
HDL in Immune-Inflammatory Responses: Implications beyond Cardiovascular Diseases



1
Department of Pharmacological and Biomolecular Sciences, Università degli Studi di Milano, 20133 Milan, Italy
2
Center for the Study of Atherosclerosis, E. Bassini Hospital, Cinisello Balsamo, 20092 Milan, Italy
3
IRCCS MultiMedica, Sesto S. Giovanni, 20099 Milan, Italy
*
Authors to whom correspondence should be addressed.
Cells 2021, 10(5), 1061; https://doi.org/10.3390/cells10051061
Submission received: 30 March 2021
/
Revised: 27 April 2021
/
Accepted: 27 April 2021
/
Published: 29 April 2021
(This article belongs to the Special Issue High Density Lipoproteins and Atherosclerosis)
Abstract
:High density lipoproteins (HDL) are heterogeneous particles composed by a vast array of proteins and lipids, mostly recognized for their cardiovascular (CV) protective effects. However, evidences from basic to clinical research have contributed to depict a role of HDL in the modulation of immune-inflammatory response thus paving the road to investigate their involvement in other diseases beyond those related to the CV system. HDL-C levels and HDL composition are indeed altered in patients with autoimmune diseases and usually associated to disease severity. At molecular levels, HDL have been shown to modulate the anti-inflammatory potential of endothelial cells and, by controlling the amount of cellular cholesterol, to interfere with the signaling through plasma membrane lipid rafts in immune cells. These findings, coupled to observations acquired from subjects carrying mutations in genes related to HDL system, have helped to elucidate the contribution of HDL beyond cholesterol efflux thus posing HDL-based therapies as a compelling interventional approach to limit the inflammatory burden of immune-inflammatory diseases.
1. Introduction
High-density lipoproteins (HDL) are commonly recognized as the “good carriers” of cholesterol in blood as they participate to cholesterol removal from the periphery (including vessel wall) to the liver for the excretion, in contrast to low-density lipoproteins (LDL), or “bad” cholesterol, that distribute dietary cholesterol from the liver to the periphery. The observation that HDL have been preserved during evolution and are the dominant lipoproteins in species that do not develop atherosclerosis and cardiovascular disease supports their role in modulating immunometabolic responses occurring at the vascular level and beyond [1]. The aim of this review is to provide a timely update on the involvement of HDL in the immune response, to discuss the molecular mechanisms that could explain this function beyond that of cholesterol cargo and to provide a rationale for targeting the HDL system in the setting of immune-inflammatory diseases.
2. HDL in Immune-Inflammatory Diseases: What Are HDL-C Levels Telling Us?
Plasma cholesterol levels are a robust and economic marker to predict cardiovascular risk in the population. Although many observational studies have demonstrated an inverse correlation between HDL-C levels and the risk of coronary heart disease and mortality, this association applies for values up to 80–90 mg/dL [2,3], whereas at higher levels a U-shaped curve is observed, with extremely high HDL-C levels being associated with an increased CVD risk [4]. In parallel, clinical studies with different pharmacological approaches, including niacin, fibrates, and cholesteryl ester transfer protein inhibitors, showed that a massive increase in plasma HDL-C levels does not translate in increased cardiovascular protection.
These findings lead to reconsider HDL-C not only as a CVD risk factor but rather as an indicator of other pathological conditions. Indeed, a U-shaped association has been reported not only for the incidence of CV events, but also for the incidence of infectious and autoimmune diseases [5,6]. On one hand, low HDL-C levels predict the risk of infection and autoimmune diseases, on the other hand, individuals with extremely high HDL-C levels are at increased risk of infectious diseases. Data from the ILLUMINATE trial showed that raising HDL-C with torcetrapib, a cholesteryl ester transfer protein (CETP) inhibitor, resulted in an increased risk of infectious disease-related deaths compared to placebo [7]. These findings highlight the connection between HDL-C levels/function, immune-inflammatory and infectious diseases.
Patients with systemic lupus erythematosus (SLE) and rheumatoid arthritis (RA) are both characterized by an increased CVD risk due to the coexistence of dyslipidaemia and chronic inflammation. SLE patients present a classical “lupus lipoprotein pattern” with increased levels of VLDL and LDL and decreased HDL, a phenotype associated with accelerated atherosclerosis and cardiovascular death [8]. Reduced levels of HDL-C are also a common, despite not unequivocal, sign of other autoimmune diseases, including RA, skin diseases, such as psoriasis [9], and bowel diseases, such as Chron’s disease [10], especially during the active phase of the disease. While these are mainly descriptive studies, where HDL-C concentrations are used as a proxy of HDL levels, emerging approaches are trying to investigate other parameters that could better mark the number of HDL particles, including NMR analysis [11,12] or the measurement of the key structural protein of HDL, namely, apoA-I, whose levels are also decreased in patients with SLE [13].
HDL Composition in Auto-Immune Diseases
It has been widely proven that, in the presence of chronic cardiometabolic diseases or even under an acute pathological condition (such as infection or myocardial infarction), HDL may switch from a protective anti-inflammatory particle to a dysfunctional pro-inflammatory player [8,14,15,16,17,18,19,20,21]. HDL from patients with coronary heart disease exhibit a lower cholesterol efflux capacity (the leading anti-atherosclerotic function of HDL), a reduced endothelial-protective activity, paralleled by the acquisition of pro-atherogenic functions [22]. In type 2 diabetic patients, HDL show several structural alterations that include the enrichment with serum amyloid A (SAA), due to underlying low-grade chronic inflammation, the reduction of apoA-I content, and the increase in oxidized lipids and advanced glycation products [22]. Chronic kidney disease negatively impacts HDL structure and function, with the incorporation of the acute phase protein symmetric dimethylarginine into the HDL particle having a major negative consequence on HDL-mediated reverse cholesterol transport and endothelial protection [22].
A closer look at patients with autoimmune diseases evidence several modifications in the composition and functionality of HDL supporting a switch from an anti-inflammatory to a pro-inflammatory particle (piHDL) (Table 1) [8]. The major alteration is the displacement of apoA-I by SAA, together with the reduction of paraoxonase (PON1) activity; these changes affect the anti-inflammatory and anti-atherogenic properties of HDL [8]. Parallel to these changes in the proteome, substantial modifications of the HDL lipidome have been reported in SLE and RA patients. These include not only lower cholesteryl esters and more triglycerides [23,24], but also a reduced phospholipid content. The latter was reported in psoriatic patients but was also shown in other pathological conditions, including acute myocardial infarction, and is consistent with an elevated activity of secretory phospholipase A2 (sPLA2), as frequently observed under these circumstances [25]. In agreement with this, HDL from RA patients show an increased content of phospholipid species carrying arachidonic acid (C20:4 n-6), paralleled by the reduction of phospholipid species carrying omega-3 fatty acids (and more specifically docosahexaenoic acid, C22:6 n-3) [26]. Changes in the lipidome impacts also HDL function; indeed, cholesterol efflux capacity (CEC) [27,28] is reduced in SLE and RA patients [29] and is partially restored by treatment with tocilizumab, an interleukin-6 receptor inhibitor [30]. These findings further strengthen the relationship between systemic to cellular cholesterol handling and immune-inflammatory response [30].
3. The Role of HDL on Immune Cell Function
HDL possess several anti-atherogenic properties, ranging from anti-oxidant to the control of vascular tone, that are protective in the context of cardiovascular diseases [83,84]; however, the most important activity, which is also associated to several immune-modulatory effects, is represented by the ability of HDL to remove free cholesterol from cell membrane [85,86]. This pathway, that is either mediated by the interaction with specific cholesterol transporters, named ATP-binding cassette transporters ABCA1 and ABCG1, or can be transporter-independent, has been shown to shape the function of immune cells [87].
