
Dosimetric Analysis of the Short-Ranged Particle Emitter 161Tb for Radionuclide Therapy of Metastatic Prostate Cancer

 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
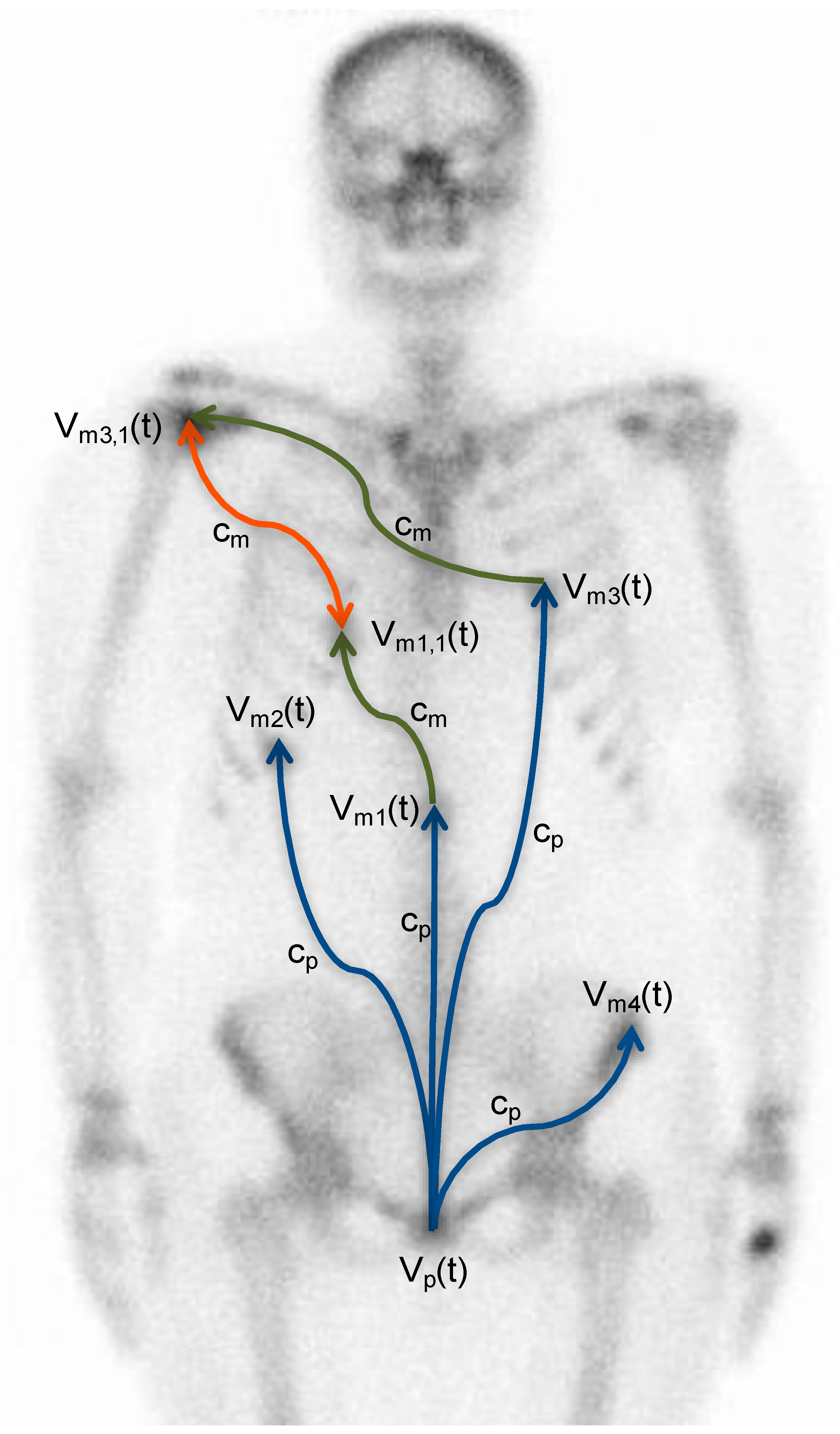
2.1. The Metastatic Dissemination Model
2.2. The Tumor Growth Model
2.3. Absorbed Tumor Doses
2.4. Biological Effective Dose and Radiosensitivity
2.5. The Metastatic Control Probability Model
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Bander, N.H.; Trabulsi, E.J.; Kostakoglu, L.; Yao, D.; Vallabhajosula, S.; Smith-Jones, P.; Joyce, M.A.; Milowsky, M.; Nanus, D.M.; Goldsmith, S.J. Targeting metastatic prostate cancer with radiolabeled monoclonal antibody J591 to the extracellular domain of prostate specific membrane antigen. J. Urol. 2003, 170, 1717–1721. [Google Scholar] [CrossRef] [PubMed]
- Von Eyben, F.E.; Roviello, G.; Kiljunen, T.; Uprimny, C.; Virgolini, I.; Kairemo, K.; Joensuu, T. Third-line treatment and 177Lu-PSMA radioligand therapy of metastatic castration-resistant prostate cancer: A systematic review. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 496–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baum, R.P.; Kulkarni, H.R.; Schuchardt, C.; Singh, A.; Wirtz, M.; Wiessalla, S.; Schottelius, M.; Müller, D.; Klette, I.; Wester, H.J. 177Lu-Labeled Prostate-Specific Membrane Antigen Radioligand Therapy of Metastatic Castration-Resistant Prostate Cancer: Safety and Efficacy. J. Nucl. Med. 2016, 57, 1006–1013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okamoto, S.; Thieme, A.; Allmann, J.; D’Alessandria, C.; Maurer, T.; Retz, M.; Tauber, R.; Heck, M.M.; Wester, H.J.; Tamaki, N.; et al. Radiation Dosimetry for 177Lu-PSMA I&T in Metastatic Castration-Resistant Prostate Cancer: Absorbed Dose in Normal Organs and Tumor Lesions. J. Nucl. Med. 2017, 58, 445–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zechmann, C.M.; Afshar-Oromieh, A.; Armor, T.; Stubbs, J.B.; Mier, W.; Hadaschik, B.; Joyal, J.; Kopka, K.; Debus, J.; Babich, J.W.; et al. Radiation dosimetry and first therapy results with a 124I/ 131I-labeled small molecule (MIP-1095) targeting PSMA for prostate cancer therapy. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1280–1292. [Google Scholar] [CrossRef] [Green Version]
- Kratochwil, C.; Bruchertseifer, F.; Rathke, H.; Bronzel, M.; Apostolidis, C.; Weichert, W.; Haberkorn, U.; Giesel, F.L.; Morgenstern, A. Targeted alpha-Therapy of Metastatic Castration-Resistant Prostate Cancer with 225Ac-PSMA-617: Dosimetry Estimate and Empiric Dose Finding. J. Nucl. Med. 2017, 58, 1624–1631. [Google Scholar] [CrossRef] [Green Version]
