity in the efficacy of therapeutic Anti-Cancer monoclonal antibodies. Cancer Metastasis Rev. 2005, 24, 487–499. [Google Scholar] [CrossRef]
- Musolino, A.; Naldi, N.; Bortesi, B.; Pezzuolo, D.; Capelletti, M.; Missale, G. Immunoglobulin G fragment C receptor polymorphisms and clinical efficacy of Trastuzumab-Based therapy in patients with HER-2/neu-positive metastatic breast cancer. J. Clin. Oncol. 2008, 26, 1789–1796. [Google Scholar] [CrossRef]
- Nordstrom, J.L.; Gorlatov, S.; Zhang, W.; Yang, Y.; Huang, L.; Burke, S. Anti-Tumor activity and toxicokinetics analysis of MGAH22, an Anti-HER2 monoclonal antibody with enhanced Fcγ receptor binding properties. Breast Cancer Res. 2011, 13, R123. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Yang, Y.; Burns, R.; Li, J.; Li, H.; Gorlatov, S. Abstract 1538: Margetuximab mediates greater Fc-Dependent Anti-Tumor activities than trastuzumab or pertuzumab in vitro. Cancer Res. 2019, 79, 1538. [Google Scholar]
- Bang, Y.; Giaccone, G.; Im, S.; Oh, D.; Bauer, T.; Nordstrom, J. First-In-Human phase 1 study of margetuximab (MGAH22), an Fc-Modified chimeric monoclonal antibody, in patients with HER2-Positive advanced solid tumors. Ann. Oncol. 2017, 28, 855–861. [Google Scholar] [CrossRef]
- Rugo, H.S.; Im, S.-A.; Wright, G.L.S.; Escriva-de-Romani, S.; DeLaurentiis, M.; Cortes, J. SOPHIA primary analysis: A phase 3 (P3) study of margetuximab (M) + chemotherapy (C) versus trastuzumab (T) + C in patients (pts) with HER2+ metastatic (met) breast cancer (MBC) after prior anti-HER2 therapies (Tx). J. Clin. Oncol. 2019, 37, 1000. [Google Scholar] [CrossRef]
- Rugo, H.S.; Im, S.-A.; Cardoso, F.; Cortes, J.; Curigliano, G.; Pegram, M.D. Abstract GS1-02: Phase 3 SOPHIA study of margetuximab + chemotherapy vs. trastuzumab + chemotherapy in patients with HER2+ metastatic breast cancer after prior anti-HER2 therapies: Second interim overall survival analysis. Cancer Res. 2020, 80, GS1-02. [Google Scholar]
- Geuijen, C.; Rovers, E.; Gallenne, T.; Maussang-Detaille, D.; Kramer, A.; Nieuwenhuizen, N. Abstract LB-261: Mechanism of action of MCLA-128, a humanized bispecific IgG1 antibody targeting the HER2:HER3 heterodimer. Cancer Res. 2015, 75, LB-261. [Google Scholar]
- Alsina, M.; Boni, V.; Schellens, J.H.M.; Moreno, V.; Bol, K.; Westendorp, M. First-In-Human phase 1/2 study of MCLA-128, a full length IgG1 bispecific antibody targeting HER2 and HER3: Final phase 1 data and preliminary activity in HER2+ metastatic breast cancer (MBC). J. Clin. Oncol. 2017, 35, 2522. [Google Scholar] [CrossRef]
- Weisser, N.; Wickman, G.; Davies, R.; Rowse, G. Abstract 31: Preclinical development of a novel biparatopic HER2 antibody with activity in low to high HER2 expressing cancers. Cancer Res. 2017, 77, 31. [Google Scholar]
- Meric-Bernstam, F.; Beeram, M.; Mayordomo, J.I.; Hanna, D.L.; Ajani, J.A.; Blum, M.M.A. Single agent activity of ZW25, a HER2-Targeted bispecific antibody, in heavily pretreated HER2-Expressing cancers. J. Clin. Oncol. 2018, 36, 2500. [Google Scholar] [CrossRef]
- Hinner, M.J.; Aiba, R.-S.B.; Schlosser, C.; Wiedenmann, A.; Allersdorfer, A.; Matschiner, G. Abstract 556: Costimulatory T-Cell engagement by the HER2/CD137 bispecific PRS-343 leads to strong antitumor effect in humanized mouse model. Cancer Res. 2016, 76, 556. [Google Scholar]
- Hinner, M.J.; Aiba, R.S.B.; Jaquin, T.J.; Berger, S.; Dürr, M.C.; Schlosser, C. Tumor-Localized costimulatory T-Cell engagement by the 4-1BB/HER2 bispecific Antibody-Anticalin fusion PRS-343. Clin. Cancer Res. 2019, 25, 5878–5889. [Google Scholar] [CrossRef] [Green Version]
- Rius, R.I.; Vicario, R.; Morancho, B.; Morales, C.B.; Arenas, E.J.; Herter, S. p95HER2-T cell bispecific antibody for breast cancer treatment. Sci. Transl. Med. 2018, 10, 461. [Google Scholar] [CrossRef] [Green Version]
- Segovia-Mendoza, M.; González-González, M.E.; Barrera, D.; Díaz, L.; García-Becerra, R. Efficacy and mechanism of action of the tyrosine kinase inhibitors gefitinib, lapatinib and neratinib in the treatment of HER2-positive breast cancer: Preclinical and clinical evidence. Am. J. Cancer Res. 2015, 5, 2531–2561. [Google Scholar]
