
Gallbladder Cancer: Current Insights in Genetic Alterations and Their Possible Therapeutic Implications

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction
2.4. Therapeutic Implications
3. Results
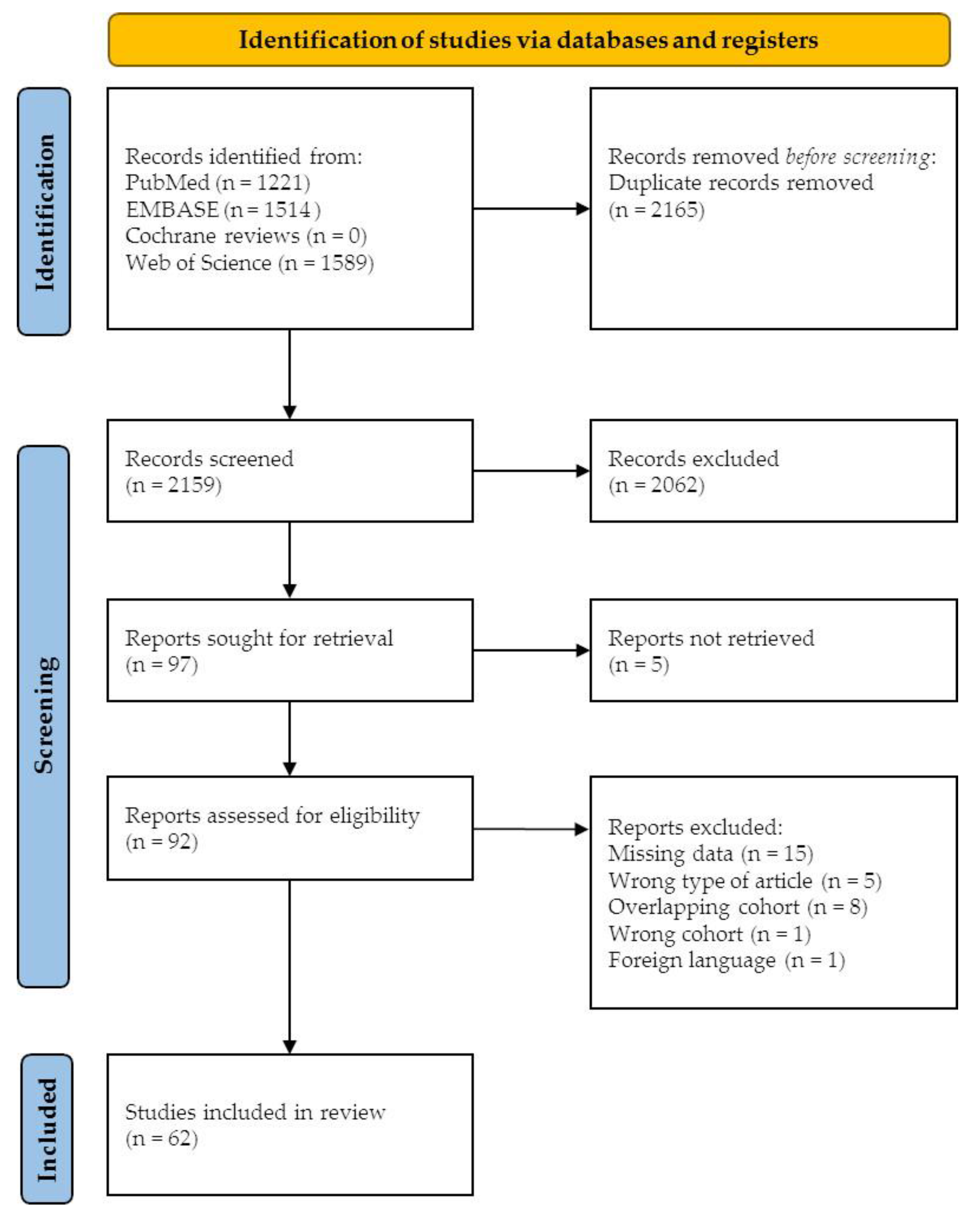
3.1. Literature Search and Study Selection
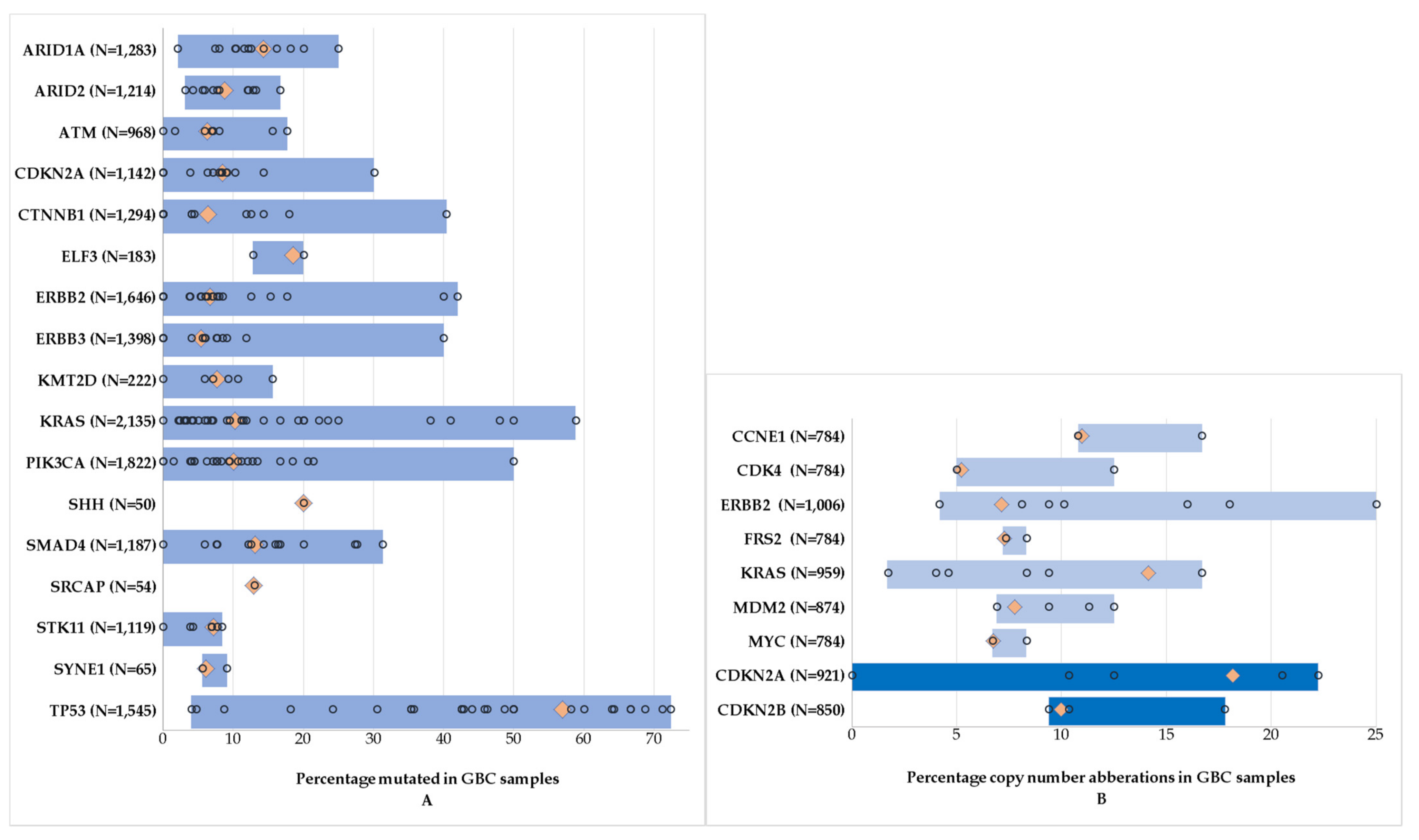
3.2. Most Frequently Mutated Genes
3.3. Amplifications and Deletions
3.4. Tumor Mutational Burden (TMB)
3.5. Microsatellite Instability (MSI)
3.6. Possible Therapeutic Implications
3.6.1. Targetable Alterations in Other Malignancies
3.6.2. Clinical Trials
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Database | |||
|---|---|---|---|
| PubMed | EMBASE | Cochrane Reviews | Web of Science |
| (“Gallbladder Neoplasms”[Mesh] OR (gallbladder[tiab] AND (neoplasm * [tiab] OR cancer * [tiab] OR lesion * [tiab] OR tumor* [tiab] OR tumour * [tiab] OR carcinom * [tiab] OR malignan * [tiab]))) AND (“Mutation”[Mesh] OR “Epigenesis, Genetic”[Mesh] OR “Genome”[Mesh] OR molecular[tiab] OR gene[tiab] OR genes[tiab] OR genetic * [tiab] OR genom * [tiab] OR sequenc * [tiab] OR mutation*[tiab] OR exome * [tiab]) | (‘gallbladder cancer’/exp OR (gallbladder AND (neoplasm * OR cancer* OR tumor * OR tumour * OR carcinom * OR malignan *)):ab,ti,kw) AND (‘gene mutation’/exp OR ‘gene sequence’/exp OR (exome * OR molecular OR gene OR genes OR genetic * OR genom * OR sequenc * OR mutation *):ab,ti,kw) | (gallbladder AND (neoplasm * OR cancer * OR tumor * OR tumour * OR carcinom * OR malignan *)) AND (molecular OR gene OR genes OR genetic * OR genom * OR sequenc * OR mutation * OR exome *) | (gallbladder AND (neoplasm * OR cancer * OR tumor * OR tumour * OR carcinom * OR malignan *)) AND (exome * OR molecular OR gene OR genes OR genetic * OR genom * OR sequenc * OR mutation *) |
| Gene | WA | N | Frequency | Methods | Histology | Population | Author | Year | Ref. |
|---|---|---|---|---|---|---|---|---|---|
| ARID1A | 14.3% | 1/5 | 20% | WES | AC | Japan | Akita | 2019 | [48] |
| 2/14 | 14% | TS | N.A. | China | Li | 2017 | [44] | ||
| 2/47 | 4% | WES | AC | China | Yang | 2021 | [56] | ||
| 2/25 | 8% | targeted exome sequencing | N.A. | Korea | Chae | 2019 | [79] | ||
| 3/24 | 13% | NGS | N.A. | America | Okamura | 2021 | [27] | ||
| 3/26 | 12% | NGS | N.A. | Italy | Simbolo | 2014 | [61] | ||
| 4/54 | 7% | NGS | AC | Greece | Papadopoulou | 2018 | [40] | ||
| 4/39 | 10% | WES/WGS | N.A. | Japan | Ebata | 2021 | [57] | ||
| 15/144 | 10% | WES | AC | India, Korea, Chile | Pandey | 2020 | [46] | ||
| 7/58 | 12% | ultra-deep targeted NGS | AC | China | Lin | 2019 | [70] | ||
| 8/32 | 25% | targeted NGS | AC | Chile, Japan | Narayan | 2019 | [73] | ||
| 10/55 | 18% | NGS | N.A. | America | Javle | 2016 | [23] | ||
| 123/760 | 16% | NGS | N.A. | America | Abdel-Wahab | 2020 | [19] | ||
| ARID2 | 8.8% | 1/32 | 3% | targeted NGS | AC | Chile, Japan | Narayan | 2019 | [73] |
| 1/17 | 6% | WES | N.A. | India | Iyer | 2019 | [29] | ||
| 1/14 | 7% | TS | N.A. | China | Li | 2017 | [44] | ||
| 1/24 | 4% | NGS | N.A. | America | Okamura | 2021 | [27] | ||
| 3/25 | 12% | targeted exome sequencing | N.A. | Korea | Chae | 2019 | [79] | ||
| 3/54 | 6% | NGS | AC | Greece | Papadopoulou | 2018 | [40] | ||
| 3/39 | 8% | WES/WGS | N.A. | Japan | Ebata | 2021 | [57] | ||
| 19/144 | 13% | WES | AC | India, Korea, Chile | Pandey | 2020 | [46] | ||
| 2/12 | 17% | NGS | N.A. | China | Li | 2020 | [47] | ||
| 7/58 | 12% | ultra-deep targeted NGS | AC | China | Lin | 2019 | [70] | ||
| 8/47 | 17% | WES | AC | China | Yang | 2021 | [56] | ||
| 61/760 | 8% | NGS | N.A. | America | Abdel-Wahab | 2020 | [19] | ||
| ATM | 6.3% | 0/4 | 0% | TS | AC | Korea | Yoo | 2016 | [37] |
| 1/14 | 7% | NGS | N.A. | Japan | Noguchi | 2017 | [32] | ||
| 1/58 | 2% | NGS | AC | America | Maynard | 2020 | [41] | ||
| 2/25 | 8% | targeted exome sequencing | N.A. | Korea | Chae | 2019 | [79] | ||
| 5/32 | 16% | targeted NGS | AC | Chile, Japan | Narayan | 2019 | [73] | ||
| 3/17 | 18% | WES | N.A. | India | Iyer | 2019 | [29] | ||
| 4/58 | 7% | ultra-deep targeted NGS | AC | China | Lin | 2019 | [70] | ||
| 45/760 | 6% | NGS | N.A. | America | Abdel-Wahab | 2020 | [19] | ||
| CDKN2A | 8.5% | 0/24 | 0% | NGS | N.A. | America | Okamura | 2021 | [27] |
| 0/5 | 0% | WES | AC | Japan | Akita | 2019 | [48] | ||
| 0/4 | 0% | TS | AC | Korea | Yoo | 2016 | [37] | ||
| 1/11 | 9% | ultra-deep targeted NGS | N.A. | India | Yadav | 2017 | [77] | ||
| 1/26 | 4% | NGS | N.A. | Italy | Simbolo | 2014 | [61] | ||
| 1/14 | 7% | NGS | N.A. | Japan | Noguchi | 2017 | [32] | ||
| 13/144 | 9% | WES | AC | India, Korea, Chile | Pandey | 2020 | [46] | ||
| 1/12 | 8% | NGS | N.A. | China | Li | 2020 | [47] | ||
| 2/25 | 8% | targeted exome sequencing | N.A. | Korea | Chae | 2019 | [79] | ||
| 2/32 | 6% | targeted NGS | AC | Chile, Japan | Narayan | 2019 | [73] | ||
| 2/14 | 14% | TS | N.A. | China | Li | 2017 | [44] | ||
| 4/13 | 31% | PCR-SSCP + DS | N.A. | Korea | Kim | 2001 | [31] | ||
| 6/58 | 10% | ultra-deep targeted NGS | AC | China | Lin | 2019 | [70] | ||
| 64/760 | 8% | NGS | N.A. | America | Abdel-Wahab | 2020 | [19] | ||
| CTNNB1 | 6.4% | 0/21 | 0% | SNaPshot | AC | America | Moy | 2015 | [53] |
| 0/68 | 0% | WES + Sanger seq | AC | Japan | Akita | 2019 | [48] | ||
| 0/26 | 0% | NGS | N.A. | Italy | Simbolo | 2014 | [61] | ||
| 0/4 | 0% | TS | AC | Korea | Yoo | 2016 | [37] | ||
| 0/14 | 0% | NGS | N.A. | Japan | Noguchi | 2017 | [32] | ||
| 0/58 | 0% | ultra-deep targeted NGS | AC | China | Lin | 2019 | [70] | ||
| 1/25 | 4% | SNaPshot | N.A. | America | Borger | 2012 | [30] | ||
| 2/46 | 4% | mass array + seq | AC | India | Kumari | 2014 | [68] | ||
| 2/14 | 14% | TS | N.A. | China | Li | 2017 | [44] | ||
| 2/17 | 12% | WES | N.A. | India | Iyer | 2019 | [29] | ||
| 18/144 | 13% | WES | AC | India, Korea, Chile | Pandey | 2020 | [46] | ||
| 9/50 | 18% | PCR-SSCP + seq | AC | India | Dixit | 2020 | [36] | ||
| 19/47 | 40% | NGS | AC | Greece | Papadopoulou | 2018 | [40] | ||
| 30/760 | 4% | NGS | N.A. | America | Abdel-Wahab | 2020 | [19] | ||
| ELF3 | 18.6% | 29/144 | 20% | WES | AC | India, Korea, Chile | Pandey | 2020 | [46] |
| 5/39 | 13% | WES/WGS | N.A. | Japan | Ebata | 2021 | [57] | ||
| ERBB2 | 6.7% | 0/21 | 0% | SNaPshot | AC | America | Moy | 2015 | [53] |
| 0/46 | 0% | mass array | AC | India | Kumari | 2014 | [68] | ||
| 0/4 | 0% | TS | AC | Korea | Yoo | 2016 | [37] | ||
| 0/58 | 0% | ultra-deep targeted NGS | AC | China | Lin | 2019 | [70] | ||
| 1/26 | 4% | NGS | N.A. | Italy | Simbolo | 2014 | [61] | ||
| 2/32 | 6% | targeted NGS | AC | Chile, Japan | Narayan | 2019 | [73] | ||
| 1/14 | 7% | TS | N.A. | China | Li | 2017 | [44] | ||
| 2/54 | 4% | NGS | AC | Greece | Papadopoulou | 2018 | [40] | ||
| 2/5 | 40% | WES | AC | Japan | Akita | 2019 | [48] | ||
| 2/25 | 8% | targeted exome sequencing | N.A. | Korea | Chae | 2019 | [79] | ||
| 3/50 | 6% | NGS | N.A. | India | Patel | 2020 | [39] | ||
| 3/17 | 18% | WES | N.A. | India | Iyer | 2019 | [29] | ||
| 3/24 | 13% | NGS | N.A. | America | Okamura | 2021 | [27] | ||
| 3/39 | 8% | WES/WGS | N.A. | Japan | Ebata | 2021 | [57] | ||
| 4/47 | 9% | WES | AC | China | Yang | 2021 | [56] | ||
| 22/144 | 15% | WES | AC | India, Korea, Chile | Pandey | 2020 | [46] | ||
