
Charting the Unknown Association of COVID-19 with Thyroid Cancer, Focusing on Differentiated Thyroid Cancer: A Call for Caution


Abstract
:Simple Summary
Abstract
1. Introduction
2. TC Epitomizes the Obesity-Related Cancers
3. Obesity in Relation to the Severity of COVID-19 in Non-Cancer and in Cancer Patients
4. Pursuing the Pathophysiological Landscape of the COVID 19–TC Association
5. The Impact of COVID-19 on the Oncological Strategy for DTC
5.1. Challenge I: Appropriate Patient Selection for Thyroid Fine-Needle Aspiration (FNA)
5.2. Challenge II: Schedule of DTC Surgery in an Overburdened Health System
5.3. Challenge III: Assessment of Delays and Disruptions in DTC Care Due to COVID-19
5.4. Challenge IV: The Safety of DTC Surgery in the COVID-19 Era
6. Discordant Data on the Impact of TC on COVID-19 Severity between Cancer Patients in General and (D)TC Patients
Are Obese Patients with (D)TC at Increased Risk for Unfavorable COVID-19 Outcomes?
7. The Hypothesis of the Oncogenic Potential of SARS-CoV-2
8. Future Perspectives
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 6 August 2021).
- Barasa, E.; Mbau, R.; Gilson, L. What Is Resilience and How Can It Be Nurtured? A Systematic Review of Empirical Literature on Organizational Resilience. Int. J. Health Policy Manag. 2018, 7, 491–503. [Google Scholar] [CrossRef] [PubMed]
- Nagai, H.; Kim, Y.H. Cancer prevention from the perspective of global cancer burden patterns. J. Thorac Dis. 2017, 9, 448–451. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Knaul, F.M.; Garcia, P.J.; Gospodarowicz, M.; Essue, B.M.; Lee, N.; Horton, R. The Lancet Commission on cancer and health systems: Harnessing synergies to achieve solutions. Lancet 2021, 6736, 19–21. [Google Scholar] [CrossRef]
- Jazieh, A.R.; Akbulut, H.; Curigliano, G.; Rogado, A.; Alsharm, A.A.; Razis, E.D.; Mula-Hussain, L.; Errihani, H.; Khattak, A.; De Guzman, R.B.; et al. Impact of the COVID-19 Pandemic on Cancer Care: A Global Collaborative Study. JCO Glob. Oncol. 2020, 6, 1428–1438. [Google Scholar] [CrossRef]
- Patt, D.; Gordan, L.; Diaz, M.; Okon, T.; Grady, L.; Harmison, M.; Markward, N.; Sullivan, M.; Peng, J.; Zhou, A. Impact of COVID-19 on Cancer Care: How the Pandemic Is Delaying Cancer Diagnosis and Treatment for American Seniors. JCO Clin. Cancer Inform. 2020, 4, 1059–1071. [Google Scholar] [CrossRef]
- London, J.W.; Fazio-Eynullayeva, E.; Palchuk, M.B.; Sankey, P.; McNair, C. Effects of the COVID-19 Pandemic on Cancer-Related Patient Encounters. JCO Clin. Cancer Inform. 2020, 4, 657–665. [Google Scholar] [CrossRef]
- Greenwood, E.; Swanton, C. Consequences of COVID-19 for cancer care a CRUK perspective. Nat. Rev. Clin. Oncol. 2021, 18, 3–4. [Google Scholar] [CrossRef]
- Bellou, V.; Tzoulaki, I.; van Smeden, M.; Moons, K.G.M.; Evangelou, E.; Belbasis, L. Prognostic factors for adverse outcomes in patients with COVID-19: A field-wide systematic review and meta-analysis. Eur. Respir. J. 2021, 2002964. [Google Scholar] [CrossRef]
- Caballero, B. Humans against Obesity: Who Will Win? Adv. Nutr. 2019, 10, S4–S9. [Google Scholar] [CrossRef]
- Colditz, G.A.; Lindsay, L. Obesity and cancer: Evidence, impact, and future directions. Clin. Chem. 2018, 64, 154–162. [Google Scholar] [CrossRef] [Green Version]
- Poly, T.N.; Islam, M.M.; Yang, H.C.; Lin, M.C.; Jian, W.S.; Hsu, M.H.; Jack Li, Y.C. Obesity and Mortality Among Patients Diagnosed With COVID-19: A Systematic Review and Meta-Analysis. Front. Med. 2021, 8, 620044. [Google Scholar] [CrossRef]
- Wichmann, I.A.; Cuello, M.A. Obesity and gynecological cancers: A toxic relationship. Int. J. Gynaecol. Obstet. 2021, 155, 123–134. [Google Scholar] [CrossRef]
- Derosa, L.; Melenotte, C.; Griscelli, F.; Gachot, B.; Marabelle, A.; Kroemer, G.; Zitvogel, L. The immuno-oncological challenge of COVID-19. Nat. Cancer 2020, 1, 946–964. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [Green Version]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Zhai, M.; Zhang, D.; Long, J.; Gong, Y.; Ye, F.; Liu, S.; Li, Y. The global burden of thyroid cancer and its attributable risk factor in 195 countries and territories: A systematic analysis for the Global Burden of Disease Study. Cancer Med. 2021, 10, 4542–4554. [Google Scholar] [CrossRef]
- Pellegriti, G.; Frasca, F.; Regalbuto, C.; Squatrito, S.; Vigneri, R. Worldwide increasing incidence of thyroid cancer: Update on epidemiology and risk factors. J. Cancer Epidemiol. 2013, 2013, 65212. [Google Scholar] [CrossRef] [Green Version]
- Morris, L.G.; Myssiorek, D. Improved detection does not fully explain the rising incidence of well-differentiated thyroid cancer: A population-based analysis. Am. J. Surg. 2010, 200, 454–461. [Google Scholar] [CrossRef] [Green Version]
- Schmid, D.; Ricci, C.; Behrens, G.; Leitzmann, M.F. Adiposity and risk of thyroid cancer: A systematic review and meta-analysis. Obes. Rev. 2015, 16, 1042–1054. [Google Scholar] [CrossRef]
