
Recent Advances in the Treatment of Bone Metastases and Primary Bone Tumors: An Up-to-Date Review


 ,
,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Bone Tumors
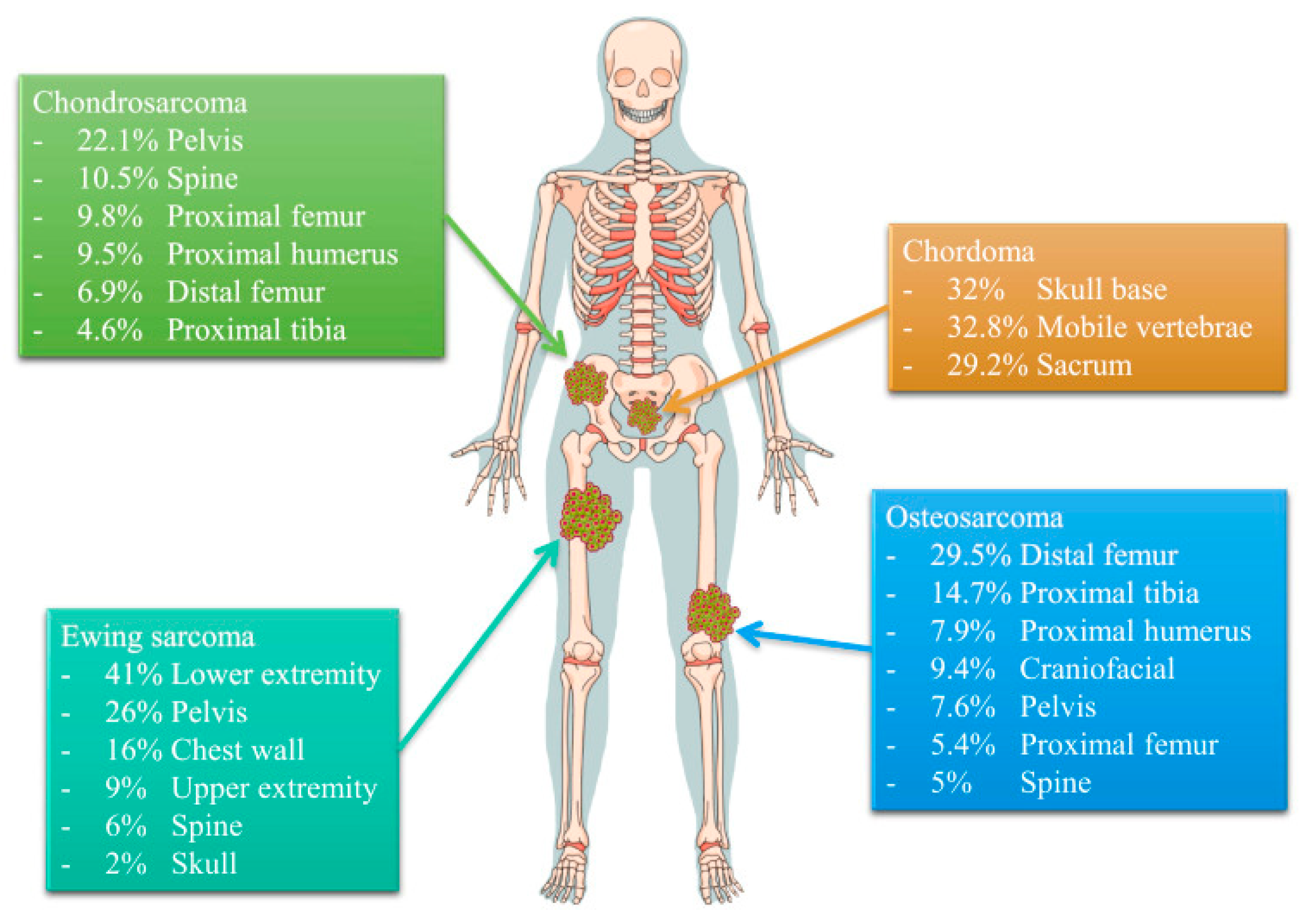
2.1. Sarcomas
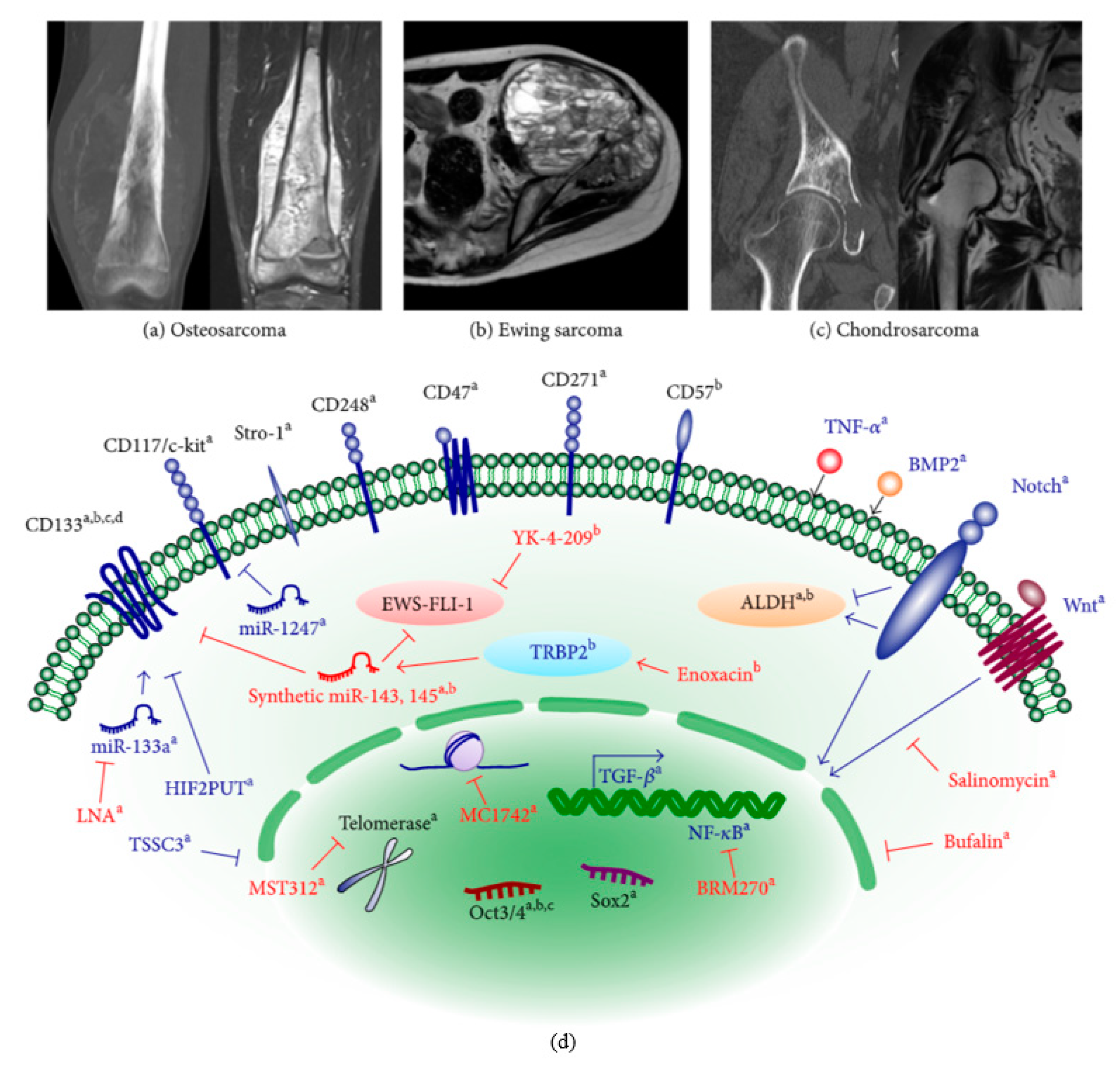
2.1.1. Osteosarcoma
2.1.2. Chondrosarcoma
2.1.3. Ewing Sarcoma
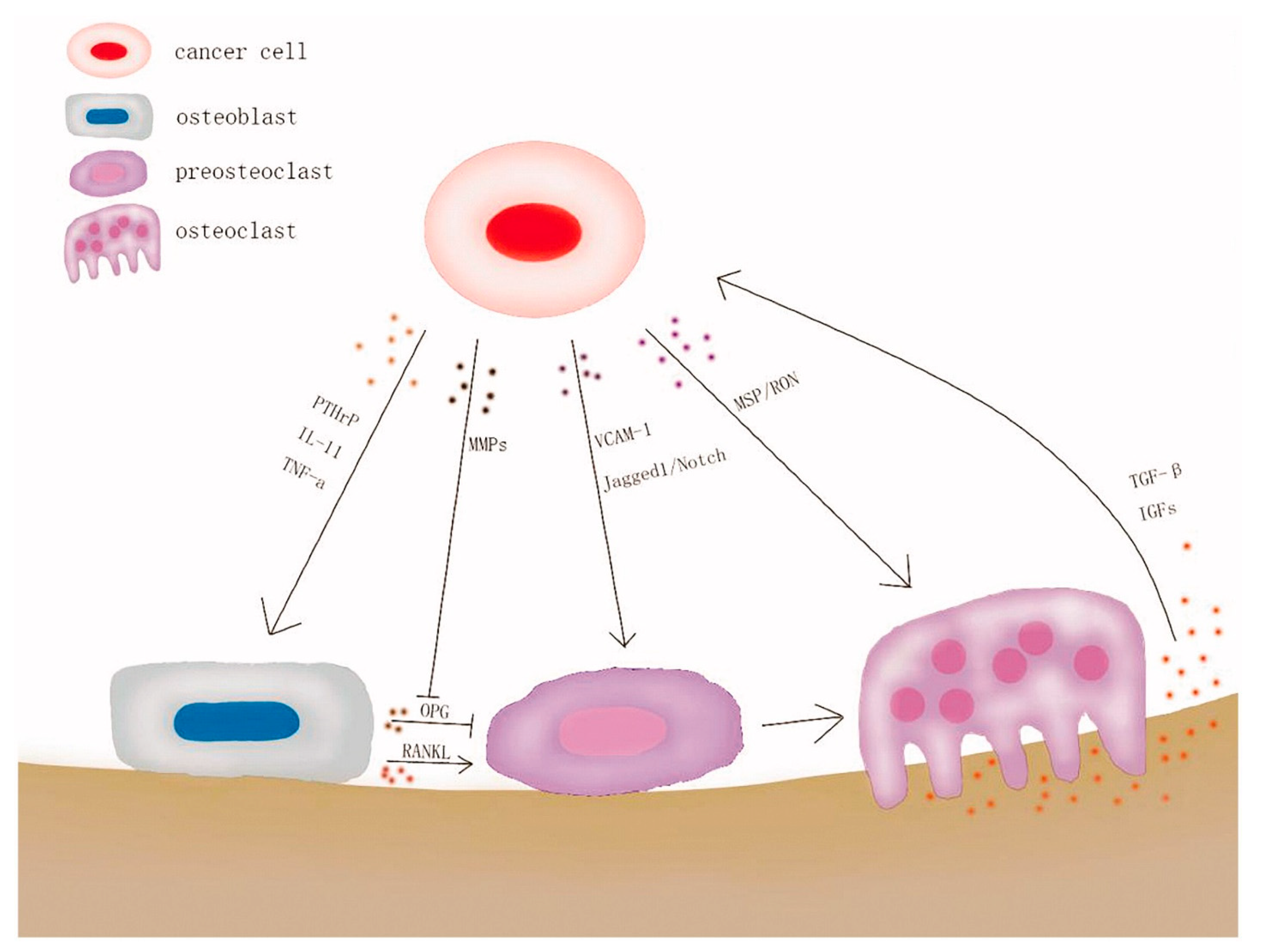
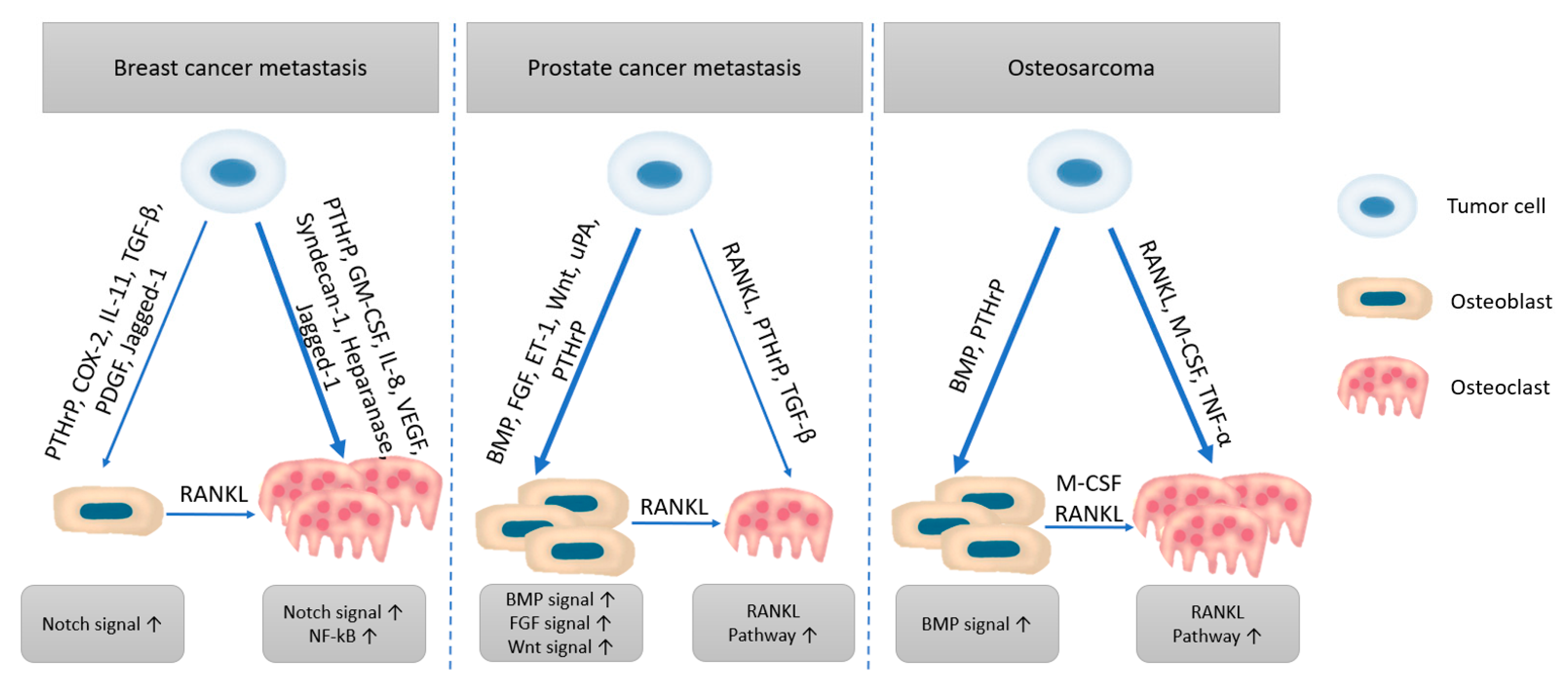
2.2. Metastases
3. Current Treatments and Tumor Resistance
3.1. Chemotherapy
3.2. Radiotherapy
3.3. Surgical Management
4. Recent Approaches against Bone Tumors
4.1. Adjuvant Therapies
4.2. Drug Delivery
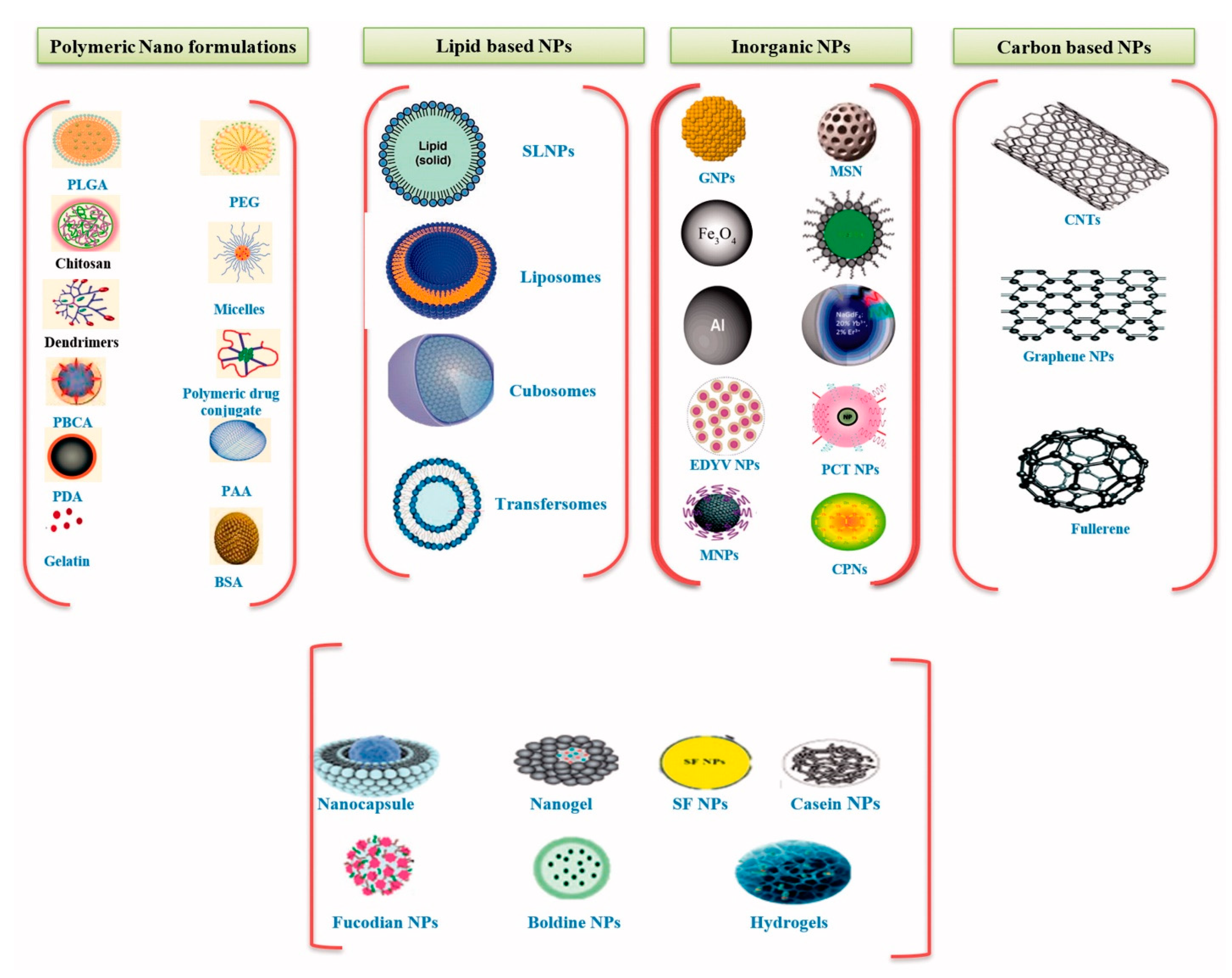
4.2.1. Carrier Systems
4.2.2. Carried Agents
5. Bone Reconstruction Following Tumor Resection
5.1. Bone Grafts
5.2. Bone Substitutes
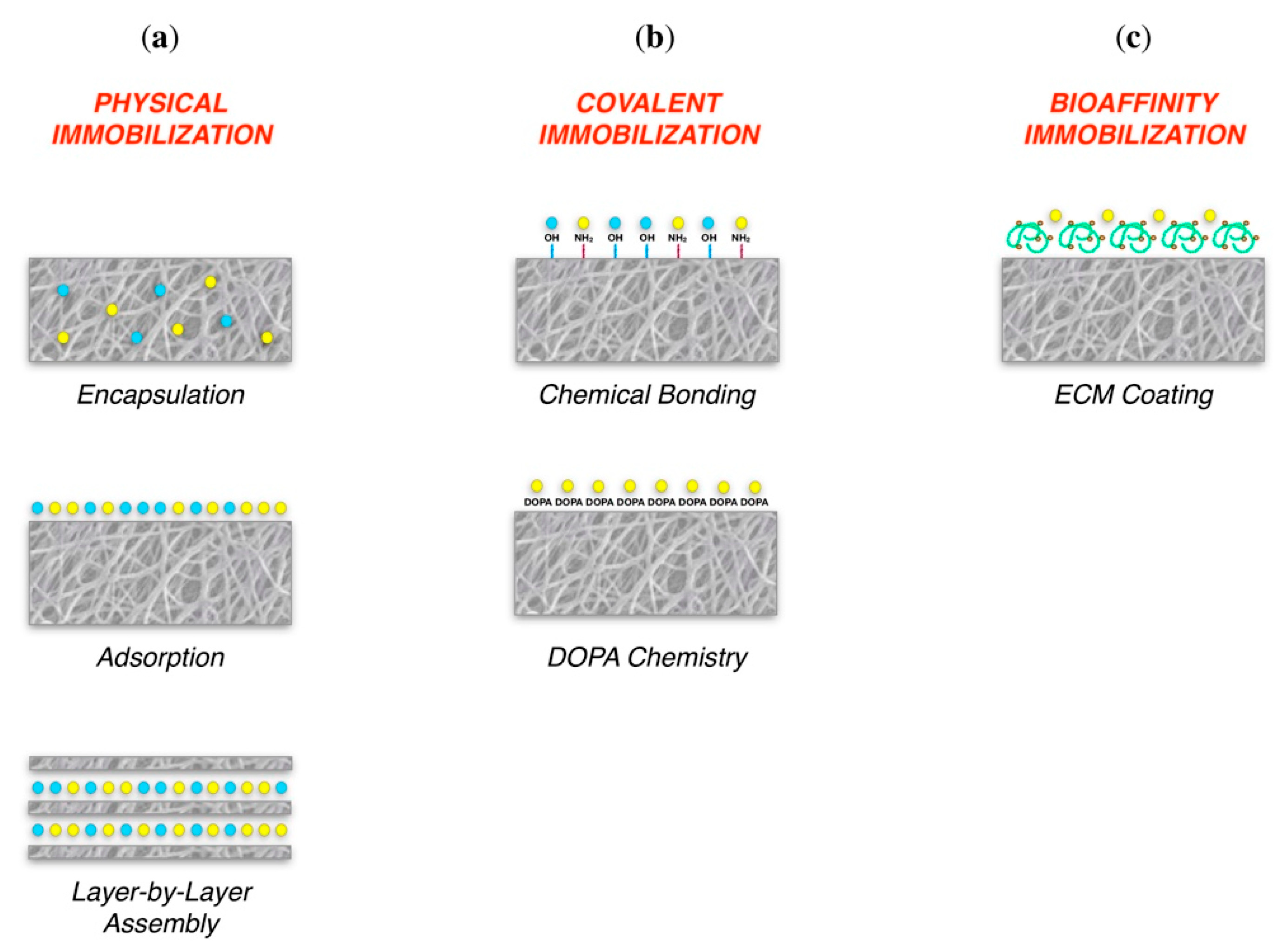
5.3. Tissue Engineering Approaches
6. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cheng, L.; Shoma Suresh, K.; He, H.; Rajput, R.S.; Feng, Q.; Ramesh, S.; Wang, Y.; Krishnan, S.; Ostrovidov, S.; Camci-Unal, G.; et al. 3D Printing of Micro- and Nanoscale Bone Substitutes: A Review on Technical and Translational Perspectives. Int. J. Nanomed. 2021, 16, 4289–4319. [Google Scholar] [CrossRef]
- Ciocca, L.; Lesci, I.; Ragazzini, S.; Gioria, S.; Valsesia, A.; Parrilli, A.; Spadari, A.; Dozza, B.; Mora, P.; Piattelli, A.; et al. Nanostructured surface bioactive composite scaffold for filling of bone defects. Biointerface Res. Appl. Chem. 2020, 10, 5038–5047. [Google Scholar] [CrossRef]
- Busch, A.; Jäger, M.; Mayer, C.; Sowislok, A. Functionalization of Synthetic Bone Substitutes. Int. J. Mol. Sci. 2021, 22, 4412. [Google Scholar] [CrossRef]
- Jayash, S.; Al-Namnam, N.M.; Shaghayegh, G. Osteoprotegerin (OPG) pathways in bone diseases and its application in therapeutic perspectives. Biointerface Res. Appl. Chem. 2020, 10, 5193–5200. [Google Scholar] [CrossRef]
- Altieri, B.; Di Dato, C.; Martini, C.; Sciammarella, C.; Di Sarno, A.; Colao, A.; Faggiano, A.; NIKE Group; on behalf of NIKE Group on behalf of NIKE Group; on behalf of NIKE Group. Bone Metastases in Neuroendocrine Neoplasms: From Pathogenesis to Clinical Management. Cancers 2019, 11, 1332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menéndez, S.; Gallego, B.; Murillo, D.; Rodríguez, A.; Rodríguez, R. Cancer Stem Cells as a Source of Drug Resistance in Bone Sarcomas. J. Clin. Med. 2021, 10, 2621. [Google Scholar] [CrossRef] [PubMed]
- Rajani, R.; Gibbs, C.P. Treatment of Bone Tumors. Surg. Pathol. Clin. 2012, 5, 301–318. [Google Scholar] [CrossRef] [Green Version]
- Thanindratarn, P.; Dean, D.C.; Nelson, S.D.; Hornicek, F.J.; Duan, Z. Advances in immune checkpoint inhibitors for bone sarcoma therapy. J. Bone Oncol. 2019, 15, 100221. [Google Scholar] [CrossRef]
- Ferracini, R.; Martínez-Herreros, I.; Russo, A.; Casalini, T.; Rossi, F.; Perale, G. Scaffolds as Structural Tools for Bone-Targeted Drug Delivery. Pharmaceutics 2018, 10, 122. [Google Scholar] [CrossRef] [Green Version]
- Cortini, M.; Baldini, N.; Avnet, S. New Advances in the Study of Bone Tumors: A Lesson from the 3D Environment. Front. Physiol. 2019, 10, 814. [Google Scholar] [CrossRef] [Green Version]