| 6/111 | 5% | NGS | N.A. | America | Mondaca | 2019 | [38] | ||
| 5/12 | 42% | NGS | N.A. | China | Li | 2020 | [47] | ||
| 11/157 | 7% | WES | N.A. | China | Li | 2019 | [18] | ||
| 40/760 | 5% | NGS | N.A. | America | Abdel-Wahab | 2020 | [19] | ||
| ERBB3 | 5.4% | 2/5 | 40% | WES | AC | Japan | Akita | 2019 | [48] |
| 1/11 | 9% | ultra-deep targeted NGS | N.A. | India | Yadav | 2017 | [77] | ||
| 1/17 | 6% | WES | N.A. | India | Iyer | 2019 | [29] | ||
| 0/24 | 0% | NGS | N.A. | America | Okamura | 2021 | [27] | ||
| 0/32 | 0% | targeted NGS | AC | Chile, Japan | Narayan | 2019 | [73] | ||
| 3/39 | 8% | WES/WGS | N.A. | Japan | Ebata | 2021 | [57] | ||
| 4/47 | 9% | WES | AC | China | Yang | 2021 | [56] | ||
| 3/50 | 6% | NGS | N.A. | India | Patel | 2020 | [39] | ||
| 3/54 | 6% | NGS | AC | Greece | Papadopoulou | 2018 | [40] | ||
| 0/58 | 0% | ultra-deep targeted NGS | AC | China | Lin | 2019 | [70] | ||
| 17/144 | 12% | WES | AC | India, Korea, Chile | Pandey | 2020 | [46] | ||
| 12/157 | 8% | WES | N.A. | China | Li | 2019 | [18] | ||
| 30/760 | 4% | NGS | N.A. | America | Abdel-Wahab | 2020 | [19] | ||
| KMT2D | 7.7% | 0/58 | 0% | ultra-deep targeted NGS | AC | China | Lin | 2019 | [70] |
| 1/17 | 6% | WES | N.A. | India | Iyer | 2019 | [29] | ||
| 1/14 | 7% | TS | N.A. | China | Li | 2017 | [44] | ||
| 5/32 | 16% | targeted NGS | AC | Chile, Japan | Narayan | 2019 | [73] | ||
| 5/54 | 9% | NGS | AC | Greece | Papadopoulou | 2018 | [40] | ||
| 5/47 | 11% | WES | AC | China | Yang | 2021 | [56] | ||
| KRAS | 10.3% | 1/42 | 2% | nested PCR, PCR-RFLP + DS | AC | Japan, Hungary | Nagahashi | 2008 | [35] |
| 0/27 | 0% | Oncomap | AC | America | Deshpande | 2011 | [66] | ||
| 0/29 | 0% | nested PCR, PCR-RFLP + DS | AC | Peru | Vidaurre | 2019 | [82] | ||
| 1/35 | 3% | PCR + seq | AC | Bolivia | Asai | 2014 | [42] | ||
| 1/25 | 4% | SNaPshot | N.A. | America | Borger | 2012 | [30] | ||
| 1/46 | 2% | mass array+ seq | AC | India | Kumari | 2014 | [68] | ||
| 1/4 | 25% | TS | AC | Korea | Yoo | 2016 | [37] | ||
| 1/24 | 4% | NGS | N.A. | America | Okamura | 2021 | [27] | ||
| 1/14 | 7% | TS | N.A. | China | Li | 2017 | [44] | ||
| 2/9 | 22% | PCR + seq | AC | Japan | Shibata | 2008 | [33] | ||
| 2/64 | 3% | Seq | AC | China | Rashid | 2002 | [49] | ||
| 2/29 | 7% | PCR | AC | America | Pai | 2011 | [62] | ||
| 2/60 | 3% | PCR + DS | AC | Taiwan | Huang | 2017 | [67] | ||
| 2/14 | 14% | NGS | N.A. | Japan | Noguchi | 2017 | [32] | ||
| 2/21 | 10% | SNaPshot | AC | America | Moy | 2015 | [53] | ||
| 2/12 | 17% | NGS | N.A. | China | Li | 2020 | [47] | ||
| 2/32 | 6% | targeted NGS | AC | Chile, Japan | Narayan | 2019 | [73] | ||
| 3/15 | 20% | PCR-RFLP + DS | N.A. | Korea | Kim | 2001 | [31] | ||
| 4/35 | 11% | DS | N.A. | Taiwan | Chang | 2013 | [25] | ||
| 4/34 | 12% | PCR | N.A. | Korea | Kim | 2015 | [60] | ||
| 4/68 | 6% | WES and Sanger seq | AC | Japan | Akita | 2019 | [48] | ||
| 6/144 | 4% | WES | AC | India, Korea, Chile | Pandey | 2020 | [46] | ||
| 4/58 | 7% | ultra-deep targeted NGS | AC | China | Lin | 2019 | [70] | ||
| 5/55 | 9% | NGS | N.A. | America | Javle | 2016 | [23] | ||
| 5/26 | 19% | NGS | N.A. | Italy | Simbolo | 2014 | [61] | ||
| 5/25 | 20% | targeted exome sequencing | N.A. | Korea | Chae | 2019 | [79] | ||
| 5/157 | 3% | WES | N.A. | China | Li | 2019 | [18] | ||
| 6/54 | 11% | NGS | AC | Greece | Papadopoulou | 2018 | [40] | ||
| 8/21 | 38% | PCR-RFLP | AC | India | Singh | 2004 | [63] | ||
| 8/34 | 24% | Seq | AC | India | Sharma | 2017 | [65] | ||
| 9/81 | 11% | PCR | N.A. | Japan | Tomioka | 2019 | [45] | ||
| 10/17 | 59% | PCR | N.A. | Japan | Nagai | 2002 | [24] | ||
| 10/20 | 50% | PCR + RFLP and DS | N.A. | Korea | Kim | 2000 | [50] | ||
| 12/25 | 48% | PCR-RFLP | AC | India | Shukla | 2020 | [34] | ||
| 16/39 | 41% | PCR-RFLP | N.A. | India | Kazmi | 2013 | [71] | ||
| 72/760 | 9% | NGS | N.A. | America | Abdel-Wahab | 2020 | [19] | ||
| PIK3CA | 10.0% | 0/34 | 0% | PCR | N.A. | Korea | Kim | 2015 | [60] |
| 0/58 | 0% | ultra-deep targeted NGS | AC | China | Lin | 2019 | [70] | ||
| 1/23 | 4% | PCR+ seq | N.A. | Switzerland | Riener | 2008 | [72] | ||
| 1/68 | 1% | WES + Sanger seq | AC | Japan | Akita | 2019 | [48] | ||
| 1/14 | 7% | TS | N.A. | China | Li | 2017 | [44] | ||
| 1/25 | 4% | targeted exome sequencing | N.A. | Korea | Chae | 2019 | [79] | ||
| 2/46 | 4% | mass array + seq | AC | India | Kumari | 2014 | [68] | ||
| 2/4 | 50% | TS | AC | Korea | Yoo | 2016 | [37] | ||
| 2/21 | 10% | SNaPshot | AC | America | Moy | 2015 | [53] | ||
| 2/24 | 8% | NGS | N.A. | America | Okamura | 2021 | [27] | ||
| 2/26 | 8% | NGS | N.A | Italy | Simbolo | 2014 | [61] | ||
| 3/27 | 11% | Oncomap | AC | America | Deshpande | 2011 | [66] | ||
| 3/25 | 12% | SNaPshot | N.A. | America | Borger | 2012 | [30] | ||
| 3/14 | 21% | NGS | N.A. | Japan | Noguchi | 2017 | [32] | ||
| 3/21 | 14% | targeted NGS | AC | Chile, Japan | Narayan | 2019 | [73] | ||
| 11/144 | 8% | WES | AC | India, Korea, Chile | Pandey | 2020 | [46] | ||
| 2/12 | 17% | NGS | N.A. | China | Li | 2020 | [47] | ||
| 5/47 | 11% | WES | AC | China | Yang | 2021 | [56] | ||
| 6/157 | 4% | WES | N.A. | China | Li | 2019 | [18] | ||
| 7/55 | 13% | NGS | N.A. | America | Javle | 2016 | [23] | ||
| 7/34 | 21% | Seq | AC | India | Sharma | 2017 | [65] | ||
| 8/130 | 6% | TS | N.A. | China | Zhao | 2016 | [78] | ||
| 10/54 | 19% | NGS | AC | Greece | Papadopoulou | 2018 | [40] | ||
| 102/760 | 13% | NGS | N.A. | America | Abdel-Wahab | 2020 | [19] | ||
| SHH | 20.0% | 10/50 | 20% | PCR + SSCP + seq | AC | India | Dixit | 2017 | [26] |
| SMAD4 | 13.1% | 0/4 | 0% | TS | AC | Korea | Yoo | 2016 | [37] |
| 1/17 | 6% | WES | N.A. | India | Iyer | 2019 | [29] | ||
| 1/5 | 20% | WES | AC | Japan | Akita | 2019 | [48] | ||
| 2/12 | 17% | NGS | N.A. | China | Li | 2020 | [47] | ||
| 2/26 | 8% | NGS | N.A. | Italy | Simbolo | 2014 | [61] | ||
| 2/14 | 14% | NGS | N.A. | Japan | Noguchi | 2017 | [32] | ||
| 3/24 | 13% | NGS | N.A. | America | Okamura | 2021 | [27] | ||
| 11/144 | 8% | WES | AC | India, Korea, Chile | Pandey | 2020 | [46] | ||
| 3/11 | 27% | ultra-deep targeted NGS | N.A. | India | Yadav | 2017 | [77] | ||
| 4/25 | 16% | targeted exome sequencing | N.A. | Korea | Chae | 2019 | [79] | ||
| 10/32 | 33% | targeted NGS | AC | Chile, Japan | Narayan | 2019 | [73] | ||
| 9/55 | 16% | NGS | N.A. | America | Javle | 2016 | [23] | ||
| 16/58 | 28% | ultra-deep targeted NGS | AC | China | Lin | 2019 | [70] | ||
| 92/760 | 12% | NGS | N.A. | America | Abdel-Wahab | 2020 | [19] | ||
| SRCAP | 13.0% | 7/54 | 13% | NGS | AC | Greece | Papadopoulou | 2018 | [40] |
| STK11 | 7.2% | 0/68 | 0% | WES and Sanger seq | AC | Japan | Akita | 2019 | [48] |
| 1/24 | 4% | NGS | N.A. | America | Okamura | 2021 | [27] | ||
| 1/26 | 4% | NGS | N.A. | Italy | Simbolo | 2014 | [61] | ||
| 10/144 | 7% | WES | AC | India, Korea, Chile | Pandey | 2020 | [46] | ||
| 3/39 | 8% | WES/WGS | N.A. | Japan | Ebata | 2021 | [57] | ||
| 4/58 | 7% | ultra-deep targeted NGS | AC | China | Lin | 2019 | [70] | ||
| 64/760 | 8% | NGS | N.A. | America | Abdel-Wahab | 2020 | [19] | ||
| SYNE1 | 6.2% | 3/54 | 6% | NGS | AC | Greece | Papadopoulou | 2018 | [40] |