- Chan, A.; Delaloge, S.; Holmes, F.A.; Moy, B.; Iwata, H.; Harvey, V.J. Neratinib after Trastuzumab-Based adjuvant therapy in patients with HER2-Positive breast cancer (ExteNET): A multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2016, 17, 367–377. [Google Scholar] [CrossRef]
- Singh, H.; Walker, A.J.; Amiri-Kordestani, L.; Cheng, J.; Tang, S.; Balcazar, P. U.S. food and drug administration approval: Neratinib for the extended adjuvant treatment of Early-Stage HER2-Positive breast cancer. Clin. Cancer Res. 2018, 24, 486–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhillon, S. Neratinib in Early-Stage breast Cancer: A profile of its use in the E.U. Clin. Drug Investig. 2019, 39, 221–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leo, C.P.; Hentschel, B.; Szucs, T.D.; Leo, C. FDA and EMA approvals of new breast cancer drugs—A comparative regulatory analysis. Cancer 2020, 12, 437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.W.; Liu, M.C.; Yee, D. Adaptive Randomization of Neratinib in Early Breast Cancer. N. Engl. J. Med. 2016, 375, 1591–1594. [Google Scholar] [CrossRef] [PubMed]
- Burstein, H.J.; Sun, Y.; Dirix, L.Y.; Jiang, Z.; Paridaens, R.; Tan, A.R. Neratinib, an irreversible ErbB receptor tyrosine kinase inhibitor, in patients with advanced ErbB2-positive breast cancer. J. Clin. Oncol. 2010, 28, 1301–1307. [Google Scholar] [CrossRef] [PubMed]
- Awada, A.; Colomer, R.; Inoue, K.; Bondarenko, I.; Badwe, R.A.; Demetriou, G. Neratinib plus paclitaxel vs. trastuzumab plus paclitaxel in previously untreated metastatic ERBB2-Positive breast cancer: The NEfERT-T randomized clinical trial. JAMA Oncol. 2016, 2, 1557–1564. [Google Scholar] [CrossRef] [PubMed]
- Saura, C.; Garcia-Saenz, J.A.; Xu, B.; Harb, W.; Moroose, R.; Pluard, T. Safety and efficacy of Neratinib in combination with capecitabine in patients with metastatic human epidermal growth factor receptor 2–Positive breast cancer. J. Clin. Oncol. 2014, 32, 3626–3633. [Google Scholar] [CrossRef]
- Saura, C.; Oliveira, M.; Feng, Y.-H.; Dai, M.-S.; Hurvitz, S.A.; Kim, S.-B. Neratinib + capecitabine versus lapatinib + capecitabine in patients with HER2+ metastatic breast cancer previously treated with ≥ 2 HER2-directed regimens: Findings from the multinational, randomized, phase III NALA trial. J. Clin. Oncol. 2019, 37, 1002. [Google Scholar] [CrossRef]
- FDA Approves Neratinib/Capecitabine for Pretreated Patients with Metastatic HER2-Positive Breast Cancer–The ASCO Post [Internet]. Available online: https://www.ascopost.com/issues/march-10-2020/fda-approves-neratinibcapecitabine-for-pretreated-patients-with-metastatic-her2-positive-breast-cancer/ (accessed on 12 April 2020).
- Freedman, R.A.; Gelman, R.S.; Wefel, J.S.; Melisko, M.E.; Hess, K.R.; Connolly, R.M. Translational breast cancer research consortium (TBCRC) 022: A phase II Trial of Neratinib for patients with human epidermal growth factor receptor 2–Positive breast cancer and brain metastases. J. Clin. Oncol. 2016, 34, 945–952. [Google Scholar] [CrossRef]
- Freedman, R.A.; Gelman, R.S.; Anders, C.K.; Melisko, M.E.; Parsons, H.A.; Cropp, A.M. TBCRC 022: A phase II trial of neratinib and capecitabine for patients with human epidermal growth factor receptor 2–Positive breast cancer and brain metastases. J. Clin. Oncol. 2019, 37, 1081–1089. [Google Scholar] [CrossRef]
- Abraham, J.; Puhalla, S.; Sikov, W.M.; Montero, A.J.; Salkeni, M.A.; Razaq, W. NSABP FB-10: Phase Ib Dose-Escalation trial evaluating trastuzumab emtansine (T-DM1) with neratinib (N) in women with metastatic HER2+ breast cancer (MBC). J. Clin. Oncol. 2018, 36, 1027. [Google Scholar] [CrossRef]
- Pheneger, T.; Bouhana, K.; Anderson, D.; Garrus, J.; Ahrendt, K.; Allen, S. Abstract #1795: In vitro and in vivo activity of ARRY-380: A potent, small molecule inhibitor of ErbB2. Cancer Res. 2009, 69, 1795. [Google Scholar]
- Lee, P.; Napier, C.; Garrus, J.; Avrustkaya, A.; White, A.; Winkler, J. Abstract #5581: In vivo activity of ARRY-380: A potent, small molecule inhibitor of ErbB-2 in combination with trastuzumab or docetaxel in a BT-474 human breast carcinoma xenograft model. Cancer Res. 2009, 69, 5581. [Google Scholar]