- Ma, H.; Li, T.; Huan, Z.; Zhang, M.; Yang, Z.; Wang, J.; Chang, J.; Wu, C. 3D printing of high-strength bioscaffolds for the synergistic treatment of bone cancer. NPG Asia Mater. 2018, 10, 31–44. [Google Scholar] [CrossRef] [Green Version]
- Sharma, A.; Sharma, P.K.; Malviya, R. Stimuli-responsive supramolecules for bone tissue engineering. Biointerface Res. Appl. Chem. 2020, 10, 5122–5127. [Google Scholar] [CrossRef]
- Bickels, J.; Campanacci, D.A. Local Adjuvant Substances Following Curettage of Bone Tumors. J. Bone Jt. Surg.-Am. Vol. 2019, 102, 164–174. [Google Scholar] [CrossRef]
- Miwa, S.; Yamamoto, N.; Tsuchiya, H. Bone and Soft Tissue Tumors: New Treatment Approaches. Cancers 2021, 13, 1832. [Google Scholar] [CrossRef]
- Hattinger, C.; Patrizio, M.; Fantoni, L.; Casotti, C.; Riganti, C.; Serra, M. Drug Resistance in Osteosarcoma: Emerging Biomarkers, Therapeutic Targets and Treatment Strategies. Cancers 2021, 13, 2878. [Google Scholar] [CrossRef]
- Parisi, L.; Toffoli, A.; Ghiacci, G.; Macaluso, G.M. Tailoring the Interface of Biomaterials to Design Effective Scaffolds. J. Funct. Biomater. 2018, 9, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.H.; Oh, J.H.; Han, I.; Kim, H.-S.; Chung, S.W. Grafting Using Injectable Calcium Sulfate in Bone Tumor Surgery: Comparison with Demineralized Bone Matrix-based Grafting. Clin. Orthop. Surg. 2011, 3, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Bedini, R.; Pecci, R.; Meleo, D.; Campioni, I. Bone Substitutes Scaffold in Human Bone: Comparative Evaluation by 3D Micro-CT Technique. Appl. Sci. 2020, 10, 3451. [Google Scholar] [CrossRef]
- Tzanakakis, G.; Giatagana, E.-M.; Berdiaki, A.; Spyridaki, I.; Hida, K.; Neagu, M.; Tsatsakis, A.; Nikitovic, D. The Role of IGF/IGF-IR-Signaling and Extracellular Matrix Effectors in Bone Sarcoma Pathogenesis. Cancers 2021, 13, 2478. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, T.; Ozaki, T. Overcoming Therapeutic Resistance of Bone Sarcomas: Overview of the Molecular Mechanisms and Therapeutic Targets for Bone Sarcoma Stem Cells. Stem Cells Int. 2016, 2016, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Franchi, A. Epidemiology and classification of bone tumors. Clin. Cases Miner. Bone Metab. 2012, 9, 92–95. [Google Scholar]
- Steinbichler, T.B.; Dudas, J.; Skvortsov, S.; Ganswindt, U.; Riechelmann, H.; Skvortsova, I.-I. Therapy resistance mediated by cancer stem cells. Semin. Cancer Biol. 2018, 53, 156–167. [Google Scholar] [CrossRef] [PubMed]
- Taran, R.; Taran, S.; Malipatil, N. Pediatric osteosarcoma: An updated review. Indian J. Med Paediatr. Oncol. 2017, 38, 33–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gambera, S.; Patiño-Garcia, A.; Alfranca, A.; Garcia-Castro, J. RGB-Marking to Identify Patterns of Selection and Neutral Evolution in Human Osteosarcoma Models. Cancers 2021, 13, 2003. [Google Scholar] [CrossRef] [PubMed]
- Society, A.C. Cancer Facts & Figures 2021; American Cancer Society: Atlanta, GA, USA, 2021. [Google Scholar]
- Society, A.C. Survival Rates for Osteosarcoma. Available online: https://www.cancer.org/cancer/osteosarcoma/detection-diagnosis-staging/survival-rates.html (accessed on 12 August 2021).