| 1/11 | 9% | ultra-deep targetedNGS | N.A. | India | Yadav | 2017 | [77] | ||
| TP53 | 57.0% | 1/21 | 5% | SNaPshot | AC | America | Moy | 2015 | [53] |
| 1/25 | 4% | SNaPshot | N.A. | America | Borger | 2012 | [30] | ||
| 2/4 | 50% | TS | AC | Korea | Yoo | 2016 | [37] | ||
| 2/11 | 18% | ultra-deep targeted NGS | N.A. | India | Yadav | 2017 | [77] | ||
| 3/5 | 60% | WES | AC | Japan | Akita | 2019 | [48] | ||
| 4/46 | 9% | mass array + seq | AC | India | Kumari | 2014 | [34] | ||
| 5/14 | 36% | PCR-SSCP + DS | N.A. | Korea | Kim | 2001 | [31] | ||
| 6/17 | 36% | PCR-SSCP + seq | N.A. | Japan | Nagai | 2002 | [24] | ||
| 6/17 | 36% | WES | N.A. | India | Iyer | 2019 | [29] | ||
| 7/14 | 50% | TS | N.A. | China | Li | 2017 | [44] | ||
| 7/29 | 24% | nested PCR, PCR-RFLP + DS | AC | Peru | Vidaurre | 2019 | [82] | ||
| 8/12 | 67% | NGS | N.A. | China | Li | 2020 | [47] | ||
| 9/14 | 64% | NGS | N.A. | Japan | Noguchi | 2017 | [32] | ||
| 17/40 | 43% | nested PCR +DS | AC | Japan, Hungary | Nagahashi | 2008 | [35] | ||
| 11/25 | 44% | PCR-SSCP | AC | India | Shukla | 2020 | [34] | ||
| 11/24 | 46% | NGS | N.A. | America | Okamura | 2021 | [27] | ||
| 12/26 | 46% | NGS | N.A. | Italy | Simbolo | 2014 | [61] | ||
| 1535 | 43% | PCR + seq | AC | Bolivia | Asai | 2014 | [42] | ||
| 16/25 | 64% | targeted exome sequencing | N.A. | Korea | Chae | 2019 | [79] | ||
| 22/32 | 69% | targeted NGS | AC | Chile, Japan | Narayan | 2019 | [73] | ||
| 18/59 | 31% | Seq | AC | Austria | Puhalla | 2004 | [69] | ||
| 72/144 | 50% | WES | AC | India, Korea, Chile | Pandey | 2020 | [46] | ||
| 19/39 | 49% | WES/WGS | N.A. | Japan | Ebata | 2021 | [57] | ||
| 20/30 | 67% | PCR + DS | AC | Chile | Moreno | 2005 | [81] | ||
| 23/54 | 43% | NGS | AC | Greece | Papadopoulou | 2018 | [40] | ||
| 32/55 | 58% | NGS | N.A. | America | Javle | 2016 | [23] | ||
| 42/58 | 72% | ultra-deep targeted NGS | AC | China | Lin | 2019 | [70] | ||
| 541/760 | 71% | NGS | N.A. | America | Abdel-Wahab | 2020 | [19] |
References
- Stinton, L.M.; Shaffer, E.A. Epidemiology of gallbladder disease: Cholelithiasis and cancer. Gut Liver 2012, 6, 172–187. [Google Scholar] [CrossRef] [Green Version]
- Lazcano-Ponce, E.C.; Miquel, J.F.; Munoz, N.; Herrero, R.; Ferrecio, C.; Wistuba, I.I.; Alonso de Ruiz, P.; Aristi Urista, G.; Nervi, F. Epidemiology and Molecular Pathology of Gallbladder Cancer. CA Cancer J. Clin. 2001, 51, 349–364. [Google Scholar] [CrossRef]
- Are, C.; Ahmad, H.; Ravipati, A.; Croo, D.; Clarey, D.; Smith, L.; Price, R.R.; Butte, J.M.; Gupta, S.; Chaturvedi, A.; et al. Global epidemiological trends and variations in the burden of gallbladder cancer. J. Surg. Oncol. 2017, 115, 580–590. [Google Scholar] [CrossRef]
- Larsson, S.C.; Wolk, A. Obesity and the risk of gallbladder cancer: A meta-analysis. Br. J. Cancer 2007, 96, 1457–1461. [Google Scholar] [CrossRef]
- Sharma, A.; Sharma, K.L.; Gupta, A.; Yadav, A.; Kumar, A. Gallbladder cancer epidemiology, pathogenesis and molecular genetics: Recent update. World J. Gastroenterol. 2017, 23, 3978–3998. [Google Scholar] [CrossRef]
- Campbell, P.T.; Newton, C.C.; Kitahara, C.M.; Patel, A.V.; Hartge, P.; Koshiol, J.; McGlynn, K.A.; Adami, H.O.; De Gonzalez, A.B.; Freeman, L.E.B.; et al. Body size indicators and risk of gallbladder cancer: Pooled analysis of individual-level data from 19 prospective cohort studies. Cancer Epidemiol. Biomarkers Prev. 2017, 26, 597–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aloia, T.A.; Járufe, N.; Javle, M.; Maithel, S.K.; Roa, J.C.; Adsay, V.; Coimbra, F.J.F.; Jarnagin, W.R. Gallbladder Cancer: Expert consensus statement. HPB 2015, 17, 681–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Misra, S.; Chaturvedi, A.; Misra, N.C.; Sharma, I.D. Carcinoma of the gallbladder. Lancet Oncol. 2003, 4, 167–176. [Google Scholar] [CrossRef]
- Duffy, A.; Capanu, M.; Abou-Alfa, G.K.; Huitzil, D.; Jarnagin, W.; Fong, Y.; D’Angelica, M.; Dematteo, R.P.; Blumgart, L.H.; O’Reilly, E.M. Gallbladder cancer (GBC): 10-Year experience at Memorial Sloan-Kettering Cancer Centre (MSKCC). J. Surg. Oncol. 2008, 98, 485–489. [Google Scholar] [CrossRef]
- Lau, C.S.M.; Zywot, A.; Mahendraraj, K.; Chamberlain, R.S. Gallbladder Carcinoma in the United States: A Population Based Clinical Outcomes Study Involving 22,343 Patients from the Surveillance, Epidemiology, and End Result Database (1973–2013). HPB Surg. 2017, 2017, 1532835. [Google Scholar] [CrossRef]
- Lohman, E.D.S.; De Bitter, T.; Verhoeven, R.; Van Der Geest, L.; Hagendoorn, J.; Mohammad, N.H.; Daams, F.; Klümpen, H.-J.; Van Gulik, T.; Erdmann, J.; et al. Trends in Treatment and Survival of Gallbladder Cancer in the Netherlands; Identifying Gaps and Opportunities from a Nation-Wide Cohort. Cancers 2020, 12, 918. [Google Scholar] [CrossRef] [PubMed]
- Valle, J.; Wasan, H.; Palmer, D.H.; Cunningham, D.; Anthoney, A.; Maraveyas, A.; Madhusudan, S.; Iveson, T.; Hughes, S.; Pereira, S.P.; et al. Cisplatin plus Gemcitabine versus Gemcitabine for Biliary Tract Cancer. N. Engl. J. Med. 2010, 362, 1273–1281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montalvo-Jave, E.E.; Rahnemai- Azar, A.A.; Papaconstantinou, D.; Deloiza, M.E.; Tsilimigras, D.I.; Moris, D.; Mendoza-Barrera, G.E.; Weber, S.M.; Pawlik, T.M. Molecular pathways and potential biomarkers in gallbladder cancer: A comprehensive review. Surg. Oncol. 2019, 31, 83–89. [Google Scholar] [CrossRef] [PubMed]
- De Lorenzo, S.; Garajova, I.; Stefanini, B.; Tovoli, F. Targeted therapies for gallbladder cancer: An overview of agents in preclinical and clinical development. Expert Opin. Investig. Drugs 2021, 30, 759–772. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, 332–336. [Google Scholar] [CrossRef] [Green Version]
- Samuel, S.; Mukherjee, S.; Ammannagari, N.; Pokuri, V.K.; Kuvshinoff, B.; Groman, A.; LeVea, C.M.; Iyer, R. Clinicopathological characteristics and outcomes of rare histologic subtypes of gallbladder cancer over two decades: A population-based study. PLoS ONE 2018, 13, e0198809. [Google Scholar] [CrossRef] [Green Version]
- Niu, C.; Wang, S.; Guan, Q.; Ren, X.; Ji, B.; Liu, Y. Neuroendocrine tumors of the gallbladder (Review). Oncol. Lett. 2020, 19, 3381–3388. [Google Scholar] [CrossRef]
- Li, M.; Liu, F.; Zhang, F.; Zhou, W.; Jiang, X.; Yang, Y.; Qu, K.; Wang, Y.; Ma, Q.; Wang, T.; et al. Genomic ERBB2 / ERBB3 mutations promote PD-L1-mediated immune escape in gallbladder cancer: A whole-exome sequencing analysis. Gut 2019, 68, 1024–1033. [Google Scholar] [CrossRef]
- Abdel-Wahab, R.; Yap, T.A.; Madison, R.; Pant, S.; Cooke, M.; Wang, K.; Zhao, H.; Bekaii-Saab, T.; Karatas, E.; Kwong, L.N.; et al. Genomic profiling reveals high frequency of DNA repair genetic aberrations in gallbladder cancer. Sci. Rep. 2020, 10, 22087. [Google Scholar] [CrossRef]
- Roos, E.; Soer, E.C.; Klompmaker, S.; Meijer, L.L.; Besselink, M.G.; Giovannetti, E.; Heger, M.; Kazemier, G.; Klümpen, H.J.; Takkenberg, R.B.; et al. Crossing borders: A systematic review with quantitative analysis of genetic mutations of carcinomas of the biliary tract. Crit. Rev. Oncol. Hematol. 2019, 140, 8–16. [Google Scholar] [CrossRef]