3.1. Anti-Oxidative, Anti-Inflammatory, and Vascular-Protective Effects of HDL
HDL are a cargo of proteins, enzymes, and molecules (from hormones to vitamins) that are not directly related to the maintenance of cholesterol homeostasis. Paraoxonase enzymes (PON1-3), for instance, confer anti-oxidative functions to HDL [88]. PiHDL from SLE patients show a reduction in the content of paraoxonase, resulting in increased oxidation of HDL and of their main apoprotein, apoA-I [89]. In addition, PON1 is also involved in the regulation of vascular tone by promoting endothelial nitric oxide synthase (eNOS) activation [90]; together with the inhibition of endothelial expression of adhesion molecules, reduction of apoptosis and the promotion of endothelial cell repair by hematopoietic precursors [91], PON1 contributes to the vaso-protective activity of HDL. On the contrary, oxidation of HDL could directly have pro-inflammatory effects on monocytes by promoting the upregulation of platelet-derived growth factor receptor β (PDGFRβ), increasing their chemotaxis and TNF-α release [45], but also enriching HDL with the pro-inflammatory SAA [45], as observed in SLE patients. Indeed, HDL from SLE patients failed to promote the synthesis and translocation of the nuclear factor ATF3, resulting in NF-κB activation and inflammatory cytokine production in macrophages [46]; this effect is mediated by the ability of oxidized HDL to bind lectin-like oxidized LDL receptor 1 (LOX1). It is worth to note, lipoprotein oxidation, included that of HDL, derives also from hyperactivated neutrophils of autoimmune patients: the release of active oxidative enzymes (including MPO, nitric oxide synthase and NOX) from their extracellular traps (NETs) results in the modification of HDL, that lose their anti-inflammatory and vasoprotective effects, as well as the ability to mediate reverse cholesterol transport [41]. Several other alterations in HDL function were associated with their oxidation [88,92,93,94].
Finally, other anti-inflammatory properties of HDL are associated to their ability to bind and neutralize the Gram-negative bacterial LPS [95] and Gram-positive bacterial lipoteichoic acid (LTA) [96], thus preventing generalized inflammatory responses. While LTA binds directly to HDL, LPS interacts with LPS-binding protein (LBP), an acute phase protein that shares similarities with CETP [97] and promotes LPS transfer from cell membranes to HDL, leading to LPS neutralization, probably via increased liver catabolism/elimination [98,99]. HDL participate to inflammatory response also by promoting the production of the acute phase protein PTX3 by endothelial cells [100]; PTX3, in turn, plays a double-edged sword role not only in infections [101], but also in atherosclerosis [102], thrombosis [103,104], and obesity [105]. Together these observations highlight the role of HDL at the crossroads between the maintenance of metabolic homeostasis and the immune-inflammatory response [106,107].
3.2. HDL, Lipid Rafts, and Immunomodulatory Function
Physiologically, a large percentage of cellular free cholesterol is localized in the plasma membrane, where it is distributed in a heterogeneous manner and enriched in the so-called lipid raft domains, which constitute ~30–40% of the mammalian cell membranes. These structures are highly dynamic, finely regulated, and essential for cellular functions, as they serve as a platform where proteins involved in signal transduction are transiently assembled or spatially organized to promote kinetically favorable interactions and generate an appropriate response to a stimulus. Indeed, many enzymes and proteins involved in the signal transduction system are active exclusively when clustered within lipid rafts. In the context of immune cell function, rafts organize signaling by many receptors and accessory proteins, including toll like receptors (TLRs), T and B cell receptors (TCR and BCR), and major histocompatibility (MHC) class II [86].
Cellular responses regulated by lipid rafts range from physiological to pathological; when cholesterol influx is high and exceeds the efflux capacity, the accumulation of cholesterol in membranes is believed to lead to cell activation and inflammation [108]. The abundance and functional properties of lipid rafts change very quickly in response to a stimulus, and thus cholesterol homeostasis is essential to ensure an optimal composition of lipid rafts and preserve the normal cell functions. Alterations in cholesterol trafficking at plasma membrane may modulate immune cell functions, including the recruitment and proliferation of monocytes, the expression of inflammatory cytokines in macrophages, and the activation and proliferation of lymphocytes [108,109].
3.3. HDL, Lipid Rafts in Innate Immune Cells
Macrophages derive from circulating monocytes, which are in turn generated following differentiation from hematopoietic stem and multipotential progenitor cells (HSPCs) in the bone marrow and other medullary organs [110]. Cholesterol metabolism plays a central role in hematopoietic precursors; in fact, these monocytes may bear a pre-programed ability to become M1-like macrophages (pro-inflammatory cells) once they enter the atherosclerotic lesion. On the other hand, removal of cholesterol from cells via HDL can regulate the production of innate immune cells, by acting on HSPCs proliferation [111]. Moreover, clinical conditions associated with very low levels of HDL-C reflect into changes in the balance of circulating monocytes subsets [112].
Cholesterol trafficking at plasma membrane and innate immunity signaling are closely linked; in fact, the cholesterol content of membrane rafts regulates cellular signaling by determining the selective localization of TLRs, involved in macrophage activation. TLR4 senses LPS and clusters within lipid rafts with CD14 to promote monocyte activation (Figure 1A) [113]. ABC transporter-deficient macrophages present with a free cholesterol accumulation in membranes that associates with an enhanced expression of inflammatory and chemokine genes in response to LPS, due to an increased cell surface expression of TLR4; this response is dampened following cholesterol depletion [114].
HDL exert an anti-inflammatory effect in macrophages even beyond their effect on cellular cholesterol levels. Indeed, HDL induce the expression and activation of activating transcription factor 3 (ATF3), a transcriptional modulator that provides negative feedback on TLR signaling (Figure 1A) [115]. In murine bone marrow-derived macrophages (BMDM), human peripheral blood mononuclear cells (PBMC), and in an in vivo model of acute inflammation (TLR ligand-treated mice), pretreatment with native HDL or reconstituted HDL (apoA-I and phospholipids) inhibited TLR-induced production of pro-inflammatory cytokines from macrophages [115]. This inhibitory effect was not due to the interaction of HDL with TLR ligands (contrarily to what observed for LPS, which is sequestered by HDL), and did not involve neither the modulation of TLR signaling events, nor the disruption of cytokine secretory processes, but instead was dependent on HDL-mediated induction of ATF3, which in turn suppressed the ability of TLRs to induce the expression of pro-inflammatory cytokines at a transcriptional level [115].
The modulation of lipid raft abundance and composition by HDL impacts cholesterol homeostasis also in HSPCs, and thus regulates the commitment to monocytes/macrophages and influences their function. Disruption of cholesterol homeostasis or prolonged exposure to hypercholesterolaemia increases the commitment of HSPCs to monocytes, resulting in monocytosis [111,116]. Similarly, loss of ABCA1, ABCG1, or apoE expression has been shown to foster hematopoietic cell proliferation by increasing cholesterol within lipid rafts, thus enhancing immune cell responsiveness. Similarly, the deficiency in the bone marrow of ABCG4 (another transporter involved in cholesterol efflux) increased cell surface expression of thrombopoietin (TPO) receptor (c-MPL) and enhanced megakaryocyte proliferation [117]; although these pathways have been connected with an increased risk of atherosclerosis, due to monocytosis, neutrophilia, and thrombocytosis, they also contribute to autoimmune diseases. This is supported by the evidence that the expansion of bone marrow cells observed in experimental models of RA correlates with a decreased expression of apoE, ABCA1, and ABCG1 in hematopoietic cells, that couples with an increased expression of key myeloid promoting growth factor receptors; this suggests that the systemic inflammation associated with the disease may, in turn, cause defective cellular cholesterol metabolism [118].
Although many potentially beneficial effects of HDL on inflammation have been reported, some studies suggested also a role in supporting the activation of the immune response: as an example, HDL-mediated passive cholesterol depletion (i.e., independent on cholesterol transporters) and lipid raft disruption result in the activation of multiple protein kinase C isoforms, which favor the production of pro-inflammatory cytokines (TNF-α and IL-12) and the reduction of IL-10 [119]. In this context, also apoA-I was shown to utilize MyD88, a TLR adaptor, to control reverse cholesterol transport [120] and induce pro-inflammatory cytokine expression (MCP-1, TNF-α, IL-6, IL-1β) [120]. This finding was confirmed in vivo following the injection of apoA-I, which elicited the MyD88- and TLR4-dependent neutrophil recruitment at the injection site [120]. Thus, HDL/apoA-I may exert anti- or pro-inflammatory effects, depending on the adaptations occurring in cell cholesterol content; in LPS-stimulated macrophages, the anti-inflammatory effect of HDL is observed in the early phases and reflects reduced TLR4 levels and signaling, whereas they become pro-inflammatory molecules under extensive cholesterol depletion conditions, reflecting a reduced interferon receptor signaling [121].
3.4. HDL, Cholesterol, and Lymphocyte Activation and Proliferation
Lymphocyte activation results from the presentation of an antigen bound to MHC-II molecules by antigen-presenting cells (APCs) [122]. APCs include macrophages and dendritic cells (DCs). The impairment of cholesterol efflux in DCs lacking ABCA1/G1 leads to cholesterol accumulation, inflammasome activation, and increased production of additional cytokines which result in enhanced T cell activation [123]. HDL and apoA-I can modulate the ability of APCs to activate T cells by cholesterol depletion from lipid rafts [124]. Furthermore, HDL suppress the activation, maturation, and cytokine secretion by DCs, which associate to a reduced expression of MHC-II and co-stimulatory molecules that are required for an efficient T cell activation [125,126]. In stimulated APCs, HDL downregulate the inflammatory response by interfering with the MyD88-dependent TLR4 signaling pathway, an effect that was mediated by ABCA1 and SR-BI, whereas ABCG1 did not appear to play a major role [126]. Similar to macrophages, also in DCs ATF3 expression was increased after exposure to HDL [126]. In addition, by inhibiting the oxidation of LDL, HDL may play an indirect role in regulating DC function; indeed, oxidized LDL were shown to promote the development of mature DCs [127,128]. Accordingly, changes in HDL function/levels typically reported in autoimmune disease (Table 1) may, at least in part, contribute to the alteration of DC functions observed in these pathological conditions [129].