- Siegel, R.L.; Mph, K.D.M.; Jemal, A. Cancer statistics, 2020. CA A Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Boehme, K.A.; Schleicher, S.B.; Traub, F.; Rolauffs, B. Chondrosarcoma: A Rare Misfortune in Aging Human Cartilage? The Role of Stem and Progenitor Cells in Proliferation, Malignant Degeneration and Therapeutic Resistance. Int. J. Mol. Sci. 2018, 19, 311. [Google Scholar] [CrossRef] [Green Version]
- Zając, A.; Kopeć, S.; Szostakowski, B.; Spałek, M.; Fiedorowicz, M.; Bylina, E.; Filipowicz, P.; Szumera-Ciećkiewicz, A.; Tysarowski, A.; Czarnecka, A.; et al. Chondrosarcoma-from Molecular Pathology to Novel Therapies. Cancers 2021, 13, 2390. [Google Scholar] [CrossRef]
- Tzeng, H.-E.; Lin, S.-L.; Thadevoos, L.-A.; Ko, C.-Y.; Liu, J.-F.; Huang, Y.-W.; Lin, C.-Y.; Fong, Y.-C.; Tang, C.-H. The mir-423-5p/MMP-2 Axis Regulates the Nerve Growth Factor-Induced Promotion of Chondrosarcoma Metastasis. Cancers 2021, 13, 3347. [Google Scholar] [CrossRef]
- Kontny, U.; Lissat, A. Chapter 36—Apoptosis and drug resistance in malignant bone tumors. In Bone Cancer, 2nd ed.; Heymann, D., Ed.; Academic Press: San Diego, CA, USA, 2015; pp. 425–436. [Google Scholar] [CrossRef]
- Thévenin-Lemoine, C.; Destombes, L.; Vial, J.; Wargny, M.; Bonnevialle, P.; Lefevre, Y.; Gomez Brouchet, A.; Sales de Gauzy, J. Planning for Bone Excision in Ewing Sarcoma: Post-Chemotherapy MRI More Accurate Than Pre-Chemotherapy MRI Assessment. J. Bone Jt. Surg. Am. 2018, 100, 13–20. [Google Scholar] [CrossRef] [Green Version]
- Macedo, F.; Ladeira, K.; Pinho, F.; Saraiva, N.; Bonito, N.; Pinto, L.; Gonçalves, F. Bone metastases: An overview. Oncol. Rev. 2017, 11, 321. [Google Scholar] [CrossRef]
- Wang, Y.; Huang, Q.; He, X.; Chen, H.; Zou, Y.; Li, Y.; Lin, K.; Cai, X.; Xiao, J.; Zhang, Q.; et al. Multifunctional melanin-like nanoparticles for bone-targeted chemo-photothermal therapy of malignant bone tumors and osteolysis. Biomaterials 2018, 183, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Chappard, D.; Bouvard, B.; Baslé, M.-F.; Legrand, E.; Audran, M. Bone metastasis: Histological changes and pathophysiological mechanisms in osteolytic or osteosclerotic localizations. A review. Morphologie 2011, 95, 65–75. [Google Scholar] [CrossRef] [Green Version]
- Cheng, X.; Wei, J.; Ge, Q.; Xing, D.; Zhou, X.; Qian, Y.; Jiang, G. The optimized drug delivery systems of treating cancer bone metastatic osteolysis with nanomaterials. Drug Deliv. 2020, 28, 37–53. [Google Scholar] [CrossRef]
- Guise, T.A. Molecular mechanisms of osteolytic bone metastases. Cancer 2000, 88, 2892–2898. [Google Scholar] [CrossRef]
- Guise, T.A.; Mohammad, K.S.; Clines, G.; Stebbins, E.G.; Wong, D.H.; Higgins, L.S.; Vessella, R.; Corey, E.; Padalecki, S.; Suva, L.; et al. Basic Mechanisms Responsible for Osteolytic and Osteoblastic Bone Metastases. Clin. Cancer Res. 2006, 12, 6213s–6216s. [Google Scholar] [CrossRef] [Green Version]
- Clézardin, P.; Teti, A. Bone metastasis: Pathogenesis and therapeutic implications. Clin. Exp. Metastasis 2007, 24, 599–608. [Google Scholar] [CrossRef]
- Jayarangaiah, A.; Kemp, A.K.; Kariyanna, P.T. Bone Metastasis. StatPearls [Internet]. Available online: https://www.ncbi.nlm.nih.gov/books/NBK507911/ (accessed on 6 July 2021).