- Kitahara, C.M.; Pfeiffer, R.M.; Sosa, J.A.; Shiels, M.S. Impact of overweight and obesity on US papillary thyroid cancer incidence trends (1995–2015). J. Nat. Cancer Inst. 2020, 112, 810–817. [Google Scholar] [CrossRef]
- Trimboli, P.; Camponovo, C.; Scappaticcio, L.; Bellastella, G.; Piccardo, A.; Rotondi, M. Thyroid sequelae of COVID-19: A systematic review of reviews. Rev. Endocr. Metab. Disord. 2021, 22, 485–491. [Google Scholar] [CrossRef]
- Ma, J.; Huang, M.; Wang, L.; Ye, W.; Tong, Y.; Wang, H. Obesity and risk of thyroid cancer: Evidence from a meta-analysis of 21 observational studies. Med. Sci. Monit. 2015, 21, 283–291. [Google Scholar]
- Lauby-Secretan, B.; Scoccianti, C.; Loomis, D.; Grosse, Y.; Bianchini, F.; Straif, K. Body Fatness and Cancer Viewpoint of the IARC Working Group. N. Engl. J. Med. 2016, 375, 794–798. [Google Scholar] [CrossRef] [Green Version]
- Sung, H.; Siegel, R.L.; Torre, L.A.; Pearson-Stuttard, J.; Islami, F.; Fedewa, S.A.; Goding Sauer, A.; Shuval, K.; Gapstur, S.M.; Jacobs, E.J.; et al. Global patterns in excess body weight and the associated cancer burden. CA Cancer J. Clin. 2019, 69, 88–112. [Google Scholar] [CrossRef]
- Bruno, D.S.; Berger, N.A. Impact of bariatric surgery on cancer risk reduction. Ann. Ttransl. Med. 2020, 8, S13. [Google Scholar] [CrossRef]
- Marcello, M.A.; Cunha, L.L.; Batista, F.A.; Ward, L.S. Obesity and thyroid cancer. Endocr. Relat. Cancer 2014, 21, T255–T271. [Google Scholar] [CrossRef]
- Zhao, Z.; Yin, X.D.; Zhang, X.H.; Li, Z.W.; Wang, D.W. Comparison of pediatric and adult medullary thyroid carcinoma based on SEER program. Sci. Rep. 2020, 10, 13310. [Google Scholar] [CrossRef]
- Bible, K.C.; Kebebew, E.; Brierley, J.; Brito, J.P.; Cabanillas, M.E.; Clark, T.J., Jr.; Di Cristofano, A.; Foote, R.; Giordano, T.; Kasperbauer, J.; et al. American Thyroid Association Guidelines for Management of Patients with Anaplastic Thyroid Cancer. Thyroid 2021, 31, 337–386. [Google Scholar] [CrossRef]
- Masone, S.; Velotti, N.; Savastano, S.; Filice, E.; Serao, R.; Vitiello, A.; Berardi, G.; Schiavone, V.; Musella, M. Morbid Obesity and Thyroid Cancer Rate. A Review of Literature. J. Clin. Med. 2021, 10, 1894. [Google Scholar] [CrossRef]
- Zhao, Z.G.; Guo, X.G.; Ba, C.X.; Wang, W.; Yang, Y.Y.; Wang, J.; Cao, H.Y. Overweight, obesity and thyroid cancer risk: A meta-analysis of cohort studies. J. Int. Med. Res. 2012, 40, 2041–2050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zane, M.; Parello, C.; Pennelli, G.; Townsend, D.M.; Merigliano, S.; Boscaro, M.; Toniato, A.; Baggio, G.; Pelizzo, M.R.; Rubello, D.; et al. Estrogen and thyroid cancer is a stem affair: A preliminary study. Biomed. Pharmacother. 2017, 85, 399–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obeid, S.; Hebbard, L. Role of adiponectin and its receptors in cancer. Cancer Biol. Med. 2012, 9, 213–220. [Google Scholar] [PubMed]
- Taylor, E.B. The complex role of adipokines in obesity, inflammation, and autoimmunity. Clin. Sci. 2021, 135, 731–752. [Google Scholar] [CrossRef]
- Ouchi, N.; Walsh, K. Adiponectin as an anti-inflammatory factor. Clin. Chim. Acta 2007, 380, 24–30. [Google Scholar] [CrossRef] [Green Version]
- Rotondi, M.; Castagna, M.G.; Cappelli, C.; Ciuoli, C.; Coperchini, F.; Chiofalo, F.; Maino, F.; Palmitesta, P.; Chiovato, L.; Pacini, F. Obesity Does Not Modify the Risk of Differentiated Thyroid Cancer in a Cytological Series of Thyroid Nodules. Eur. Thyroid J. 2016, 5, 125–131. [Google Scholar] [CrossRef] [Green Version]
- Farfel, A.; Kark, J.D.; Derazne, E.; Tzur, D.; Barchana, M.; Lazar, L.; Afek, A.; Shamiss, A. Predictors for thyroid carcinoma in Israel: A national cohort of 1,624,310 adolescents followed for up to 40 years. Thyroid 2014, 24, 987–993. [Google Scholar] [CrossRef]
- Fussey, J.M.; Beaumont, R.N.; Wood, A.R.; Vaidya, B.; Smith, J.; Tyrrell, J. Does Obesity Cause Thyroid Cancer? A Mendelian Randomization Study. J. Clin. Endocrinol. Metab. 2020, 105, e2398–e2407. [Google Scholar] [CrossRef]
- Kumar, A.; Arora, A.; Sharma, P.; Anikhindi, S.A.; Bansal, N.; Singla, V.; Khare, S.; Srivastava, A. Is diabetes mellitus associated with mortality and severity of COVID-19? A meta-analysis. Diabetes Metab. Syndr. 2020, 14, 535–545. [Google Scholar] [CrossRef]
- Vuorio, A.; Watts, G.F.; Kovanen, P.T. Familial hypercholesterolaemia and COVID-19: Triggering of increased sustained cardiovascular risk. J. Intern. Med. 2020, 287, 746–747. [Google Scholar] [CrossRef] [Green Version]
- Mehra, M.R.; Desai, S.S.; Kuy, S.; Henry, T.D.; Patel, A.N. Cardiovascular Disease, Drug Therapy, and Mortality in COVID-19. N. Engl. J. Med. 2020, 382, e102. [Google Scholar] [CrossRef]
- Mohammad, S.; Aziz, R.; Al Mahri, S.; Malik, S.S.; Haji, E.; Khan, A.H.; Khatlani, T.S.; Bouchama, A. Obesity and COVID-19: What makes obese host so vulnerable? Immun. Ageing 2021, 18, 1. [Google Scholar] [CrossRef]