- Kratochwil, C.; Schmidt, K.; Afshar-Oromieh, A.; Bruchertseifer, F.; Rathke, H.; Morgenstern, A.; Haberkorn, U.; Giesel, F.L. Targeted alpha therapy of mCRPC: Dosimetry estimate of 213Bismuth-PSMA-617. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 31–37. [Google Scholar] [CrossRef] [Green Version]
- Dos Santos, J.C.; Schafer, M.; Bauder-Wüst, U.; Lehnert, W.; Leotta, K.; Morgenstern, A.; Kopka, K.; Haberkorn, U.; Mier, W.; Kratochwil, C. Development and dosimetry of 203Pb/212Pb-labelled PSMA ligands: Bringing "the lead" into PSMA-targeted alpha therapy? Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1081–1091. [Google Scholar] [CrossRef] [Green Version]
- Fendler, W.P.; Kratochwil, C.; Ahmadzadehfar, H.; Rahbar, K.; Baum, R.P.; Schmidt, M.; Pfestroff, A.; Lutzen, U.; Prasad, V.; Heinzel, A.; et al. 177Lu-PSMA-617 therapy, dosimetry and follow-up in patients with metastatic castration-resistant prostate cancer. Nuklearmedizin 2016, 55, 123–128. [Google Scholar] [CrossRef]
- Scarpa, L.; Buxbaum, S.; Kendler, D.; Fink, K.; Bektic, J.; Gruber, L.; Decristoforo, C.; Uprimny, C.; Lukas, P.; Horninger, W.; et al. The 68Ga/177Lu theragnostic concept in PSMA targeting of castration-resistant prostate cancer: Correlation of SUVmax values and absorbed dose estimates. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 788–800. [Google Scholar] [CrossRef] [PubMed]
- Violet, J.; Jackson, P.; Ferdinandus, J.; Sandhu, S.; Akhurst, T.; Iravani, A.; Kong, G.; Kumar, A.R.; Thang, S.P.; Eu, P.; et al. Dosimetry of 177Lu-PSMA-617 in Metastatic Castration-Resistant Prostate Cancer: Correlations Between Pretherapeutic Imaging and Whole-Body Tumor Dosimetry with Treatment Outcomes. J. Nucl. Med. 2019, 60, 517–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernhardt, P.; Ahlman, H.; Forssell-Aronsson, E. Model of metastatic growth valuable for radionuclide therapy. Med. Phys. 2003, 30, 3227–3232. [Google Scholar] [CrossRef] [PubMed]
- Bernhardt, P.; Benjegard, S.A.; Kolby, L.; Johanson, V.; Nilsson, O.; Ahlman, H.; Forssell-Aronsson, E. Dosimetric comparison of radionuclides for therapy of somatostatin receptor-expressing tumors. Int. J. Radiat. Oncol. Biol. Phys. 2001, 51, 514–524. [Google Scholar] [CrossRef]
- Müller, C.; Reber, J.; Haller, S.; Dorrer, H.; Bernhardt, P.; Zhernosekov, K.; Türler, A.; Schibli, R. Direct in vitro and in vivo comparison of 161Tb and 177Lu using a tumour-targeting folate conjugate. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 476–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller, C.; Umbricht, C.A.; Gracheva, N.; Tschan, V.J.; Pellegrini, G.; Bernhardt, P.; Zeevaart, J.R.; Köster, U.; Schibli, R.; van der Meulen, N.P. Terbium-161 for PSMA-targeted radionuclide therapy of prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1919–1930. [Google Scholar] [CrossRef] [Green Version]
