
Early Tumor Response and Safety of Atezolizumab Plus Bevacizumab for Patients with Unresectable Hepatocellular Carcinoma in Real-World Practice

 , , add
Show full author list
, , add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Treatment Regimens
2.3. Assessment of Response to Therapy
2.4. Safety Assessment
2.5. Statistical Analysis
3. Results
3.1. Patient Background Characteristics
3.2. Tumor Responses
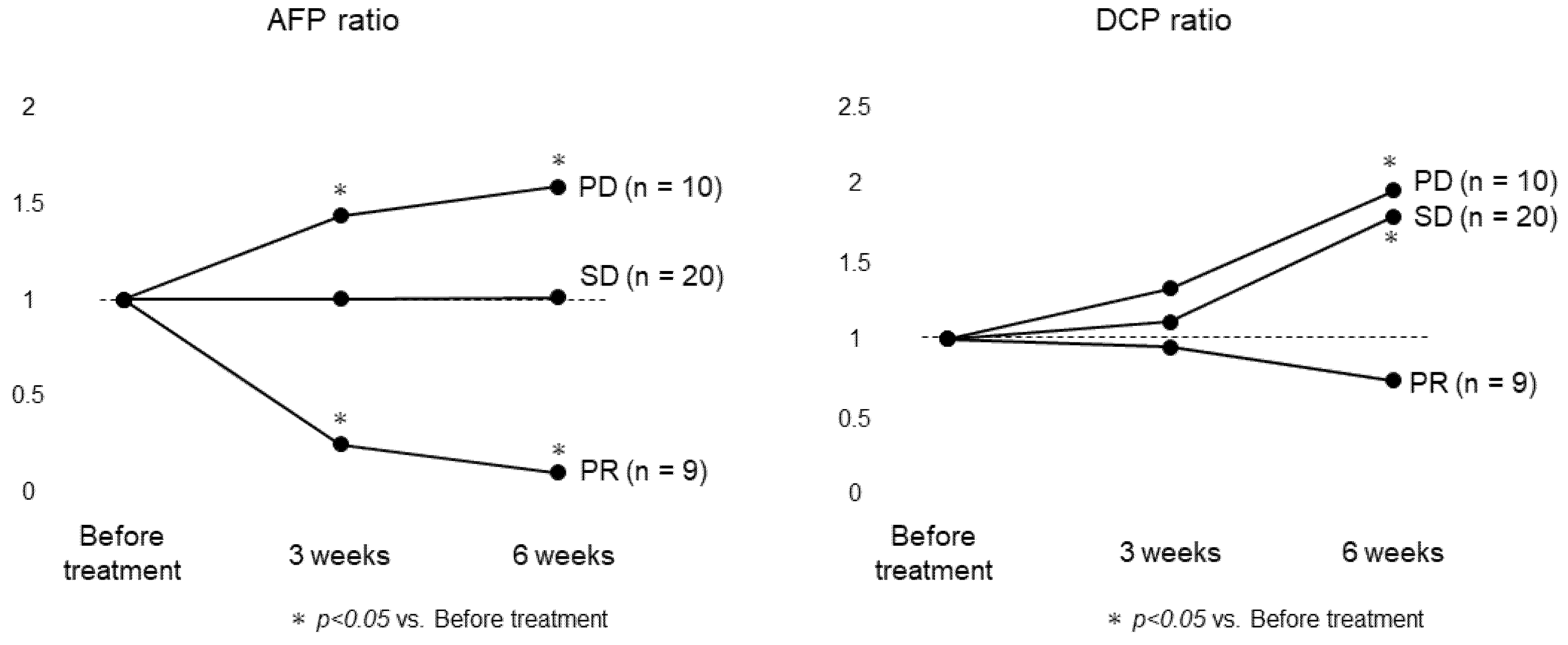
3.3. Changes in Tumor Markers
3.4. Correlation between Assessment by Tumor Markers and mRECIST
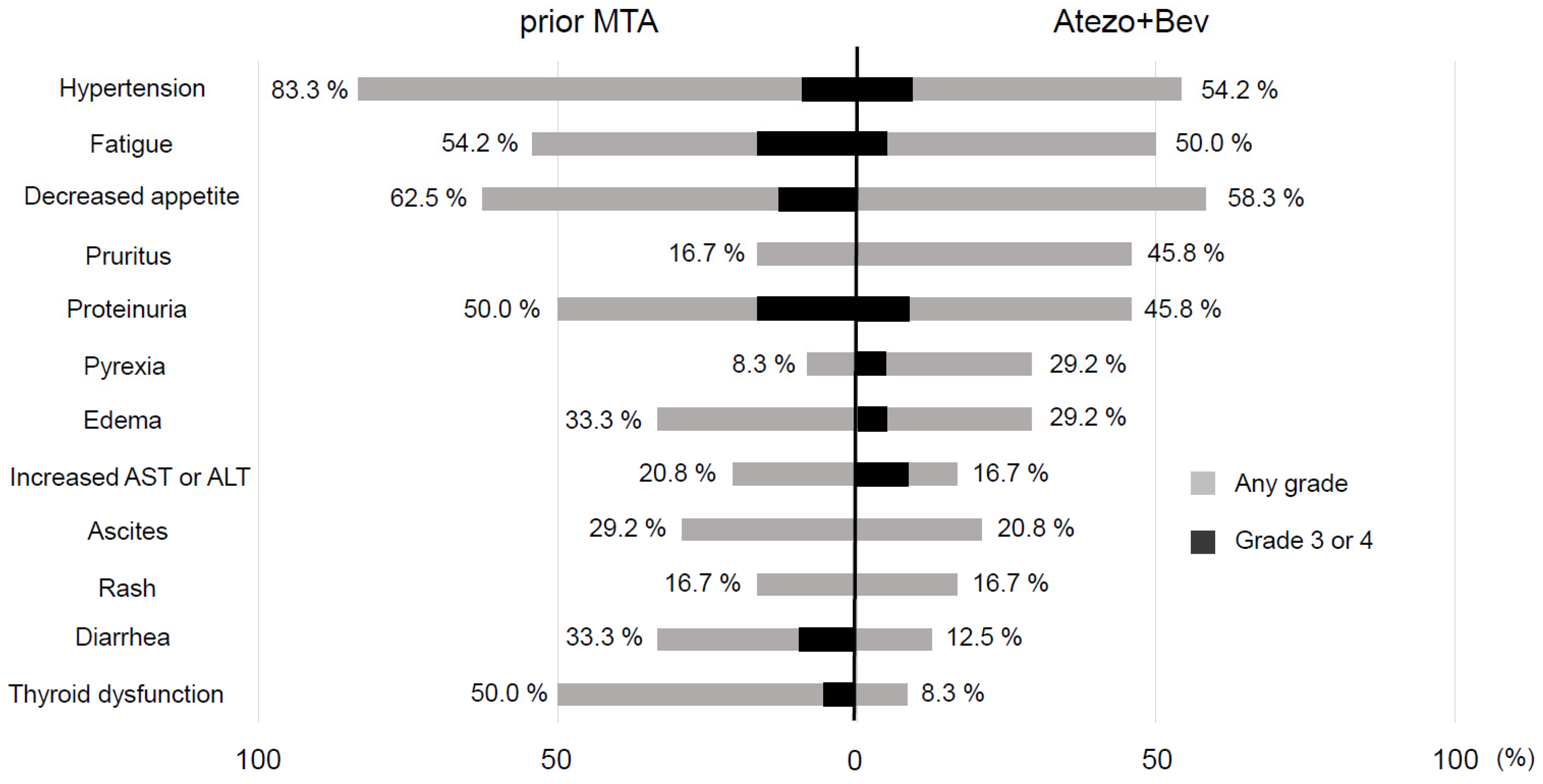
3.5. Adverse Events
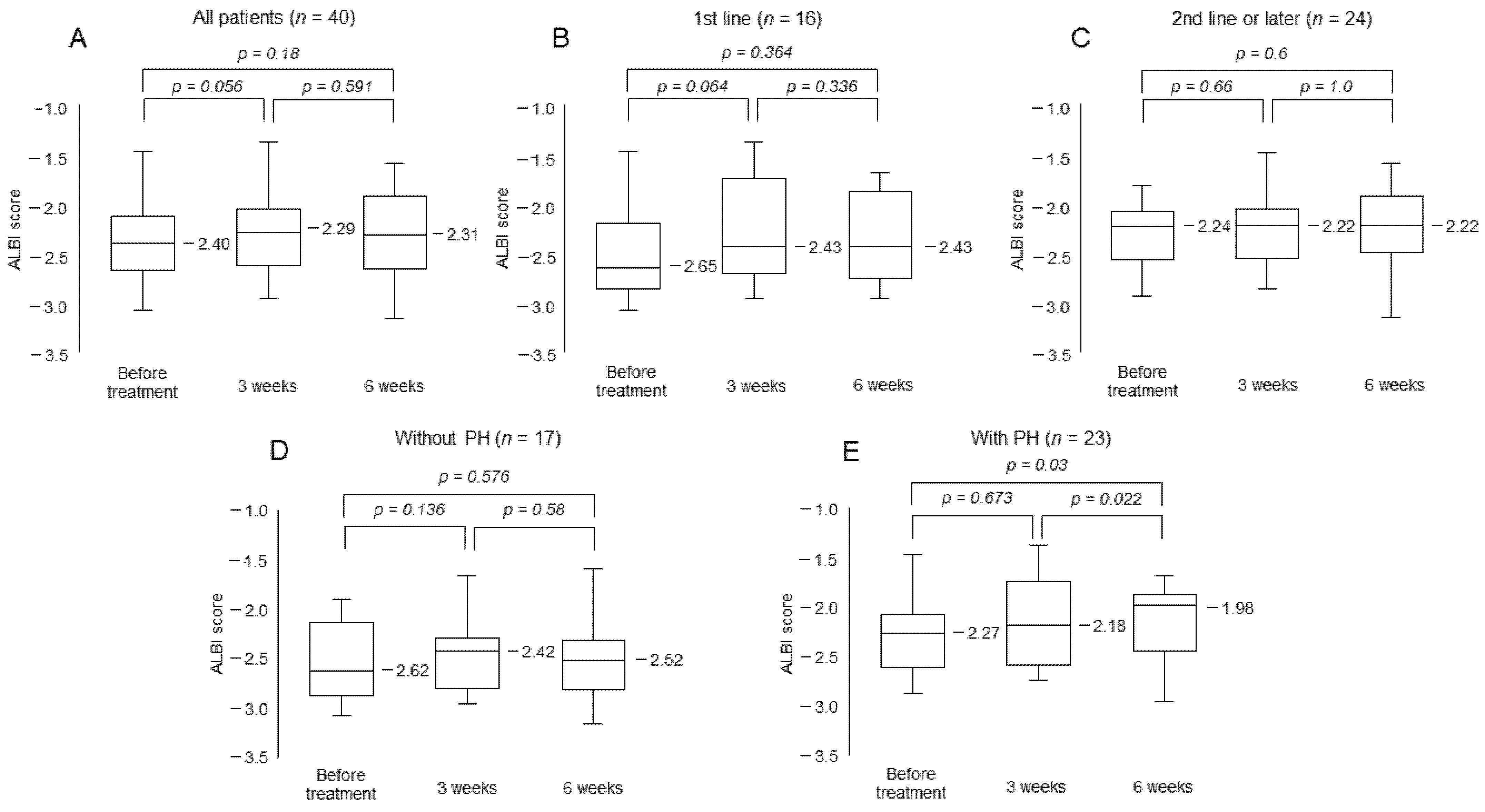
3.6. Change in ALBI Score
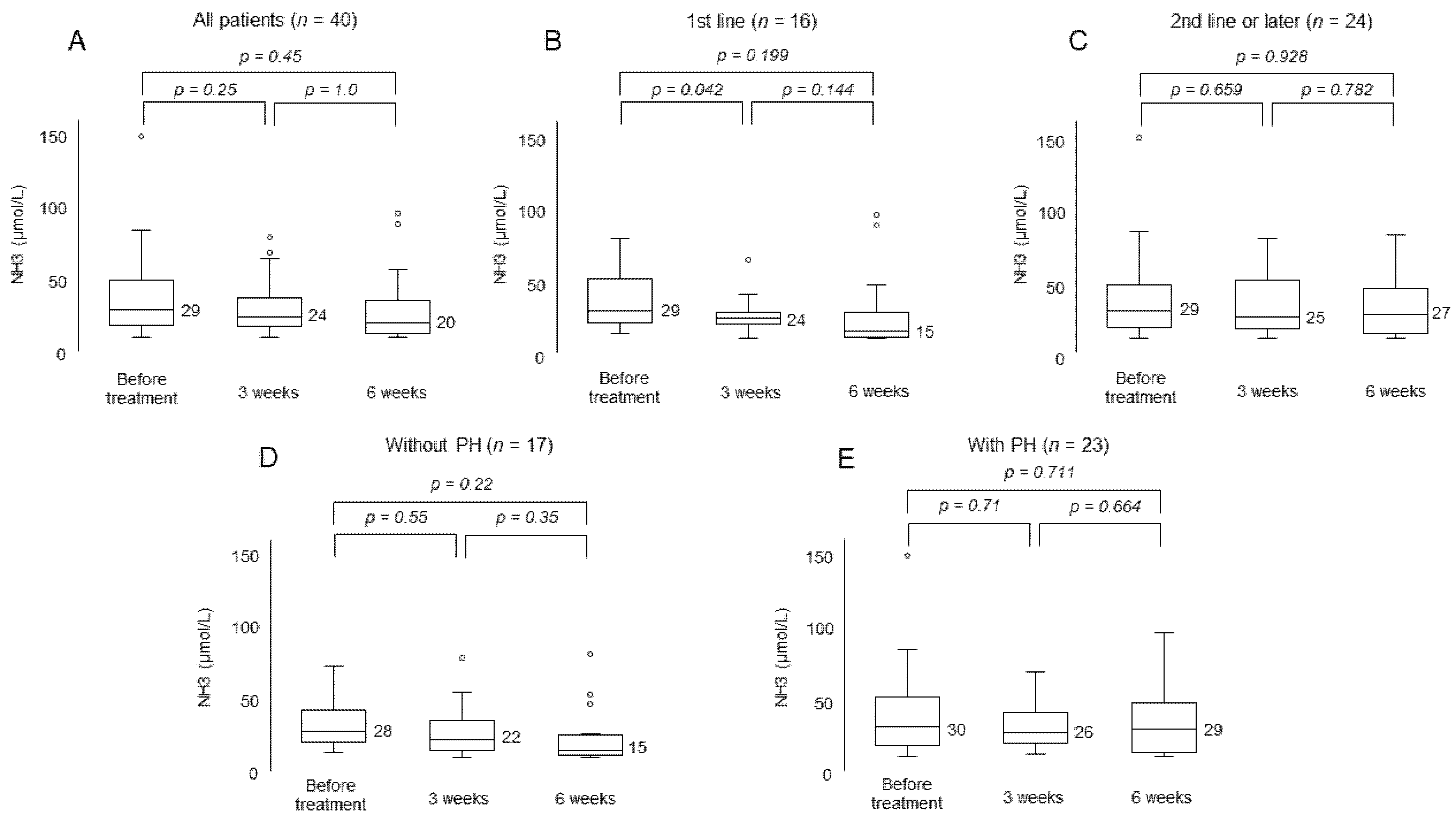
3.7. Change in Serum Ammonia Level
4. Discussion
5. Conclusion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Forner, A.; Reig, M.; Bruix, J. Hepatocellular carcinoma. Lancet 2018, 391, 1301–1314. [Google Scholar] [CrossRef]
- Singal, A.G.; El-Serag, H.B. Hepatocellular carcinoma from epidemiology to prevention: Translating knowledge into practice. Clin. Gastroenterol. Hepatol. 2015, 13, 2140–2151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herbst, R.S.; Soria, J.-C.; Kowanetz, M.; Fine, G.D.; Hamid, O.; Gordon, M.S.; Sosman, J.A.; McDermott, D.F.; Powderly, J.D.; Gettinger, S.N.; et al. Predictive correlates of response to the anti-PD-L1 antibody MPDL3280A in cancer patients. Nature 2014, 515, 563–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrara, N.; Hillan, K.J.; Novotny, W. Bevacizumab (Avastin), a humanized anti-VEGF monoclonal antibody for cancer therapy. Biochem. Biophys. Res. Commun. 2005, 333, 328–335. [Google Scholar] [CrossRef]