- Bhattacharya, I.; Ghayor, C.; Pérez Dominguez, A.; Weber, F.E. From Influenza Virus to Novel Corona Virus (SARS-CoV-2)–The Contribution of Obesity. Front. Endocrinol. 2020, 11, 556962. [Google Scholar] [CrossRef]
- Stefan, N.; Birkenfeld, A.L.; Schulze, M.B.; Ludwig, D.S. Obesity and impaired metabolic health in patients with COVID-19. Nat. Rev. Endocrinol. 2020, 16, 341–342. [Google Scholar] [CrossRef] [Green Version]
- Park, R.; Wulff-Burchfield, E.; Sun, W.; Kasi, A. Is obesity a risk factor in cancer patients with COVID-19? Future Oncol. 2021, 17, 3541–3544. [Google Scholar] [CrossRef]
- Cava, E.; Neri, B.; Carbonelli, M.G.; Riso, S.; Carbone, S. Obesity pandemic during COVID-19 outbreak: Narrative review and future considerations. Clin. Nutr. 2021, 40, 1637–1643. [Google Scholar] [CrossRef]
- Yang, J.; Hu, J.; Zhu, C. Obesity aggravates COVID-19: A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 257–261. [Google Scholar] [CrossRef]
- Albiges, L.; Foulon, S.; Bayle, A.; Gachot, B.; Pommeret, F.; Willekens, C.; Stoclin, A.; Merad, M.; Griscelli, F.; Lacroix, L.; et al. Determinants of the outcomes of patients with cancer infected with SARS-CoV-2: Results from the Gustave Roussy cohort. Nat. Cancer 2020, 1, 965–975. [Google Scholar] [CrossRef]
- Kuderer, N.M.; Choueiri, T.K.; Shah, D.P.; Shyr, Y.; Rubinstein, S.M.; Rivera, D.R.; Shete, S.; Hsu, C.Y.; Desai, A.; de Lima Lopes, G.; et al. COVID-19 and Cancer Consortium. Clinical impact of COVID-19 on patients with cancer (CCC19): A cohort study. Lancet 2020, 395, 1907–1918. [Google Scholar] [CrossRef]
- Park, R.; Wulff-Burchfield, E.M.; Mehta, K.; Sun, W.; Kasi, A. Prognostic impact of obesity in cancer patients with COVID-19 infection: A systematic review and meta-analysis. J. Clin. Oncol. 2021, 39, e18578. [Google Scholar] [CrossRef]
- Avgerinos, K.I.; Spyrou, N.; Mantzoros, C.S.; Dalamaga, M. Obesity and cancer risk: Emerging biological mechanisms and perspectives. Metabolism 2019, 92, 121–135. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Roche, L.; Mesta, F. Oxidative Stress as Key Player in Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV) Infection. Arch. Med. Res. 2020, 51, 384–387. [Google Scholar] [CrossRef] [PubMed]
- Ntyonga-Pono, M.P. COVID-19 infection and oxidative stress: An under-explored approach for prevention and treatment? Pan Afr. Med. J. 2020, 35, 12. [Google Scholar] [CrossRef] [PubMed]
- Hayes, J.D.; Dinkova-Kostova, A.T.; Tew, K.D. Oxidative Stress in Cancer. Cancer Cell 2020, 38, 167–197. [Google Scholar] [CrossRef] [PubMed]
- Arfin, S.; Jha, N.K.; Jha, S.K.; Kesari, K.K.; Ruokolainen, J.; Roychoudhury, S.; Rathi, B.; Kumar, D. Oxidative stress in cancer cell metabolism. Antioxidants 2021, 10, 642. [Google Scholar] [CrossRef] [PubMed]
- Dröge, W. Free radicals in the physiological control of cell function. Physiol. Rev. 2002, 82, 47–95. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.L.; Sinha, S.; Lindner, A.B. The good, the bad, and the ugly of ROS: New insights on aging and aging-related diseases from eukaryotic and prokaryotic model organisms. Oxidative Med. Cell. Longev. 2018, 2018, 1941285. [Google Scholar] [CrossRef]
- Liao, Z.; Damien, C.; Tan, N. Reactive oxygen species: A volatile driver of field cancerization and metastasis. Mol. Cancer 2019, 18, 65. [Google Scholar] [CrossRef]
- Deligiorgi, M.V.; Liapi, C.; Trafalis, D.T. How Far Are We from Prescribing Fasting as Anticancer Medicine? Int. J. Mol. Sci. 2020, 21, 9175. [Google Scholar] [CrossRef]
- Ameziane El Hassani, R.; Buffet, C.; Leboulleux, S.; Dupuy, C. Oxidative stress in thyroid carcinomas: Biological and clinical significance. Endocr. Relat. Cancer 2019, 26, R131–R143. [Google Scholar] [CrossRef] [Green Version]
- Ni, W.; Yang, X.; Yang, D.; Bao, J.; Li, R.; Xiao, Y.; Hou, C.; Wang, H.; Liu, J.; Yang, D.; et al. Role of angiotensin-converting enzyme 2 (ACE2) in COVID-19. Crit. Care 2020, 24, 422. [Google Scholar] [CrossRef]
- Scappaticcio, L.; Pitoia, F.; Esposito, K.; Piccardo, A.; Trimboli, P. Impact of COVID-19 on the thyroid gland: An update. Rev. Endocr. Metab. Disord. 2020, 2020, 1–13. [Google Scholar] [CrossRef]
- Davis, P.J.; Lin, H.Y.; Hercbergs, A.; Keating, K.A.; Mousa, S.A. Coronaviruses and Integrin αvβ3: Does Thyroid Hormone Modify the Relationship? Endocr. Res. 2020, 45, 210–215. [Google Scholar] [CrossRef]
- McFadyen, J.D.; Stevens, H.; Peter, K. The Emerging Threat of (Micro)Thrombosis in COVID-19 and Its Therapeutic Implications. Circ. Res. 2020, 127, 571–587. [Google Scholar] [CrossRef]
- Croce, L.; Gangemi, D.; Ancona, G.; Liboà, F.; Bendotti, G.; Minelli, L.; Chiovato, L. The cytokine storm and thyroid hormone changes in COVID-19. J. Endocrinol. Invest. 2021, 44, 891–904. [Google Scholar] [CrossRef]
- Deligiorgi, M.V.; Trafalis, D.T. Papillary Thyroid Carcinoma Intertwined with Hashimoto’s Thyroiditis: An Intriguing Correlation, Knowledges on Thyroid Cancer, Omer Engin, IntechOpen. Available online: https://www.intechopen.com/chapters/66252 (accessed on 17 August 2021).