- Dinkel, V.; Anderson, D.; Winski, S.; Winkler, J.; Koch, K.; Lee, P.A. Abstract 852: ARRY-380, a potent, small molecule inhibitor of ErbB2, increases survival in intracranial ErbB2+ xenograft models in mice. Cancer Res. 2012, 72, 852. [Google Scholar]
- Moulder, S.L.; Borges, V.F.; Baetz, T.; Mcspadden, T.; Fernetich, G.; Murthy, R.K. Phase I study of ONT-380, a HER2 Inhibitor, in Patients with HER2+-advanced solid tumors, with an expansion cohort in HER2+ metastatic breast cancer (MBC). Clin. Cancer Res. 2017, 23, 3529–3536. [Google Scholar] [CrossRef] [Green Version]
- Murthy, R.; Borges, V.F.; Conlin, A.; Chaves, J.; Chamberlain, M.; Gray, T. Tucatinib with capecitabine and trastuzumab in advanced HER2-Positive metastatic breast cancer with and without brain metastases: A Non-Randomised, Open-Label, phase 1b study. Lancet Oncol. 2018, 19, 880–888. [Google Scholar] [CrossRef]
- Murthy, R.K.; Loi, S.; Okines, A.; Paplomata, E.; Hamilton, E.; Hurvitz, S.A. Tucatinib, trastuzumab, and capecitabine for HER2-Positive metastatic breast cancer. N. Engl. J. Med. 2020, 382, 597–609. [Google Scholar] [CrossRef]
- Borges, V.F.; Ferrario, C.; Aucoin, N.; Falkson, C.; Khan, Q.; Krop, I. Tucatinib combined with Ado-Trastuzumab emtansine in advanced ERBB2/HER2-Positive metastatic breast cancer: A phase 1b clinical trial. JAMA Oncol. 2018, 4, 1214–1220. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Yang, C.; Wan, H.; Zhang, G.; Feng, J.; Zhang, L. Discovery and development of pyrotinib: A novel irreversible EGFR/HER2 dual tyrosine kinase inhibitor with favorable safety profiles for the treatment of breast cancer. Eur. J. Pharm. Sci. 2017, 110, 51–61. [Google Scholar] [CrossRef]
- Ma, F.; Li, Q.; Chen, S.; Zhu, W.; Fan, Y.; Wang, J. Phase I study and biomarker analysis of pyrotinib, a novel irreversible Pan-ErbB receptor tyrosine kinase inhibitor, in patients with human epidermal growth factor receptor 2–Positive metastatic breast cancer. J. Clin. Oncol. 2017, 35, 3105–3112. [Google Scholar] [CrossRef]
- Li, Q.; Guan, X.; Chen, S.; Yi, Z.; Lan, B.; Xing, P. Safety, efficacy, and biomarker analysis of pyrotinib in combination with capecitabine in HER2-Positive metastatic breast cancer patients: A phase I clinical trial. Clin. Cancer Res. 2019, 25, 5212–5220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, F.; Ouyang, Q.; Li, W.; Jiang, Z.; Tong, Z.; Liu, Y. Pyrotinib or lapatinib combined with capecitabine in HER2-Positive metastatic breast cancer with prior taxanes, anthracyclines, and/or trastuzumab: A randomized, phase II study. J. Clin. Oncol. 2019, 37, 2610–2619. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Z.; Yan, M.; Hu, X.; Zhang, Q.; Ouyang, Q.; Feng, J. Pyrotinib combined with capecitabine in women with HER2+ metastatic breast cancer previously treated with trastuzumab and taxanes: A randomized phase III study. J. Clin. Oncol. 2019, 37, 1001. [Google Scholar] [CrossRef]
- Kim, H.J.; Kim, H.-P.; Yoon, Y.-K.; Kim, M.-S.; Lee, G.-S.; Han, S.-W. Antitumor activity of HM781-36B, a pan-HER tyrosine kinase inhibitor, in HER2-Amplified breast cancer cells. Anticancer Drugs 2012, 23, 288–297. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.M.; Lee, K.-W.; Oh, D.-Y.; Lee, J.-S.; Im, S.-A.; Kim, D.-W. Phase 1 studies of poziotinib, an irreversible Pan-HER tyrosine kinase inhibitor in patients with advanced solid tumors. Cancer Res. Treat. Off. J. Korean Cancer Assoc. 2018, 50, 835–842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, Y.H.; Lee, K.-H.; Sohn, J.H.; Lee, K.S.; Jung, K.H.; Kim, J.-H. A phase II trial of the Pan-HER inhibitor poziotinib, in patients with HER2-Positive metastatic breast cancer who had received at least two prior HER2-Directed regimens: Results of the NOV120101-203 trial. Int. J. Cancer 2018, 143, 3240–3247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wickstroem, K.; Karlsson, J.; Ellingsen, C.; Cruciani, V.; Kristian, A.; Hagemann, U.B. Synergistic effect of a HER2 targeted Thorium-227 conjugate in combination with olaparib in a BRCA2 Deficient xenograft model. Pharmaceuticals 2019, 12, 155. [Google Scholar] [CrossRef] [Green Version]