- Finn, R.S.; Bentley, G.; Britten, C.D.; Amado, R.; Busuttil, R.W. Targeting vascular endothelial growth factor with the monoclonal antibody bevacizumab inhibits human hepatocellular carcinoma cells growing in an orthotopic mouse model. Liver Int. 2009, 29, 284–290. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Lu, Y.; Qin, S. Atezolizumab and bevacizumab for hepatocellular carcinoma: Mechanism, pharmacokinetics and future treatment strategies. Future Oncol. 2021, 17, 2243–2256. [Google Scholar] [CrossRef]
- Schwartz, L.H.; Seymour, L.; Litière, S.; Ford, R.; Gwyther, S.; Mandrekar, S.; Shankar, L.; Bogaerts, J.; Chen, A.; Dancey, J.; et al. RECIST 1.1—Standardisation and disease-specific adaptations: Perspectives from the RECIST Working Group. Eur. J. Cancer 2016, 62, 138–145. [Google Scholar] [CrossRef] [Green Version]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [Green Version]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Hiraoka, A.; Kumada, T.; Tsuji, K.; Takaguchi, K.; Itobayashi, E.; Kariyama, K.; Ochi, H.; Tajiri, K.; Hirooka, M.; Shimada, N.; et al. Validation of modified ALBI grade for more detailed assessing hepatic function of hepatocellular carcinoma—Multicenter analysis. Liver Cancer 2019, 8, 121–129. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [Green Version]
- Kuzuya, T.; Kawabe, N.; Hashimoto, S.; Miyahara, R.; Nakano, T.; Nakaoka, K.; Tanaka, H.; Miyachi, Y.; Mii, A.; Tanahashi, Y.; et al. Initial Experience of Atezolizumab Plus Bevacizumab for Advanced Hepatocellular Carcinoma in Clinical Practice. Cancer Diagn. Progn. 2021, 1, 83–88. [Google Scholar]
- Iwamoto, H.; Shimose, S.; Noda, Y.; Shirono, T.; Niizeki, T.; Nakano, M.; Okamura, S.; Kamachi, N.; Suzuki, H.; Sakai, M.; et al. Initial Experience of Atezolizumab Plus Bevacizumab for Unresectable Hepatocellular Carcinoma in Real-World Clinical Practice. Cancers 2021, 13, 2786. [Google Scholar] [CrossRef]