- Ruggeri, R.M.; Campennì, A.; Deandreis, D.; Siracusa, M.; Tozzoli, R.; Petranović Ovčariček, P.; Giovanella, L. SARS-COV-2-related immune-inflammatory thyroid disorders: Facts and perspectives. Expert Rev. Clin. Immunol. 2021, 17, 737–759. [Google Scholar] [CrossRef]
- Palladino, R.; Migliatico, I.; Sgariglia, R.; Nacchio, M.; Iaccarino, A.; Malapelle, U.; Vigliar, E.; Salvatore, D.; Troncone, G.; Bellevicine, C. Thyroid fine-needle aspiration trends before, during, and after the lockdown: What we have learned so far from the COVID-19 pandemic. Endocrine 2021, 71, 20–25. [Google Scholar] [CrossRef]
- Vigliar, E.; Cepurnaite, R.; Alcaraz-Mateos, E.; Ali, S.Z.; Baloch, Z.W.; Bellevicine, C.; Bongiovanni, M.; Botsun, P.; Bruzzese, D.; Bubendorf, L.; et al. Global impact of the COVID-19 pandemic on cytopathology practice: Results from an international survey of laboratories in 23 countries. Cancer Cytopathol. 2020, 128, 885–894. [Google Scholar] [CrossRef]
- Zhang, D.; Fu, Y.; Zhou, L.; Liang, N.; Wang, T.; Del Rio, P.; Rausei, S.; Boni, L.; Park, D.; Jafari, J.; et al. Thyroid surgery during coronavirus-19 pandemic phases I, II and III: Lessons learned in China, South Korea, Iran and Italy. J. Endocrinol. Investig. 2021, 44, 1065–1073. [Google Scholar] [CrossRef]
- COVIDSurg Collaborative. Elective surgery cancellations due to the COVID-19 pandemic: Global predictive modelling to inform surgical recovery plans. Br. J. Surg. 2020, 107, 1440–1449. [Google Scholar]
- Agcaoglu, O.; Sezer, A.; Makay, O.; Erdogan, M.F.; Bayram, F.; Guldiken, S.; Raffaelli, M.; Sonmez, Y.A.; Lee, Y.S.; Vamvakidis, K.; et al. Management of endocrine surgical disorders during COVID-19 pandemic: Expert opinion for non-surgical options. Updates Surg. 2021, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Baud, G.; Brunaud, L.; Lifante, J.C.; Tresallet, C.; Sebag, F.; Bizard, J.P.; Mathonnet, M.; Menegaux, F.; Caiazzo, R.; Mirallié, É.; et al. Endocrine surgery during and after the COVID-19 epidemic: Expert guidelines from AFCE. J. Visc. Surg. 2020, 157, S44–S51. [Google Scholar] [CrossRef] [PubMed]
- Aygun, N.; Iscan, Y.; Ozdemir, M.; Soylu, S.; Aydin, O.U.; Sormaz, I.C.; Dural, A.C.; Sahbaz, N.A.; Teksoz, S.; Makay, O.; et al. Endocrine Surgery during the COVID-19 Pandemic: Recommendations from the Turkish Association of Endocrine Surgery. Sisli Etfal Hastan. Tip Bul. 2020, 54, 117–131. [Google Scholar] [PubMed]
- Martins, J.; Villagelin, D.; Carvalho, G.A.; Vaisman, F.; Teixeira, P.; Scheffel, R.S.; Sgarbi, J.A. Management of thyroid disorders during the COVID-19 outbreak: A position statement from the Thyroid Department of the Brazilian Society of Endocrinology and Metabolism (SBEM). Arch. Endocrinol. Metab. 2021, 65, 368–375. [Google Scholar] [CrossRef]
- Riera, R.; Bagattini, Â.M.; Pacheco, R.L.; Pachito, D.V.; Roitberg, F.; Ilbawi, A. Delays and Disruptions in Cancer Health Care Due to COVID-19 Pandemic: Systematic Review. JCO Glob. Oncol. 2021, 7, 311–323. [Google Scholar] [CrossRef]
- Bakkar, S.; Al-Omar, K.; Aljarrah, Q.; Al-Dabbas, M.; Al-Dabbas, N.; Samara, S.; Miccoli, P. Impact of COVID-19 on thyroid cancer surgery and adjunct therapy. Updates Surg. 2020, 72, 867–869. [Google Scholar] [CrossRef]
- Hojaij, F.C.; Chinelatto, L.A.; Boog, G.H.P.; Kasmirski, J.A.; Lopes, J.V.Z.; Medeiros, V.M.B. Head and Neck Practice in the COVID-19 Pandemics Today: A Rapid Systematic Review. Int. Arch. Otorhinolaryngol. 2020, 24, 518–526. [Google Scholar] [CrossRef]
- Scappaticcio, L.; Maiorino, M.I.; Iorio, S.; Camponovo, C.; Piccardo, A.; Bellastella, G.; Docimo, G.; Esposito, K.; Trimboli, P. Thyroid surgery during the COVID-19 pandemic: Results from a systematic review. J. Endocrinolog. Investig. 2021, Jul 19, 1–8. [Google Scholar] [CrossRef]
- COVIDSurg Collaborative. Head and neck cancer surgery during the COVID-19 pandemic: An international, multicenter, observational cohort study. Cancer 2021, 127, 2476–2488. [Google Scholar] [CrossRef]
- Zhang, L.; Zhu, F.; Xie, L.; Wang, C.; Wang, J.; Chen, R.; Jia, P.; Guan, H.Q.; Peng, L.; Chen, Y.; et al. Clinical characteristics of COVID-19-infected cancer patients: A retrospective case study in three hospitals within Wuhan, China. Ann. Oncol. 2020, 31, 894–901. [Google Scholar] [CrossRef]
- Tagliamento, M.; Agostinetto, E.; Bruzzone, M.; Ceppi, M.; Saini, K.S.; de Azambuja, E.; Punie, K.; Westphalen, C.B.; Morgan, G.; Pronzato, P.; et al. Mortality in adult patients with solid or hematological malignancies and SARS-CoV-2 infection with a specific focus on lung and breast cancers: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2021, 163, 103365. [Google Scholar] [CrossRef]
- Dai, M.; Liu, D.; Liu, M.; Zhou, F.; Li, G.; Chen, Z.; Zhang, Z.; You, H.; Wu, M.; Zheng, Q.; et al. Patients with cancer appear more vulnerable to SARS-CoV-2: A multicenter study during the COVID-19 outbreak. Cancer Discov. 2020, 10, 783. [Google Scholar]
- Wang, Q.; Berger, N.A.; Xu, R. Analyses of Risk, Racial Disparity, and Outcomes among US Patients with Cancer and COVID-19 Infection. JAMA Oncol. 2021, 7, 220–227. [Google Scholar] [CrossRef]
- Addeo, A.; Friedlaender, A. Cancer and COVID-19: Unmasking their ties. Cancer Treat. Rev. 2020, 88, 102041. [Google Scholar] [CrossRef]
- Van Dam, P.A.; Huizing, M.; Mestach, G.; Dierckxsens, S.; Tjalma, W.; Trinh, X.B.; Papadimitriou, K.; Altintas, S.; Vermorken, J.; Vulsteke, C.; et al. SARS-CoV-2 and cancer: Are they really partners in crime? Cancer Treat. Rev. 2020, 89, 102068. [Google Scholar] [CrossRef]
- Sahin, M.; Haymana, C.; Demirci, I.; Tasci, I.; Rıfat, E.; Unluturk, U.; Satman, I.; Demir, T.; Cakal, E.; Ata, N.; et al. The clinical outcomes of COVID-19 infection in patients with a history of thyroid cancer: A nationwide study. Clin. Endocrinol. 2021, 95, 628–637. [Google Scholar] [CrossRef]
- Kathuria-Prakash, N.; Mosaferi, T.; Xie, M.; Antrim, L.; Angell, T.E.; In, G.K.; Su, M.A.; Lechner, M.G. COVID-19 Outcomes of Patients with Differentiated Thyroid Cancer: A Multicenter Los Angeles Cohort Study. Endocr. Pract. 2021, 27, 90–94. [Google Scholar] [CrossRef]