- Eckerman, K.; Endo, A. ICRP Publication 107. Nuclear decay data for dosimetric calculations. Ann. ICRP 2008, 38, 7–96. [Google Scholar] [CrossRef]
- Gundem, G.; Van Loo, P.; Kremeyer, B.; Alexandrov, L.B.; Tubio, J.M.C.; Papaemmanuil, E.; Brewer, D.S.; Kallio, H.M.L.; Hognas, G.; Annala, M.; et al. The evolutionary history of lethal metastatic prostate cancer. Nature 2015, 520, 353–357. [Google Scholar] [CrossRef]
- Wilkerson, J.; Abdallah, K.; Hugh-Jones, C.; Curt, G.; Rothenberg, M.; Simantov, R.; Murphy, M.; Morrell, J.; Beetsch, J.; Sargent, D.J.; et al. Estimation of tumour regression and growth rates during treatment in patients with advanced prostate cancer: A retrospective analysis. Lancet Oncol. 2017, 18, 143–154. [Google Scholar] [CrossRef]
- Bubendorf, L.; Schopfer, A.; Wagner, U.; Sauter, G.; Moch, H.; Willi, N.; Gasser, T.C.; Mihatsch, M.J. Metastatic patterns of prostate cancer: An autopsy study of 1,589 patients. Hum. Pathol. 2000, 31, 578–583. [Google Scholar] [CrossRef]
- Fowler, J.; Chappell, R.; Ritter, M. Is alpha/beta for prostate tumors really low? Int. J. Radiat. Oncol. Biol. Phys. 2001, 50, 1021–1031. [Google Scholar] [CrossRef]
- Wang, J.Z.; Guerrero, M.; Li, X.A. How low is the alpha/beta ratio for prostate cancer? Int. J. Radiat. Oncol. Biol. Phys. 2003, 55, 194–203. [Google Scholar] [CrossRef]
- Zaorsky, N.G.; Palmer, J.D.; Hurwitz, M.D.; Keith, S.W.; Dicker, A.P.; Den, R.B. What is the ideal radiotherapy dose to treat prostate cancer? A meta-analysis of biologically equivalent dose escalation. Radiother. Oncol. 2015, 115, 295–300. [Google Scholar] [CrossRef]
- Eichelberger, L.E.; Koch, M.O.; Eble, J.N.; Ulbright, T.M.; Juliar, B.E.; Cheng, L. Maximum tumor diameter is an independent predictor of prostate-specific antigen recurrence in prostate cancer. Mod. Pathol. 2005, 18, 886–890. [Google Scholar] [CrossRef] [Green Version]
- D’Agostino, D.; Corsi, P.; Colicchia, M.; Romagnoli, D.; Busetto, G.M.; Ferro, M.; Tafuri, A.; Cevenini, M.; Mineo Bianchi, F.; Giampaoli, M.; et al. The pathological and clinical features of anterior lesions of prostate cancer: Evaluation in a single cohort of patients. Arch. Ital. Urol. Androl. 2020, 92. [Google Scholar] [CrossRef]
- Rauscher, I.; Maurer, T.; Beer, A.J.; Graner, F.P.; Haller, B.; Weirich, G.; Doherty, A.; Gschwend, J.E.; Schwaiger, M.; Eiber, M. Value of 68Ga-PSMA HBED-CC PET for the Assessment of Lymph Node Metastases in Prostate Cancer Patients with Biochemical Recurrence: Comparison with Histopathology After Salvage Lymphadenectomy. J. Nucl. Med. 2016, 57, 1713–1719. [Google Scholar] [CrossRef] [Green Version]