- Hiraoka, A.; Kumada, T.; Tada, T.; Hirooka, M.; Kariyama, K.; Yani, J.; Atsukawa, M.; Takaguchi, K.; Itobayashi, E.; Fukunishi, S.; et al. Atezolizumab plus bevacizumab treatment for unresectable hepatocellular carcinoma: Early clinical experience. Cancer Rep. (Hoboken) 2021, e1464. [Google Scholar] [CrossRef]
- Sánchez, A.I.; Roces, L.V.; García, I.Z.; López, E.L.; Hernandez, M.A.; Parejo, M.I.; Díaz, J.P. Value of α-fetoprotein as an early biomarker for treatment response to sorafenib therapy in advanced hepatocellular carcinoma. Oncol. Lett. 2018, 15, 8863–8870. [Google Scholar] [PubMed] [Green Version]
- Liu, L.; Zhao, Y.; Jia, J.; Chen, H.; Bai, W.; Yang, M.; Yin, Z.; He, C.; Zhang, L.; Guo, W.; et al. The prognostic value of alpha-fetoprotein response for advanced-stage hepatocellular carcinoma treated with sorafenib combined with transarterial chemoembolization. Sci. Rep. 2016, 6, 19851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuzuya, T.; Ishigami, M.; Ishizu, Y.; Honda, T.; Hayashi, K.; Katano, Y.; Hirooka, Y.; Ishikawa, T.; Nakano, I.; Goto, H.; et al. Early clinical response after 2 weeks of sorafenib therapy predicts outcomes and anti-tumor response in patients with advanced hepatocellular carcinoma. PLoS ONE 2015, 10, e0138776. [Google Scholar] [CrossRef]
- Kawaoka, T.; Aikata, H.; Murakami, E.; Nakahara, T.; Naeshiro, N.; Tanaka, M.; Honda, Y.; Miyaki, D.; Nagaoki, Y.; Takaki, S.; et al. Evaluation of the mRECIST and α-fetoprotein ratio for stratification of the prognosis of advanced hepatocellular-carcinoma patients treated with sorafenib. Oncology 2012, 83, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Kodama, K.; Kawaoka, T.; Namba, M.; Uchikawa, S.; Ohya, K.; Morio, K.; Nakahara, T.; Murakami, E.; Yamauchi, M.; Hiramatsu, A.; et al. Correlation between early tumor marker response and imaging response in patients with advanced