Not only MHC-II, but also B-cell receptor (BCR) and T-cell receptor (TCR) are localized in lipids rafts rich areas. In T cells, cholesterol plasma membrane mediates TCR clustering, inhibits spontaneous TCR activation, and reduces TCR mobility when the conditions for activation are not appropriate (Figure 1B). Interestingly, distinct plasma membrane lipid profiles are associated with specific T helper subsets (Th1, Th2, or Th17), suggesting that lipid composition of cell membrane contributes to define functional T cell phenotypes [130].
Cholesterol is known to stabilize raft membrane domains and binds to the TCRβ-chain to facilitate TCR dimerization, thus increasing its avidity towards antigens. Hypercholesterolaemia enhances TCR stimulation and facilitates proliferative T cell response. These changes are associated also with alterations in regulatory T (Treg) cell development [131]. In resting T-cells, TCR and CD3 are localized in non-raft domains; following cholesterol enrichment within lipid rafts, TCR and related signaling proteins converge in these domains, an event which facilitates the formation of immunological synapses and the activation of downstream pathways [132]. Lipid raft integrity is thus crucial for T cell activation; the hyperactivity and hypersensitivity of T cells observed in autoimmune diseases, such as systemic lupus erythematosus, are associated with membrane cholesterol enrichment in lipid rafts and facilitate TCR-dependent signaling [133].
In an experimental model, the administration of exogenous apoA-I or recombinant HDL attenuates arthritis in an ABCA1-dependent manner [134]. This activity appears to be associated with a HDL-mediated modulation of maturation and function of dendritic cells, which suppresses T cell proliferation in vitro [126]. In an experimental model of dyslipidaemia-induced dermatitis, the ectopic macrophage apoA-I expression reduced cholesterol accumulation and CD4+ T cell levels in aortic lesions, skin, and skin-draining lymph nodes (LNs) without affecting HDL-C levels or tissue macrophage levels [135].
Tregs are a subset of CD4 T cells involved in immune homeostasis through the inhibition of the immune response in several cell types, including macrophages, APCs, and T cells, and have been shown to be atheroprotective. Still, in the context of atherosclerosis, Treg levels increase [136,137]. Hypercholesterolaemia, indeed, promotes TCR stimulation in CD4+ T cells and facilitates proliferative T cell response, and these effects are associated with a higher Treg population development in the thymus of mice fed with cholesterol-containing diet [131].
In mice with T cell-specific deficiency of ABCG1, an increased differentiation of naïve CD4 T cells into Tregs has been reported, protecting mice against atherosclerosis [138]; on the other hand, in Ldlr−/−ApoAI−/− mice, which exhibit an autoimmune phenotype (with large spleens and peripheral lymph nodes enriched in cholesterol, expanded populations of T cells, B cells, DCs, and macrophages, and increase in T cell proliferation and activation), apoA-I infusion decreased the numbers of immune cells in LNs, increased the number of Tregs, and reduced lipid accumulation in LNs and skin [139]. Accordingly, apoA-I injection in apoE−/− mice reduces intracellular cholesterol levels in Tregs and prevents their conversion into pro-atherogenic T follicular helper cells [140]. Tregs have also an elevated capacity to bind and internalize HDL, likely due to the high expression of SR-BI compared with other CD4 cell subsets [141]. The internalization of HDL increases the survival of Tregs through several mechanisms [141].
Altogether, these observations suggest that an optimal level of plasma membrane cholesterol is crucial for Treg development and/or function, and that variations in cholesterol levels may alter Treg homeostasis.
4. Genetics as a Proxy to Study the Impact of HDL Cholesterol and Functions in Inflammation and Immune Disorders
A powerful tool to appreciate the role of HDL comes from studies on monogenic disorders resulting in extremely low or high HDL-C levels. Monogenic disorders associated with low HDL-C levels include those related to loss-of-function mutations in APOA1, the gene encoding apoA-I, LCAT, encoding lecithin-cholesterol acyl transferase (LCAT), and ABCA1, encoding ABCA1. Genes implicated in monogenic disorders associated with high HDL-C levels include CETP, encoding cholesteryl ester transfer protein (CETP), SCARB1, encoding scavenger receptor class B member 1 (SRB1), and LIPC, encoding hepatic triacylglycerol lipase [142]. Patients with Tangier disease, despite having very low HDL-C levels due to ABCA1 deficiency, do not manifest premature coronary artery disease, but rather present an increased inflammatory status [143]; this has been associated to an increased inflammasome activation triggered by reduced cholesterol efflux from myeloid cells [144]. Moreover, mendelian randomization studies failed to demonstrate a causal link between HDL-C and CVD risk [145], but rather indicate that low HDL-C levels increase the risk of infections [6]. In addition, elevated peripheral blood leukocyte counts were reported in subjects with low HDL-C levels of any origin [146]. In line with this observation, subjects carrying a low HDL-C polygenic score have been shown to present an increased risk of hospitalization for infections [147]; this is consistent with the increased mortality for sepsis reported in subjects with gain-of-function mutation on CETP, who present a dramatic reduction of HDL-C levels during infection [148]. It is tempting to speculate that CETP, beyond transferring cholesteryl esters from HDL to apolipoprotein (apo) B-containing triglyceride-rich lipoproteins (TRLs), could also participate to immune response following a bacterial insult. This hypothesis is supported by the evidence that CETP is predominantly produced by Kupffer cells, specialized liver macrophages, and that its expression is reduced during inflammation; in turn, this leads to an increase in HDL-C levels that may contribute to LPS clearance during infections [149]. Similarly, LCAT deficiency in mice was associated with the presence of immature discoidal HDL and a reduced LPS-neutralizing capacity [150], thus suggesting that not only the concentration but also the type of HDL subclasses differently modulates immune responses [151].
5. Conclusions
HDL are complex particles constituted by different proteins and lipids, also acting as cargo of other molecules, such as hormones and vitamins. The aspects highlighting a role for HDL in immune-inflammatory diseases support the investigation of HDL-based therapies in the context of these diseases. However, clinical trials and genetic studies have demonstrated that raising HDL-C levels would not have beneficial effects, thus directing pharmacology toward the identification of therapeutic approaches able to mirror HDL protective functions. Recombinant HDL and HDL mimetics have shown favorable effects in increasing cholesterol efflux [152,153], improving endothelial functions [154], and reducing inflammation [155], that might prove to be beneficial beyond atherosclerosis [156,157,158]. Parallel to increasing small, discoidal HDL, which possess the highest cholesterol efflux potential [159], interfering with HDL maturation might be beneficial in the context of inflammatory diseases. This is the case of CETP inhibitors that, despite the failure in preventing cardiovascular events, have been shown to increase the survival rate in humanized models of sepsis [160], or recombinant human LCAT, that, by reducing HDL-bound SAA and increasing HDL-bound apoA-I as well as HDL functionality [161], could exert protective effect also against SARS-Cov2 infections [162]. Indeed, increased COVID-19 disease severity and worse prognosis was reported in patients with low HDL-C levels [163,164,165]; in addition, major changes in HDL proteome and decreased functionality have been described in severe COVID-19 patients [166].
Therefore, the identification of the molecular mechanisms that lead to HDL dysfunction in immune-inflammatory diseases would offer the opportunity to design intervention approaches aimed at restoring HDL functionality, representing a complementary approach to current anti-inflammatory treatments.
Author Contributions
F.B., A.P., A.L.C., and G.D.N. made substantial contribution to the concept, writing, editing, and revision of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. The work of the authors is supported by Fondazione Cariplo 2016-0852 (GDN) and 2019-1560 (FB); Telethon Foundation (GGP19146) (GDN); European Foundation for the Study of Diabetes (EFSD)/Lilly European Diabetes Research Programme (GDN); Ministero dell’Università, Progetti di Rilevante Interesse Nazionale (PRIN 2017 K55HLC) (GDN), (PRIN 2017 H5F943) (ALC), Ministero della Salute, Ricerca Finalizzata RF-2019-12370896 (ALC, GDN); “Post-Doctoral Fellowship 2021” by “Fondazione Umberto Veronesi” (FB).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
F.B. and A.P. do not report conflicts of interest; G.D.N. reports research grants from Amgen, Novartis, and Pfizer, outside the submitted work; A.L.C. reports grants from Amgen, Sanofi, Regeneron personal fees from Merck, Sanofi, Regeneron, AstraZeneca, Amgen, Novartis, outside the submitted work.