- Meredith, R.; Torgue, J.; Shen, S.; Fisher, D.R.; Banaga, E.; Bunch, P. Dose escalation and dosimetry Of First-In-Human α radioimmunotherapy with 212Pb-TCMC-trastuzumab. J. Nucl. Med. 2014, 55, 1636–1642. [Google Scholar] [CrossRef] [Green Version]
- Karlsson, J.; Hagemann, U.B.; Schatz, C.; Grant, D.; Ellingsen, C.; Kristian, A.; Mihaylova, D.; Uran, S.R.; Suominen, M.; Bjerke, R.M.; et al. Abstract 5857: HER2-Targeted thorium-227 conjugate (HER2-TTC): Efficacy in a HER2 positive orthotopic bone model. Tumor Biol. 2017, 77, 5857. [Google Scholar]
- Karlsson, J.; Hagemann, U.B.; Schatz, C.; Grant, D.; Kristian, A.; Ellingsen, C.; Mihaylova, D.; Geraudie, S.; Indrevoll, B.; Wirnitzer, U.; et al. Abstract 5859: HER2-Targeted thorium-227 conjugate (HER2-TTC): Efficacy in preclinical models of trastuzumab and T-DM1 resistance. Tumor Biol. 2017, 77, 5859. [Google Scholar]
- Savas, P.; Salgado, R.; Denkert, C.; Sotiriou, C.; Darcy, P.K.; Smyth, M.J.; Loi, S. Clinical relevance of host immunity in breast cancer: From TILs to the clinic. Nat. Rev. Clin. Oncol. 2015, 13, 228–241. [Google Scholar] [CrossRef] [PubMed]
- Cortazar, P.; Zhang, L.; Untch, M.; Mehta, K.; Costantino, J.P.; Wolmark, N.; Bonnefoi, H.; Cameron, D.; Gianni, L.; Valagussa, P.; et al. Pathological complete response and long-term clinical benefit in breast cancer: The CTNeoBC pooled analysis. Lancet 2014, 384, 164–172. [Google Scholar] [CrossRef] [Green Version]
- Clynes, R.A.; Towers, T.L.; Presta, L.G.; Ravetch, J.V. Inhibitory Fc receptors modulate in vivo cytoxicity against tumor targets. Nat. Med. 2000, 6, 443–446. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Jiang, Z.; Mortenson, E.D.; Deng, L.; Radkevich-Brown, O.; Yang, X. The therapeutic effect of Anti-HER2/neu antibody depends on both innate and adaptive immunity. Cancer Cell 2010, 18, 160–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hou, Y.; Nitta, H.; Wei, L.; Banks, P.M.; Lustberg, M.; Wesolowski, R.; Ramaswamy, B.; Parwani, A.V.; Li, Z. PD-L1 expression and CD8-positive T cells are associated with favorable survival in HER2-positive invasive breast cancer. Breast J. 2018, 24, 911–919. [Google Scholar] [CrossRef]
- Loi, S.; Giobbie-Hurder, A.; Gombos, A.; Bachelot, T.; Hui, R.; Curigliano, G.; Campone, M.; Biganzoli, L.; Bonnefoi, H.; Jerusalem, G.; et al. Pembrolizumab plus trastuzumab in Trastuzumab-Resistant, advanced, HER2-Positive breast cancer (PANACEA): A Single-Arm, multicentre, phase 1b–2 trial. Lancet Oncol. 2019, 20, 371–382. [Google Scholar] [CrossRef]
- Emens, L.; Esteva, F.; Beresford, M.; Saura, C.; De Laurentiis, M.; Kim, S.-B.; Im, S.-A.; Patre, M.; Wang, Y.; Mani, A.; et al. Abstract PD3-01: Results from KATE2, a randomized phase 2 study of atezolizumab (atezo)+trastuzumab emtansine (T-DM1) vs placebo (pbo) + T-DM1 in previously treated HER2 + advanced breast cancer (BC). Poster Discuss. Abstr. 2019, 79, PD3-01. [Google Scholar]
- Iancu, G.; Vasile, D.; Iancu, R.C.; DaviŢoiu, D.V. “Triple positive” breast cancer—A novel category? Rom. J. Morphol. Embryol. Rev. Roum. Morphol. Embryol. 2017, 58, 21–26. [Google Scholar]
- Finn, R.S.; Dering, J.; Conklin, D.; Kalous, O.; Cohen, D.J.; Desai, A.J.; Ginther, C.; Atefi, M.; Chen, I.; Fowst, C.; et al. PD 0332991, a selective cyclin D kinase 4/6 inhibitor, preferentially inhibits proliferation of luminal estrogen receptor-positive human breast cancer cell lines in vitro. Breast Cancer Res. 2009, 11, R77. [Google Scholar] [CrossRef] [Green Version]