hepatocellular carcinoma treated with lenvatinib. Oncology 2019, 97, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Brahmer, J.R.; Lacchetti, C.; Schneider, B.J.; Aktins, M.B.; Brassil, K.J.; Caterino, J.M.; Chau, I.; Ernstoff, M.S.; Gardner, J.M.; Ginex, P.; et al. Management of Immune-Related Adverse Events in Patients Treated With Immune Checkpoint Inhibitor Therapy: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2018, 36, 1714–1768. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, A.; Kumada, T.; Atsukawa, M.; Hirooka, M.; Tsuji, K.; Ishikawa, T.; Takaguchi, K.; Kariyama, K.; Itobayashi, E.; Tajiri, K.; et al. Early Relative Change in Hepatic Function with Lenvatinib for Unresectable Hepatocellular Carcinoma. Oncology 2019, 97, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Uchikawa, S.; Kawaoka, T.; Ando, Y.; Yamaoka, K.; Kosaka, Y.; Suehiro, Y.; Fujii, Y.; Morio, K.; Nakahara, T.; Murakami, E.; et al. Trends in Hepatic Functional Reserve of Patients with Hepatocellular Carcinoma Treated with Tyrosine Kinase Inhibitors. Oncology 2020, 98, 727–733. [Google Scholar] [CrossRef]
- Ohya, H.; Kawaoka, T.; Namba, M.; Uchikawa, S.; Kodama, K.; Morio, K.; Nakahara, T.; Murakami, E.; Hiramatsu, A.; Tsuge, M.; et al. Early changes in ammonia levels and liver function in patients with advanced hepatocellular carcinoma treated by lenvatinib therapy. Sci. Rep. 2019, 9, 12101. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | All Patients (n = 40) | 1st Line Patients (n = 16) | 2nd Line or Later Patients (n = 24) | p-Value * |
|---|---|---|---|---|
| Age (yr), range | 69 (47–90) | 69 (55–90) | 70 (47–87) | 0.383 |
| Sex (males/females), n | 30/10 | 11/5 | 19/5 | 0.482 |
| Etiology (Viral/NBNC), n | 26/14 | 11/5 | 15/9 | 0.746 |
| Child-Pugh score (5/6), n | 21/19 | 11/5 | 10/14 | 0.117 |