References
- Bonacina, F.; Da Dalt, L.; Catapano, A.L.; Norata, G. Metabolic adaptations of cells at the vascular-immune interface during atherosclerosis. Mol. Asp. Med. 2020, 100918. [Google Scholar]
- Wilson, P.W.; Abbott, R.D.; Castelli, W.P. High density lipoprotein cholesterol and mortality. The Framingham Heart Study. Arteriosclerosis 1988, 8, 737–741. [Google Scholar] [CrossRef] [Green Version]
- Emerging Risk Factors Collaboration; Di Angelantonio, E.; Sarwar, N.; Perry, P.; Kaptoge, S.; Ray, K.K.; Thompson, A.; Wood, A.M.; Lewington, S.; Sattar, N.; et al. Major lipids, apolipoproteins, and risk of vascular disease. JAMA 2009, 302, 1993–2000. [Google Scholar] [CrossRef] [Green Version]
- Madsen, C.M.; Varbo, A.; Nordestgaard, B.G. Extreme high high-density lipoprotein cholesterol is paradoxically associated with high mortality in men and women: Two prospective cohort studies. Eur. Heart J. 2017, 38, 2478–2486. [Google Scholar] [CrossRef] [Green Version]
- Madsen, C.M.; Varbo, A.; Nordestgaard, B.G. Low HDL Cholesterol and High Risk of Autoimmune Disease: Two Population-Based Cohort Studies Including 117341 Individuals. Clin. Chem. 2019, 65, 644–652. [Google Scholar] [CrossRef]
- Madsen, C.M.; Varbo, A.; Tybjaerg-Hansen, A.; Frikke-Schmidt, R.; Nordestgaard, B.G. U-shaped relationship of HDL and risk of infectious disease: Two prospective population-based cohort studies. Eur. Heart J. 2018, 39, 1181–1190. [Google Scholar] [CrossRef] [PubMed]
- Barter, P.J.; Caulfield, M.; Eriksson, M.; Grundy, S.M.; Kastelein, J.J.P.; Komajda, M.; Lopez-Sendon, J.; Mosca, L.; Tardif, J.-C.; Waters, D.D.; et al. Effects of torcetrapib in patients at high risk for coronary events. N. Engl. J. Med. 2007, 357, 2109–2122. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.Y.; Yu, M.; Morin, E.E.; Kang, J.; Kaplan, M.J.; Schwendeman, A. High-Density Lipoprotein in Lupus: Disease Biomarkers and Potential Therapeutic Strategy. Arthritis Rheumatol. 2020, 72, 20–30. [Google Scholar] [CrossRef]
- Trakaki, A.; Marsche, G. High-Density Lipoprotein (HDL) in Allergy and Skin Diseases: Focus on Immunomodulating Functions. Biomedicines 2020, 8, 558. [Google Scholar] [CrossRef]
- Romanato, G.; Scarpa, M.; Angriman, I.; Faggian, D.; Ruffolo, C.; Marin, R.; Zambon, S.; Basato, S.; Zanoni, S.; Filosa, T.; et al. Plasma lipids and inflammation in active inflammatory bowel diseases. Aliment. Pharmacol. Ther. 2009, 29, 298–307. [Google Scholar] [CrossRef] [PubMed]
- Matyus, S.P.; Braun, P.J.; Wolak-Dinsmore, J.; Saenger, A.K.; Shalaurova, I.; Warner, S.M.; Fischer, T.J.; Connelly, M.A. HDL particle number measured on the Vantera(R), the first clinical NMR analyzer. Clin. Biochem. 2015, 48, 148–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, C.P.; Oeser, A.; Raggi, P.; Sokka, T.; Pincus, T.; Solus, J.F.; Linton, M.F.; Fazio, S.; Stein, C.M. Lipoprotein subclasses determined by nuclear magnetic resonance spectroscopy and coronary atherosclerosis in patients with rheumatoid arthritis. J. Rheumatol. 2010, 37, 1633–1638. [Google Scholar] [CrossRef] [Green Version]
- Lilleby, V.; Haugen, M.; Mørkrid, L.; Frøslie, F.K.; Holven, K.B.; Førre, Ø. Body composition, lipid and lipoprotein levels in childhood-onset systemic lupus erythematosus. Scand. J. Rheumatol. 2007, 36, 40–47. [Google Scholar] [CrossRef]
- O’Neill, F.; Riwanto, M.; Charakida, M.; Colin, S.; Manz, J.; McLoughlin, E.; Khan, T.; Klein, N.; Kay, C.W.; Patel, K.; et al. Structural and functional changes in HDL with low grade and chronic inflammation. Int. J. Cardiol. 2015, 188, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Shroff, R.; Speer, T.; Colin, S.; Charakida, M.; Zewinger, S.; Staels, B.; Chinetti-Gbaguidi, G.; Hettrich, I.; Rohrer, L.; O’Neill, F.; et al. HDL in children with CKD promotes endothelial dysfunction and an abnormal vascular phenotype. J. Am. Soc. Nephrol. 2014, 25, 2658–2668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiesa, S.T.; Charakida, M.; McLoughlin, E.; Nguyen, H.C.; Georgiopoulos, G.; Motran, L.; Elia, Y.; Marcovecchio, M.L.; Dunger, D.B.; Dalton, R.N.; et al. Elevated high-density lipoprotein in adolescents with Type 1 diabetes is associated with endothelial dysfunction in the presence of systemic inflammation. Eur. Heart J. 2019, 40, 3559–3566. [Google Scholar] [CrossRef] [Green Version]
- Rysz, J.; Gluba-Brzózka, A.; Rysz-Górzyńska, M.; Franczyk, B. The Role and Function of HDL in Patients with Chronic Kidney Disease and the Risk of Cardiovascular. Dis. Int. J. Mol. Sci. 2020, 21, 601. [Google Scholar] [CrossRef] [Green Version]
- Rosenson, R.S.; Jr, H.B.B.; Ansell, B.J.; Barter, P.J.; Chapman, M.J.; Heinecke, J.W.; Kontush, A.; Tall, A.R.; Webb, N.R. Dysfunctional HDL and atherosclerotic cardiovascular disease, Nature reviews. Cardiology 2016, 13, 48–60. [Google Scholar]
- Srivastava, R.A.K. Dysfunctional HDL in diabetes mellitus and its role in the pathogenesis of cardiovascular disease. Mol. Cell. Biochem. 2018, 440, 167–187. [Google Scholar] [CrossRef]
- Pirillo, A.; Catapano, A.L.; Norata, G.D. HDL in infectious diseases and sepsis. Handb. Exp. Pharmacol. 2015, 224, 483–508. [Google Scholar] [PubMed] [Green Version]
- Tietge, U.J.F. The impact of myeloperoxidase on HDL function in myocardial infarction. Curr. Opin. Endocrinol. Diabetes Obes. 2018, 25, 137–142. [Google Scholar] [CrossRef]
- Chiesa, S.T.; Charakida, M. High-Density Lipoprotein Function and Dysfunction in Health and Disease. Cardiovasc. Drugs 2019, 33, 207–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMahon, M.; Grossman, J.; Fitzgerald, J.; Dahlin-Lee, E.; Wallace, D.J.; Thong, B.Y.; Badsha, H.; Kalunian, K.; Charles, C.; Navab, M.; et al. Proinflammatory high-density lipoprotein as a biomarker for atherosclerosis in patients with systemic lupus erythematosus and rheumatoid arthritis. Arthritis Rheum. 2006, 54, 2541–2549. [Google Scholar] [CrossRef]
- Holzer, M.; Wolf, P.; Curcic, S.; Birner-Gruenberger, R.; Weger, W.; Inzinger, M.; El-Gamal, D.; Wadsack, C.; Heinemann, A.; Marsche, G. Psoriasis alters HDL composition and cholesterol efflux capacity. J. Lipid Res. 2012, 53, 1618–1624. [Google Scholar] [CrossRef] [Green Version]
- Kontush, A.; Lhomme, M.; Chapman, M.J. Unraveling the complexities of the HDL lipidome. J. Lipid Res. 2013, 54, 2950–2963. [Google Scholar] [CrossRef] [Green Version]
- Giraud, C.; Tournadre, A.; Pereira, B.; Dutheil, F.; Soubrier, M.; Lhomme, M.; Kontush, A.; Sébédio, J.-L.; Capel, F. Alterations of HDL particle phospholipid composition and role of inflammation in rheumatoid arthritis. J. Physiol. Biochem. 2019, 75, 453–462. [Google Scholar] [CrossRef]