- Yang, C.; Tian, Y.; Zhao, F.; Chen, Z.; Su, P.; Li, Y.; Qian, A. Bone Microenvironment and Osteosarcoma Metastasis. Int. J. Mol. Sci. 2020, 21, 6985. [Google Scholar] [CrossRef]
- Gupta, G.P.; Massagué, J. Cancer metastasis: Building a framework. Cell 2006, 127, 679–695. [Google Scholar] [CrossRef] [Green Version]
- Nakajima, K.; Kho, D.H.; Yanagawa, T.; Zimel, M.; Heath, E.; Hogan, V.; Raz, A. Galectin-3 in bone tumor microenvironment: A beacon for individual skeletal metastasis management. Cancer Metastasis Rev. 2016, 35, 333–346. [Google Scholar] [CrossRef]
- Wang, M.; Xia, F.; Wei, Y.; Wei, X. Molecular mechanisms and clinical management of cancer bone metastasis. Bone Res. 2020, 8, 1–20. [Google Scholar] [CrossRef]
- Saraf, A.J.; Fenger, J.M.; Roberts, R.D. Osteosarcoma: Accelerating Progress Makes for a Hopeful Future. Front. Oncol. 2018, 8, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferguson, J.L.; Turner, S.P. Bone Cancer: Diagnosis and Treatment Principles. Am. Fam. Physician 2018, 98, 205–213. [Google Scholar]
- Radwan, A.; Khalid, M.; Amer, H.; Alotaibi, M. Anticancer and molecular docking studies of some new pyrazole-1-carbothioamide nucleosides. Biointerface Res. Appl. Chem. 2019, 9, 4642–4648. [Google Scholar] [CrossRef]
- Dickens, E.; Ahmed, S. Principles of cancer treatment by chemotherapy. Surgery 2018, 36, 134–138. [Google Scholar] [CrossRef]
- Małek, A.; Taciak, B.; Sobczak, K.; Grzelak, A.; Wójcik, M.; Mieczkowski, J.; Lechowski, R.; Zabielska-Koczywąs, K. Enhanced Cytotoxic Effect of Doxorubicin Conjugated to Glutathione-Stabilized Gold Nanoparticles in Canine Osteosarcoma—In Vitro Studies. Molecules 2021, 26, 3487. [Google Scholar] [CrossRef] [PubMed]
- Bukowski, K.; Kciuk, M.; Kontek, R. Mechanisms of Multidrug Resistance in Cancer Chemotherapy. Int. J. Mol. Sci. 2020, 21, 3233. [Google Scholar] [CrossRef]
- Hattinger, C.; Fanelli, M.; Tavanti, E.; Vella, S.; Riganti, C.; Picci, P.; Serra, M. Doxorubicin-resistant osteosarcoma: Novel therapeutic approaches in sight? Futur. Oncol. 2017, 13, 673–677. [Google Scholar] [CrossRef]
- Baskar, R.; Lee, K.A.; Yeo, R.; Yeoh, K.-W. Cancer and Radiation Therapy: Current Advances and Future Directions. Int. J. Med. Sci. 2012, 9, 193–199. [Google Scholar] [CrossRef] [Green Version]
- De Felice, F.; Piccioli, A.; Musio, D.; Tombolini, V. The role of radiation therapy in bone metastases management. Oncotarget 2017, 8, 25691–25699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerr, D.L.; Dial, B.L.; Lazarides, A.; Catanzano, A.A.; Lane, W.O.; Blazer, D.G.; Brigman, B.E.; Mendoza-Lattes, S.; Eward, W.C.; Erickson, M.E. Epidemiologic and survival trends in adult primary bone tumors of the spine. Spine J. 2019, 19, 1941–1949. [Google Scholar] [CrossRef] [PubMed]
- Dang, W.; Li, T.; Li, B.; Ma, H.; Zhai, D.; Wang, X.; Chang, J.; Xiao, Y.; Wang, J.; Wu, C. A bifunctional scaffold with CuFeSe2 nanocrystals for tumor therapy and bone reconstruction. Biomaterials 2018, 160, 92–106. [Google Scholar] [CrossRef]
- Capanna, R.; Van Horn, J.R.; Biagini, R.; Ruggieri, P.; Bettelli, G.; Campanacci, M. Reconstruction after resection of the distal fibula for bone tumor. Acta Orthop. Scand. 1986, 57, 290–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sørensen, M.; Colding-Rasmussen, T.; Horstmann, P.; Hindsø, K.; Dehlendorff, C.; Johansen, J.; Petersen, M. Pretreatment Plasma IL-6 and YKL-40 and Overall Survival after Surgery for Metastatic Bone Disease of the Extremities. Cancers 2021, 13, 2833. [Google Scholar] [CrossRef] [PubMed]
- Prasad, S.R.; Kumar, T.S.S.; Jayakrishnan, A. Nanocarrier-based drug delivery systems for bone cancer therapy: A review. Biomed. Mater. 2021, 16, 044107. [Google Scholar] [CrossRef] [PubMed]
- Piccioli, A.; Ventura, A.; Maccauro, G.; Spinelli, M.; Del Bravo, V.; Rosa, M.A. Local Adjuvants in Surgical Management of Bone Metastases. Int. J. Immunopathol. Pharmacol. 2011, 24, 129–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenberg, D.D.; Lee, F.Y. Bisphosphonate-loaded Bone Cement as a Local Adjuvant Therapy for Giant Cell Tumor of Bone: A 1 to 12-Year Follow-up Study. Am. J. Clin. Oncol. 2019, 42, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Ringe, K.I.; Panzica, M.; Von Falck, C. Thermoablation of Bone Tumors. Rofo 2016, 188, 539–550. [Google Scholar] [CrossRef] [Green Version]
- Cazzato, R.L.; Palussière, J.; Auloge, P.; Rousseau, C.; Koch, G.; Dalili, D.; Buy, X.; Garnon, J.; De Marini, P.; Gangi, A. Complications Following Percutaneous Image-guided Radiofrequency Ablation of Bone Tumors: A 10-year Dual-Center Experience. Radiology 2020, 296, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Barei, D.P.; Moreau, G.; Scarborough, M.T.; Neel, M.D. Percutaneous Radiofrequency Ablation of Osteoid Osteoma. Clin. Orthop. Relat. Res. 2000, 373, 115–124. [Google Scholar] [CrossRef]
- Kashima, M.; Yamakado, K.; Takaki, H.; Kaminou, T.; Tanigawa, N.; Nakatsuka, A.; Takeda, K. Radiofrequency Ablation for the Treatment of Bone Metastases From Hepatocellular Carcinoma. Am. J. Roentgenol. 2010, 194, 536–541. [Google Scholar] [CrossRef] [PubMed]
- Finstein, J.L.; Hosalkar, H.S.; Ogilvie, C.M.; Lackman, R.D. Case Reports: An Unusual Complication of Ra-diofrequency Ablation Treatment of Osteoid Osteoma. Clin. Orthop. Relat. Res. 2006, 448, 248–251. [Google Scholar] [CrossRef]
- Mirza, A.N.; Fornage, B.D.; Sneige, N.; Kuerer, H.M.; Newman, L.A.; Ames, F.C.; Singletary, S.E. Radiofre-quency ablation of solid tumors. Cancer J. 2001, 7, 95–102. [Google Scholar] [PubMed]
- Hong, K.; Georgiades, C. Radiofrequency Ablation: Mechanism of Action and Devices. J. Vasc. Interv. Radiol. 2010, 21, S179–S186. [Google Scholar] [CrossRef] [PubMed]
- Jennings, J.W. Is Percutaneous Bone Cryoablation Safe? Radiology 2019, 291, 529–530. [Google Scholar] [CrossRef] [PubMed]
- Callstrom, M.R.; Charboneau, J.W.; Goetz, M.P.; Rubin, J.; Atwell, T.D.; Farrell, M.A.; Welch, T.J.; Maus, T.P. Image-guided ablation of painful metastatic bone tumors: A new and effective approach to a difficult problem. Skelet. Radiol. 2005, 35, 1–15. [Google Scholar] [CrossRef]
- Gangi, A.; Buy, X. Percutaneous Bone Tumors Management. In Imaging in Percutaneous Musculoskeletal Interventions; Gangi, A., Guth, S., Guermazi, A., Eds.; Springer: Berlin/Heidelberg, Germany, 2009; pp. 301–328. [Google Scholar] [CrossRef]
- Groenemeyer, D.H.; Schirp, S.; Gevargez, A. Image-Guided Percutaneous Thermal Ablation of Bone Tumors. Acad. Radiol. 2002, 9, 467–477. [Google Scholar] [CrossRef]
- Cazzato, R.L.; de Rubeis, G.; de Marini, P.; Dalili, D.; Koch, G.; Auloge, P.; Garnon, J.; Gangi, A. Percutaneous microwave ablation of bone tumors: A systematic review. Eur. Radiol. 2020, 31, 3530–3541. [Google Scholar] [CrossRef]
- Fan, Q.-Y.; Zhou, Y.; Zhang, M.; Ma, B.; Yang, T.; Long, H.; Yu, Z.; Li, Z. Microwave Ablation of Primary Ma-lignant Pelvic Bone Tumors. Front. Sur. 2019, 6, 5. [Google Scholar] [CrossRef]
- Zheng, K.; Yu, X.; Hu, Y.; Zhang, Y.; Wang, Z.; Wu, S.; Shen, J.; Ye, Z.; Tu, C.; Zhang, Y.; et al. Clinical Guideline for Microwave Ablation of Bone Tumors in Extremities. Orthop. Surg. 2020, 12, 1036–1044. [Google Scholar] [CrossRef]
- Simon, C.J.; Dupuy, D.; Mayo-Smith, W.W. Microwave Ablation: Principles and Applications. RadioGraphics 2005, 25, S69–S83. [Google Scholar] [CrossRef]
- Tomasian, A.; Jennings, J.W. Percutaneous Minimally Invasive Thermal Ablation of Osseous Metastases: Evidence-Based Practice Guidelines. Am. J. Roentgenol. 2020, 215, 502–510. [Google Scholar] [CrossRef]
- Kurup, A.N.; Callstrom, M.R.; Moynagh, M.R. Thermal Ablation of Bone Metastases. Semin. Interv. Radiol. 2018, 35, 299–308. [Google Scholar] [CrossRef]
- Pacella, C.M.; Di Stasio, E.; Guglielmi, R.; Baroli, A.; Pedrazzini, L.; Misischi, I.; Persichetti, A.; Papini, E. Role of laser ablation in multimodal treatment of radioiodine- refractory bone metastases of thyroid cancer: A retrospective study. Endocrine 2020, 70, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Barile, A.; Arrigoni, F.; Zugaro, L.; Zappia, M.; Cazzato, R.L.; Garnon, J.; Ramamurthy, N.; Brunese, L.; Gangi, A.; Masciocchi, C. Minimally invasive treatments of painful bone lesions: State of the art. Med. Oncol. 2017, 34. [Google Scholar] [CrossRef] [PubMed]
- Zekry, K.M.; Yamamoto, N.; Hayashi, K.; Takeuchi, A.; Araki, Y.; Alkhooly, A.Z.A.; Abd-Elfattah, A.S.; Fouly, E.H.; Elsaid, A.N.S.; Tsuchiya, H. Surgical treatment of chondroblastoma using extended intralesional curettage with phenol as a local adjuvant. J. Orthop. Surg. 2019, 27. [Google Scholar] [CrossRef] [Green Version]