| Modified ALBI grade (1–2a/2b), n | 23/17 | 12/4 | 11/13 | 0.104 |
| ALBI score | −2.40 (–3.07–1.47) | –2.65 (–3.07–1.47) | –2.24 (–2.94–1.83) | 0.048 |
| Serum ammonia level (μg/dL), range | 29 (10–149) | 29 (13–79) | 29 (10–149) | 0.793 |
| Size of main tumor (intrahepatic) (mm), range | 40 (0–130) | 40 (0–130) | 38 (0–130) | 0.934 |
| Relative tumor size (<50%/≥50%), n | 36/4 | 16/0 | 20/4 | 0.278 |
| MVI (absent/present), n | 28/12 | 11/5 | 17/7 | 1.0 |
| EHM (absent/present), n | 24/16 | 13/3 | 11/13 | 0.047 |
| BCLC stage (B/C), n | 18/22 | 9/7 | 9/15 | 0.335 |
| Serum AFP level (ng /mL), range | 79.0 (1.8–35,780) | 174.1 (2.3–35,780) | 79.0 (1.8–34,200) | 0.730 |
| Serum DCP level (mAU/mL), range | 347 (15–108,710) | 292 (19–35,040) | 446 (15–108,710) | 0.945 |
| Observation period (day), range | 120 (42–174) | 100 (42–184) | 136 (46–188) | 0.204 |
| Line | Treatment | n |
|---|---|---|
| 2nd line | Len | 14 |
| Sor | 1 | |
| Investigational products | 1 | |
| 3rd line | Len→Sor | 1 |
| Len→Ram | 1 | |
| 4th line | Len→Sor→Reg | 2 |
| Sor→Reg→Len | 2 | |
| 5th line | Len→Sor→Reg→Ram | 1 |
| Sor→Reg→Len→Ram | 1 |
| mRECIST | RECIST 1.1 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| % (n) | All Patients | 1st Line Patients | 2nd Line or Later Patients | Difference | % (n) | All Patients | 1st Line Patients | 2nd Line or LaterPatients | Difference |
| (n = 40) | (n = 16) | (n = 24) | (p-Value *) | (n = 40) | (n = 16) | (n = 24) | (p-Value *) | ||
| Confirmed ORR | 22.5 (9) | 37.5 (6) | 12.5 (3) | 0.12 | Confirmed ORR | 7.5 (3) | 6.2 (1) | 8.3 (2) | 1 |
| CR | 0 (0) | 0 (0) | 0 (0) | CR | 0 (0) | 0 (0) | 0 (0) | ||
| PR | 22.5 (9) | 37.5 (6) | 12.5 (3) | PR | 7.5 (3) | 6.2 (1) | 8.3 (2) | ||
| SD | 50.0 (20) | 43.8 (7) | 54.2 (13) | SD | 67.5 (27) | 81.3 (13) | 58.4 (14) | ||