- Sohani, Z.N.; Sarma, S.; Alyass, A.; De Souza, R.J.; Robiou-Du-Pont, S.; Li, A.; Mayhew, A.; Yazdi, F.; Reddon, H.; Lamri, A.; et al. Empirical evaluation of the Q-Genie tool: A protocol for assessment of effectiveness. BMJ Open 2016, 6, e010403. [Google Scholar] [CrossRef] [Green Version]
- Chakravarty, D.; Gao, J.; Phillips, S.M.; Kundra, R.; Zhang, H.; Wang, J.; Rudolph, J.E.; Yaeger, R.; Soumerai, T.; Nissan, M.H.; et al. OncoKB: A Precision Oncology Knowledge Base. JCO Precis. Oncol. 2017, 1, 1–16. [Google Scholar] [CrossRef]
- Javle, M.; Bekaii-Saab, T.; Jain, A.; Wang, Y.; Kelley, R.K.; Wang, K.; Kang, H.C.; Catenacci, D.; Ali, S.; Krishnan, S.; et al. Biliary cancer: Utility of next-generation sequencing for clinical management. Cancer 2016, 122, 3838–3847. [Google Scholar] [CrossRef] [Green Version]
- Nagai, M.; Watanabe, M.; Iwase, T.; Yamao, K.; Isaji, S. Clinical and genetic analysis of noncancerous and cancerous biliary epithelium in patients with pancreaticobiliary maljunction. World J. Surg. 2002, 26, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.T.; Chang, M.C.; Huang, K.W.; Tung, C.C.; Hsu, C.; Wong, J.M. Clinicopathological and prognostic significances of EGFR, KRAS and BRAF mutations in biliary tract carcinomas in Taiwan. J. Gastroenterol. Hepatol. 2014, 29, 1119–1125. [Google Scholar] [CrossRef] [PubMed]
- Dixit, R.; Pandey, M.; Tripathi, S.K.; Dwivedi, A.N.D.; Shukla, V.K. Comparative Analysis of Mutational Profile of Sonic hedgehog Gene in Gallbladder Cancer. Dig. Dis. Sci. 2017, 62, 708–714. [Google Scholar] [CrossRef] [PubMed]
- Okamura, R.; Kurzrock, R.; Mallory, R.J.; Fanta, P.T.; Burgoyne, A.M.; Clary, B.M.; Kato, S.; Sicklick, J.K. Comprehensive genomic landscape and precision therapeutic approach in biliary tract cancers. Int. J. Cancer 2021, 148, 702–712. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Mishra, P.K.; Sharma, S.; Arora, A.; Saluja, S.S. Effects of PTEN gene alteration in patients with gallbladder cancer. Cancer Genet. 2015, 208, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Iyer, P.; Shrikhande, S.V.; Ranjan, M.; Joshi, A.; Gardi, N.; Prasad, R.; Dharavath, B.; Thorat, R.; Salunkhe, S.; Sahoo, B.; et al. ERBB2 and KRAS alterations mediate response to EGFR inhibitors in early stage gallbladder cancer. Int. J. Cancer 2019, 144, 2008–2019. [Google Scholar] [CrossRef] [Green Version]
- Borger, D.R.; Tanabe, K.K.; Fan, K.C.; Lopez, H.U.; Fantin, V.R.; Straley, K.S.; Schenkein, D.P.; Hezel, A.F.; Ancukiewicz, M.; Liebman, H.M.; et al. Frequent Mutation of Isocitrate Dehydrogenase (IDH)1 and IDH2 in Cholangiocarcinoma Identified Through Broad-Based Tumor Genotyping. Oncologist 2012, 17, 72–79. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.T.; Kim, J.; Jang, Y.H.; Lee, W.J.; Ryu, J.K.; Park, Y.K.; Kim, S.W.; Kim, W.H.; Yoon, Y.B.; Kim, C.Y. Genetic alterations in gallbladder adenoma, dysplasia and carcinoma. Cancer Lett. 2001, 169, 59–68. [Google Scholar] [CrossRef]
- Noguchi, R.; Yamaguchi, K.; Ikenoue, T.; Terakado, Y.; Ohta, Y.; Yamashita, N.; Kainuma, O.; Yokoi, S.; Maru, Y.; Nagase, H.; et al. Genetic alterations in Japanese extrahepatic biliary tract cancer. Oncol. Lett. 2017, 14, 877–884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shibata, T.; Kokubu, A.; Gotoh, M.; Ojima, H.; Ohta, T.; Yamamoto, M.; Hirohashi, S. Genetic Alteration of Keap1 Confers Constitutive Nrf2 Activation and Resistance to Chemotherapy in Gallbladder Cancer. Gastroenterology 2008, 135, 1358–1368. [Google Scholar] [CrossRef] [PubMed]
- Shukla, S.K.; Singh, G.; Shahi, K.S.; Pant, P. Genetic Changes of P 53 and Kras in Gallbladder Carcinoma in Kumaon Region of Uttarakhand. J. Gastrointest. Cancer 2020, 51, 552–559. [Google Scholar] [CrossRef]
- Nagahashi, M.; Ajioka, Y.; Lang, I.; Szentirmay, Z.; Kasler, M.; Nakadaira, H.; Yokoyama, N.; Watanabe, G.; Nishikura, K.; Wakai, T.; et al. Genetic changes of p53, K-ras, and microsatellite instability in gallbladder carcinoma in high-incidence areas of Japan and Hungary. World J. Gastroenterol. 2008, 14, 70–75. [Google Scholar] [CrossRef]
- Dixit, R.; Pandey, M.; Tripathi, S.K.; Dwivedi, A.N.D.; Shukla, V.K. Genetic mutational analysis of β-catenin gene affecting GSK-3β phosphorylation plays a role in gallbladder carcinogenesis: Results from a case control study. Cancer Treat. Res. Commun. 2020, 23, 100173. [Google Scholar] [CrossRef]
- Yoo, K.H.; Kim, N.K.D.; Kwon, W.I.; Lee, C.; Kim, S.Y.; Jang, J.; Ahn, J.; Kang, M.; Jang, H.; Kim, S.T.; et al. Genomic alterations in biliary tract cancer using targeted sequencing. Transl. Oncol. 2016, 9, 173–178. [Google Scholar] [CrossRef] [Green Version]
- Mondaca, S.; Razavi, P.; Xu, C.; Offin, M.; Myers, M.; Scaltriti, M.; Hechtman, J.F.; Bradley, M.; O’Reilly, E.M.; Berger, M.F.; et al. Genomic Characterization of ERBB2 -Driven Biliary Cancer and a Case of Response to Ado-Trastuzumab Emtansine. JCO Precis. Oncol. 2019, 3, 1–9. [Google Scholar] [CrossRef]
- Patel, A.; Soneji, D.; Singh, H.P.; Kumar, M.; Bandyopadhyay, A.; Mathur, A.; Sharma, A.; Gahlot, G.P.S.; MS, S.; Guleria, B.; et al. Genomic Landscape and Targeted Treatment of Gallbladder Cancer: Results of a First Ongoing Prospective Study. South Asian J. Cancer 2020, 9, 074–079. [Google Scholar] [CrossRef]
- Papadopoulou, K.; Murray, S.; Manousou, K.; Tikas, I.; Dervenis, C.; Sgouros, J.; Rontogianni, D.; Lakis, S.; Poulios, C.; Pervana, S.; et al. Genotyping and mRNA profiling reveal actionable targets in biliary tract cancers. Ann. Oncol. 2017, 28, v246. [Google Scholar] [CrossRef]
- Maynard, H.; Stadler, Z.K.; Berger, M.F.; Solit, D.B.; Ly, M.; Lowery, M.A.; Mandelker, D.; Zhang, L.; Jordan, E.; El Dika, I.; et al. Germline alterations in patients with biliary tract cancers: A spectrum of significant and previously underappreciated findings. Cancer 2020, 126, 1995–2002. [Google Scholar] [CrossRef]
- Asai, T.; Loza, E.; Roig, G.V.G.; Ajioka, Y.; Tsuchiya, Y.; Yamamoto, M.; Nakamura, K. High frequency of TP53 but not K-ras gene mutations in bolivian patients with gallbladder cancer. Asian Pac. J. Cancer Prev. 2014, 15, 5449–5454. [Google Scholar] [CrossRef] [Green Version]
- Wistuba, I.I.; Maitra, A.; Carrasco, R.; Tang, M.; Troncoso, P.; Minna, J.D.; Gazdar, A.F. High resolution chromosome 3p, 8p, 9q and 22q allelotyping analysis in the pathogenesis of gallbladder carcinoma. Br. J. Cancer 2002, 87, 432–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, M.; Chen, L.; Qu, Y.; Sui, F.; Yang, Q.; Ji, M.; Shi, B.; Chen, M.; Hou, P. Identification of MAP kinase pathways as therapeutic targets in gallbladder carcinoma using targeted parallel sequencing. Oncotarget 2017, 8, 36319–36330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomioka, Y.; Sung, Y.N.; Sawada, R.; Hong, S.M.; Akita, M.; Itoh, T.; Ajiki, T.; Fukumoto, T.; Zen, Y. IL-33 overexpression in gallbladder cancers associated with pancreatobiliary maljunction. Histopathology 2019, 75, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.; Stawiski, E.W.; Durinck, S.; Gowda, H.; Goldstein, L.D.; Barbhuiya, M.A.; Schröder, M.S.; Sreenivasamurthy, S.K.; Kim, S.W.; Phalke, S.; et al. Integrated genomic analysis reveals mutated ELF3 as a potential gallbladder cancer vaccine candidate. Nat. Commun. 2020, 11, 4225. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wei, Q.; Wu, X.; Sima, J.; Xu, Q.; Wu, M.; Wang, F.; Mou, H.; Hu, H.; Zhao, J.; et al. Integrative clinical and molecular analysis of advanced biliary tract cancers on immune checkpoint blockade reveals potential markers of response. Clin. Transl. Med. 2020, 10, e118. [Google Scholar] [CrossRef]