- Di Giacomo, G.; Ziranu, A.; Perisano, C.; Piccioli, A.; Maccauro, G. Local Adjuvants in Surgical Management of Bone Lesions. J. Cancer Ther. 2015, 06, 473–481. [Google Scholar] [CrossRef] [Green Version]
- Jones, K.B.; Deyoung, B.R.; A Morcuende, J.; Buckwalter, J. Ethanol as a local adjuvant for giant cell tumor of bone. Iowa Orthop. J. 2006, 26, 69–76. [Google Scholar] [PubMed]
- Bs, B.B.; Haase, D.; Sweeney, K.; Friedman, E.; Poppe, T.; Hughes, N. A comparison of depth of necrosis among adjuvant therapies used for the treatment of benign bone tumors. J. Surg. Oncol. 2021, 123, 1299–1303. [Google Scholar] [CrossRef]
- Tarim, K.; Kilic, M.; Koseoglu, E.; Canda, A.E.; Kordan, Y.; Balbay, M.D.; Acar, O.; Esen, T. Feasibility, safety and efficacy of argon beam coagulation in robot-assisted partial nephrectomy for solid renal masses ≤ 7 cm in size. J. Robotic Surg. 2020, 13, 1–7. [Google Scholar] [CrossRef]
- Xu, W.; Qian, J.; Hou, G.; Wang, Y.; Wang, J.; Sun, T.; Ji, L.; Suo, A.; Yao, Y. A dual-targeted hyaluronic acid-gold nanorod platform with triple-stimuli responsiveness for photodynamic/photothermal therapy of breast cancer. Acta Biomater. 2018, 83, 400–413. [Google Scholar] [CrossRef]
- Wang, B.-C.; Fu, C.; Qin, L.; Zeng, X.-Y.; Liu, Q. Photodynamic therapy with methyl-5-aminolevulinate for basal cell carcinoma: A systematic review and meta-analysis. Photodiagnosis Photodyn. Ther. 2020, 29, 101667. [Google Scholar] [CrossRef] [PubMed]
- Traylor, J.; Pernik, M.; Plitt, A.; Lim, M.; Garzon-Muvdi, T. Immunotherapy for Chordoma and Chondrosarcoma: Current Evidence. Cancers 2021, 13, 2408. [Google Scholar] [CrossRef]
- Nanodoses of melatonin induces apoptosis on human breast cancer cells co-cultured with colostrum cells. Biointerface Res. Appl. Chem. 2019, 9, 4416–4423. [CrossRef]
- Zhao, X.; Wu, Q.; Gong, X.; Liu, J.; Ma, Y. Osteosarcoma: A review of current and future therapeutic approaches. Biomed. Eng. Online 2021, 20, 1–14. [Google Scholar] [CrossRef]
- Zeng, Y.; Hoque, J.; Varghese, S. Biomaterial-assisted local and systemic delivery of bioactive agents for bone repair. Acta Biomater. 2019, 93, 152–168. [Google Scholar] [CrossRef] [PubMed]
- Rotman, S.; Grijpma, D.; Richards, R.; Moriarty, F.; Eglin, D.; Guillaume, O. Drug delivery systems functionalized with bone mineral seeking agents for bone targeted therapeutics. J. Control. Release 2018, 269, 88–99. [Google Scholar] [CrossRef]
- Yang, Y.; Zhao, Z.; Xie, C.; Zhao, Y. Dual-targeting liposome modified by glutamic hexapeptide and folic acid for bone metastatic breast cancer. Chem. Phys. Lipids 2020, 228, 104882. [Google Scholar] [CrossRef]
- Wang, S.-Y.; Hu, H.-Z.; Qing, X.-C.; Zhang, Z.-C.; Shao, Z.-W. Recent advances of drug delivery nanocarriers in osteosarcoma treatment. J. Cancer 2020, 11, 69–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farooq, M.A.; Aquib; Farooq, A.; Khan, D.H.; Maviah, M.B.J.; Filli, M.S.; Kesse, S.; Boakye-Yiadom, K.O.; Mavlyanova, R.; Parveen, A.; et al. Recent progress in nanotechnology-based novel drug delivery systems in designing of cisplatin for cancer therapy: An overview. Artif. Cells Nanomed. Biotechnol. 2019, 47, 1674–1692. [Google Scholar] [CrossRef] [Green Version]
- Vinay, R.; Kusumdevi, V. Potential of targeted drug delivery system for the treatment of bone metastasis. Drug Deliv. 2014, 23, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Miller, T.; Goude, M.C.; McDevitt, T.C.; Temenoff, J.S. Molecular engineering of glycosaminoglycan chemistry for biomolecule delivery. Acta Biomater. 2013, 10, 1705–1719. [Google Scholar] [CrossRef] [Green Version]
- Shafabakhsh, R.; Yousefi, B.; Asemi, Z.; Nikfar, B.; Mansournia, M.A.; Hallajzadeh, J. Chitosan: A compound for drug delivery system in gastric cancer-a review. Carbohydr. Polym. 2020, 242, 116403. [Google Scholar] [CrossRef]
- Parhi, R. Drug delivery applications of chitin and chitosan: A review. Environ. Chem. Lett. 2020, 18, 577–594. [Google Scholar] [CrossRef]
- Tao, F.; Ma, S.; Tao, H.; Jin, L.; Luo, Y.; Zheng, J.; Xiang, W.; Deng, H. Chitosan-based drug delivery systems: From synthesis strategy to osteomyelitis treatment—A review. Carbohydr. Polym. 2020, 251, 117063. [Google Scholar] [CrossRef] [PubMed]
- Abirami, S.; Nagarajan, D.; Antony, V.S.; Mini Varsini, A.; Sugasini, A.; Anand, D.A. Extraction, charac-terization, and utilization of shrimp waste chitin derived chitosan in antimicrobial activity, seed germina-tion, preservative, and microparticle formulation. Biointerface Res. Appl. Chem. 2021, 11, 8725–8739. [Google Scholar]
- Del Prado-Audelo, M.L.; Caballero-Florán, I.H.; Sharifi-Rad, J.; Mendoza-Muñoz, N.; Torres, M.G.; Urbán-Morlán, Z.; Florán, B.; Cortes, H.; Leyva-Gómez, G. Chitosan-decorated nanoparticles for drug delivery. J. Drug Deliv. Sci. Technol. 2020, 59, 101896. [Google Scholar] [CrossRef]
- Wang, H.; Boerman, O.C.; Sariibrahimoglu, K.; Li, Y.; Jansen, J.A.; Leeuwenburgh, S.C. Comparison of micro- vs. nanostructured colloidal gelatin gels for sustained delivery of osteogenic proteins: Bone morphogenetic protein-2 and alkaline phosphatase. Biomaterials 2012, 33, 8695–8703. [Google Scholar] [CrossRef]
- Foox, M.; Zilberman, M. Drug delivery from gelatin-based systems. Expert Opin. Drug Deliv. 2015, 12, 1547–1563. [Google Scholar] [CrossRef] [PubMed]
- Geiger, M. Collagen sponges for bone regeneration with rhBMP-2. Adv. Drug Deliv. Rev. 2003, 55, 1613–1629. [Google Scholar] [CrossRef]
- Muthukumar, T.; Sreekumar, G.; Sastry, T.; Chamundeeswari, M. Collagen as a Potential Biomaterial in Biomedical Applications. Rev. Adv. Mater. Sci. 2018, 53, 29–39. [Google Scholar] [CrossRef]
- Spicer, P.P.; Mikos, A.G. Fibrin glue as a drug delivery system. J. Control. Release 2010, 148, 49–55. [Google Scholar] [CrossRef] [Green Version]
- Kolambkar, Y.M.; Dupont, K.M.; Boerckel, J.D.; Huebsch, N.; Mooney, D.J.; Hutmacher, D.W.; Guldberg, R.E. An alginate-based hybrid system for growth factor delivery in the functional repair of large bone defects. Biomaterials 2011, 32, 65–74. [Google Scholar] [CrossRef] [Green Version]
- Rahman, M.; Alrobaian, M.; Almalki, W.H.; Mahnashi, M.H.; Alyami, B.A.; Alqarni, A.O.; Alqahtani, Y.S.; Alharbi, K.S.; Alghamdi, S.; Panda, S.K.; et al. Superbranched polyglycerol nanostructures as drug delivery and theranostics tools for cancer treatment. Drug Discov. Today 2021, 26, 1006–1017. [Google Scholar] [CrossRef]
- Gadag, S.; Sinha, S.; Nayak, Y.; Garg, S.; Nayak, U.Y. Combination Therapy and Nanoparticulate Systems: Smart Approaches for the Effective Treatment of Breast Cancer. Pharmaceutics 2020, 12, 524. [Google Scholar] [CrossRef]
- Islam, T.; Felfel, R.M.; Neel, E.A.A.; Grant, D.; Ahmed, I.; Hossain, K.M.Z. Bioactive calcium phosphate–based glasses and ceramics and their biomedical applications: A review. J. Tissue Eng. 2017, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cremers, S.; Ebetino, F.; Phipps, R. On the pharmacological evaluation of bisphosphonates in humans. Bone 2020, 139, 115501. [Google Scholar] [CrossRef]
- Lin, Y.; Villacanas, M.G.; Zou, H.; Liu, H.; Carcedo, I.G.; Wu, Y.; Sun, B.; Wu, X.; Prasadam, I.; Monteiro, M.J.; et al. Calcium-bisphosphonate Nanoparticle Platform as a Prolonged Nanodrug and Bone-Targeted Delivery System for Bone Diseases and Cancers. ACS Appl. Bio. Mater. 2021, 4, 2490–2501. [Google Scholar] [CrossRef]
- Savvidou, O.D.; Bolia, I.K.; Chloros, G.D.; Papanastasiou, J.; Koutsouradis, P.; Papagelopoulos, P.J. Denosumab: Current Use in the Treatment of Primary Bone Tumors. Orthopedics 2017, 40, 204–210. [Google Scholar] [CrossRef] [Green Version]
- Vijayaraghavalu, S.; Gao, Y.; Rahman, M.; Rozic, R.; Sharifi, N.; Midura, R.J.; Labhasetwar, V. Synergistic combination treatment to break cross talk between cancer cells and bone cells to inhibit progression of bone metastasis. Biomaterials 2019, 227, 119558. [Google Scholar] [CrossRef] [PubMed]
- Gül, G.; Sendur, M.A.N.; Aksoy, S.; Sever, A.R.; Altundag, K. A comprehensive review of denosumab for bone metastasis in patients with solid tumors. Curr. Med. Res. Opin. 2015, 32, 133–145. [Google Scholar] [CrossRef]
- Lipton, A.; Fizazi, K.; Stopeck, A.; Henry, D.; Smith, M.; Shore, N.; Martin, M.; Vadhan-Raj, S.; Brown, J.; Richardson, G.; et al. Effect of denosumab versus zoledronic acid in preventing skeletal-related events in patients with bone metastases by baseline characteristics. Eur. J. Cancer 2015, 53, 75–83. [Google Scholar] [CrossRef] [Green Version]