- Gracheva, N.; Müller, C.; Talip, Z.; Heinitz, S.; Köster, U.; Zeevaart, J.R.; Vogele, A.; Schibli, R.; van der Meulen, N.P. Production and characterization of no-carrier-added 161Tb as an alternative to the clinically-applied 177Lu for radionuclide therapy. EJNMMI Radiopharm. Chem. 2019, 4, 12. [Google Scholar] [CrossRef]
- Haller, S.; Pellegrini, G.; Vermeulen, C.; van der Meulen, N.P.; Köster, U.; Bernhardt, P.; Schibli, R.; Müller, C. Contribution of Auger/conversion electrons to renal side effects after radionuclide therapy: Preclinical comparison of 161Tb-folate and 177Lu-folate. EJNMMI Res. 2016, 6, 13. [Google Scholar] [CrossRef] [Green Version]
- Grünberg, J.; Lindenblatt, D.; Dorrer, H.; Cohrs, S.; Zhernosekov, K.; Koster, U.; Türler, A.; Fischer, E.; Schibli, R. Anti-L1CAM radioimmunotherapy is more effective with the radiolanthanide terbium-161 compared to lutetium-177 in an ovarian cancer model. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1907–1915. [Google Scholar] [CrossRef]
- Lehenberger, S.; Barkhausen, C.; Cohrs, S.; Fischer, E.; Grunberg, J.; Hohn, A.; Köster, U.; Schibli, R.; Türler, A.; Zhernosekov, K. The low-energy beta(-) and electron emitter 161Tb as an alternative to 177Lu for targeted radionuclide therapy. Nucl. Med. Biol. 2011, 38, 917–924. [Google Scholar] [CrossRef]
- Alcocer-Avila, M.E.; Ferreira, A.; Quinto, M.A.; Morgat, C.; Hindie, E.; Champion, C. Radiation doses from 161Tb and 177Lu in single tumour cells and micrometastases. EJNMMI Phys. 2020, 7, 33. [Google Scholar] [CrossRef]
- Champion, C.; Quinto, M.A.; Morgat, C.; Zanotti-Fregonara, P.; Hindie, E. Comparison between Three Promising β−emitting Radionuclides, 67Cu, 47Sc and 161Tb, with Emphasis on Doses Delivered to Minimal Residual Disease. Theranostics 2016, 6, 1611–1618. [Google Scholar] [CrossRef] [Green Version]
- Hindie, E.; Zanotti-Fregonara, P.; Quinto, M.A.; Morgat, C.; Champion, C. Dose Deposits from 90Y, 177Lu, 111In, and 161Tb in Micrometastases of Various Sizes: Implications for Radiopharmaceutical Therapy. J. Nucl. Med. 2016, 57, 759–764. [Google Scholar] [CrossRef] [Green Version]
- Cackowski, F.C.; Taichman, R.S. Parallels between hematopoietic stem cell and prostate cancer disseminated tumor cell regulation. Bone 2019, 119, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Phan, T.G.; Croucher, P.I. The dormant cancer cell life cycle. Nat. Rev. Cancer 2020, 20, 398–411. [Google Scholar] [CrossRef] [PubMed]