- Akita, M.; Fujikura, K.; Ajiki, T.; Fukumoto, T.; Otani, K.; Hirose, T.; Tominaga, M.; Itoh, T.; Zen, Y. Intracholecystic Papillary Neoplasms Are Distinct from Papillary Gallbladder Cancers: A Clinicopathologic and Exome-sequencing Study. Am. J. Surg. Pathol. 2019, 43, 783–791. [Google Scholar] [CrossRef]
- Rashid, A.; Ueki, T.; Gao, Y.T.; Houlihan, P.S.; Wallace, C.; Wang, B.S.; Shen, M.C.; Deng, J.; Hsing, A.W. K-ras mutation, p53 overexpression, and microsatellite instability in biliary tract cancers: A population-based study in China. Clin. Cancer Res. 2002, 8, 3156–3163. [Google Scholar]
- Kim, S.W.; Her, K.H.; Jang, J.Y.; Kim, W.H.; Kim, Y.T.; Park, Y.H. K-ras oncogene mutation in cancer and precancerous lesions of the gallbladder. J. Surg. Oncol. 2000, 75, 246–251. [Google Scholar] [CrossRef]
- Hirosawa, T.; Ishida, M.; Ishii, K.; Kanehara, K.; Kudo, K.; Ohnuma, S.; Kamei, T.; Motoi, F.; Naitoh, T.; Selaru, F.M.; et al. Loss of BAP1 expression is associated with genetic mutation and can predict outcomes in gallbladder cancer. PLoS ONE 2018, 13, e0206643. [Google Scholar] [CrossRef]
- Goeppert, B.; Roessler, S.; Renner, M.; Loeffler, M.; Singer, S.; Rausch, M.; Albrecht, T.; Mehrabi, A.; Vogel, M.N.; Pathil, A.; et al. Low frequency of mismatch repair deficiency in gallbladder cancer. Diagn. Pathol. 2019, 14, 36. [Google Scholar] [CrossRef]
- Moy, A.P.; Shahid, M.; Ferrone, C.R.; Borger, D.R.; Zhu, A.X.; Ting, D.; Deshpande, V. Microsatellite instability in gallbladder carcinoma. Virchows Arch. 2015, 466, 393–402. [Google Scholar] [CrossRef]
- Yoshida, T.; Sugai, T.; Habano, W.; Nakamura, S.I.; Uesugi, N.; Funato, O.; Saito, K. Microsatellite instability in gallbladder carcinoma: Two independent genetic pathways of gallbladder carcinogenesis. J. Gastroenterol. 2000, 35, 768–774. [Google Scholar] [CrossRef]
- Roa, J.C.; Roa, I.; Correa, P.; Vo, Q.; Araya, J.C.; Villaseca, M.; Guzmán, P.; Schneider, B.G. Microsatellite instability in preneoplastic and neoplastic lesions of the gallbladder. J. Gastroenterol. 2005, 40, 79–86. [Google Scholar] [CrossRef]
- Yang, D.; Chen, T.; Zhan, M.; Xu, S.; Yin, X.; Liu, Q.; Chen, W.; Zhang, Y.; Liu, D.; Yan, J.; et al. Modulation of mTOR and epigenetic pathways as therapeutics in gallbladder cancer. Mol. Ther. Oncolytics 2021, 20, 59–70. [Google Scholar] [CrossRef]
- Ebata, N.; Fujita, M.; Sasagawa, S.; Maejima, K.; Okawa, Y.; Hatanaka, Y.; Mitsuhashi, T.; Oosawa-tatsuguchi, A.; Tanaka, H.; Miyano, S.; et al. Molecular classification and tumor microenvironment characterization of gallbladder cancer by comprehensive genomic and transcriptomic analysis. Cancers 2021, 13, 733. [Google Scholar] [CrossRef] [PubMed]
- Spizzo, G.; Puccini, A.; Xiu, J.; Goldberg, R.M.; Grothey, A.; Shields, A.F.; Arora, S.P.; Khushmann, M.; Salem, M.E.; Battaglin, F.; et al. Molecular profile of BRCA-mutated biliary tract cancers. ESMO Open 2020, 5, e000682. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, B.A.; Xiu, J.; Lindberg, M.R.; Shields, A.F.; Hwang, J.J.; Poorman, K.; Salem, M.E.; Pishvaian, M.J.; Holcombe, R.F.; Marshall, J.L.; et al. Molecular profiling of biliary cancers reveals distinct molecular alterations and potential therapeutic targets. J. Gastrointest. Oncol. 2019, 10, 652–662. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.T.; Jang, K.T.; Lee, J.; Jang, H.M.; Choi, H.J.; Jang, H.L.; Park, S.H.; Park, Y.S.; Lim, H.Y.; Kang, W.K.; et al. Molecular subgroup analysis of clinical outcomes in a phase 3 study of gemcitabine and oxaliplatin with or without erlotinib in advanced biliary tract cancer. Transl. Oncol. 2015, 8, 40–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simbolo, M.; Fassan, M.; Ruzzenente, A.; Mafficini, A.; Wood, L.D.; Corbo, V.; Melisi, D.; Malleo, G.; Vicentini, C.; Malpeli, G.; et al. Multigene mutational profiling of cholangiocarcinomas identifies actionable molecular subgroups. Oncotarget 2014, 5, 2839–2852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pai, R.K.; Pai, R.K.; Mojtahed, K. Mutations in the RAS/RAF/MAP kinase pathway commonly occur in gallbladder adenomas but are uncommon in gallbladder adenocarcinomas. Appl. Immunohistochem. Mol. Morphol. 2011, 19, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.K.; Chetri, K.; Pandey, U.B.; Kapoor, V.K.; Mittal, B.; Choudhuri, G. Mutational spectrum of K-ras oncogene among Indian patients with gallbladder cancer. J. Gastroenterol. Hepatol. 2004, 19, 916–921. [Google Scholar] [CrossRef] [PubMed]
- Saetta, A.A.; Papanastasiou, P.; Michalopoulos, N.V.; Gigelou, F.; Korkolopoulou, P.; Bei, T.; Patsouris, E. Mutational analysis of BRAF in gallbladder carcinomas in association with K-ras and p53 mutations and microsatellite instability. Virchows Arch. 2004, 445, 179–182. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Kumar, A.; Kumari, N.; Krishnani, N.; Rastogi, N. Mutational frequency of KRAS, NRAS, IDH2, PIK3CA, and EGFR in North Indian gallbladder cancer patients. Ecancermedicalscience 2017, 11, 757. [Google Scholar] [CrossRef] [Green Version]
- Deshpande, V.; Nduaguba, A.; Zimmerman, S.M.; Kehoe, S.M.; MacConaill, L.E.; Lauwers, G.Y.; Ferrone, C.; Bardeesy, N.; Zhu, A.X.; Hezel, A.F. Mutational profiling reveals PIK3CA mutations in gallbladder carcinoma. BMC Cancer 2011, 11, 60. [Google Scholar] [CrossRef] [Green Version]
- Huang, W.C.; Tsai, C.C.; Chan, C.C. Mutation analysis and copy number changes of KRAS and BRAF genes in Taiwanese cases of biliary tract cholangiocarcinoma. J. Formos. Med. Assoc. 2017, 116, 464–468. [Google Scholar] [CrossRef] [Green Version]
- Kumari, N.; Corless, C.L.; Warrick, A.; Beadling, C.; Nelson, D.; Neff, T.; Krishnani, N.; Kapoor, V.K. Mutation profiling in gallbladder cancer in Indian population. Indian J. Pathol. Microbiol. 2014, 57, 9–12. [Google Scholar] [CrossRef]
- Puhalla, H.; Kandioler, D.; Ludwig, C.; Filipits, M.; Wrba, F.; Laengle, F.; Jakesz, R.; Gruenberger, T. p53 Analysis in Gallbladder Cancer: Comparison of Gene Analysis Versus Immunohistochemistry. Anticancer Res. 2004, 24, 1201–1206. [Google Scholar]
- Lin, J.; Dong, K.; Bai, Y.; Zhao, S.; Dong, Y.; Shi, J.; Shi, W.; Long, J.; Yang, X.; Wang, D.; et al. Precision oncology for gallbladder cancer: Insights from genetic alterations and clinical practice. Ann. Transl. Med. 2019, 7, 467. [Google Scholar] [CrossRef]
- Kazmi, H.R.; Chandra, A.; Nigam, J.; Noushif, M.; Parmar, D.; Gupta, V. Prognostic significance of k-ras Codon 12 mutation in patients with Resected gallbladder cancer. Dig. Surg. 2013, 30, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Riener, M.O.; Bawohl, M.; Clavien, P.A.; Jochum, W. Rare PIK3CA hotspot mutations in carcinomas of the biliary tract. Genes Chromosom. Cancer 2008, 47, 363–367. [Google Scholar] [CrossRef] [PubMed]