- Zhao, P.; Li, M.; Chen, Y.; He, C.; Zhang, X.; Fan, T.; Yang, T.; Lu, Y.; Lee, R.J.; Ma, X.; et al. Selenium-doped calcium carbonate nanoparticles loaded with cisplatin enhance efficiency and reduce side effects. Int. J. Pharm. 2019, 570, 118638. [Google Scholar] [CrossRef]
- Brown, A.; Kumar, S.; Tchounwou, P.B. Cisplatin-Based Chemotherapy of Human Cancers. J. Cancer Sci. Ther. 2019, 11, 2148661. [Google Scholar]
- Ferrari, S.; Bielack, S.S.; Smeland, S.; Longhi, A.; Egerer, G.; Hall, K.S.; Donati, D.; Kevric, M.; Brosjö, O.; Comandone, A.; et al. EURO-B.O.S.S.: A European study on chemotherapy in bone-sarcoma patients aged over 40: Outcome in primary high-grade osteosarcoma. Tumori J. 2018, 104, 30–36. [Google Scholar] [CrossRef]
- Ferreira, N.H.; Furtado, R.A.; Ribeiro, A.B.; Oliveira, P.; Ozelin, S.D.; de Souza, L.D.R.; Neto, F.R.; Miura, B.A.; Magalhães, G.M.; Nassar, E.J.; et al. Europium(III)-doped yttrium vanadate nanoparticles reduce the toxicity of cisplatin. J. Inorg. Biochem. 2018, 182, 9–17. [Google Scholar] [CrossRef]
- Salerno, M.; Cenni, E.; Fotia, C.; Avnet, S.; Granchi, D.; Castelli, F.; Micieli, D.; Pignatello, R.; Capulli, M.; Rucci, N.; et al. Bone-Targeted Doxorubicin-Loaded Nanoparticles as a Tool for the Treatment of Skeletal Metastases. Curr. Cancer Drug Targets 2010, 10, 649–659. [Google Scholar] [CrossRef]
- Tan, M.L.; Friedhuber, A.M.; Dunstan, D.E.; Choong, P.F.; Dass, C.R. The performance of doxorubicin encapsulated in chitosan–dextran sulphate microparticles in an osteosarcoma model. Biomaterials 2010, 31, 541–551. [Google Scholar] [CrossRef]
- Haghiralsadat, B.F.; Naderinezhad, S.; Amoabediny, G.; Montazeri, F.; Zandieh Doulabi, B. Evaluation of the effects of surface charge on cytotoxicity of liposomal Doxorubicin on bone cancer cell line (Osteosar-coma). Daneshvar Med. 2020, 25, 19–26. [Google Scholar]
- Alexandrino, E.M.; Ritz, S.; Marsico, F.; Baier, G.; Mailänder, V.; Landfester, K.; Wurm, F.R. Paclitax-el-loaded polyphosphate nanoparticles: A potential strategy for bone cancer treatment. J. Mater. Chem. B 2014, 2, 1298–1306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamashita, S.; Katsumi, H.; Hibino, N.; Isobe, Y.; Yagi, Y.; Tanaka, Y.; Yamada, S.; Naito, C.; Yamamoto, A. Development of PEGylated aspartic acid-modified liposome as a bone-targeting carrier for the delivery of paclitaxel and treatment of bone metastasis. Biomaterials 2018, 154, 74–85. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.S.; Haney, M.J.; Zhao, Y.; Mahajan, V.; Deygen, I.; Klyachko, N.L.; Inskoe, E.; Piroyan, A.; Sokolsky, M.; Okolie, O.; et al. Development of exosome-encapsulated paclitaxel to overcome MDR in cancer cells. Nanomed. Nanotechnol. Biol. Med. 2015, 12, 655–664. [Google Scholar] [CrossRef] [Green Version]
- Zaheer, U.; Hassain, N.A.; Banu, S.; Mathew, S. Oncolytic Viruses as Nanomedicines against the Tumor Microenvironment. Biointerface Res. Appl. Chem. 2021, 11, 14825–14852. [Google Scholar] [CrossRef]
- Nassireslami, E.; Motififard, M.; Kamyab Moghadas, B.; Hami, Z.; Jasemi, A.; Lachiyani, A.; Shokrani Foroushani, R.; Saber-Samandari, S.; Khandan, A. Potential of magnetite nanoparticles with biopolymers loaded with gentamicin drug for bone cancer treatment. J. Nanoanal. 2020. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, H.; Lin, K.; Ying, T.; Huang, Q.; Cai, X.; Xiao, J.; Zhang, Q.; Cheng, Y. Breaking the vicious cycle between tumor cell proliferation and bone resorption by chloroquine-loaded and bone-targeted polydopamine nanoparticles. Sci. China Mater. 2020, 64, 474–487. [Google Scholar] [CrossRef]
- Zhang, M.; Hagan, C.T.; Foley, H.; Tian, X.; Yang, F.; Au, K.M.; Mi, Y.; Medik, Y.; Roche, K.; Wagner, K.; et al. Co-delivery of etoposide and cisplatin in dual-drug loaded nanoparticles synergistically improves chemoradiotherapy in non-small cell lung cancer models. Acta Biomater. 2021, 124, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Miodragovic, D.; Swindell, E.P.; Waxali, Z.S.; Bogachkov, A.; O’Halloran, T.V. Beyond cisplatin: Combination therapy with arsenic trioxide. Inorg. Chim. Acta 2019, 496, 119030. [Google Scholar] [CrossRef] [PubMed]
- Yi, X.; Lian, X.; Dong, J.; Wan, Z.; Xia, C.; Song, X.; Fu, Y.; Gong, T.; Zhang, Z. Co-delivery of Pirarubicin and Paclitaxel by Human Serum Albumin Nanoparticles to Enhance Antitumor Effect and Reduce Systemic Toxicity in Breast Cancers. Mol. Pharm. 2015, 12, 4085–4098. [Google Scholar] [CrossRef] [PubMed]
- Webster, T.J.; Sun, L.; Chang, K. Short communication: Selective cytotoxicity of curcumin on osteosarcoma cells compared to healthy osteoblasts. Int. J. Nanomed. 2014, 9, 461–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, B.; Yang, J.-Z.; Wang, L.-F.; Zhang, Y.-J.; Lin, X.-J. Ifosfamide-loaded poly (lactic-co-glycolic acid) PLGA-dextran polymeric nanoparticles to improve the antitumor efficacy in Osteosarcoma. BMC Cancer 2015, 15, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prasad, S.R.; Jayakrishnan, A.; Kumar, T.S. Hydroxyapatite-poly(vinyl alcohol) core-shell nanoparticles for dual delivery of methotrexate and gemcitabine for bone cancer treatment. J. Drug Deliv. Sci. Technol. 2019, 51, 629–638. [Google Scholar] [CrossRef]
- Hingorani, P.; Sampson, V.; Lettieri, C.; Kolb, E.A. Oncolytic Viruses for Potential Osteosarcoma Therapy. Curr. Adv. Osteosarcoma 2014, 804, 259–283. [Google Scholar] [CrossRef]
- Martinez-Quintanilla, J.; Seah, I.; Chua, M.; Shah, K. Oncolytic viruses: Overcoming translational challenges. J. Clin. Investig. 2019, 129, 1407–1418. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Moure, M.; Martinez-Velez, N.; Patiño-García, A.; Alonso, M.M. Oncolytic adenoviruses as a therapeutic approach for osteosarcoma: A new hope. J. Bone Oncol. 2016, 9, 41–47. [Google Scholar] [CrossRef]
- Witlox, A.M.; Van Beusechem, V.W.; Molenaar, B.; Bras, H.; Schaap, G.R.; Alemany, R.; Curiel, D.T.; Pinedo, H.M.; Wuisman, P.I.J.M.; Gerritsen, W.R. Conditionally Replicative Adenovirus with Tropism Expanded towards Integrins Inhibits Osteosarcoma Tumor Growth in Vitro and in Vivo. Clin. Cancer Res. 2004, 10, 61–67. [Google Scholar] [CrossRef] [Green Version]
- Graat, H.C.; Van Beusechem, V.W.; Schagen, F.H.; Witlox, M.A.; Kleinerman, E.S.; Helder, M.N.; Gerritsen, W.R.; Kaspers, G.J.; Wuisman, P.I. Intravenous administration of the conditionally replicative adenovirus Ad5-Δ24RGD induces regression of osteosarcoma lung metastases. Mol. Cancer 2008, 7, 9. [Google Scholar] [CrossRef] [Green Version]
- Wedekind, M.F.; Cripe, T.P. Oncolytic Viruses and Their Potential as a Therapeutic Opportunity in Oste-osarcoma. Adv. Exp. Med. Biol. 2020, 1258, 77–89. [Google Scholar] [CrossRef] [PubMed]
- Howard, F.; Muthana, M. Designer nanocarriers for navigating the systemic delivery of oncolytic viruses. Nanomedicine 2020, 15, 93–110. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, P.-H.; Kim, S.W.; Yun, C.-O. Enhancing the therapeutic efficacy of adenovirus in combination with biomaterials. Biomaterials 2012, 33, 1838–1850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iram, S.; Zahera, M.; Khan, S.; Khan, I.; Syed, A.; Ansary, A.A.; Ameen, F.; Shair, O.H.; Khan, M.S. Gold nanoconjugates reinforce the potency of conjugated cisplatin and doxorubicin. Colloids Surf. B Biointerfaces 2017, 160, 254–264. [Google Scholar] [CrossRef]
- Shibuya, N.; Jupiter, D.C. Bone Graft Substitute. Clin. Podiatr. Med. Surg. 2015, 32, 21–34. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, K.; Miyamoto, Y.; Tsuchiya, A.; Hayashi, K.; Tsuru, K.; Ohe, G. Physical and Histological Comparison of Hydroxyapatite, Carbonate Apatite, and β-Tricalcium Phosphate Bone Substitutes. Materials 2018, 11, 1993. [Google Scholar] [CrossRef] [Green Version]
- Diomede, F.; Marconi, G.D.; Fonticoli, L.; Pizzicanella, J.; Merciaro, I.; Bramanti, P.; Mazzon, E.; Trubiani, O. Functional Relationship between Osteogenesis and Angiogenesis in Tissue Regeneration. Int. J. Mol. Sci. 2020, 21, 3242. [Google Scholar] [CrossRef] [PubMed]
- Åberg, M.; Rydholm, A.; Holmberg, J.; Wleslander, J.B. Reconstruction with a free vascularized fibular graft for malignant bone tumor. Acta Orthop. Scand. 1988, 59, 430–437. [Google Scholar] [CrossRef] [PubMed]
- Bretschneider, H.; Quade, M.; Lode, A.; Gelinsky, M.; Rammelt, S.; Vater, C. Chemotactic and Angiogenic Potential of Mineralized Collagen Scaffolds Functionalized with Naturally Occurring Bioactive Factor Mixtures to Stimulate Bone Regeneration. Int. J. Mol. Sci. 2021, 22, 5836. [Google Scholar] [CrossRef]