- Kratochwil, C.; Bruchertseifer, F.; Rathke, H.; Hohenfellner, M.; Giesel, F.L.; Haberkorn, U.; Morgenstern, A. Targeted Alpha Therapy of mCRPC with 225Actinium-PSMA-617: Swimmer-Plot analysis suggests efficacy regarding duration of tumor-control. J. Nucl. Med. 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sekhar, K.R.; Wang, J.; Freeman, M.L.; Kirschner, A.N. Radiosensitization by enzalutamide for human prostate cancer is mediated through the DNA damage repair pathway. PLoS ONE 2019, 14, e0214670. [Google Scholar] [CrossRef] [Green Version]
- Elsesy, M.E.; Oh-Hohenhorst, S.J.; Loser, A.; Oing, C.; Mutiara, S.; Kocher, S.; Meien, S.; Zielinski, A.; Burdak-Rothkamm, S.; Tilki, D.; et al. Second-Generation Antiandrogen Therapy Radiosensitizes Prostate Cancer Regardless of Castration State through Inhibition of DNA Double Strand Break Repair. Cancers 2020, 12, 2467. [Google Scholar] [CrossRef]
- Ghashghaei, M.; Niazi, T.M.; Aguilar-Mahecha, A.; Klein, K.O.; Greenwood, C.M.T.; Basik, M.; Muanza, T.M. Identification of a Radiosensitivity Molecular Signature Induced by Enzalutamide in Hormone-sensitive and Hormone-resistant Prostate Cancer Cells. Sci. Rep. 2019, 9, 8838. [Google Scholar] [CrossRef] [Green Version]
- Klusa, D.; Lohaus, F.; Furesi, G.; Rauner, M.; Benesova, M.; Krause, M.; Kurth, I.; Peitzsch, C. Metastatic Spread in Prostate Cancer Patients Influencing Radiotherapy Response. Front. Oncol. 2020, 10, 627379. [Google Scholar] [CrossRef]
- Brauer, A.; Grubert, L.S.; Roll, W.; Schrader, A.J.; Schäfers, M.; Bogemann, M.; Rahbar, K. 177Lu-PSMA-617 radioligand therapy and outcome in patients with metastasized castration-resistant prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1663–1670. [Google Scholar] [CrossRef]
- Yordanova, A.; Becker, A.; Eppard, E.; Kurpig, S.; Fisang, C.; Feldmann, G.; Essler, M.; Ahmadzadehfar, H. The impact of repeated cycles of radioligand therapy using [177Lu]Lu-PSMA-617 on renal function in patients with hormone refractory metastatic prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1473–1479. [Google Scholar] [CrossRef] [PubMed]
- Schlenkhoff, C.D.; Gaertner, F.; Essler, M.; Schmidt, M.; Ahmadzadehfar, H. Positive Influence of 177Lu PSMA-617 Therapy on Bone Marrow Depression Caused by Metastatic Prostate Cancer. Clin. Nucl. Med. 2016, 41, 478–480. [Google Scholar] [CrossRef] [PubMed]
- Kabasakal, L.; AbuQbeitah, M.; Aygun, A.; Yeyin, N.; Ocak, M.; Demirci, E.; Toklu, T. Pre-therapeutic dosimetry of normal organs and tissues of 177Lu-PSMA-617 prostate-specific membrane antigen (PSMA) inhibitor in patients with castration-resistant prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1976–1983. [Google Scholar] [CrossRef] [PubMed]