| PD | 25.0 (10) | 12.5 (2) | 33.3 (8) | PD | 25.0 (10) | 12.5 (2) | 33.3 (8) | ||
| N.E | 2.5 (1) | 6.2 (1) | 0 (0) | N.E | 0 (0) | 0 (0) | 0 (0) | ||
| DCR | 72.5 (29) | 81.3 (13) | 66.7 (16) | 0.477 | DCR | 75.0 (30) | 87.5 (14) | 66.7 (16) | 0.473 |
| Variable | Univariate | Multivariate | ||
|---|---|---|---|---|
| p-Value * | OR | 95% CI | p-Value ** | |
| Age (yr) (<70 vs. ≥70) | 1.0 | |||
| Sex (male vs. female) | 1.0 | |||
| Etiology (Viral vs. NBNC) | 0.694 | |||
| ECOG performance status (0 vs. 1) | 1.0 | |||
| Child-Pugh score (5 vs. 6) | 0.021 | |||
| Modified ALBI grade (1 or 2a vs. 2b) | 0.256 | |||
| Relative tumor volume (<50% vs. ≥50%) | 0.570 | |||
| MVI (absent vs present) | 0.697 | |||
| EHM (absent vs present) | 0.272 | |||
| Serum AFP level (<400 vs. ≥400) | 0.690 | |||
| Serum DCP level (<340 vs. ≥340) | 0.060 | |||
| History of systemic therapy (without vs. with) | 0.120 | |||
| AFP ratio at 3weeks (<1.0 vs. ≥1.0) | 0.014 | 21.3 | 2.01–225.0 | 0.011 |
| DCP ratio at 3weeks (<1.0 vs. ≥1.0) | 0.705 | |||
| Event% (n) | All Patients (n = 40) | 1st Line Patients (n = 16) | 2nd Line or Later Patients (n = 24) | Difference (p-Value *) | ||||
|---|---|---|---|---|---|---|---|---|
| Any Grade | Grade 3 or 4 | Time (Days) | Any Grade | Grade 3 or 4 | Any Grade | Grade 3 or 4 | ||
| Hypertension | 60.0 (24) | 10.0 (4) | 24 (2–73) | 68.8 (11) | 12.5 (2) | 54.2 (13) | 8.3 (2) | 0.512 |
| Fatigue | 57.5 (23) | 2.5 (1) | 22 (6–155) | 68.8 (11) | 0 | 50.0 (12) | 4.2 (1) | 0.332 |
| Decreased appetite | 57.5 (23) | 2.5 (1) | 21 (3–155) | 56.3 (9) | 1 (6.3) | 58.3 (14) | 0 | 1.0 |
| Pruritus | 50.0 (20) | 0 | 21 (6–85) | 56.3 (9) | 0 | 45.8 (11) | 0 | 0.748 |
| Proteinuria | 37.5 (15) | 7.5 (3) | 23 (6–101) | 25.0 (4) | 6.3 (1) | 45.8 (11) | 8.3 (2) | 0.74 |
| Pyrexia | 35.0 (14) | 2.5 (1) | 11 (4–77) | 43.8 (7) | 0 | 29.2 (7) | 4.2 (1) | 0.5 |