- Offner, D.; De Grado, G.F.; Meisels, I.; Pijnenburg, L.; Fioretti, F.; Benkirane-Jessel, N.; Musset, A.-M. Bone Grafts, Bone Substitutes and Regenerative Medicine Acceptance for the Management of Bone Defects among French Population: Issues about Ethics, Religion or Fear? Cell Med. 2019, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aoki, K.; Saito, N. Biodegradable Polymers as Drug Delivery Systems for Bone Regeneration. Pharmaceutics 2020, 12, 95. [Google Scholar] [CrossRef] [Green Version]
- Alho, A.; Karaharju, E.O.; Korkala, O.; Laasonen, E.M.; Holmström, T.; Müller, C. Allogeneic grafts for bone tumor: 21 cases of osteoarticular and segmental grafts. Acta Orthop. Scand. 1989, 60, 143–153. [Google Scholar] [CrossRef] [Green Version]
- Parikh, S.N. Bone Graft Substitutes in Modern Orthopedics. Orthopedics 2002, 25, 1301–1309. [Google Scholar] [CrossRef]
- De Grado, G.F.; Keller, L.; Idoux-Gillet, Y.; Wagner, Q.; Musset, A.-M.; Benkirane-Jessel, N.; Bornert, F.; Offner, D. Bone substitutes: A review of their characteristics, clinical use, and perspectives for large bone defects management. J. Tissue Eng. 2018, 9. [Google Scholar] [CrossRef] [Green Version]
- Campana, V.; Milano, G.; Pagano, E.D.; Barba, M.; Cicione, C.; Salonna, G.; Lattanzi, W.; Logroscino, G. Bone substitutes in orthopaedic surgery: From basic science to clinical practice. J. Mater. Sci. Mater. Med. 2014, 25, 2445–2461. [Google Scholar] [CrossRef]
- Almutairi, A.S. A descriptive analysis of patient’s preferences in bone graft therapy in dentistry. Int. J. Health. Sci. 2019, 13, 24–28. [Google Scholar]
- Güngörmüş, Z.; Güngörmüş, M. Effect of Religious Belief on Selecting of Graft Materials Used in Oral and Maxillofacial Surgery. J. Oral Maxillofac. Surg. 2017, 75, 2347–2353. [Google Scholar] [CrossRef] [PubMed]
- Romanos, G.E.; Romanos, E.B.; Alqahtani, F.; Alqahtani, M.; Javed, F. “Religious Belief”: An Undervalued Ethical Inclusion Criterion for Clinical Trials on Bone Grafting Procedures. J. Relig. Health 2019, 59, 2928–2934. [Google Scholar] [CrossRef]
- Barbeck, M.; Schröder, M.-L.; Alkildani, S.; Jung, O.; Unger, R. Exploring the Biomaterial-Induced Secretome: Physical Bone Substitute Characteristics Influence the Cytokine Expression of Macrophages. Int. J. Mol. Sci. 2021, 22, 4442. [Google Scholar] [CrossRef]
- Tsai, S.-W.; Huang, S.-S.; Yu, W.-X.; Hsu, Y.-W.; Hsu, F.-Y. Collagen Scaffolds Containing Hydroxyapatite-CaO Fiber Fragments for Bone Tissue Engineering. Polymers 2020, 12, 1174. [Google Scholar] [CrossRef] [PubMed]
- Brunello, G.; Panda, S.; Schiavon, L.; Sivolella, S.; Biasetto, L.; Del Fabbro, M. The Impact of Bioceramic Scaffolds on Bone Regeneration in Preclinical In Vivo Studies: A Systematic Review. Materials 2020, 13, 1500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bekmez, S.; Ayvaz, M.; Yucekul, A.; Tokgozoglu, M. Modular cementless prosthetic reconstruction after resection of lower extremity malignant tumor. Acta Orthop. Traumatol. Turc. 2016, 50, 674–680. [Google Scholar] [CrossRef]
- Verron, E.; Bouler, J.-M.; Guicheux, J. Controlling the biological function of calcium phosphate bone substitutes with drugs. Acta Biomater. 2012, 8, 3541–3551. [Google Scholar] [CrossRef]
- Gomes, S.; Vichery, C.; Descamps, S.; Martinez, H.; Kaur, A.; Jacobs, A.; Nedelec, J.-M.; Renaudin, G. Cu-doping of calcium phosphate bioceramics: From mechanism to the control of cytotoxicity. Acta Biomater. 2018, 65, 462–474. [Google Scholar] [CrossRef]
- Vincent, M.; Duval, R.; Hartemann, P.; Engels-Deutsch, M. Contact killing and antimicrobial properties of copper. J. Appl. Microbiol. 2018, 124, 1032–1046. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Ho, J.; Ooi, C.P. Antibacterial efficacy and cytotoxicity studies of copper (II) and titanium (IV) substituted hydroxyapatite nanoparticles. Mater. Sci. Eng. C 2010, 30, 1137–1144. [Google Scholar] [CrossRef]
- Adzila, S.; Murad, M.; Sopyan, I. Doping Metal into Calcium Phosphate Phase for Better Performance of Bone Implant Materials. Recent Pat. Mater. Sci. 2012, 5, 18–47. [Google Scholar] [CrossRef]
- Pandya, H.M.; Anitha, P.; Mathammal, R.; Kalaiselvi, V. Incorporation and in vitro application of hy-droxyapatite with silver and titanium dopants synthesized by wet chemical method. J. Environ. Nanotechnol. 2017, 6, 42–46. [Google Scholar]
- Li, G.; Zhang, N.; Zhao, S.; Zhang, K.; Li, X.; Jing, A.; Liu, X.; Zhang, T. Fe-doped brushite bone cements with antibacterial property. Mater. Lett. 2018, 215, 27–30. [Google Scholar] [CrossRef]
- Schatkoski, V.M.; Montanheiro, T.L.D.A.; de Menezes, B.R.C.; Pereira, R.M.; Rodrigues, K.F.; Ribas, R.G.; da Silva, D.M.; Thim, G.P. Current advances concerning the most cited metal ions doped bioceramics and silicate-based bioactive glasses for bone tissue engineering. Ceram. Int. 2020, 47, 2999–3012. [Google Scholar] [CrossRef]
- Alioui, H.; Bouras, O.; Bollinger, J.-C. Toward an efficient antibacterial agent: Zn- and Mg-doped hydroxyapatite nanopowders. J. Environ. Sci. Health Part A 2019, 54, 315–327. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharjee, A.; Gupta, A.; Verma, M.; Murugan, P.A.; Sengupta, P.; Matheshwaran, S.; Manna, I.; Balani, K. Site-specific antibacterial efficacy and cyto/hemo-compatibility of zinc substituted hydroxyapatite. Ceram. Int. 2019, 45, 12225–12233. [Google Scholar] [CrossRef]
- Yuan, J.; Wang, B.; Han, C.; Huang, X.; Xiao, H.; Lu, X.; Lu, J.; Zhang, D.; Xue, F.; Xie, Y. Nanosized-Ag-doped porous β-tricalcium phosphate for biological applications. Mater. Sci. Eng. C 2020, 114, 111037. [Google Scholar] [CrossRef]
- Chou, Y.-J.; Ningsih, H.S.; Shih, S.-J. Preparation, characterization and investigation of antibacterial silver-zinc co-doped β-tricalcium phosphate by spray pyrolysis. Ceram. Int. 2020, 46, 16708–16715. [Google Scholar] [CrossRef]
- Galli, C.; Parisi, L.; Elviri, L.; Bianchera, A.; Smerieri, A.; Lagonegro, P.; Lumetti, S.; Manfredi, E.; Bettini, R.; Macaluso, G.M. Chitosan scaffold modified with D-(+) raffinose and enriched with thiol-modified gela-tin for improved osteoblast adhesion. Biomed. Mater. 2016, 11, 015004. [Google Scholar] [CrossRef] [Green Version]
- Cai, Y.; Tong, S.; Zhang, R.; Zhu, T.; Wang, X. In vitro evaluation of a bone morphogenetic protein-2 nanometer hydroxyapatite collagen scaffold for bone regeneration. Mol. Med. Rep. 2018, 17, 5830–5836. [Google Scholar] [CrossRef] [PubMed]
- Abdelghany, A.M.; Meikhail, M.S.; Hegazy, E.; Badr, S.I.; Agag, D.A. Synthesis of borate modified bioac-tive glass scaffold using PVP burning-out method for bone tissue replacement. Biointerface Res. Appl. Chem. 2019, 9, 4044–4049. [Google Scholar]
- Słota, D.; Głąb, M.; Tyliszczak, B.; Douglas, T.; Rudnicka, K.; Miernik, K.; Urbaniak, M.M.; Rusek-Wala, P.; Sobczak-Kupiec, A. Composites Based on Hydroxyapatite and Whey Protein Isolate for Applications in Bone Regeneration. Materials 2021, 14, 2317. [Google Scholar] [CrossRef]
- Ślósarczyk, A.; Czechowska, J.; Cichoń, E.; Zima, A. New Hybrid Bioactive Composites for Bone Substitution. Processes 2020, 8, 335. [Google Scholar] [CrossRef] [Green Version]
- Siddiqui, H.A.; Pickering, K.L.; Mucalo, M.R. A Review on the Use of Hydroxyapatite-Carbonaceous Structure Composites in Bone Replacement Materials for Strengthening Purposes. Materials 2018, 11, 1813. [Google Scholar] [CrossRef] [Green Version]
- Senra, M.R.; Marques, M.D.F.V. Synthetic Polymeric Materials for Bone Replacement. J. Compos. Sci. 2020, 4, 191. [Google Scholar] [CrossRef]
- Sansone, V. The effects on bone cells of metal ions released from orthopaedic implants. A review. Clin. Cases Miner. Bone Metab. 2013, 10, 34–40. [Google Scholar] [CrossRef]
- Koolen, M.; Yavari, S.A.; Lietaert, K.; Wauthle, R.; Zadpoor, A.A.; Weinans, H. Bone Regeneration in Critical-Sized Bone Defects Treated with Additively Manufactured Porous Metallic Biomaterials: The Effects of Inelastic Mechanical Properties. Materials 2020, 13, 1992. [Google Scholar] [CrossRef]
- Bobbert, F.; Lietaert, K.; Eftekhari, A.A.; Pouran, B.; Ahmadi, S.; Weinans, H.; Zadpoor, A.A. Additively manufactured metallic porous biomaterials based on minimal surfaces: A unique combination of topological, mechanical, and mass transport properties. Acta Biomater. 2017, 53, 572–584. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Xu, S.; Zhou, S.; Xu, W.; Leary, M.; Choong, P.; Qian, M.; Brandt, M.; Xie, Y.M. Topological design and additive manufacturing of porous metals for bone scaffolds and orthopaedic implants: A review. Biomaterials 2016, 83, 127–141. [Google Scholar] [CrossRef]
- Honda, M.; Matsumoto, M.; Aizawa, M. Potential Application of Protamine for Antimicrobial Biomaterials in Bone Tissue Engineering. Int. J. Mol. Sci. 2020, 21, 4368. [Google Scholar] [CrossRef]