- Walitt, B.; Bartrum, E. A clinical primer for the expected and potential post-COVID-19 syndromes. Pain Rep. 2021, 6, e887. [Google Scholar] [CrossRef]
- Proal, A.D.; VanElzakker, M.B. Long COVID or Post-acute Sequelae of COVID-19 (PASC): An Overview of Biological Factors That May Contribute to Persistent Symptoms. Front. Microbiol. 2021, 12, 1494. [Google Scholar] [CrossRef]
- Chippa, V.; Aleem, A.; Anjum, F. Post Acute Coronavirus (COVID-19) Syndrome. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Ciuffo, G. Innesto positivo con filtrato di verruca volgare. Giorn. Italy Mal. Venereol. 1907, 48, 12–17. [Google Scholar]
- Rous, P. A transmissible avian neoplasm. (Sarcoma of the common fowl.). J. Exp. Med. 1910, 12, 696–705. [Google Scholar] [CrossRef] [PubMed]
- Mesri, E.A.; Feitelson, M.A.; Munger, K. Human viral oncogenesis: A cancer hallmarks analysis. Cell Host Microbe 2014, 15, 266–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagano, J.S.; Blaser, M.; Buendia, M.A.; Damania, B.; Khalili, K.; Raab-Traub, N.; Roizman, B. Infectious agents and cancer: Criteria for a causal relation. Semin. Cancer Biol. 2004, 14, 453–471. [Google Scholar] [CrossRef] [PubMed]
- Evans, A.S.; Mueller, N.E. Viruses and cancer. Causal associations. Ann. Epidemiol. 1990, 1, 71–92. [Google Scholar] [CrossRef]
- Alhusseini, L.B.; Yassen, L.T.; Kouhsari, E.; Al Marjani, M.F. Persistence of SARS-CoV-2: A new paradigm of COVID-19 management. Ann. Ig. 2021, 33, 426–432. [Google Scholar]
- Stingi, A.; Cirillo, L. SARS-CoV-2 infection and cancer: Evidence for and against a role of SARS-CoV-2 in cancer onset. BioEssays 2021, 43, 16–21. [Google Scholar] [CrossRef]
- Alpalhão, M.; Ferreira, J.A.; Filipe, P. Persistent SARS-CoV-2 infection and the risk for cancer. Med. Hypotheses 2020, 14, 109882. [Google Scholar] [CrossRef]
- Dyson, N.J. RB1: A prototype tumor suppressor and an enigma. Genes Dev. 2016, 30, 1492–1502. [Google Scholar] [CrossRef] [Green Version]
- Anwar, F.; Emond, M.J.; Schmidt, R.A.; Hwang, H.C.; Bronner, M.P. Retinoblastoma expression in thyroid neoplasms. Modern Pathol. 2000, 13, 562–569. [Google Scholar] [CrossRef]
- Park, R.; Jang, M.; Park, Y.I.; Park, Y.; Namkoong, S.; Lee, J.I.; Park, J. Elevated Levels of CTRP1 in Obesity Contribute to Tumor Progression in a p53-Dependent Manner. Cancers 2021, 13, 3619. [Google Scholar] [CrossRef]
- ClinicalTrials.gov Identifier. Available online: https://clinicaltrials.gov/NCT04370834 (accessed on 14 September 2021).
- Weng, Y.S.; Tseng, H.Y.; Chen, Y.A.; Shen, P.C.; Al Haq, A.T.; Chen, L.M.; Tung, Y.C.; Hsu, H.L. MCT-1/miR-34a/IL-6/IL-6R signaling axis promotes EMT progression, cancer stemness and M2 macrophage polarization in triple-negative breast cancer. Mol. Cancer 2019, 18, 42. [Google Scholar] [CrossRef] [Green Version]
- Alraouji, N.N.; Al-Mohanna, F.H.; Ghebeh, H.; Arafah, M.; Almeer, R.; Al-Tweigeri, T.; Aboussekhra, A. Tocilizumab potentiates cisplatin cytotoxicity and targets cancer stem cells in triple-negative breast cancer. Mol. Carcinog. 2020, 59, 1041–1051. [Google Scholar] [CrossRef]
- Tleyjeh, I.M.; Kashour, Z.; Damlaj, M.; Riaz, M.; Tlayjeh, H.; Altannir, M.; Altannir, Y.; Al-Tannir, M.; Tleyjeh, R.; Hassett, L.; et al. Efficacy and safety of tocilizumab in COVID-19 patients: A living systematic review and meta-analysis. Clin. Microbiol. Infect. 2021, 27, 215–227. [Google Scholar] [CrossRef]
- Dalamaga, M.; Karampela, I.; Mantzoros, C.S. Commentary: Phosphodiesterase 4 inhibitors as potential adjunct treatment targeting the cytokine storm in COVID-19. Metabolism 2020, 109, 154282. [Google Scholar] [CrossRef]
- Peng, T.; Gong, J.; Jin, Y.; Zhou, Y.; Tong, R.; Wei, X.; Bai, L.; Shi, J. Inhibitors of phosphodiesterase as cancer therapeutics. Eur. J. Med. Chem. 2018, 150, 742–756. [Google Scholar] [CrossRef] [Green Version]
- Sponziello, M.; Verrienti, A.; Rosignolo, F.; De Rose, R.F.; Pecce, V.; Maggisano, V.; Durante, C.; Bulotta, S.; Damante, G.; Giacomelli, L.; et al. PDE5 expression in human thyroid tumors and effects of PDE5 inhibitors on growth and migration of cancer cells. Endocrine 2015, 50, 434–441. [Google Scholar] [CrossRef]
- Beltrán-García, J.; Osca-Verdegal, R.; Pallardó, F.V.; Ferreres, J.; Rodríguez, M.; Mulet, S.; Sanchis-Gomar, F.; Carbonell, N.; García-Giménez, J.L. Oxidative Stress and Inflammation in COVID-19-Associated Sepsis: The Potential Role of Anti-Oxidant Therapy in Avoiding Disease Progression. Antioxidants 2020, 9, 936. [Google Scholar] [CrossRef]
- Assi, M. The differential role of reactive oxygen species in early and late stages of cancer. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2017, 313, R646–R653. [Google Scholar] [CrossRef] [Green Version]
- Kramer, C.K.; Zinman, B.; Retnakaran, R. Are metabolically healthy overweight and obesity benign conditions? A systematic review and meta-analysis. Ann. Intern. Med. 2013, 159, 758–769. [Google Scholar] [CrossRef]
- Kwon, H.; Chang, Y.; Cho, A.; Ahn, J.; Park, S.E.; Park, C.Y.; Lee, W.Y.; Oh, K.W.; Park, S.W.; Shin, H.; et al. Metabolic Obesity Phenotypes and Thyroid Cancer Risk: A Cohort Study. Thyroid 2019, 29, 349–358. [Google Scholar] [CrossRef]
- Mayoral, L.P.; Andrade, G.M.; Mayoral, E.P.; Huerta, T.H.; Canseco, S.P.; Rodal Canales, F.J.; Cabrera-Fuentes, H.A.; Cruz, M.M.; Pérez Santiago, A.D.; Alpuche, J.J.; et al. Obesity subtypes, related biomarkers & heterogeneity. Indian J. Med. Res. 2020, 151, 11–21. [Google Scholar]
- Vasileva, L.V.; Marchev, A.S.; Georgiev, M.I. Causes and solutions to “globesity”: The new fa(s)t alarming global epidemic. Food Chem. Toxicol. 2018, 121, 173–193. [Google Scholar] [CrossRef]
- Blüher, M. Obesity: Global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef]
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metabolism 2019, 92, 6–10. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://www.cdc.gov/obesity/data/obesity-and-covid-19.html (accessed on 13 September 2021).