- Landis, M.W.; Pawlyk, B.S.; Li, T.; Sicinski, P.; Hinds, P.W. Cyclin D1-dependent kinase activity in murine development and mammary tumorigenesis. Cancer Cell 2006, 9, 13–22. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, N.; Conklin, D.; Beckmann, R.; Luo, T.; Chau, K.; Thomas, J.; Mc Nulty, A.; Marchal, C.; Kalous, O.; Von Euw, E.; et al. Preclinical activity of abemaciclib alone or in combination with antimitotic and targeted therapies in breast cancer. Mol. Cancer 2018, 17, 897–907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patnaik, A.; Rosen, L.S.; Tolaney, S.M.; Tolcher, A.W.; Goldman, J.W.; Gandhi, L.; Papadopoulos, K.P.; Beeram, M.; Rasco, D.W.; Hilton, J.F.; et al. Efficacy and safety of abemaciclib, an inhibitor of CDK4 and CDK6, for patients with breast cancer, Non-Small cell lung cancer, and other solid tumors. Cancer Discov. 2016, 6, 740–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tolaney, S.M.; Wardley, A.M.; Zambelli, S.; Hilton, J.F.; Troso-Sandoval, T.A.; Ricci, F.; Im, S.-A.; Kim, S.-B.; Johnston, S.R.; Chan, A.; et al. Abemaciclib plus trastuzumab with or without fulvestrant versus trastuzumab plus Standard-Of-Care chemotherapy in women with hormone receptor-positive, HER2-Positive advanced breast cancer (monarcHER): A randomised, open-label, phase 2 trial. Lancet Oncol. 2020, 21, 763–775. [Google Scholar] [CrossRef]
- Metzger, O.; Mandrekar, S.; Loibl, S.; Mundhenke, C.; Seiler, S.; Valagussa, P. Abstract OT3-02-07: Patina: A randomized, open label, phase III trial to evaluate the efficacy and safety of palbociclib + anti-HER2 therapy + endocrine therapy (ET) vs. anti-HER2 therapy + ET after induction treatment for hormone receptor positive (HR+)/HER2-positive metastatic breast cancer (MBC). Cancer Res. 2019, 79, OT3-02. [Google Scholar]
- Villagrasa, P.; Prat, A.; Oliveira, M.; De La Pena, L.; Gonzalez, X.; Cortés, J.; Simon, S.P.; Rios, J.; Canes, J.; Ciruelos, E. SOLTI-1303 PATRICIA: A phase II study of palbociclib and trastuzumab (HR+ with or without letrozole) in Trastuzumab-Pretreated, postmenopausal patients with HER2-Positive metastatic breast cancer. J. Clin. Oncol. 2018, 36, TPS1101. [Google Scholar] [CrossRef]
- Shagisultanova, E.; Chalasani, P.; Brown-Glaberman, U.A.; Gradishar, W.J.; Brenner, A.J.; Stopeck, A.; Gao, D.; Mcspadden, T.; Kabos, P.; Borges, V.F.; et al. Tucatinib, palbociclib, and letrozole in HR+/HER2+ metastatic breast cancer: Report of phase IB safety cohort. J. Clin. Oncol. 2019, 37, 1029. [Google Scholar] [CrossRef]
- Andre, F.; Campone, M.; O’Regan, R.; Manlius, C.; Massacesi, C.; Tarek, S.; Mukhopadhyay, P.; Soria, J.-C.; Naughton, M.; Hurvitz, S.A. Phase I study of everolimus plus weekly paclitaxel and trastuzumab in patients with metastatic breast cancer pretreated with trastuzumab. J. Clin. Oncol. 2010, 28, 5110–5115. [Google Scholar] [CrossRef]
- Jerusalem, G.; Fasolo, A.; Dieras, V.; Cardoso, F.; Bergh, J.; Vittori, L.; Zhang, Y.; Massacesi, C.; Sahmoud, T.; Gianni, L. Phase I trial of oral mTOR inhibitor everolimus in combination with trastuzumab and vinorelbine in pre-treated patients with HER2-overexpressing metastatic breast cancer. Breast Cancer Res. Treat. 2010, 125, 447–455. [Google Scholar] [CrossRef]
- Andre, F.; O’Regan, R.; Özgüroglu, M.; Toi, M.; Xu, B.; Jerusalem, G.; Masuda, N.; Wilks, S.; Arena, F.; Isaacs, C.; et al. Everolimus for women with Trastuzumab-Resistant, HER2-Positive, advanced breast cancer (BOLERO-3): A randomised, double-blind, Placebo-Controlled phase 3 trial. Lancet Oncol. 2014, 15, 580–591. [Google Scholar] [CrossRef]
- Hurvitz, S.A.; Andre, F.; Jiang, Z.; Shao, Z.; Mano, M.S.; Neciosup, S.P.; Tseng, L.-M.; Zhang, Q.; Shen, K.; Liu, D.; et al. Combination of everolimus with trastuzumab plus paclitaxel as first-line treatment for patients with HER2-positive advanced breast cancer (BOLERO-1): A phase 3, randomised, Double-Blind, multicentre trial. Lancet Oncol. 2015, 16, 816–829. [Google Scholar] [CrossRef] [Green Version]
- Andre, F.; Hurvitz, S.; Fasolo, A.; Tseng, L.-M.; Jerusalem, G.; Wilks, S.; O’Regan, R.; Isaacs, C.; Toi, M.; Burris, H.A.; et al. Molecular alterations and everolimus efficacy in human epidermal growth factor receptor 2–Overexpressing metastatic breast cancers: Combined exploratory biomarker analysis from BOLERO-1 and BOLERO-3. J. Clin. Oncol. 2016, 34, 2115–2124. [Google Scholar] [CrossRef] [PubMed]