- Von Eyben, F.E.; Kiljunen, T.; Joensuu, T.; Kairemo, K.; Uprimny, C.; Virgolini, I. 177Lu-PSMA-617 radioligand therapy for a patient with lymph node metastatic prostate cancer. Oncotarget 2017, 8, 66112–66116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernhardt, P.; Forssell-Aronsson, E.; Jacobsson, L.; Skarnemark, G. Low-energy electron emitters for targeted radiotherapy of small tumours. Acta Oncol. 2001, 40, 602–608. [Google Scholar] [PubMed]
- Umbricht, C.A.; Köster, U.; Bernhardt, P.; Gracheva, N.; Johnston, K.; Schibli, R.; van der Meulen, N.P.; Müller, C. Alpha-PET for Prostate Cancer: Preclinical investigation using 149Tb-PSMA-617. Sci. Rep. 2019, 9, 17800. [Google Scholar] [CrossRef] [Green Version]
- Marin, I.; Ryden, T.; Van Essen, M.; Svensson, J.; Gracheva, N.; Köster, U.; Zeevaart, J.R.; van der Meulen, N.P.; Müller, C.; Bernhardt, P. Establishment of a clinical SPECT/CT protocol for imaging of 161Tb. EJNMMI Phys. 2020, 7, 45. [Google Scholar] [CrossRef]
- Baum, R.P.; Singh, A.; Kulkarni, H.R.; Bernhardt, P.; Ryden, T.; Schuchardt, C.; Gracheva, N.; Grundler, P.V.; Koster, U.; Muller, D.; et al. First-in-Human Application of Terbium-161: A Feasibility Study Using 161Tb-DOTATOC. J. Nucl. Med. 2021. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PSMA-Ligand/ Study | n | Range | Tumor (Gy/GBq) | Kidney (Gy/GBq) | Bone Marrow (Gy/GBq) | Salivary Gland (Gy/GBq) |
|---|---|---|---|---|---|---|
| [177Lu]Lu-PSMA-617 Baum el at. [3] | 8 | mean TND | 3.3 (0.03–78) | 0.8 4.1 (0.03–97) | 0.025 132 | 1.3 2.5 |
| [177Lu]Lu-PSMA-617 Fendler et al. [9] | 15 | mean TND | 6.1 | 0.55 11 | 0.02 (0.05) 305 | 1.0 6.1 |
| [177Lu]Lu-PSMA-617 Scarpa et al. [10] | 10 | mean TND | 3.4 (1.1–7.17) | 0.6 (0.11–1.39) 4.9 (2.2–66) | 0.04 (0.02–0.1) 74 (24–290) | 1.0 (0.48–2.7) 3.8 (2.0–8.3) |
| [177Lu]Lu-PSMA-617 Violet et al [11]. | 30 | mean | 5.3 (0.41–11) | 0.39 (0.09–0.84) 14 | 0.11 (0.01–0.34) 48 | 0.58 (0.13–1.87) 9.1 |
| [225Ac]Ac-PSMA-617 Kratochwil et al. [6] | 4 | mean TND | 5.7 Sv5/MBq | 0.74 Sv5/MBq 7.7 | 0.05 Sv5/MBq 110 | 2.3 Sv5/MBq 2.5 |
| [213Bi]Bi-PSMA-617 Kratochwil et al. [7] | 3 | mean TND | 6.3 Sv5/MBq | 8.1 Sv5/MBq 0.78 | 0.52 Sv5/MBq 12 | 8.1 Sv5/MBq 1.3 |
| [212Pb]Pb-PSMA-CA012 dos Santos et al., [8] | 2 | mean TND | 140 mSv5/MBq | 49 ± 2 mSv5/MBq 2.9 | 6.2 ± 1.2 m Sv5/MBq 23 | 75 m Sv5/MBq 1.9 |
| Physical Properties | 90Y | 131I | 177Lu | 161Tb | 225Ac/../../../ 209Bi |
|---|---|---|---|---|---|
| Main decay modes | β- | β- | β- | β- | α/β- |
| Physical half-life (d) | 2.7 | 8.0 | 6.6 | 6.9 | 10.2 |