- Jury, E.C.; Kabouridis, P.S.; Flores-Borja, F.; Mageed, R.A.; Isenberg, D.A. Altered lipid raft-associated signaling and ganglioside expression in T lymphocytes from patients with systemic lupus erythematosus. J. Clin. Investig. 2004, 113, 1176–1187. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, S.; Nambiar, M.P.; Warke, V.G.; Fisher, C.U.; Mitchell, J.; Delaney, N.; Tsokos, G.C. Alterations in lipid raft composition and dynamics contribute to abnormal T cell responses in systemic lupus erythematosus. J. Immunol. 2004, 172, 7821–7831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montecucco, F.; Favari, E.; Norata, G.D.; Ronda, N.; Nofer, J.R.; Vuilleumier, N. Impact of systemic inflammation and autoimmune diseases on apoA-I and HDL plasma levels and functions. Handb. Exp. Pharm. 2015, 224, 455–482. [Google Scholar]
- Greco, D.; Gualtierotti, R.; Agosti, P.; Adorni, M.P.; Ingegnoli, F.; Rota, M.; Bernini, F.; Meroni, P.L.; Ronda, N. Anti-atherogenic Modification of Serum Lipoprotein Function in Patients with Rheumatoid Arthritis after Tocilizumab Treatment, a Pilot Study. J. Clin. Med. 2020, 9, 2157. [Google Scholar] [CrossRef] [PubMed]
- De Carvalho, J.F.; Bonfa, E.; Borba, E.F. Systemic lupus erythematosus and lupus dyslipoproteinemia. Autoimmun. Rev. 2008, 7, 246–250. [Google Scholar] [CrossRef]
- Hahn, B.H.; Grossman, J.; Ansell, B.J.; Skaggs, B.J.; McMahon, M. Altered lipoprotein metabolism in chronic inflammatory states: Proinflammatory high-density lipoprotein and accelerated atherosclerosis in systemic lupus erythematosus and rheumatoid arthritis. Arthritis Res. Ther. 2008, 10, 213. [Google Scholar] [CrossRef] [Green Version]
- Toloza, S.M.A.; Uribe, A.G.; McGwin, G.; Alarcón, G.S.; Fessler, B.J.; Bastian, H.M.; Vilá, L.M.; Wu, R.; Shoenfeld, Y.; Roseman, J.M.; et al. Systemic lupus erythematosus in a multiethnic US cohort (LUMINA). XXIII. Baseline predictors of vascular events. Arthritis Rheum. 2004, 50, 3947–3957. [Google Scholar]
- Gamal, S.M.; Fawzy, S.M.; Abdo, M.; Elgengehy, F.T.; Ghoniem, S.; Alkemry, A. Immunological profile and dyslipidemia in Egyptian Systemic Lupus Erythematosus patients. Egypt. Rheumatol. 2017, 39, 89–92. [Google Scholar] [CrossRef] [Green Version]
- Yuan, J.; Li, L.; Wang, Z.; Song, W.; Zhang, Z. Dyslipidemia in patients with systemic lupus erythematosus: Association with disease activity and B-type natriuretic peptide levels. Biomed. Rep. 2016, 4, 68–72. [Google Scholar] [CrossRef] [Green Version]
- Kiss, E.; Seres, I.; Tarr, T.; Kocsis, Z.; Szegedi, G.; Paragh, G. Reduced paraoxonase1 activity is a risk for atherosclerosis in patients with systemic lupus erythematosus. Ann. N. Y. Acad. Sci. 2007, 1108, 83–91. [Google Scholar] [CrossRef]
- Gaál, K.; Tarr, T.; Lőrincz, H.; Borbás, V.; Seres, I.; Harangi, M.; Fülöp, P.; Paragh, G. High-density lipopoprotein antioxidant capacity, subpopulation distribution and paraoxonase-1 activity in patients with systemic lupus erythematosus. Lipids Health Dis. 2016, 15, 60. [Google Scholar] [CrossRef] [Green Version]
- McMahon, M.; Skaggs, B.J.; Sahakian, L.; Grossman, J.; Fitzgerald, J.; Ragavendra, N.; Charles-Schoeman, C.; Chernishof, M.; Gorn, A.; Witztum, J.L.; et al. High plasma leptin levels confer increased risk of atherosclerosis in women with systemic lupus erythematosus, and are associated with inflammatory oxidised lipids. Ann. Rheum. Dis. 2011, 70, 1619–1624. [Google Scholar] [CrossRef] [PubMed]
- G., H.B.; Rao, V.S.; Kakkar, V.V. Friend Turns Foe: Transformation of Anti-Inflammatory HDL to Proinflammatory HDL during Acute-Phase Response. Cholesterol 2011, 2011, 274629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Lenten, B.J.; Wagner, A.C.; Nayak, D.P.; Hama, S.; Navab, M.; Fogelman, A.M. High-density lipoprotein loses its anti-inflammatory properties during acute influenza a infection. Circulation 2001, 103, 2283–2288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, C.K.; Vivekanandan-Giri, A.; Tang, C.; Knight, J.S.; Mathew, A.; Padilla, R.L.; Gillespie, B.W.; Carmona-Rivera, C.; Liu, X.; Subramanian, V.; et al. Neutrophil extracellular trap-derived enzymes oxidize high-density lipoprotein: An additional proatherogenic mechanism in systemic lupus erythematosus. Arthritis Rheumatol. 2014, 66, 2532–2544. [Google Scholar] [CrossRef] [Green Version]
- Chung, C.P.; Oeser, A.; Raggi, P.; Solus, J.F.; Avalos, I.; Linton, M.F.; Fazio, S.; Stein, C.M. Lipoprotein subclasses and particle size determined by nuclear magnetic resonance spectroscopy in systemic lupus erythematosus. Clin. Rheumatol. 2008, 27, 1227–1233. [Google Scholar] [CrossRef] [PubMed]
- Hua, X.; Su, J.; Svenungsson, E.; Hurt-Camejo, E.; Jensen-Urstad, K.; Angelin, B.; Båvenholm, P.; Frostegård, J. Dyslipidaemia and lipoprotein pattern in systemic lupus erythematosus (SLE) and SLE-related cardiovascular disease. Scand. J. Rheumatol. 2009, 38, 184–189. [Google Scholar] [CrossRef]
- Juárez-Rojas, J.; Medina-Urrutia, A.; Posadas-Sánchez, R.; Jorge-Galarza, E.; Mendoza-Pérez, E.; Caracas-Portilla, N.; Cardoso-Saldaña, G.; Muñoz-Gallegos, G.; Posadas-Romero, C. High-density lipoproteins are abnormal in young women with uncomplicated systemic lupus erythematosus. Lupus 2008, 17, 981–987. [Google Scholar] [CrossRef]
- Skaggs, B.J.; Hahn, B.H.; Sahakian, L.; Grossman, J.; McMahon, M. Dysfunctional, pro-inflammatory HDL directly upregulates monocyte PDGFRbeta, chemotaxis and TNFalpha production. Clin. Immunol. 2010, 137, 147–156. [Google Scholar] [CrossRef] [Green Version]
- Smith, C.K.; Seto, N.L.; Vivekanandan-Giri, A.; Yuan, W.; Playford, M.P.; Manna, Z.; Hasni, S.A.; Kuai, R.; Mehta, N.N.; Schwendeman, A.; et al. Lupus high-density lipoprotein induces proinflammatory responses in macrophages by binding lectin-like oxidised low-density lipoprotein receptor 1 and failing to promote activating transcription factor 3 activity. Ann. Rheum. Dis. 2017, 76, 602–611. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-R.; Lee, E.-Y.; Park, J.K.; Song, Y.W.; Cho, K.-H. Patients with Rheumatoid Arthritis Show Altered Lipoprotein Profiles with Dysfunctional High-Density Lipoproteins that Can Exacerbate Inflammatory and Atherogenic Process. PLoS ONE 2016, 11, e0164564. [Google Scholar] [CrossRef] [PubMed]
- Myasoedova, E.; Crowson, C.S.; Kremers, H.M.; Roger, V.L.; Fitz-Gibbon, P.D.; Therneau, T.M.; Gabriel, S.E. Lipid paradox in rheumatoid arthritis: The impact of serum lipid measures and systemic inflammation on the risk of cardiovascular disease. Ann. Rheum. Dis. 2011, 70, 482–487. [Google Scholar] [CrossRef] [Green Version]
- Chung, C.P.; Oeser, A.; Raggi, P.; Gebretsadik, T.; Shintani, A.K.; Sokka, T.; Pincus, T.; Avalos, I.; Stein, C.M. Increased coronary-artery atherosclerosis in rheumatoid arthritis: Relationship to disease duration and cardiovascular risk factors. Arthritis Rheum. 2005, 52, 3045–3053. [Google Scholar] [CrossRef]