| Edema | 25.0 (10) | 2.5 (1) | 24 (16–133) | 18.8 (3) | 0 | 29.2 (7) | 4.2 (1) | 0.711 |
| Increased AST or ALT | 20.0 (8) | 7.5 (3) | 16 (2–41) | 25.0 (4) | 6.3 (1) | 16.7 (4) | 8.3 (2) | 0.69 |
| Ascites | 15.0 (6) | 0 | 15 (6–69) | 6.3 (1) | 0 | 20.8 (5) | 0 | 0.373 |
| Rash | 15.0 (6) | 0 | 29 (7–71) | 12.5 (2) | 0 | 16.7 (4) | 0 | 1.0 |
| Diarrhea | 12.5 (5) | 0 | 21 (15–171) | 12.5 (2) | 0 | 12.5 (3) | 0 | 1.0 |
| Thyroid dysfunction | 10.0 (4) | 0 | 44 (37–174) | 12.5 (2) | 0 | 8.3 (2) | 0 | 1.0 |
| Gastrointestinal bleeding | 7.5 (3) | 7.5 (3) | 6.3 (1) | 6.3 (1) | 8.3 (2) | 8.3 (2) | 1.0 | |
| Portal vein thrombus | 2.5 (1) | 0 | 0 | 0 | 4.2 (1) | 0 | 1.0 | |
| Stroke | 2.5 (1) | 0 | 0 | 0 | 4.2 (1) | 0 | 1.0 | |
| Atezo + Bev | |||||
| Hypertension | (+) | (−) | Incidence rate (%) | p-value * | |
| Prior MTA | (+) | 11 | 9 | 55.0 | 1.0 |
| (−) | 2 | 2 | 50.0 | ||
| Atezo + Bev | |||||
| Fatigue | (+) | (−) | Incidence rate (%) | p-value * | |
| Prior MTA | (+) | 10 | 3 | 76.9 | 0.012 |
| (−) | 2 | 9 | 18.2 | ||
| Atezo + Bev | |||||
| Decreased appetite | (+) | (−) | Incidence rate (%) | p-value * | |
| Prior MTA | (+) | 10 | 5 | 66.7 | 0.403 |
| (−) | 4 | 5 | 44.4 | ||
| Atezo + Bev | |||||
| Pruritus | (+) | (−) | Incidence rate (%) | p-value * | |
| Prior MTA | (+) | 2 | 2 | 50.0 | 1.0 |
| (−) | 9 | 11 | 45.0 | ||
| Atezo + Bev | |||||
| Proteinuria | (+) | (−) | Incidence rate (%) | p-value * | |
| Prior MTA | (+) | 9 | 3 | 75.0 | 0.012 |
| (−) | 2 | 10 | 16.7 | ||
| Atezo + Bev | |||||
| Pyrexia | (+) | (−) | Incidence rate (%) | p-value * | |
| Prior MTA | (+) | 2 | 0 | 100 | 0.076 |
| (−) | 5 | 17 | 22.7 | ||
| Atezo + Bev | |||||
| Edema | (+) | (−) | Incidence rate (%) | p-value * | |
| Prior MTA | (+) | 2 | 6 | 25.0 | 1.0 |
| (−) | 5 | 11 | 31.2 | ||
| Atezo + Bev | |||||