- Narayan, R.R.; Creasy, J.M.; Goldman, D.A.; Gönen, M.; Kandoth, C.; Kundra, R.; Solit, D.B.; Askan, G.; Klimstra, D.S.; Basturk, O.; et al. Regional differences in gallbladder cancer pathogenesis: Insights from a multi-institutional comparison of tumor mutations. Cancer 2019, 125, 575–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peraldo Neia, C.; Cavalloni, G.; Balsamo, A.; Venesio, T.; Napoli, F.; Sassi, F.; Martin, V.; Frattini, M.; Aglietta, M.; Leone, F. Screening for the FIG-ROS1 fusion in biliary tract carcinomas by nested PCR. Genes Chromosom. Cancer 2014, 53, 1033–1040. [Google Scholar] [CrossRef]
- Leone, F.; Cavalloni, G.; Pignochino, Y.; Sarotto, I.; Ferraris, R.; Piacibello, W.; Venesio, T.; Capussotti, L.; Risio, M.; Aglietta, M. Somatic mutations of epidermal growth factor receptor in bile duct and gallbladder carcinoma. Clin. Cancer Res. 2006, 12, 1680–1685. [Google Scholar] [CrossRef] [Green Version]
- Roa, I.; Garcia, H.; Game, A.; De Toro, G.; De Aretxabala, X.; Javle, M. Somatic Mutations of PI3K in Early and Advanced Gallbladder Cancer: Additional Options for an Orphan Cancer. J. Mol. Diagn. 2016, 18, 388–394. [Google Scholar] [CrossRef]
- Yadav, S.; DE Sarkar, N.; Kumari, N.; Krishnani, N.; Kumar, A.; Mittal, B. Targeted Gene Sequencing of Gallbladder Carcinoma Identifies High-impact Somatic and Rare Germline Mutations. Cancer Genom. Proteom. 2017, 14, 495–506. [Google Scholar] [CrossRef] [Green Version]
- Zhao, S.; Cao, Y.; Liu, S.B.; Wang, X.A.; Bao, R.F.; Shu, Y.J.; Hu, Y.P.; Zhang, Y.J.; Jiang, L.; Zhang, F.; et al. The E545K mutation of PIK3CA promotes gallbladder carcinoma progression through enhanced binding to EGFR. J. Exp. Clin. Cancer Res. 2016, 35. [Google Scholar] [CrossRef] [Green Version]
- Chae, H.; Kim, D.; Yoo, C.; Kim, K.-P.; Jeong, J.H.; Chang, H.-M.; Lee, S.S.; Park, D.H.; Song, T.J.; Hwang, S.; et al. Therapeutic relevance of targeted sequencing in management of patients with advanced biliary tract cancer: DNA damage repair gene mutations as a predictive biomarker. Eur. J. Cancer 2019, 120, 31–39. [Google Scholar] [CrossRef]
- Goldenberg, D.; Rosenbaum, E.; Argani, P.; Wistuba, I.I.; Sidransky, D.; Thuluvath, P.J.; Hidalgo, M.; Califano, J.; Maitra, A. The V599E BRAF mutation is uncommon in biliary tract cancers. Mod. Pathol. 2004, 17, 1386–1391. [Google Scholar] [CrossRef] [Green Version]
- Moreno, M.; Pimentel, F.; Gazdar, A.F.; Wistuba, I.I.; Miquel, J.F. TP53 abnormalities are frequent and early events in the sequential pathogenesis of gallbladder carcinoma. Ann. Hepatol. Off. J. Mex. Assoc. Hepatol. 2005, 4, 192–199. [Google Scholar] [CrossRef]
- Vidaurre, T.; Casavilca, S.; Montenegro, P.; Gomez, H.; Calderón, M.; Navarro, J.; Aramburu, J.; Poquioma, E.; Tsuchiya, Y.; Asai, T.; et al. Tumor protein p53 and K-ras gene mutations in Peruvian patients with gallbladder cancer. Asian Pac. J. Cancer Prev. 2019, 20, 289–294. [Google Scholar] [CrossRef] [Green Version]
- Tadokoro, H.; Shigihara, T.; Ikeda, T.; Takase, M.; Suyama, M. Two distinct pathways of p16 gene inactivation in gallbladder cancer. World J. Gastroenterol. 2007, 13, 6396–6403. [Google Scholar] [CrossRef]
- de Bono, J.; Mateo, J.; Fizazi, K.; Saad, F.; Shore, N.; Sandhu, S.; Chi, K.N.; Sartor, O.; Agarwal, N.; Olmos, D.; et al. Olaparib for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2020, 382, 2091–2102. [Google Scholar] [CrossRef] [PubMed]
- Janjigian, Y.Y.; Maron, S.B.; Chatila, W.K.; Millang, B.; Chavan, S.S.; Alterman, C.; Chou, J.F.; Segal, M.F.; Simmons, M.Z.; Momtaz, P.; et al. First-line pembrolizumab and trastuzumab in HER2-positive oesophageal, gastric, or gastro-oesophageal junction cancer: An open-label, single-arm, phase 2 trial. Lancet Oncol. 2020, 21, 821–831. [Google Scholar] [CrossRef]
- Bang, Y.J.; Van Cutsem, E.; Feyereislova, A.; Chung, H.C.; Shen, L.; Sawaki, A.; Lordick, F.; Ohtsu, A.; Omuro, Y.; Satoh, T.; et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): A phase 3, open-label, randomised controlled trial. Lancet 2010, 376, 687–697. [Google Scholar] [CrossRef]
- Shitara, K.; Bang, Y.-J.; Iwasa, S.; Sugimoto, N.; Ryu, M.-H.; Sakai, D.; Chung, H.-C.; Kawakami, H.; Yabusaki, H.; Lee, J.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Positive Gastric Cancer. N. Engl. J. Med. 2020, 382, 2419–2430. [Google Scholar] [CrossRef]
- Verma, S.; Miles, D.; Gianni, L.; Krop, I.E.; Welslau, M.; Baselga, J.; Pegram, M.; Oh, D.-Y.; Diéras, V.; Guardino, E.; et al. Trastuzumab Emtansine for HER2-Positive Advanced Breast Cancer. N. Engl. J. Med. 2012, 367, 1783–1791. [Google Scholar] [CrossRef] [Green Version]
- Johnston, S.; Pippen, J.; Pivot, X.; Lichinitser, M.; Sadeghi, S.; Dieras, V.; Gomez, H.L.; Romieu, G.; Manikhas, A.; Kennedy, M.J.; et al. Lapatinib combined with letrozole versus letrozole and placebo as first-line therapy for postmenopausal hormone receptor-Positive metastatic breast cancer. J. Clin. Oncol. 2009, 27, 5538–5546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geyer, C.E.; Forster, J.; Lindquist, D.; Chan, S.; Romieu, C.G.; Pienkowski, T.; Jagiello-Gruszfeld, A.; Crown, J.; Chan, A.; Kaufman, B.; et al. Lapatinib plus Capecitabine for HER2-Positive Advanced Breast Cancer. N. Engl. J. Med. 2006, 355, 2733–2743. [Google Scholar] [CrossRef] [Green Version]
- Rugo, H.S.; Im, S.A.; Cardoso, F.; Cortés, J.; Curigliano, G.; Musolino, A.; Pegram, M.D.; Wright, G.S.; Saura, C.; Escrivá-De-Romaní, S.; et al. Efficacy of Margetuximab vs Trastuzumab in Patients with Pretreated ERBB2-Positive Advanced Breast Cancer: A Phase 3 Randomized Clinical Trial. JAMA Oncol. 2021, 7, 573–584. [Google Scholar] [CrossRef] [PubMed]
- Martin, M.; Bonneterre, J.; Geyer, C.E.; Ito, Y.; Ro, J.; Lang, I.; Kim, S.B.; Germa, C.; Vermette, J.; Wang, K.; et al. A phase two randomised trial of neratinib monotherapy versus lapatinib plus capecitabine combination therapy in patients with HER2+ advanced breast cancer. Eur. J. Cancer 2013, 49, 3763–3772. [Google Scholar] [CrossRef]
- Vogel, C.L.; Cobleigh, M.A.; Tripathy, D.; Gutheil, J.C.; Harris, L.N.; Fehrenbacher, L.; Slamon, D.J.; Murphy, M.; Novotny, W.F.; Burchmore, M.; et al. Efficacy and safety of trastuzumab as a single agent in first-line treatment of HER2-overexpressing metastatic breast cancer. J. Clin. Oncol. 2002, 20, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Baselga, J.; Cortés, J.; Kim, S.-B.; Im, S.-A.; Hegg, R.; Im, Y.-H.; Roman, L.; Pedrini, J.L.; Pienkowski, T.; Knott, A.; et al. Pertuzumab plus Trastuzumab plus Docetaxel for Metastatic Breast Cancer. N. Engl. J. Med. 2012, 366, 109–119. [Google Scholar] [CrossRef] [Green Version]
- Murthy, R.K.; Loi, S.; Okines, A.; Paplomata, E.; Hamilton, E.; Hurvitz, S.A.; Lin, N.U.; Borges, V.; Abramson, V.; Anders, C.; et al. Tucatinib, Trastuzumab, and Capecitabine for HER2-Positive Metastatic Breast Cancer. N. Engl. J. Med. 2020, 382, 597–609. [Google Scholar] [CrossRef] [PubMed]
- Modi, S.; Saura, C.; Yamashita, T.; Park, Y.H.; Kim, S.-B.; Tamura, K.; Andre, F.; Iwata, H.; Ito, Y.; Tsurutani, J.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Positive Breast Cancer. N. Engl. J. Med. 2020, 382, 610–621. [Google Scholar] [CrossRef] [PubMed]
- Tosi, F.; Sartore-Bianchi, A.; Lonardi, S.; Amatu, A.; Leone, F.; Ghezzi, S.; Martino, C.; Bencardino, K.; Bonazzina, E.; Bergamo, F.; et al. Long-term Clinical Outcome of Trastuzumab and Lapatinib for HER2-positive Metastatic Colorectal Cancer. Clin. Colorectal Cancer 2020, 19, 256–262.e2. [Google Scholar] [CrossRef] [PubMed]