- Liao, K.P.; Cai, T.; Gainer, V.S.; Cagan, A.; Murphy, S.N.; Liu, C.; Churchill, S.; Shaw, S.Y.; Kohane, I.; Solomon, D.H.; et al. Lipid and lipoprotein levels and trend in rheumatoid arthritis compared to the general population. Arthritis Care Res. 2013, 65, 2046–2050. [Google Scholar] [CrossRef]
- Charles-Schoeman, C.; Watanabe, J.; Lee, Y.Y.; Furst, D.E.; Amjadi, S.; Elashoff, D.; Park, G.; McMahon, M.; Paulus, H.E.; Fogelman, A.M.; et al. Abnormal function of high-density lipoprotein is associated with poor disease control and an altered protein cargo in rheumatoid arthritis. Arthritis Rheum. 2009, 60, 2870–2879. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, J.; Charles-Schoeman, C.; Miao, Y.; Elashoff, D.; Lee, Y.Y.; Katselis, G.S.; Lee, T.D.; Reddy, S.T. Proteomic profiling following immunoaffinity capture of high-density lipoprotein: Association of acute-phase proteins and complement factors with proinflammatory high-density lipoprotein in rheumatoid arthritis. Arthritis Rheum. 2012, 64, 1828–1837. [Google Scholar] [CrossRef] [Green Version]
- Vivekanandan-Giri, A.; Slocum, J.L.; Byun, J.; Tang, C.; Sands, R.L.; Gillespie, B.W.; Heinecke, J.W.; Saran, R.; Kaplan, M.J.; Pennathur, S. High density lipoprotein is targeted for oxidation by myeloperoxidase in rheumatoid arthritis. Ann. Rheum. Dis. 2013, 72, 1725–1731. [Google Scholar] [CrossRef] [PubMed]
- Rosso, L.G.; Lhomme, M.; Meroño, T.; Sorroche, P.; Catoggio, L.; Soriano, E.; Saucedo, C.; Malah, V.; Dauteuille, C.; Boero, L.; et al. Altered lipidome and antioxidative activity of small, dense HDL in normolipidemic rheumatoid arthritis: Relevance of inflammation. Atherosclerosis 2014, 237, 652–660. [Google Scholar] [CrossRef] [PubMed]
- Tejera-Segura, B.; Macía-Díaz, M.; Machado, J.D.; De Vera-González, A.; García-Dopico, J.A.; Olmos, J.M.; Hernández, J.L.; Díaz-González, F.; González-Gay, M.A.; Ferraz-Amaro, I. HDL cholesterol efflux capacity in rheumatoid arthritis patients: Contributing factors and relationship with subclinical atherosclerosis. Arthritis Res. Ther. 2017, 19, 113. [Google Scholar] [CrossRef] [Green Version]
- Charles-Schoeman, C.; Lee, Y.Y.; Grijalva, V.; Amjadi, S.; Fitzgerald, J.; Ranganath, V.K.; Taylor, M.; McMahon, M.; E Paulus, H.; Reddy, S.T. Cholesterol efflux by high density lipoproteins is impaired in patients with active rheumatoid arthritis. Ann. Rheum. Dis. 2012, 71, 1157–1162. [Google Scholar] [CrossRef] [PubMed]
- Ronda, N.; Favari, E.; Borghi, M.O.; Ingegnoli, F.; Gerosa, M.; Chighizola, C.; Zimetti, F.; Adorni, M.P.; Bernini, F.; Meroni, P.L. Impaired serum cholesterol efflux capacity in rheumatoid arthritis and systemic lupus erythematosus. Ann. Rheum. Dis. 2014, 73, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Tam, L.-S.; Tomlinson, B.; Chu, T.T.-W.; Li, M.; Leung, Y.-Y.; Kwok, L.-W.; Li, T.K.; Yu, T.; Zhu, Y.-E.; Wong, K.-C.; et al. Cardiovascular risk profile of patients with psoriatic arthritis compared to controls--the role of inflammation. Rheumatology 2008, 47, 718–723. [Google Scholar] [CrossRef] [Green Version]
- Mallbris, L.; Granath, F.; Hamsten, A.; Ståhle, M. Psoriasis is associated with lipid abnormalities at the onset of skin disease. J. Am. Acad. Derm. 2006, 54, 614–621. [Google Scholar] [CrossRef] [PubMed]
- Borska, L.; Kremlacek, J.; Andrys, C.; Krejsek, J.; Hamakova, K.; Borsky, P.; Palicka, V.; Rehacek, V.; Malkova, A.; Fiala, Z. Systemic Inflammation, Oxidative Damage to Nucleic Acids, and Metabolic Syndrome in the Pathogenesis of Psoriasis. Int. J. Mol. Sci. 2017, 18, 2238. [Google Scholar] [CrossRef] [Green Version]
- Nakhwa, Y.C.; Rashmi, R.; Basavaraj, K.H. Dyslipidemia in Psoriasis: A Case Controlled Study. Int. Sch. Res. Not. 2014, 2014, 729157. [Google Scholar] [CrossRef] [Green Version]
- Pietrzak, A.; Chabros, P.; Grywalska, E.; Kicinski, P.; Pietrzak-Franciszkiewicz, K.; Krasowka, D.; Kandzierski, G. Serum lipid metabolism in psoriasis and psoriatic arthritis—An update. Arch. Med. Sci. Ams. 2019, 15, 369–375. [Google Scholar] [CrossRef]
- Pietrzak, A.; Grywalska, E.; Walankiewicz, M.; Lotti, T.; Roliński, J.; Myśliński, W.; Chabros, P.; Piekarska-Myślińska, D.; Reich, K. Psoriasis and metabolic syndrome in children: Current data. Clin. Exp. Derm. 2017, 42, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Veetil, B.M.A.; Matteson, E.L.; Maradit-Kremers, H.; McEvoy, M.T.; Crowson, C.S. Trends in lipid profiles in patients with psoriasis: A population-based analysis. BMC Derm. 2012, 12, 20. [Google Scholar]
- Uyanik, B.S.; Ari, Z.; Onur, E.; Gündüz, K.; Tanülkü, S.; Durkan, K. Serum lipids and apolipoproteins in patients with psoriasis. Clin. Chem. Lab. Med. 2002, 40, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Singal, A.; Asha, K.; Sharma, S.B.; Arora, V.K.; Aggarwal, A. Dyslipidaemia & oxidative stress in patients of psoriasis: Emerging cardiovascular risk factors. Indian J. Med. Res. 2017, 146, 708–713. [Google Scholar]
- Miller, I.; Skaaby, T.; Ellervik, C.; Jemec, G. Quantifying cardiovascular disease risk factors in patients with psoriasis: A meta-analysis. Br. J. Derm. 2013, 169, 1180–1187. [Google Scholar] [CrossRef]
- Yu, Y.; Sheth, N.; Krishnamoorthy, P.; Saboury, B.; Raper, A.; Baer, A.; Ochotony, R.; Doveikis, J.; DerOhannessian, S.; Van Voorhees, A.S.; et al. Aortic vascular inflammation in psoriasis is associated with HDL particle size and concentration: A pilot study. Am. J. Cardiovasc. Dis. 2012, 2, 285–292. [Google Scholar] [PubMed]
- Tom, W.L.; Playford, M.P.; Admani, S.; Natarajan, B.; Joshi, A.A.; Eichenfield, L.F.; Mehta, N.N. Characterization of Lipoprotein Composition and Function in Pediatric Psoriasis Reveals a More Atherogenic Profile. J. Investig. Dermatol. 2016, 136, 67–73. [Google Scholar] [CrossRef] [Green Version]
- Wolk, R.; Armstrong, E.J.; Hansen, P.R.; Thiers, B.; Lan, S.; Tallman, A.M.; Kaur, M.; Tatulych, S. Effect of tofacitinib on lipid levels and lipid-related parameters in patients with moderate to severe psoriasis. J. Clin. Lipidol. 2017, 11, 1243–1256. [Google Scholar] [CrossRef] [Green Version]
- He, L.; Qin, S.; Dang, L.; Song, G.; Yao, S.; Yang, N.; Li, Y. Psoriasis decreases the anti-oxidation and anti-inflammation properties of high-density lipoprotein. Biochim. Biophys. Acta 2014, 1841, 1709–1715. [Google Scholar] [CrossRef] [PubMed]
- Staniak, H.L.; Bittencourt, M.S.; Santos, I.D.S.; Sharovsky, R.; Sabbag, C.; Goulart, A.C.; Lotufo, P.A.; Benseñor, I.M. Association between psoriasis and coronary calcium score. Atherosclerosis 2014, 237, 847–852. [Google Scholar] [CrossRef] [Green Version]