| Increased AST/ALT | (+) | (−) | Incidence rate (%) | p-value * | |
| Prior MTA | (+) | 1 | 4 | 20.0 | 1.0 |
| (−) | 3 | 16 | 15.8 | ||
| Atezo + Bev | |||||
| Ascites | (+) | (−) | Incidence rate (%) | p-value * | |
| Prior MTA | (+) | 4 | 3 | 57.1 | 0.015 |
| (−) | 1 | 16 | 5.9 | ||
| Atezo + Bev | |||||
| Rash | (+) | (−) | Incidence rate (%) | p-value * | |
| Prior MTA | (+) | 0 | 4 | 0 | 1.0 |
| (−) | 4 | 16 | 20.0 | ||
| Atezo + Bev | |||||
| Diarrhea | (+) | (−) | Incidence rate (%) | p-value * | |
| Prior MTA | (+) | 0 | 8 | 0 | 0.526 |
| (−) | 3 | 13 | 18.8 | ||
| Atezo + Bev | |||||
| Thyroid dysfunction | (+) | (−) | Incidence rate (%) | p-value * | |
| Prior MTA | (+) | 2 | 10 | 16.7 | 0.478 |
| (−) | 0 | 12 | 0 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ando, Y.; Kawaoka, T.; Kosaka, M.; Shirane, Y.; Johira, Y.; Miura, R.; Murakami, S.; Yano, S.; Amioka, K.; Naruto, K.; et al. Early Tumor Response and Safety of Atezolizumab Plus Bevacizumab for Patients with Unresectable Hepatocellular Carcinoma in Real-World Practice. Cancers 2021, 13, 3958. https://doi.org/10.3390/cancers13163958
Ando Y, Kawaoka T, Kosaka M, Shirane Y, Johira Y, Miura R, Murakami S, Yano S, Amioka K, Naruto K, et al. Early Tumor Response and Safety of Atezolizumab Plus Bevacizumab for Patients with Unresectable Hepatocellular Carcinoma in Real-World Practice. Cancers. 2021; 13(16):3958. https://doi.org/10.3390/cancers13163958
Chicago/Turabian StyleAndo, Yuwa, Tomokazu Kawaoka, Masanari Kosaka, Yuki Shirane, Yusuke Johira, Ryoichi Miura, Serami Murakami, Shigeki Yano, Kei Amioka, Kensuke Naruto, and et al. 2021. "Early Tumor Response and Safety of Atezolizumab Plus Bevacizumab for Patients with Unresectable Hepatocellular Carcinoma in Real-World Practice" Cancers 13, no. 16: 3958. https://doi.org/10.3390/cancers13163958