- Meric-Bernstam, F.; Hurwitz, H.; Raghav, K.P.S.; McWilliams, R.R.; Fakih, M.; VanderWalde, A.; Swanton, C.; Kurzrock, R.; Burris, H.; Sweeney, C.; et al. Pertuzumab plus trastuzumab for HER2-amplified metastatic colorectal cancer (MyPathway): An updated report from a multicentre, open-label, phase 2a, multiple basket study. Lancet Oncol. 2019, 20, 518–530. [Google Scholar] [CrossRef]
- Siena, S.; Di Bartolomeo, M.; Raghav, K.; Masuishi, T.; Loupakis, F.; Kawakami, H.; Yamaguchi, K.; Nishina, T.; Fakih, M.; Elez, E.; et al. Trastuzumab deruxtecan (DS-8201) in patients with HER2-expressing metastatic colorectal cancer (DESTINY-CRC01): A multicentre, open-label, phase 2 trial. Lancet Oncol. 2021, 22, 779–789. [Google Scholar] [CrossRef]
- Fader, A.N.; Roque, D.M.; Siegel, E.; Buza, N.; Hui, P.; Abdelghany, O.; Chambers, S.K.; Secord, A.A.; Havrilesky, L.; O’Malley, D.M.; et al. Randomized Phase II trial of carboplatin-paclitaxel versus carboplatin-paclitaxel-trastuzumab in uterine serous carcinomas that overexpress human epidermal growth factor receptor 2/neu. J. Clin. Oncol. 2018, 36, 2044–2051. [Google Scholar] [CrossRef] [PubMed]
- Li, B.T.; Shen, R.; Buonocore, D.; Olah, Z.T.; Ni, A.; Ginsberg, M.S.; Ulaner, G.A.; Offin, M.; Feldman, D.; Hembrough, T.; et al. Ado-trastuzumab emtansine for patients with HER2-mutant lung cancers: Results from a phase II basket trial. J. Clin. Oncol. 2018, 36, 2532–2537. [Google Scholar] [CrossRef] [PubMed]
- Li, B.T.; Smit, E.F.; Goto, Y.; Nakagawa, K.; Udagawa, H. Trastuzumab Deruxtecan in HER2-Mutant Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Rugo, H.S.; Lerebours, F.; Ciruelos, E.; Drullinsky, P.; Ruiz-Borrego, M.; Neven, P.; Park, Y.H.; Prat, A.; Bachelot, T.; Juric, D.; et al. Alpelisib plus fulvestrant in PIK3CA-mutated, hormone receptor-positive advanced breast cancer after a CDK4/6 inhibitor (BYLieve): One cohort of a phase 2, multicentre, open-label, non-comparative study. Lancet Oncol. 2021, 22, 489–498. [Google Scholar] [CrossRef]
- Marabelle, A.; Fakih, M.; Lopez, J.; Shah, M.; Shapira-Frommer, R.; Nakagawa, K.; Chung, H.C.; Kindler, H.L.; Lopez-Martin, J.A.; Miller, W.H.; et al. Association of tumour mutational burden with outcomes in patients with advanced solid tumours treated with pembrolizumab: Prospective biomarker analysis of the multicohort, open-label, phase 2 KEYNOTE-158 study. Lancet Oncol. 2020, 21, 1353–1365. [Google Scholar] [CrossRef]
- Marcus, L.; Lemery, S.J.; Keegan, P.; Pazdur, R. FDA approval summary: Pembrolizumab for the treatment of microsatellite instability-high solid tumors. Clin. Cancer Res. 2019, 25, 3753–3758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Overman, M.J.; McDermott, R.; Leach, J.L.; Lonardi, S.; Lenz, H.J.; Morse, M.A.; Desai, J.; Hill, A.; Axelson, M.; Moss, R.A.; et al. Nivolumab in patients with metastatic DNA mismatch repair-deficient or microsatellite instability-high colorectal cancer (CheckMate 142): An open-label, multicentre, phase 2 study. Lancet Oncol. 2017, 18, 1182–1191. [Google Scholar] [CrossRef]
- Overman, M.J.; Lonardi, S.; Wong, K.Y.M.; Lenz, H.J.; Gelsomino, F.; Aglietta, M.; Morse, M.A.; Van Cutsem, E.; McDermott, R.; Hill, A.; et al. Durable clinical benefit with nivolumab plus ipilimumab in DNA mismatch repair-deficient/microsatellite instability-high metastatic colorectal cancer. J. Clin. Oncol. 2018, 36, 773–779. [Google Scholar] [CrossRef]
- Goodman, A.M.; Kato, S.; Bazhenova, L.; Patel, S.P.; Frampton, G.M.; Miller, V.; Stephens, P.J.; Daniels, G.A.; Kurzrock, R. Tumor mutational burden as an independent predictor of response to immunotherapy in diverse cancers. Mol. Cancer Ther. 2017, 16, 2598–2608. [Google Scholar] [CrossRef] [Green Version]
- Yarchoan, M.; Hopkins, A.; Jaffee, E.M. Tumor Mutational Burden and Response Rate to PD-1 Inhibition. N. Engl. J. Med. 2017, 377, 2500–2501. [Google Scholar] [CrossRef]
- Ott, P.A.; Bang, Y.J.; Piha-Paul, S.A.; Abdul Razak, A.R.; Bennouna, J.; Soria, J.C.; Rugo, H.S.; Cohen, R.B.; O’Neil, B.H.; Mehnert, J.M.; et al. T-cell–inflamed gene-expression profile, programmed death ligand 1 expression, and tumor mutational burden predict efficacy in patients treated with pembrolizumab across 20 cancers: KEYNOTE-028. J. Clin. Oncol. 2019, 37, 318–327. [Google Scholar] [CrossRef]
- Marabelle, A.; Le, D.T.; Ascierto, P.A.; Di Giacomo, A.M.; de Jesus-Acosta, A.; Delord, J.P.; Geva, R.; Gottfried, M.; Penel, N.; Hansen, A.R.; et al. Efficacy of pembrolizumab in patients with noncolorectal high microsatellite instability/ mismatch repair–deficient cancer: Results from the phase II KEYNOTE-158 study. J. Clin. Oncol. 2020, 38, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.R. Next-Generation Sequencing in High-Sensitive Detection of Mutations in Tumors: Challenges, Advances, and Applications. J. Mol. Diagn. 2020, 22, 994–1007. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Shao, Y.; Tian, L.; Flasch, D.A.; Mulder, H.L.; Edmonson, M.N.; Liu, Y.; Chen, X.; Newman, S.; Nakitandwe, J.; et al. Analysis of error profiles in deep next-generation sequencing data. Genome Biol. 2019, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berger, M.F.; Mardis, E.R. The emerging clinical relevance of genomics in cancer medicine. Nat. Rev. Clin. Oncol. 2018, 15, 353–365. [Google Scholar] [CrossRef]
- Boland, C.R.; Thibodeau, S.N.; Hamilton, S.R.; Sidransky, D.; Eshleman, J.R.; Burt, R.W.; Meltzer, S.J.; Rodriguez-Bigas, M.A.; Fodde, R.; Ranzani, G.N.; et al. A National Cancer Institute workshop on microsatellite instability for cancer detection and familial predisposition: Development of international criteria for the determination of microsatellite instability in colorectal cancer. Cancer Res. 1998, 58, 5248–5257. [Google Scholar]
- Kato, S.; Goodman, A.; Walavalkar, V.; Barkauskas, D.A.; Sharabi, A.; Kurzrock, R. Hyperprogressors after immunotherapy: Analysis of genomic alterations associated with accelerated growth rate. Clin. Cancer Res. 2017, 23, 4242–4250. [Google Scholar] [CrossRef] [PubMed] [Green Version]


| Gene | WA | N | Frequency | Methods | Histology | Population | Author | Year | Ref. |
|---|---|---|---|---|---|---|---|---|---|
| CCNE1 | 11.0% | 82/760 | 11% | NGS | N.A. | America | Abdel-Wahab | 2020 | [19] |
| 4/24 | 17% | NGS | N.A. | America | Okamura | 2021 | [27] | ||
| CDK4 | 5.2% | 38/760 | 5% | NGS | N.A. | America | Abdel-Wahab | 2020 | [19] |
| 3/24 | 13% | NGS | N.A. | America | Okamura | 2021 | [27] | ||
| CDKN2A | 18.2% | 156/760 | 21% | NGS | N.A. | America | Abdel-Wahab | 2020 | [19] |
| 6/58 | 10% | ultra-deep targeted NGS | AC | China | Lin | 2019 | [70] | ||
| 4/32 | 13% | targeted NGS | AC | Chile, Japan | Narayan | 2019 | [73] | ||
| 0/25 | 0% | targeted exome sequencing | N.A. | Korea | Chae | 2019 | [79] | ||
| 10/45 | 22% | real-time PCR | AC | Japan | Tadokoro | 2007 | [83] | ||
| CDKN2B | 10.0% | 135/760 | 18% | NGS | N.A. | America | Abdel-Wahab | 2020 | [19] |
| 6/58 | 10% | ultra-deep targeted NGS | AC | China | Lin | 2019 | [70] | ||
| 3/32 | 9% | targeted NGS | AC | Chile, Japan | Narayan | 2019 | [73] | ||
| ERBB2 | 7.1% | 77/760 | 10% | NGS | N.A. | America | Abdel-Wahab | 2020 | [19] |