- Holzer, M.; Wolf, P.; Inzinger, M.; Trieb, M.; Curcic, S.; Pasterk, L.; Weger, W.; Heinemann, A.; Marsche, G. Anti-psoriatic therapy recovers high-density lipoprotein composition and function. J. Investig. Dermatol. 2014, 134, 635–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, N.N.; Li, R.; Krishnamoorthy, P.; Yu, Y.; Farver, W.; Rodrigues, A.; Raper, A.; Wilcox, M.; Baer, A.; DerOhannesian, S.; et al. Abnormal lipoprotein particles and cholesterol efflux capacity in patients with psoriasis. Atherosclerosis 2012, 224, 218–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, J.; Huang, Y. Meta-analysis of the association between asthma and serum levels of high-density lipoprotein cholesterol and low-density lipoprotein cholesterol. Ann. Allergy Asthma Immunol. 2017, 118, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Barochia, A.V.; Gordon, E.M.; Kaler, M.; Cuento, R.A.; Theard, P.; Figueroa, D.M.; Yao, X.; Weir, N.A.; Sampson, M.L.; Stylianou, M.; et al. High density lipoproteins and type 2 inflammatory biomarkers are negatively correlated in atopic asthmatics. J. Lipid Res. 2017, 58, 1713–1721. [Google Scholar] [CrossRef] [Green Version]
- Rastogi, D.; Fraser, S.; Oh, J.; Huber, A.M.; Schulman, Y.; Bhagtani, R.H.; Khan, Z.S.; Tesfa, L.; Hall, C.B.; Macian, F. Inflammation, metabolic dysregulation, and pulmonary function among obese urban adolescents with asthma. Am. J. Respir. Crit. Care Med. 2015, 191, 149–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cirillo, D.J.; Agrawal, Y.; Cassano, P.A. Lipids and pulmonary function in the Third National Health and Nutrition Examination Survey. Am. J. Epidemiol. 2002, 155, 842–848. [Google Scholar] [CrossRef] [Green Version]
- Park, S.-W.; Lee, E.H.; Kim, H.J.; Bae, D.-J.; Han, S.; Kim, D.; Jang, A.S.; Uh, S.-T.; Kim, Y.H.; Erle, D.J.; et al. Apolipoprotein A1 potentiates lipoxin A4 synthesis and recovery of allergen-induced disrupted tight junctions in the airway epithelium. Clin. Exp. Allergy 2013, 43, 914–927. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, T.; Ruhdorfer, S.; Weigl, L.; Wessner, D.; Heinrich, J.; Döring, A.; Wichmann, H.-E.; Ring, J. Intake of unsaturated fatty acids and HDL cholesterol levels are associated with manifestations of atopy in adults. Clin. Exp. Allergy 2003, 33, 1360–1367. [Google Scholar] [CrossRef]
- Agón-Banzo, P.J.; Sanmartin, R.; García-Malinis, A.J.; Hernández-Martín, Á.; Puzo, J.; Doste, D.; Pardos, C.; Gilaberte, Y. Body mass index and serum lipid profile: Association with atopic dermatitis in a paediatric population. Australas. J. Derm. 2020, 61, e60–e64. [Google Scholar] [CrossRef]
- Trieb, M.; Wolf, P.; Knuplez, E.; Weger, W.; Schuster, C.; Peinhaupt, M.; Holzer, M.; Trakaki, A.; Eichmann, T.; Lass, A.; et al. Abnormal composition and function of high-density lipoproteins in atopic dermatitis patients. Allergy 2019, 74, 398–402. [Google Scholar] [CrossRef] [Green Version]
- Norata, G.D.; Catapano, A.L. Molecular mechanisms responsible for the antiinflammatory and protective effect of HDL on the endothelium. Vasc. Health Risk Manag. 2005, 1, 119–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norata, G.D.; Pirillo, A.; Catapano, A.L. HDLs, immunity, and atherosclerosis. Curr. Opin. Lipidol. 2011, 22, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Norata, G.D.; Catapano, A.L. HDL and adaptive immunity: A tale of lipid rafts. Atherosclerosis 2012, 225, 34–35. [Google Scholar] [CrossRef] [PubMed]
- Bonacina, F.; Pirillo, A.; Catapano, A.L.; Norata, G.D. Cholesterol membrane content has a ubiquitous evolutionary function in immune cell activation: The role of HDL. Curr. Opin. Lipidol. 2019, 30, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Sala, F.; Catapano, A.L.; Norata, G.D. High density lipoproteins and atherosclerosis: Emerging aspects. J. Geriatr. Cardiol. 2012, 9, 401–407. [Google Scholar]
- Pirillo, A.; Catapano, A.L.; Norata, G.D. Biological Consequences of Dysfunctional HDL. Curr. Med. Chem. 2019, 26, 1644–1664. [Google Scholar] [CrossRef]
- Marsillach, J.; Becker, J.O.; Vaisar, T.; Hahn, B.H.; Brunzell, J.D.; Furlong, C.E.; De Boer, I.H.; McMahon, M.A.; Hoofnagle, A.N. DCCT/EDIC Research Group Paraoxonase-3 is depleted from the high-density lipoproteins of autoimmune disease patients with subclinical atherosclerosis. J. Proteome Res. 2015, 14, 2046–2054. [Google Scholar] [CrossRef] [Green Version]
- Barter, P.J.; Nicholls, S.; Rye, K.-A.; Anantharamaiah, G.M.; Navab, M.; Fogelman, A.M. Antiinflammatory properties of HDL. Circ. Res. 2004, 95, 764–772. [Google Scholar] [CrossRef]
- Riwanto, M.; Landmesser, U. High density lipoproteins and endothelial functions: Mechanistic insights and alterations in cardiovascular disease. J. Lipid. Res. 2013, 54, 3227–3243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norata, G.D.; Pirillo, A.; Catapano, A.L. Modified HDL: Biological and physiopathological consequences. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 371–386. [Google Scholar] [CrossRef]
- Callegari, E.; Norata, G.D.; Inoue, H.; Catapano, A.L. Oxidized-HDL3 modulates the expression of Cox-2 in human endothelial cells. Int. J. Mol. Med. 2006, 18, 209–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norata, G.D.; Banfi, C.; Pirillo, A.; Tremoli, E.; Hamsten, A.; Catapano, A.L.; Eriksson, P. Oxidised-HDL3 induces the expression of PAI-1 in human endothelial cells. Role of p38MAPK activation and mRNA stabilization. Br. J. Haematol. 2004, 127, 97–104. [Google Scholar] [PubMed]
- Munford, R.S.; Hall, C.L.; Lipton, J.M.; Dietschy, J.M. Biological activity, lipoprotein-binding behavior, and in vivo disposition of extracted and native forms of Salmonella typhimurium lipopolysaccharides. J. Clin. Invest. 1982, 70, 877–888. [Google Scholar] [CrossRef] [Green Version]
- Grunfeld, C.; Marshall, M.; Shigenaga, J.K.; Moser, A.H.; Tobias, P.; Feingold, K.R. Lipoproteins inhibit macrophage activation by lipoteichoic acid. J. Lipid. Res. 1999, 40, 245–252. [Google Scholar] [CrossRef]
- Gautier, T.; Lagrost, L. Plasma PLTP (phospholipid-transfer protein): An emerging role in ’reverse lipopolysaccharide transport’ and innate immunity. Biochem. Soc. Trans. 2011, 39, 984–988. [Google Scholar] [CrossRef] [Green Version]
- Hailman, E.; Albers, J.J.; Wolfbauer, G.; Tu, A.-Y.; Wright, S.D. Neutralization and transfer of lipopolysaccharide by phospholipid transfer protein. J. Biol. Chem. 1996, 271, 12172–12178. [Google Scholar] [CrossRef] [Green Version]
- Vesy, C.J.; Kitchens, R.L.; Wolfbauer, G.; Albers, J.J.; Munford, R.S. Lipopolysaccharide-binding protein and phospholipid transfer protein release lipopolysaccharides from gram-negative bacterial membranes. Infect. Immun. 2000, 68, 2410–2417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norata, G.D.; Marchesi, P.; Pirillo, A.; Uboldi, P.; Chiesa, G.; Maina, V.; Garlanda, C.; Mantovani, A.; Catapano, A.L. Long pentraxin 3, a key component of innate immunity, is modulated by high-density lipoproteins in endothelial cells. Arter. Thromb. Vasc. Biol. 2008, 28, 925–931. [Google Scholar] [CrossRef] [Green Version]