- Guerin, M.; Rezai, K.; Isambert, N.; Campone, M.; Autret, A.; Pakradouni, J.; Provansal, M.; Camerlo, J.; Sabatier, R.; Bertucci, F.; et al. PIKHER2: A phase IB study evaluating buparlisib in combination with lapatinib in Trastuzumab-Resistant HER2-Positive advanced breast cancer. Eur. J. Cancer 2017, 86, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Krop, I.E.; Saura, C.; Ahnert, J.R.; Becerra, C.; Britten, C.D.; Isakoff, S.J.; Demanse, D.; Hackl, W.; Quadt, C.; Silva, A.P.; et al. A phase I/IB Dose-Escalation study of BEZ235 in combination with trastuzumab in patients with PI3-kinase or PTEN altered HER2+ metastatic breast cancer. J. Clin. Oncol. 2012, 30, 508. [Google Scholar] [CrossRef]
- Jain, S.; Santa-Maria, C.A.; Rademaker, A.; Giles, F.J.; Cristofanilli, M.; Gradishar, W.J. Phase I study of alpelisib (BYL-719) and T-DM1 in HER2-Positive metastatic breast cancer after trastuzumab and taxane therapy. J. Clin. Oncol. 2017, 35, 1026. [Google Scholar] [CrossRef]
- Shah, P.D.; Chandarlapaty, S.; Dickler, M.N.; Ulaner, G.; Zamora, S.J.; Sterlin, V.; Iasonos, A.; Coughlin, C.M.; Morozov, A.; Ero, J.; et al. Phase I study of LJM716, BYL719, and trastuzumab in patients (pts) with HER2-amplified (HER2+) metastatic breast cancer (MBC). J. Clin. Oncol. 2015, 33, 590. [Google Scholar] [CrossRef]
- Keegan, N.M.; Walshe, J.M.; Toomey, S.; Gullo, G.; Kennedy, M.J.; Bulger, K.N.; McCaffrey, J.; Kelly, C.M.; Crown, J.; Egan, K.; et al. A phase Ib trial of copanlisib and tratuzumab in pretreated recurrent or metastatic HER2-positive breast cancer “PantHER”. J. Clin. Oncol. 2018, 36, 1036. [Google Scholar] [CrossRef]
- Piccart-Gebhart, M.J.; Aftimos, P.G.; Duhoux, F.P.; Wildiers, H.; Isambert, N.; Campone, M. B-PRECISE-01 study: A phase Ib trial of MEN1611, a PI3K Inhibitor, combined with trastuzumab ± fulvestrant for the treatment of HER2-Positive advanced or metastatic breast cancer. J. Clin. Oncol. 2019, 37, TPS1101. [Google Scholar] [CrossRef]
- Gianni, L.; Pienkowski, T.; Im, Y.-H.; Roman, L.; Tseng, L.-M.; Liu, M.-C.; Lluch, A.; Staroslawska, E.; De La Haba-Rodriguez, J.; Im, S.-A.; et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): A randomised multicentre, Open-Label, phase 2 trial. Lancet Oncol. 2012, 13, 25–32. [Google Scholar] [CrossRef]
- Piccart, M.; Procter, M.; Fumagalli, D.; De Azambuja, E.; Clark, E.; Ewer, M.S.; Restuccia, E.; Jerusalem, G.; Dent, S.; Reaby, L.; et al. Abstract GS1-04: Interim overall survival analysis of APHINITY (BIG 4-11): A randomized multicenter, Double-Blind, Placebo-Controlled trial comparing chemotherapy plus trastuzumab plus pertuzumab versus chemotherapy plus trastuzumab plus placebo as adjuvant therapy in patients with operable HER2-Positive early breast cancer. Gen. Sess. Abstr. 2020, 80, GS1-04. [Google Scholar]
- Baselga, J.; Cortés, J.; Im, S.-A.; Clark, E.; Ross, G.; Kiermaier, A.; Swain, S.M. Biomarker analyses in CLEOPATRA: A Phase III, Placebo-Controlled Study of pertuzumab in human epidermal growth factor receptor 2–Positive, First-Line metastatic breast cancer. J. Clin. Oncol. 2014, 32, 3753–3761. [Google Scholar] [CrossRef]
- Filho, O.M.; Viale, G.; Trippa, L.; Li, T.; Yardley, D.A.; Mayer, I.A.; Abramson, V.G.; Arteaga, C.L.; Spring, L.; Waks, A.G.; et al. HER2 heterogeneity as a predictor of response to neoadjuvant T-DM1 plus pertuzumab: Results from a prospective clinical trial. J. Clin. Oncol. 2019, 37, 502. [Google Scholar] [CrossRef]
- Perez, E.A.; de Haas, S.L.; Eiermann, W.; Barrios, C.H.; Toi, M.; Im, Y.-H. Relationship between tumor biomarkers and efficacy in MARIANNE, a phase III study of trastuzumab emtansine ± pertuzumab versus trastuzumab plus taxane in HER2-Positive advanced breast cancer. BMC Cancer 2019, 19, 517. [Google Scholar]
- Modi, S.; Park, H.; Murthy, R.K.; Iwata, H.; Tamura, K.; Tsurutani, J.; Moreno-Aspitia, A.; Doi, T.; Sagara, Y.; Redfern, C.; et al. Antitumor activity and safety of trastuzumab deruxtecan in patients with HER2-Low-Expressing advanced breast cancer: Results from a phase Ib study. J. Clin. Oncol. 2020, JCO1902318. [Google Scholar] [CrossRef] [PubMed]