| 1/24 | 4% | NGS | N.A. | America | Okamura | 2021 | [27] | ||
| 1/4 | 25% | TS | AC | Korea | Yoo | 2016 | [37] | ||
| 9/111 | 8% | NGS | N.A. | America | Mondaca | 2019 | [38] | ||
| 9/50 | 18% | NGS | N.A. | India | Patel | 2020 | [39] | ||
| 3/32 | 9% | targeted NGS | AC | Chile, Japan | Narayan | 2019 | [73] | ||
| 4/25 | 16% | targeted exome sequencing | N.A. | Korea | Chae | 2019 | [79] | ||
| FRS2 | 7.3% | 55/760 | 7% | NGS | N.A. | America | Abdel-Wahab | 2020 | [19] |
| 2/24 | 8% | NGS | N.A. | America | Okamura | 2021 | [27] | ||
| KRAS | 14.1% | 35/760 | 5% | NGS | N.A. | America | Abdel-Wahab | 2020 | [19] |
| 2/24 | 8% | NGS | N.A. | America | Okamura | 2021 | [27] | ||
| 10/60 | 17% | PCR + DS | AC | Taiwan | Huang | 2017 | [67] | ||
| 1/58 | 2% | ultra-deep targeted NGS | AC | China | Lin | 2019 | [70] | ||
| 3/32 | 9% | targeted NGS | AC | Chile, Japan | Narayan | 2019 | [73] | ||
| 1/25 | 4% | targeted exome sequencing | N.A. | Korea | Chae | 2019 | [79] | ||
| MDM2 | 7.8% | 86/760 | 11% | NGS | N.A. | America | Abdel-Wahab | 2020 | [19] |
| 3/24 | 13% | NGS | N.A. | America | Okamura | 2021 | [27] | ||
| 4/58 | 7% | ultra-deep targeted NGS | AC | China | Lin | 2019 | [70] | ||
| 3/32 | 9% | targeted NGS | AC | Chile, Japan | Narayan | 2019 | [73] | ||
| MYC | 6.8% | 51/760 | 7% | NGS | N.A. | America | Abdel-Wahab | 2020 | [19] |
| 2/24 | 8% | NGS | N.A. | America | Okamura | 2021 | [27] |
| Author | Origin | Histology | N | TMB (Mut/Mb [Range]) | TMB-H Definition | TMB-H | Ref. |
|---|---|---|---|---|---|---|---|
| Patel | India | N.A. | 43 | 5 (1–14) | - | - | [39] |
| Weinberg | America | N.A | 104 | - | ≥17 mut/Mb | 6/104 (5.8%) | [59] |
| Li | China | N.A. | 12 | 7.03 | - | - | [47] |
| Abdel-Wahab | America | N.A. | 760 | 2.6 (0–403) | ≥19.5 mut/Mb | 9/760 (1.2%) | [19] |
| Author | Origin | Histology | MSI Markers | MSI Definition | MSI | Ref. |
|---|---|---|---|---|---|---|
| Nagai | Japan | N.A. | D2S97, D6S477, D8S339, D9S131, D10S197, D17S796, D18S36, TP53 (17p12), DCC (18q21), APC (5q21) | Shifts in ≥30% of markers | 7/17 (41%) | [24] |
| Kim | Korea | N.A. | 3p12-22 (D3S1274, D3S4103, D3S1766) 5q11-23 (D5S107, D5S409, IRF1) 8p22-23 (D8S254, D8S261) 9p22 (IFNA, D9S126, D9S104) 13q13-14 (D13S118 and D13S133) 17p11-13 (D17S786, D17S796,TP53) 18q12-21 (D18S34) | Shifts in ≥1 marker | 3/15 (20%) | [31] |
| Nagahashi | Japan, Hungary | AC | NCI: BAT-25, BAT-26, D2S123, D5S346, D17S250 | Shifts in ≥2 markers | 9/34 (27%) | [35] |
| Patel | India | N.A. | Genome-wide analysis of 95 loci | N.A. | 0/43 (0%) | [39] |
| Abdel-Wahab | U.S. | N.A. | 114 loci | Shifts in ≥2 markers | 3/551 (1%) | [19] |
| Wistuba | Chile | AC | 81 loci on 3p, 8p, 9q and 22q | Shifts in ≥1 marker | 6/12 (50%) | [43] |
| Pandey | Chile, Korea, India | AC | Exome-wide analysis | MSI score > 0.35 | 3/152 (2%) | [46] |
| Li | China | N.A. | NGS | N.A. | 0/12 (0%) | [47] |
| Rashid | China | AC | NCI (BAT-25, BAT-26, D2S123, D5S346, D17S250) and TGFβRII | Shifts in ≥40% of D2S123, D5S346, D17S25, or alteration of BAT-25, BAT-26 or TGFβRII | 2/64 (3%) | [49] |
| Goeppert | Germany | AC | BAT25, BAT26, and CAT25 | Shifts in ≥2 markers | 1/69 (1%) | [52] |
| Yoshida | Japan | AC | p53, APC, DCC, NM23-H1, D2S123, D3S1029, D5S107, D17S261, D18S34 | Shifts in ≥33% of markers | 0/30 (0%) | [54] |
| Roa | Chile | AC | NCI: BAT25, BAT26, D2S123, D5S346, D17S250 and BAT40, D3S1067, D3S1286, D3S1262, D3S1478, D12S1638, D12S347, D16S265 | Shifts in >30% of markers | 6/59 (10%) | [55] |
| Weinberg | U.S. | N.A. | Targeted NGS over 7000 loci | N.A. | 1/104 (1%) | [59] |
| Target | Level | Malignancy | Agent | ORR | Ref. |
|---|---|---|---|---|---|
| ATM¥ | 1 | Prostate cancer | Olaparib | BRCA1, BRCA2, or ATM: 28/84 (33%) | [84] |
| ERBB2 * | 1 | Esophagogastric cancer | Pembrolizumab + trastuzumab + chemotherapy | 32/35 (91%) | [85] |
| Trastuzumab + chemotherapy | 139/294 (47%) | [86] | |||
| Trastuzumab deruxtecan | 61/119 (51%) | [87] | |||
| ERBB2 * | 1 | Breast cancer | Ado-trastuzumab emtansine | 173/397 (44%) | [88] |
| Lapatinib + letrozole | 31/111 (28%) | [89] | |||
| Lapatinib + capecitabine | 36/163 (22%) | [90] | |||
| Margetuximab + chemotherapy | 67/266 (25%) | [91] | |||
| Neratinib | 34/117 (29%) | [92] | |||
| Trastuzumab | 30/114 (26%) | [93] | |||
| Trastuzumab + pertuzumab + chemotherapy | 275/343 (80%) | [94] | |||
| Trastuzumab + tucatinib + capecitabine | 138/340 (41%) | [95] | |||
| Trastuzumab deruxtecan | 112/184 (61%) | [96] | |||
| ERBB2 * | 2 | Colorectal cancer | Lapatinib + trastuzumab | 9/32 (28%) | [97] |
| Trastuzumab + pertuzumab | 18/57 (32%) | [98] | |||
| Trastuzumab deruxtecan | 24/53 (45%) | [99] | |||
| ERBB2 * | 2 | Uterine serous carcinoma | Trastuzumab + carboplatin-taxol | 4/9 (44%) | [100] |
| ERBB2¥ | 2 | NSCLC | Ado-trastuzumab emtansine | 8/18 (44%) | [101] |
| Trastuzumab deruxtecan | 50/91 (55%) | [102] | |||
| PIK3CA¥ | 1 | Breast cancer | Alpelisib + fulvestrant | 21/121 (17% | [103] |
| TMB-H | 1 | Solid tumors | Pembrolizumab | 30/102 (29%) | [104] |
| MSI-H | 1 | Solid tumors | Pembrolizumab | 59/149 (40%) | [105] |
| MSI-H | 1 | Colorectal cancer | Nivolumab | 23/74 (31%) | [106] |
| Ipilumab + nivolumab | 65/119 (55%) | [107] |
| Target | Phase | Agent | Country | Trial ID |
|---|---|---|---|---|
| ERBB2 signal pathway components | 2 | FORFIRINOX + (cetuximab, trastuzumab, gefitinib, lapatinib, everolimus, sorafenib, or crizotinib) | China | NCT03768375 |
| ERBB2 signal pathway components | 2 | GEMOX + afatinib | China | NCT04183712 |
| ERBB2 overexpression/ amplification | 2 | Trastuzumab + pertuzumab | U.S. | NCT02091141 |
| ERBB2 overexpression/ amplification | 1,2 | Tucatinib + trastuzumab + (FOLFOX or CAPOX) | U.S. | NCT04430738 |
| ERBB2 overexpression/ amplification or mutations | 2, basket | Tucatinib + trastuzumab | U.S., Japan, Belgium | NCT04579380 |
| ERBB2 amplification | 2 | Zanidatamab | U.S., Canada, Chile, China, France, Italy, Korea, Spain, U.K. | NCT04466891 |
| KRAS (or NRAS) mutation | 1 | ELI-002 immunotherapy | U.S. | NCT04853017 |
| DNA repair gene mutations (including ARID1A, ATM, and others) | 2 | Olaparib | U.S. | NCT04042831 |
| TMB ≥ 10 mutations/Mb | 2 | Atezolizumab | U.S. | NCT02091141 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuipers, H.; de Bitter, T.J.J.; de Boer, M.T.; van der Post, R.S.; Nijkamp, M.W.; de Reuver, P.R.; Fehrmann, R.S.N.; Hoogwater, F.J.H. Gallbladder Cancer: Current Insights in Genetic Alterations and Their Possible Therapeutic Implications. Cancers 2021, 13, 5257. https://doi.org/10.3390/cancers13215257
Kuipers H, de Bitter TJJ, de Boer MT, van der Post RS, Nijkamp MW, de Reuver PR, Fehrmann RSN, Hoogwater FJH. Gallbladder Cancer: Current Insights in Genetic Alterations and Their Possible Therapeutic Implications. Cancers. 2021; 13(21):5257. https://doi.org/10.3390/cancers13215257
Chicago/Turabian StyleKuipers, Hendrien, Tessa J. J. de Bitter, Marieke T. de Boer, Rachel S. van der Post, Maarten W. Nijkamp, Philip R. de Reuver, Rudolf S. N. Fehrmann, and Frederik J. H. Hoogwater. 2021. "Gallbladder Cancer: Current Insights in Genetic Alterations and Their Possible Therapeutic Implications" Cancers 13, no. 21: 5257. https://doi.org/10.3390/cancers13215257