- Lee, S.J.; Lee, D.; Yoon, T.R.; Kim, H.K.; Jo, H.H.; Park, J.S.; Lee, J.H.; Kim, W.D.; Kwon, I.K.; A Park, S. Surface modification of 3D-printed porous scaffolds via mussel-inspired polydopamine and effective immobilization of rhBMP-2 to promote osteogenic differentiation for bone tissue engineering. Acta Biomater. 2016, 40, 182–191. [Google Scholar] [CrossRef] [PubMed]
- De Witte, T.-M.; Fratila-Apachitei, L.E.; Zadpoor, A.A.; Peppas, N.A. Bone tissue engineering via growth factor delivery: From scaffolds to complex matrices. Regen. Biomater. 2018, 5, 197–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, H.; Feng, C.; Chang, J.; Wu, C. 3D-printed bioceramic scaffolds: From bone tissue engineering to tumor therapy. Acta Biomater. 2018, 79, 37–59. [Google Scholar] [CrossRef] [PubMed]
- Martin, V.; Bettencourt, A. Bone regeneration: Biomaterials as local delivery systems with improved osteoinductive properties. Mater. Sci. Eng. C 2018, 82, 363–371. [Google Scholar] [CrossRef]
- Mondal, S.; Dorozhkin, S.V.; Pal, U. Recent progress on fabrication and drug delivery applications of nanostructured hydroxyapatite. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2017, 10, e1504. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Bone Metastasis | Radiographic Appearance | Manifestation | Types of Cancer in Which It Appears | Producing Factors | Refs. |
|---|---|---|---|---|---|
| Osteolytic | Radiolucent areas located in the skull and proximal ends of long bones | Destruction of normal bone resulting in complications of bone pain, fracture, hypercalcemia, and nerve compression syndromes | Breast cancer Multiple myeloma Renal cell carcinoma Melanoma Non-small cell lung cancer Non-Hodgkin lymphoma Thyroid cancer Langerhans-cell histiocytosis | Parathyroid hormone-related protein (PTHrP) Interleukin (IL)-11 IL-8 IL-6 Receptor activator of nuclear factor-κ B ligand (RANKL) Bone-derived transforming growth factor-β (TGF-β) Connective tissue growth factor (CTGF) | [33,35,37,38,39] |
| Osteoblastic (or osteosclerotic) | Dense areas located to the axial skeleton and, particularly, in vertebral bodies and pelvis | Deposition of new bone with dysregulated bone resorption and bone formation | Prostate cancer Carcinoid Small cell lung cancer Hodgkin lymphoma Medulloblastoma | Platelet-derived growth factor (PDGF) Insulin-like growth factors Adrenomedullin Vasoactive peptide ET-1 PTHrP fragments | [33,35,38,39] |
| Mixed | Fuzzy aspect; a sclerotic rim of reactive bone, starting at the periphery and eventually involving the center of osteolytic lesions with continued healing is observed | Association of both osteolytic and osteoblastic lesions, or osteolytic and osteoblastic components in an individual metastasis | Breast cancer Gastrointestinal cancers Squamous cancers | Factors of both osteolytic and osteoblastic tumors | [33,35,40] |
| Clinicaltrails.Gov Identifier | Official Title | Purpose of the Study | (Estimated) Primary Completion Date |
|---|---|---|---|
| NCT01117246 | “Pilot Study for the Treatment of Bone Metastases by High Intensity Focused Ultrasound Guided by MRI to Perform Pain Palliation” | Confirm the safety and effectiveness of MR-guided HIFU for pain palliation of skeletal metastases | July 2011 |
| NCT01765907 | “Antalgic Treatment of Painful Bone Metastases by US-guided High Intensity Focused Ultrasound (HIFU)” | Assess safety, including adverse and serious adverse events, local and systemic tolerance of HIFU in patients with bone metastasis | March 2014 |
| NCT01964677 | “Magnetic Resonance-Guided High Intensity Focused Ultrasound for Palliation of Painful Skeletal Metastases—a Multicenter Study” | Evaluate the effectiveness of Philips Sonalleve MR-HIFU device for the palliation of pain in patients with bone metastases | 14 November 2016 |
| NCT02618369 | “Magnetic Resonance-Guided High Intensity Focused Ultrasound for Pain Management of Osteoid Osteoma and Benign Bone Tumors in Children and Young Adults” | Determine if MR-guided HIFU is safe and effective for alleviating pain associated with osteoid osteoma and other benign bone tumors in pediatric patients and adults (up 40 years old) | April 2018 |
| NCT02349971 | “Safety and Feasibility of MR-Guided High Intensity Focused Ultrasound (MR-HIFU) Ablation of Osteoid Osteoma in Children” | Examine the feasibility and efficacy of using MR-HIFU to ablate osteoid osteoma in children and young adults | 3 October 2020 |
| NCT03106675 | “MR Imaging- Guided High Intensity Focused Ultrasound (HIFU) Therapy of Bone Metastases” | Evaluate the effectiveness of MR-guided HIFU in treating metastatic bone tumors | 31 December 2021 |
| NCT02076906 | “Safety and Feasibility Study of Using MR-guided High Intensity Focused Ultrasound (HIFU) for the Ablation of Relapsed or Refractory Pediatric Solid Tumors” | Determine if MR-guided HIFU is safe and feasible for children, adolescents, and young adults with refractory or relapsed solid tumors | 30 January 2022 |
| NCT04658771 | “Pivotal / Phase II Clinical Trial of Magnetic Resonance-Guided Focused Ultrasound (MR-HIFU) Treatment of Painful Osteoid Osteoma in Children and Young Adults” | Determine treatment safety and efficacy of MR-HIFU ablation of painful osteoid osteoma in children and young adults | 30 January 2023 |
| NCT04307914 | “Focused Ultrasound and RadioTHERapy for Noninvasive Palliative Pain Treatment in Patients with Bone Metastases” | Evaluate the effectiveness and cost effectiveness of MR-HIFU (alone or in combination with EBRT) compared to EBRT alone | 1 January 2024 |
| Clinicaltrails.Gov Identifier | Official Title | Purpose of the Study | (Estimated) Primary Completion Date |
|---|---|---|---|
| NCT02423928 | “A Phase I Clinical Trial of Combined Cryotherapy and Intra-tumoral Immunotherapy with Autologous Immature Dendritic Cells in Men with Castration Resistant Prostatic Cancer and Metastases to Lymph Nodes and/or Bone Pre or Post Chemotherapy” | Evaluate the combined anti-cancer therapy response in patients with invasive castration resistant prostate cancer and radiologically verified metastases | 16 August 2019 |
| NCT03996473 | “An Open-label, Multicenter, Phase 1/2 Study of Radium-223 Dichloride in Combination with Pembrolizumab in Participants with Stage IV Non-small Cell Lung Cancer” | Determine the safety and efficacy of the combination of radium-223 dichloride and pembrolizumab in patients with stage IV non-small cell lung cancer (NSCLC) with bone metastases who either have not received any systemic therapy for their advanced disease or have progressed on prior immunologic checkpoint blockade with antibodies against the programmed cell death protein-(ligand) 1 (PD-1/PD-L1) | 14 April 2021 |
| NCT03406858 | “Phase II Trial of Immune Checkpoint Inhibitor with Anti-CD3 x Anti-HER2 Bispecific Antibody Armed Activated T Cells in Metastatic Castrate Resistant Prostate Cancer” | Study how well pembrolizumab and HER2Bi-armed activated T cells work in treating castration resistant prostate cancer that has spread to other places in the body, including bone | 1 December 2021 |
| NCT04516122 | “Bone Loss in Cancer Survivors Receiving Adjuvant Immune Checkpoint Inhibitor Therapy” | Investigate the bone-related side effects caused by immunotherapy drugs | 31 July 2022 |
| Bone Substitute | Neobone® (HAp) | Cytrans® (CO3Ap) | Cerasorb® (β-TCP) | |
|---|---|---|---|---|
| Property | ||||
| Crystallite size (nm) | 75.4 ± 0.9 | 30.8 ± 0.8 | 78.5 ± 7.5 | |
| Specific surface area (m3/g) | 1.0 | 18.2 | 0.06 | |
| CO3 content (%) | - | 11.9 | - | |
| Bulk density (g/cm3) | 0.47 ± 0.02 | 0.99 ± 0.03 | 0.72 ± 0.03 | |
| Porosity (%) | 85.1 ± 0.5 | 68.7 ± 0.9 | 76.4 ± 0.8 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bădilă, A.E.; Rădulescu, D.M.; Niculescu, A.-G.; Grumezescu, A.M.; Rădulescu, M.; Rădulescu, A.R. Recent Advances in the Treatment of Bone Metastases and Primary Bone Tumors: An Up-to-Date Review. Cancers 2021, 13, 4229. https://doi.org/10.3390/cancers13164229
Bădilă AE, Rădulescu DM, Niculescu A-G, Grumezescu AM, Rădulescu M, Rădulescu AR. Recent Advances in the Treatment of Bone Metastases and Primary Bone Tumors: An Up-to-Date Review. Cancers. 2021; 13(16):4229. https://doi.org/10.3390/cancers13164229
Chicago/Turabian StyleBădilă, Adrian Emilian, Dragoș Mihai Rădulescu, Adelina-Gabriela Niculescu, Alexandru Mihai Grumezescu, Marius Rădulescu, and Adrian Radu Rădulescu. 2021. "Recent Advances in the Treatment of Bone Metastases and Primary Bone Tumors: An Up-to-Date Review" Cancers 13, no. 16: 4229. https://doi.org/10.3390/cancers13164229