| Beta/CE/Auger (keV/decay) | |||||
| 0.01–10 | 0 | 1 | 2 | 9 | 6 |
| 10–50 | 1 | 6 | 9 | 43 | 18 |
| 50–100 | 2 | 13 | 16 | 16 | 24 |
| 100–200 | 7 | 41 | 52 | 45 | 62 |
| 200–1000 | 294 | 129 | 67 | 87 | 504 |
| 1000–9000 | 630 | 0 | 0 | 0 | 52 |
| Alpha (keV/decay) | 0 | 0 | 0 | 0 | 5787/6304/7068/5846 (2.1)/8377 (97.9) |
| Main photon-energies keV (%) | Bremsstrahlung | 364 (82) 637 (7) | 113 (6) 208 (11) | 26 (23) 49 (17) 75 (10) | 218 (11) 221Fr 440 (26) 213Bi |
| Number of Detectable Metastases | Metastatic Formation Constant (%/day/g) | Formation Time (d) | Median Size of Detectable Metastases | Total Number of Metastases | Total Metastatic Burden (cm3) |
|---|---|---|---|---|---|
| 1 | 0.16 | 1390 | 0.80 (0.19–9.0) | 7.70 | 1.80 |
| 5 | 0.16 | 1750 | 2.0 (0.20–23.8) | 18.7 | 23.8 |
| 10 | 0.16 | 1990 | 3.5 (0.21–35.1) | 33.6 | 80.2 |
| 20 | 0.16 | 2290 | 5.0 (0.21–46.7) | 67.1 | 228 |
| 1 | 2.56 | 1070 | 0.40 (0.18–3.0) | 47.3 | 0.94 |
| 5 | 2.56 | 1220 | 0.54 (0.19–5.0) | 91.3 | 5.72 |
| 10 | 2.56 | 1310 | 0.66 (0.19–7.2) | 136 | 14.7 |
| 20 | 2.56 | 1410 | 0.81 (0.19–9.7) | 220 | 37.7 |
| Radionuclide | Required Absorbed Dose | ||||
|---|---|---|---|---|---|
| Number of Detectable Metastases | |||||
| 0 | 1 | 5 | 10 | 20 | |
| 90Y | 80 Gy | 2630–3010 Gy | 2740–3130 Gy | 2860–3220 Gy | 3000–3330 Gy |
| 131I | 80 Gy | 920–1120 Gy | 985–1170 Gy | 1040–1220 Gy | 1100–1270 Gy |
| 177Lu | 80 Gy | 558–682 Gy | 598–715 Gy | 630–742 Gy | 672–777 Gy |
| 225Ac | 80 Gy | 243–292 Gy5 | 252–307 Gy5 | 269–320 Gy5 | 288–335 Gy5 |
| 161Tb | 80 Gy | 207–247 Gy | 220–260 Gy | 230–270 Gy | 245–281 Gy |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernhardt, P.; Svensson, J.; Hemmingsson, J.; van der Meulen, N.P.; Zeevaart, J.R.; Konijnenberg, M.W.; Müller, C.; Kindblom, J. Dosimetric Analysis of the Short-Ranged Particle Emitter 161Tb for Radionuclide Therapy of Metastatic Prostate Cancer. Cancers 2021, 13, 2011. https://doi.org/10.3390/cancers13092011
Bernhardt P, Svensson J, Hemmingsson J, van der Meulen NP, Zeevaart JR, Konijnenberg MW, Müller C, Kindblom J. Dosimetric Analysis of the Short-Ranged Particle Emitter 161Tb for Radionuclide Therapy of Metastatic Prostate Cancer. Cancers. 2021; 13(9):2011. https://doi.org/10.3390/cancers13092011
Chicago/Turabian StyleBernhardt, Peter, Johanna Svensson, Jens Hemmingsson, Nicholas P. van der Meulen, Jan Rijn Zeevaart, Mark W. Konijnenberg, Cristina Müller, and Jon Kindblom. 2021. "Dosimetric Analysis of the Short-Ranged Particle Emitter 161Tb for Radionuclide Therapy of Metastatic Prostate Cancer" Cancers 13, no. 9: 2011. https://doi.org/10.3390/cancers13092011