- Magreni, A.; Bann, D.V.; Schubart, J.R.; Goldenberg, D. The effects of race and ethnicity on thyroid cancer incidence. JAMA Otolaryngol. Head Neck Surg. 2015, 141, 319–323. [Google Scholar] [CrossRef] [Green Version]
- Orosco, R.K.; Hussain, T.; Noel, J.E.; Chang, D.C.; Dosiou, C.; Mittra, E.; Divi, V.; Orloff, L.A. Radioactive iodine in differentiated thyroid cancer: A national database perspective. Endocr. Relat. Cancer 2019, 26, 795–802. [Google Scholar] [CrossRef]
- Du, W.; Dong, Q.; Lu, X.; Liu, X.; Wang, Y.; Li, W.; Pan, Z.; Gong, Q.; Liang, C.; Gao, G. Iodine-131 therapy alters the immune/inflammatory responses in the thyroids of patients with Graves’ disease. Exp. Ther. Med. 2017, 13, 1155–1159. [Google Scholar] [CrossRef] [Green Version]
- Riley, A.S.; McKenzie, G.; Green, V.; Schettino, G.; England, R.; Greenman, J. The effect of radioiodine treatment on the diseased thyroid gland. Int. J. Radiat. Biol. 2019, 95, 1718–1727. [Google Scholar] [CrossRef]
- Galimberti, S.; Petrini, M.; Baratè, C.; Ricci, F.; Balducci, S.; Grassi, S.; Guerrini, F.; Ciabatti, E.; Mechelli, S.; Di Paolo, A.; et al. Tyrosine Kinase Inhibitors Play an Antiviral Action in Patients Affected by Chronic Myeloid Leukemia: A Possible Model Supporting Their Use in the Fight Against SARS-CoV-2. Front. Oncol. 2020, 10, 1428. [Google Scholar] [CrossRef]
- Pillaiyar, T.; Laufer, S. Kinases as Potential Therapeutic Targets for Anti-coronaviral Therapy. J. Med. Chem. 2021. [Google Scholar] [CrossRef]
- Haugen, B.R. Drugs that suppress TSH or cause central hypothyroidism. Best Pract. Res. Clin. Endocrinol. Metab. 2009, 23, 793–800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sohrabpour, S.; Heidari, F.; Karimi, E.; Ansari, R.; Tajdini, A.; Heidari, F. Subacute Thyroiditis in COVID-19 Patients. Eur. Thyroid J. 2021, 9, 321–323. [Google Scholar] [CrossRef] [PubMed]
- Brancatella, A.; Ricci, D.; Cappellani, D.; Viola, N.; Sgrò, D.; Santini, F.; Latrofa, F. Is subacute thyroiditis an underestimated manifestation of SARS-CoV-2 infection? Insights from a case series. J. Clin. Endocrinol. Metab. 2020, 105, e3742–e3746. [Google Scholar] [CrossRef] [PubMed]
- Ucan, B.; Delibasi, T.; Cakal, E.; Arslan, M.S.; Bozkurt, N.C.; Demirci, T.; Ozbek, M.; Sahin, M. Caso de carcinoma papilar de tiroide mascarado por tireoidite subaguda. Arq. Bras. Endocrinol. Metab. 2014, 58, 851–854. [Google Scholar] [CrossRef] [Green Version]
- Azer, P.; Zhai, J.; Yu, R. Atypical de Quervain’s thyroiditis masquerading as papillary thyroid cancer. Endocrinol. Nutr. 2013, 60, 158–159. [Google Scholar] [CrossRef]
- Gül, N.; Üzüm, A.K.; Selçukbiricik, Ö.S.; Yegen, G.; Tanakol, R.; Aral, F. Prevalence of papillary thyroid cancer in subacute thyroiditis patients may be higher than it is presumed: Retrospective analysis of 137 patients. Radiol. Oncol. 2018, 52, 257–262. [Google Scholar] [CrossRef] [Green Version]
- Škorić, L.; Glasnović, A.; Petrak, J. A publishing pandemic during the COVID-19 pandemic: How challenging can it become? Croat. Med. J. 2020, 61, 79–81. [Google Scholar] [CrossRef]
- Chablani, S.V.; Sabra, M.M. Thyroid cancer and telemedicine during the COVID-19 pandemic. J. Endocr. Soc. 2021, 5, bvab059. [Google Scholar] [CrossRef]
- Serafini, G.; Parmigiani, B.; Amerio, A.; Aguglia, A.; Sher, L.; Amore, M. The psychological impact of COVID-19 on the mental health in the general population. QJM 2020, 113, 229–235. [Google Scholar] [CrossRef]