- Prat, A.; Carey, L.A.; Adamo, B.; Vidal, M.; Tabernero, J.; Cortés, J.; Parker, J.S.; Perou, C.M.; Baselga, J. Molecular features and survival outcomes of the intrinsic subtypes within HER2-Positive breast cancer. J. Natl. Cancer Inst. 2014, 106. [Google Scholar] [CrossRef] [Green Version]
- Ciruelos, E.; Villagrasa, P.; Oliveira, M.; Pernas, S.; Cortes, J.; Vazquez, S. Abstract OT2-02-06: Palbociclib in combination with trastuzumab and endocrine therapy (ET) versus treatment of physician’s choice (TPC) in metastatic HER2-positive and hormone receptor-positive (HER2+/HR+) breast cancer with PAM50 luminal intrinsic subtype (SOLTI-1303, II): A Multi-Center, randomized, Open-Label, phase II trial. Cancer Res. 2020, 80, OT2-02. [Google Scholar]


{kind=link}
| Trial | Phase | Population | Arms | Primary Endpoint |
|---|---|---|---|---|
| DESTINY-Breast 02 [16] (NCT03523585) | III | HER2+ ABC pretreated with T-DM1 | T-DXd vs. Investigator’s choice (capecitabine with trastuzumab or lapatinib) | PFS, OS, ORR, CBR, duration of response |
| DESTINY-Breast 03 [17] (NCT03529110) | III | HER2 + MBC previously treated with trastuzumab and taxane | T-DXd vs. T-DM1 | PFS, OS, ORR, CBR, duration of response |
| DAISY (NCT04132960) | II | HER2 high and low HER2 ABC | monotherapy T-DXd | Best ORR in three cohorts according HER2 expression. Biomarkers analysis to characterize response and resistance to therapy. |
| Agent | Antibody | Cytotoxic payload | Trial | Phase | Population |
|---|---|---|---|---|---|
| SYD985 [19] | Vic-Trastuzumab | Duocarmazine (irreversible alkylation of the DNA in tumor cells) | NCT02277717 [20] | I | MBC regardless HER2 and ER statutes, in the 3rd ou 4th line with HER2 targeting |
| NCT03262935 TULIP | III | HER2-positive ABC beyond the second line therapy | |||
| XMT-1522 [22] | XMT-1519 (novel anti-HER2 monoclonal antibody) | 10–15 molecules of the payload AF-HPA, an auristatin-derivative (anti tubulin). | NCT02952729 | Ib | ABC and other advanced tumors expressing HER2 |
| ARX788 [23] | Anti HER2 Mab | Amberstatin269 or AS269 (a potent cytotoxic tubulin inhibitor) | NCT02512237 [24] | I | Two cohorts with different ABC HER+ expansion cohorts, and one cohort with advanced HER+ gastric cancer. |
| NCT03255070 | I | HER+ MBC or gastric cancer. | |||
| DHES0815A | Trastuzumab | PBD-MA (alkylator) | NCT03451162 | I | Heavily pretreated HER2-positive ABC |
| Trial | Phase | Population | Experimental Arm | Standard Arm | Status |
|---|---|---|---|---|---|
| NCT04034589 | II | HR+/HER2+ MBC | Pyrotinib + Fulvestrant | NA | Recruiting |
| NCT03691051 | II | HER2+ MBC with brain metastases | Pyrotinib + Capecitabine | NA | Not yet recruiting |
| NCT03997539 | II R* | HER2+ ABC previously treated by Trastuzumab-Based Therapy | Pyrotinib + Vinorelbine | Treatment of physician’s choice | Not yet recruiting |
| NCT04246502 | II R | First-line treatment of HER2+ MBC | Pyrotinib + Capecitabine | Capecitabine, trastuzumab, and pertuzumab | Not yet recruiting |
| NCT03876587 | II | First-line Treatment of HER2+ MBC | Pyrotinib + Docetaxel | NA | Not yet recruiting |
| NCT03993964 | II | HER2+ MBC | SHR6390 + Pyrotinib SHR6390 is a novel small molecule inhibitor specifically targeting the CDK4/6 pathway | Not yet recruiting | |
| NCT03863223 | III R | First-line treatment of HER2+ MBC | Pyrotinib + Trastuzumab and Docetaxel | Placebo + trastuzumab and docetaxel | Recruiting |
| NCT04033172 | II | HR+/HER2+ MBC | Pyrotinib + Fulvestrant | NA* | Recruiting |
| NCT04001621 | II | Trastuzumab-resistant HER2+ ABC | Pyrotinib + Capecitabine | NA | Recruiting |
| NCT03910712 | II R | First-line Treatment of HER2+/HR+ MBC | Pyrotinib + Trastuzumab + Aromatase inhibitors | trastuzumab + Aromatase inhibitors | Not yet recruiting |
| TKI | Randomized Trial | Phase | n | Arms | ORR | 1-year PFS | HR |
|---|---|---|---|---|---|---|---|
| Neratinib | NALA trial [49] (NCT01808573) | III | 621 | Neratinib + Capecitabine vs. Lapatinib + Capecitabine | 33% vs. 27% | 29% vs. 15% | 0.76; 95% CI, 0.63–0.93; p = 0.0059 |
| Tucatinib | HER2CLIMB [59] (NCT02614794). | III | 603 | Capecitabine + trastutuzumab +/− Tucatinib | 33% vs. 12% | 40% vs. 22.8% | 0.54; 95% CI, 0.42–0.71; p < 0.001 |