- Graves, C.E.; Goyal, N.; Levin, A.; Nuno, M.A.; Kim, J.; Campbell, M.J.; Shen, W.T.; Gosnell, J.E.D.; Roman, S.; Sosa, J.A.; et al. Anxiety and Fear During the Covid-19 Pandemic: A Web-Based Survey of Thyroid Cancer Survivors. J. Endocr. Soc. 2021, 5, A836. [Google Scholar] [CrossRef]
- Stipcević, T.; Pivac, N.; Kozarić-Kovacić, D.; Mück-Seler, D. Thyroid activity in patients with major depression. Coll. Antropol. 2008, 32, 973–976. [Google Scholar]
- Olff, M.; Güzelcan, Y.; de Vries, G.J.; Assies, J.; Gersons, B.P. HPA- and HPT-axis alterations in chronic posttraumatic stress disorder. Psychoneuroendocrinology 2006, 31, 1220–1230. [Google Scholar] [CrossRef]
- Siegmann, E.M.; Müller, H.; Luecke, C.; Philipsen, A.; Kornhuber, J.; Grömer, T.W. Association of Depression and Anxiety Disorders With Autoimmune Thyroiditis: A Systematic Review and Meta-analysis. JAMA Psychiatry 2018, 75, 577–584. [Google Scholar] [CrossRef] [Green Version]
- Feng, G.; Kang, C.; Yuan, J.; Zhang, Y.; Wei, Y.; Xu, L.; Zhou, F.; Fan, X.; Yang, J. Neuroendocrine abnormalities associated with untreated first episode patients with major depressive disorder and bipolar disorder. Psychoneuroendocrinology 2019, 107, 119–123. [Google Scholar] [CrossRef]
- Shen, Y.; Wu, F.; Zhou, Y.; Ma, Y.; Huang, X.; Ning, Y.; Lang, X.; Luo, X.; Zhang, X. Association of thyroid dysfunction with suicide attempts in first-episode and drug naïve patients with major depressive disorder. J. Affect. Disord. 2019, 259, 180–185. [Google Scholar] [CrossRef]
- Fischer, S.; Strahler, J.; Markert, C.; Skoluda, N.; Doerr, J.M.; Kappert, M.; Nater, U.M. Effects of acute psychosocial stress on the hypothalamic-pituitary-thyroid (HPT) axis in healthy women. Psychoneuroendocrinology 2019, 110, 104438. [Google Scholar] [CrossRef]
- Joseph-Bravo, P.; Jaimes-Hoy, L.; Uribe, R.M.; Charli, J.L. 60 Years of Neuroendocrinology: TRH, the first hypophysiotropic releasing hormone isolated: Control of the pituitary-thyroid axis. J. Endocrinol. 2015, 226, T85–T100. [Google Scholar] [CrossRef] [Green Version]
- Keestra, S.; Högqvist Tabor, V.; Alvergne, A. Reinterpreting patterns of variation in human thyroid function: An evolutionary ecology perspective. Evol. Med. Public Health 2020, 9, 93–112. [Google Scholar] [CrossRef]
- Dietrich, J.W.; Midgley, J.; Hoermann, R. Editorial: “Homeostasis and Allostasis of Thyroid Function”. Front. Endocrinol. 2018, 9, 287. [Google Scholar] [CrossRef] [Green Version]
- Chatzitomaris, A.; Hoermann, R.; Midgley, J.E.; Hering, S.; Urban, A.; Dietrich, B.; Abood, A.; Klein, H.H.; Dietrich, J.W. Thyroid Allostasis-Adaptive Responses of Thyrotropic Feedback Control to Conditions of Strain, Stress, and Developmental Programming. Front. Endocrinol. 2017, 8, 163. [Google Scholar] [CrossRef] [Green Version]
 ; stimulation:
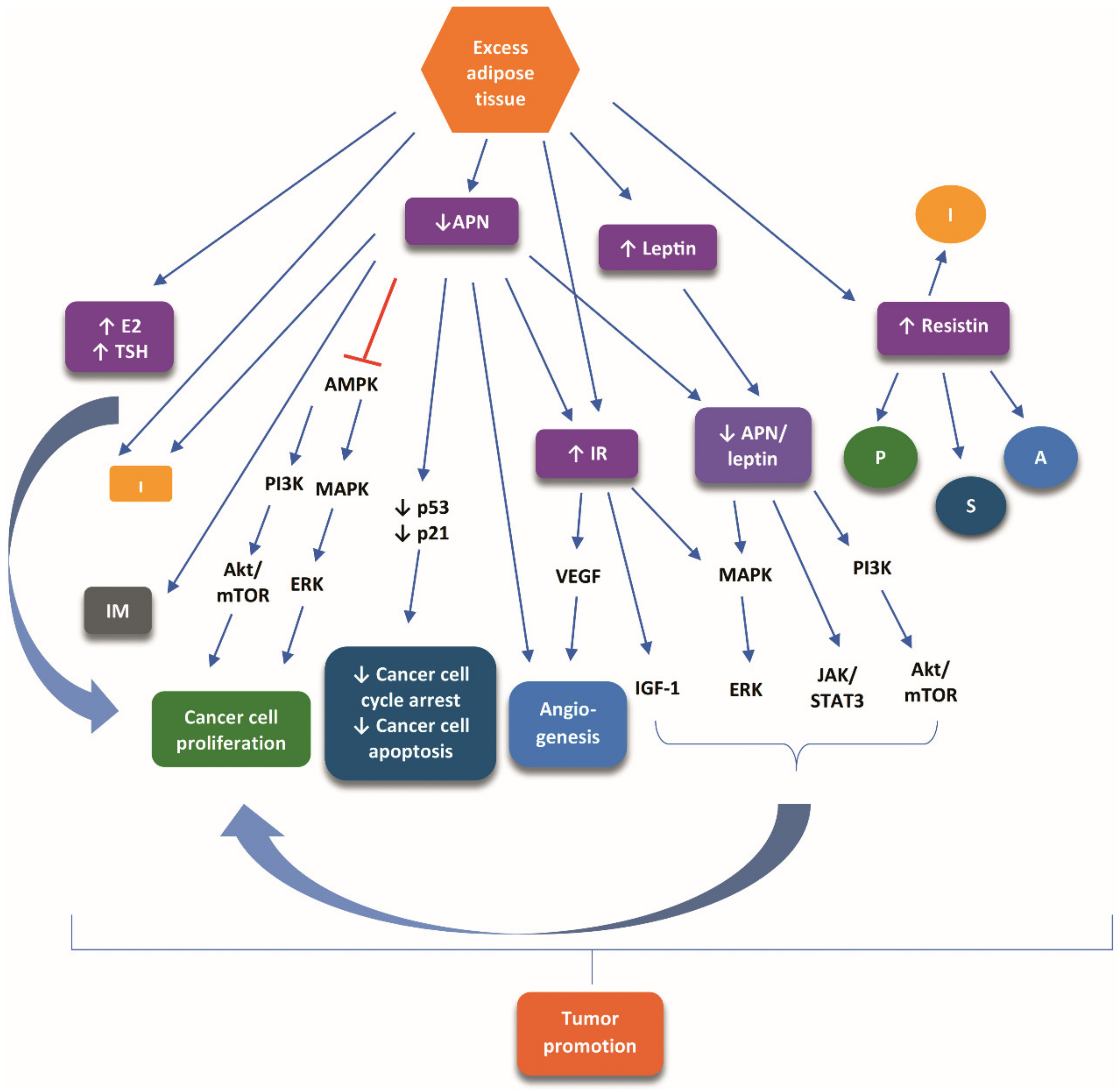
; stimulation:  . Abbreviations: A, angiogenesis; Akt, protein kinase B; AMPK, adenosine monophosphate-activated protein kinase; APN, adiponectin; E2, 17-β-estradiol; ERK, extracellular signal-regulated kinases; I, inflammation; IGF-1, insulin-like growth factor 1; IM, inflammatory-immune responses; IR, insulin resistance; JAK, MAPK; mitogen-activated protein kinase; mTOR, mammalian target of rapamycin; P, proliferation; PI3K, phosphoinositide-3 kinase; S, survival; STAT3, signal transducer and activator of transcription 3; TSH, thyroid-stimulating hormone; VEGF, vascular endothelial growth factor.