| Pyrotinib | PHENIX [65] (NCT02973737) | III | 279 | Capecitabine-Pyrotinib vs. Capecitabine-placebo | 68.6% vs. 16.0% | 0.18; 95% CI, 0.13–0.26; p < 0.001 | |
| (NCT02422199) [64] | II | 128 | Capecitabine-Pyrotinib vs. Capecitabine-Lapatinib | 78% vs. 57% | 18 vs. 7% | 0.36; 95% CI, 0.23–0.58; p = 0. 001 |
| Trial | Phase | Population | Regimens | Primary Endpoint |
|---|---|---|---|---|
| PATINA [86] (NCT02947685) | III Randomized | HR+/HER2+ MBC after induction treatment | anti-HER2 therapy ± Palbociclib | PFS |
| PATRICIA [87] (NCT02448420) | II | previously treated HR+/HER2+ ABC | Palbociclib + Trastuzumab ± Létrozole | PFS |
| (NCT 02657343) | II | HER+ MBC not responded to standard treatment | Ribociclib + Trastuzumab vs T-DM1 ± Fulvestrant | MTD and/or recommended Phase II dose CBR |
| (NCT03054363) [88] | Ib/II | first or second line of therapy in HR+/HER+ MBC | Tucatinib + Palbociclib, + Letrozole | adverse events PFS |
| Drug | Trial | Phase | Regimens | Population | Activity | Toxicities |
|---|---|---|---|---|---|---|
| Alpelisib | NCT02038010 [96] | I | Alpelisib + T-DM1 | HER2+ MBC Progressing on prior trastuzumab and taxane-based therapy | Median PFS (months): No prior T-DM1 (n = 11): 6 Prior T-DM1 (n = 6): 4.3 | Hyperglycemia (53%), fatigue (53%), nausea (35%), and rash (47%) |
| NCT02167854 [97] | I | LJM716 + alpelisib + Trastuzumab | HER2+ MBC | SD in 5/6 evaluable patients | Significant toxicities (and worst grades): diarrhea, hyperglycemia hypokalemia, mucositis, transaminitis | |
| NCT04208178 | III | Alpelisib + Trastuzumab + Pertuzumab | Maintenance therapy in patients with HER2+ ABC with a PIK3CA mutation | unknown | unknown | |
| Taselisib | NCT02390427 | Ib | Arm A: Taselisib + Trastuzumab + T-DM1 Arm B: Taselisib + T-DM1 + Pertuzumab Arm C: Taselisib + Pertuzumab + Trastuzumab Arm D: Taselisib + Pertuzumab + Trastuzumab + Paclitaxel | HER2+ ABC | unknown | unknown |
| Copanlisib | NCT02705859 [98] | Ib/2 | Copanlisib + Trastuzumab | HER2+ MBC | SD in 9/12 patients. Six patients continued treatment ≥ 16 weeks | G3 hypertension (33%), G3 infections (36%), hepatic toxicities |
| MEN1611 | NCT03767335 [99] | Ib | MEN1611 + Trastuzumab +/− Fulvestrant | PIK3CA mutated HER2+ ABC progressed to anti-HER2 based therapy | unknown | unknown |
| Class | Treatment | ORR | PFS (months) |
|---|---|---|---|
| Antibody-drug conjugates | T-DXd | 60.9% | 16.4 |
| SYD985 | 33% | 7.6 | |
| Margetuximab | Margetuximab + chemotherapy | 25.2% | 5.8 |
| Bispecific antibodies | MCLA 128 | 77.7% | unknown |
| ZW25 | 54% | unknown | |
| HER2 TKI | Neratinib + Capecitabine | 33% | 8.5 |
| Tucatinib + Capecitabine + Trastutuzumab | 33% | 7.8 | |
| Tucatinib + T-DM1 | 47% | 8.2 | |
| Pyrotinib + Capecitabine | 68.6% | 11.1 | |
| Poziotinib | 75.5% | 4 | |
| ICIs | Pembrolizumab | 25% in the PD-L1 positive cohort | 2.7 |
| Atezolizumab + T-DM1 | no benefit | ||
| Nivolumab | unknown | unknown | |
| Cell cycle inhibitors | Abemaciclib + Trastuzumab +/− Fulvestrant | 35.4% | 8.3 |
| mTOR inhibitors | Everolimus + Trastuzumab + Vinorelbine | 7 | |
| Alpelisib + T-DM1 | 6 if no prior T-DM1 4.3 if prior T-DM1 | ||
| LJM716 + Alpelisib +Trastuzumab | 5/6 | unknown | |
| Copanlisib + Trastuzumab | 9/12 | unknown |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mezni, E.; Vicier, C.; Guerin, M.; Sabatier, R.; Bertucci, F.; Gonçalves, A. New Therapeutics in HER2-Positive Advanced Breast Cancer: Towards a Change in Clinical Practices? Cancers 2020, 12, 1573. https://doi.org/10.3390/cancers12061573
Mezni E, Vicier C, Guerin M, Sabatier R, Bertucci F, Gonçalves A. New Therapeutics in HER2-Positive Advanced Breast Cancer: Towards a Change in Clinical Practices? Cancers. 2020; 12(6):1573. https://doi.org/10.3390/cancers12061573
Chicago/Turabian StyleMezni, Essia, Cécile Vicier, Mathilde Guerin, Renaud Sabatier, François Bertucci, and Anthony Gonçalves. 2020. "New Therapeutics in HER2-Positive Advanced Breast Cancer: Towards a Change in Clinical Practices?" Cancers 12, no. 6: 1573. https://doi.org/10.3390/cancers12061573