; stimulation: . Abbreviations: A, angiogenesis; Akt, protein kinase B; AMPK, adenosine monophosphate-activated protein kinase; APN, adiponectin; E2, 17-β-estradiol; ERK, extracellular signal-regulated kinases; I, inflammation; IGF-1, insulin-like growth factor 1; IM, inflammatory-immune responses; IR, insulin resistance; JAK, MAPK; mitogen-activated protein kinase; mTOR, mammalian target of rapamycin; P, proliferation; PI3K, phosphoinositide-3 kinase; S, survival; STAT3, signal transducer and activator of transcription 3; TSH, thyroid-stimulating hormone; VEGF, vascular endothelial growth factor.
. Abbreviations: A, angiogenesis; Akt, protein kinase B; AMPK, adenosine monophosphate-activated protein kinase; APN, adiponectin; E2, 17-β-estradiol; ERK, extracellular signal-regulated kinases; I, inflammation; IGF-1, insulin-like growth factor 1; IM, inflammatory-immune responses; IR, insulin resistance; JAK, MAPK; mitogen-activated protein kinase; mTOR, mammalian target of rapamycin; P, proliferation; PI3K, phosphoinositide-3 kinase; S, survival; STAT3, signal transducer and activator of transcription 3; TSH, thyroid-stimulating hormone; VEGF, vascular endothelial growth factor.
; stimulation: . Abbreviations: A, angiogenesis; Akt, protein kinase B; AMPK, adenosine monophosphate-activated protein kinase; APN, adiponectin; E2, 17-β-estradiol; ERK, extracellular signal-regulated kinases; I, inflammation; IGF-1, insulin-like growth factor 1; IM, inflammatory-immune responses; IR, insulin resistance; JAK, MAPK; mitogen-activated protein kinase; mTOR, mammalian target of rapamycin; P, proliferation; PI3K, phosphoinositide-3 kinase; S, survival; STAT3, signal transducer and activator of transcription 3; TSH, thyroid-stimulating hormone; VEGF, vascular endothelial growth factor.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Controversy over the Association of Obesity with (D)TC | |
|---|---|
| Data Sustaining the Association of Obesity with (D)TC [Ref]. | Data Sustaining no Association of Obesity with (D)TC [Ref]. |
|
|
| Discordance about the Contribution of Obesity to Unfavorable COVID-19 Outcome in Non-Cancer and Cancer Patients | |
|---|---|
| Obesity is Related to Unfavorable COVID-19 Outcome in Non-Cancer Patients | Obesity is Not Related to Unfavorable COVID-19 Outcome in Cancer Patients |
|
|
| Committee of 67 experts (45 endocrine surgeons and 22 endocrinologists) from multiple countries a [73]. | |
| FNA result | Recommendation |
|
|
|
|
|
|
| Committee of French-speaking Association of Endocrine Surgery (AFCE) [74]. | |
| FNA result | Recommendation |
|
|
|
|
| Committee of Turkish Association of Endocrine Surgery [75]. | |
| FNA result | Recommendation |
|
|
|
|
|
|
|
|
| Committee of Brazilian Society of Endocrinology and Metabolism (SBEM) [76]. | |
| FNA result | Recommendation |
|
|
| Challenges in in the Oncological Strategy for DTC Due to COVID-19 | |
|---|---|
| Challenge I: Appropriate patient selection for FNA | |
| Study type [Ref] | Results |
| Analysis of thyroid FNA trends at Federico II University of Naples before, during and after first lockdown in Italy a. [69] |
|
| International survey of cytopathologic laboratories in 23 countries. [70] |
|
| Analysis of databases of China, South Korea, Iran, and Italy concerning thyroid surgery during 3 COVID-19 pandemic phases b. [71] |
|
| Challenge II: Reschedule of DTC surgery | |
| Study type [Ref] | Results |
| Analysis of databases of China, South Korea, Iran, and Italy concerning thyroid surgery during 3 COVID-19 pandemic phases b. [71] |
|
| Challenge III: Assessment of delays and disruptions in DTC care | |
| Study type [Ref] | Results |
| Systematic review of 62 studies. [77] |
|
| Study on PTC treatment plans of 12 PTC patients. [78] |
|
| Challenge IV: The safety of DTC surgery in the COVID-19 era. | |
| Study type [Ref] | Results |
| Systematic review on thyroid surgery. [80] |
|
| Analysis of databases of China, South Korea, Iran, and Italy concerning thyroid surgery during 3 COVID-19 pandemic phases. [71] |
|
| International, observational cohort study of 1137 consecutive head and neck cancer patients subjected to primary surgery in 26 countries. [81] |
|
| Impact of Cancer in General on COVID-19 Severity | Impact of (D)TC on COVID-19 Severity |
|---|---|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deligiorgi, M.V.; Siasos, G.; Vakkas, L.; Trafalis, D.T. Charting the Unknown Association of COVID-19 with Thyroid Cancer, Focusing on Differentiated Thyroid Cancer: A Call for Caution. Cancers 2021, 13, 5785. https://doi.org/10.3390/cancers13225785
Deligiorgi MV, Siasos G, Vakkas L, Trafalis DT. Charting the Unknown Association of COVID-19 with Thyroid Cancer, Focusing on Differentiated Thyroid Cancer: A Call for Caution. Cancers. 2021; 13(22):5785. https://doi.org/10.3390/cancers13225785
Chicago/Turabian StyleDeligiorgi, Maria V., Gerasimos Siasos, Lampros Vakkas, and Dimitrios T. Trafalis. 2021. "Charting the Unknown Association of COVID-19 with Thyroid Cancer, Focusing on Differentiated Thyroid Cancer: A Call for Caution" Cancers 13, no. 22: 5785. https://doi.org/10.3390/cancers13225785