- Porte, R.; Davoudian, S.; Asgari, F.; Parente, R.; Mantovani, A.; Garlanda, C.; Bottazzi, B. The Long Pentraxin PTX3 as a Humoral Innate Immunity Functional Player and Biomarker of Infections and Sepsis. Front. Immunol. 2019, 10, 794. [Google Scholar] [CrossRef]
- Norata, G.D.; Marchesi, P.; Venu, V.K.P.; Pasqualini, F.; Anselmo, A.; Moalli, F.; Pizzitola, I.; Garlanda, C.; Mantovani, A.; Catapano, A.L. Deficiency of the long pentraxin PTX3 promotes vascular inflammation and atherosclerosis. Circulation 2009, 120, 699–708. [Google Scholar] [CrossRef] [Green Version]
- Doni, A.; Musso, T.; Morone, D.; Bastone, A.; Zambelli, V.; Sironi, M.; Castagnoli, C.; Cambieri, I.; Stravalaci, M.; Pasqualini, F.; et al. An acidic microenvironment sets the humoral pattern recognition molecule PTX3 in a tissue repair mode. J. Exp. Med. 2015, 212, 905–925. [Google Scholar] [CrossRef]
- Bonacina, F.; Barbieri, S.; Cutuli, L.; Amadio, P.; Doni, A.; Sironi, M.; Tartari, S.; Mantovani, A.; Bottazzi, B.; Garlanda, C.; et al. Vascular pentraxin 3 controls arterial thrombosis by targeting collagen and fibrinogen induced platelets aggregation. Biochim. Biophys. Acta 2016, 1862, 1182–1190. [Google Scholar] [CrossRef]
- Bonacina, F.; Moregola, A.; Porte, R.; Baragetti, A.; Bonavita, E.; Salatin, A.; Grigore, L.; Pellegatta, F.; Molgora, M.; Sironi, M.; et al. Pentraxin 3 deficiency protects from the metabolic inflammation associated to diet-induced obesity. Cardiovasc. Res. 2019, 115, 1861–1872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norata, G.D.; Pirillo, A.; Ammirati, E.; Catapano, A.L. Emerging role of high density lipoproteins as a player in the immune system. Atherosclerosis 2012, 220, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Catapano, A.L.; Pirillo, A.; Bonacina, F.; Norata, G.D. HDL in innate and adaptive immunity. Cardiovasc. Res. 2014, 103, 372–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorci-Thomas, M.G.; Thomas, M.J. Microdomains, Inflammation, and Atherosclerosis. Circ. Res. 2016, 118, 679–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonacina, F.; Coe, D.; Wang, G.; Longhi, M.P.; Baragetti, A.; Moregola, A.; Garlaschelli, K.; Uboldi, P.; Pellegatta, F.; Grigore, L.; et al. Myeloid apolipoprotein E controls dendritic cell antigen presentation and T cell activation. Nat. Commun. 2018, 9, 3083. [Google Scholar] [CrossRef]
- Baragetti, A.; Bonacina, F.; Catapano, A.L.; Norata, G.D. Effect of lipids and lipoproteins on hematopoietic cell metabolism and commitment in atherosclerosis. Immunometabolism 2021, 3, e210014. [Google Scholar]
- Murphy, A.J.; Dragoljevic, D.; Tall, A.R. Cholesterol efflux pathways regulate myelopoiesis: A potential link to altered macrophage function in atherosclerosis. Front. Immunol. 2014, 5, 490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sala, F.; Cutuli, L.; Grigore, L.; Pirillo, A.; Chiesa, G.; Catapano, A.L.; Norata, G.D. Prevalence of classical CD14++/CD16- but not of intermediate CD14++/CD16+ monocytes in hypoalphalipoproteinemia. Int. J. Cardiol. 2013, 168, 2886–2889. [Google Scholar] [CrossRef]
- Ruysschaert, J.M.; Lonez, C. Role of lipid microdomains in TLR-mediated signalling. Biochim. Biophys. Acta 2015, 1848, 1860–1867. [Google Scholar] [CrossRef] [PubMed]
- Yvan-Charvet, L.; Welch, C.; Pagler, T.A.; Ranalletta, M.; Lamkanfi, M.; Han, S.; Ishibashi, M.; Li, R.; Wang, N.; Tall, A.R. Increased inflammatory gene expression in ABC transporter-deficient macrophages: Free cholesterol accumulation, increased signaling via toll-like receptors, and neutrophil infiltration of atherosclerotic lesions. Circulation 2008, 118, 1837–1847. [Google Scholar] [CrossRef]
- De Nardo, D.; Labzin, L.I.; Kono, H.; Seki, R.; Schmidt, S.V.; Beyer, M.; Xu, D.; Zimmer, S.; Lahrmann, C.; Schildberg, F.A.; et al. High-density lipoprotein mediates anti-inflammatory reprogramming of macrophages via the transcriptional regulator ATF3. Nat. Immunol. 2014, 15, 152–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hajishengallis, G.; Li, X.; Chavakis, T. Immunometabolic control of hematopoiesis. Mol. Asp. Med. 2021, 77, 100923. [Google Scholar] [CrossRef]
- Murphy, A.J.; Bijl, N.; Yvan-Charvet, L.; Welch, C.B.; Bhagwat, N.; Reheman, A.; Wang, Y.; Shaw, J.A.; Levine, R.L.; Ni, H.; et al. Cholesterol efflux in megakaryocyte progenitors suppresses platelet production and thrombocytosis. Nat. Med. 2013, 19, 586–594. [Google Scholar] [CrossRef] [Green Version]
- Dragoljevic, D.; Kraakman, M.J.; Nagareddy, P.R.; Ngo, D.; Shihata, W.; Kammoun, H.L.; Whillas, A.; Lee, M.K.S.; Al-Sharea, A.; Pernes, G.; et al. Defective cholesterol metabolism in haematopoietic stem cells promotes monocyte-driven atherosclerosis in rheumatoid arthritis. Eur. Heart J. 2018, 39, 2158–2167. [Google Scholar] [CrossRef] [Green Version]
- van der Vorst, E.P.C.; Theodorou, K.; Wu, Y.; Hoeksema, M.A.; Goossens, P.; Bursill, C.A.; Aliyev, T.; Huitema, L.F.A.; Tas, S.W.; Wolfs, I.M.J.; et al. High-Density Lipoproteins Exert Pro-inflammatory Effects on Macrophages via Passive Cholesterol Depletion and PKC-NF-kappaB/STAT1-IRF1 Signaling. Cell. Metab. 2017, 25, 197–207. [Google Scholar] [CrossRef] [Green Version]
- Smoak, K.A.; Aloor, J.J.; Madenspacher, J.; Merrick, B.A.; Collins, J.B.; Zhu, X.; Cavigiolio, G.; Oda, M.N.; Parks, J.S.; Fessler, M.B. Myeloid differentiation primary response protein 88 couples reverse cholesterol transport to inflammation. Cell. Metab. 2010, 11, 493–502. [Google Scholar] [CrossRef] [Green Version]
- Fotakis, P.; Kothari, V.; Thomas, D.G.; Westerterp, M.; Molusky, M.M.; Altin, E.; Abramowicz, S.; Wang, N.; He, Y.; Heinecke, J.W.; et al. Anti-Inflammatory Effects of HDL (High-Density Lipoprotein) in Macrophages Predominate Over Proinflammatory Effects in Atherosclerotic Plaques. Arter. Thromb. Vasc. Biol. 2019, 39, e253–e272. [Google Scholar] [CrossRef]
- Anderson, H.A.; Roche, P.A. MHC class II association with lipid rafts on the antigen presenting cell surface. Biochim. Biophys. Acta 2015, 1853, 775–780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westerterp, M.; Gautier, E.L.; Ganda, A.; Molusky, M.M.; Wang, W.; Fotakis, P.; Wang, N.; Randolph, G.J.; D’Agati, V.D.; Yvan-Charvet, L.; et al. Cholesterol Accumulation in Dendritic Cells Links the Inflammasome to Acquired Immunity. Cell. Metab. 2017, 25, 1294–1304 e1296. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.H.; Yuan, S.G.; Peng, D.Q.; Zhao, S.P. HDL and ApoA-I inhibit antigen presentation-mediated T cell activation by disrupting lipid rafts in antigen presenting cells. Atherosclerosis 2012, 225, 105–114. [Google Scholar] [CrossRef]
- Perrin-Cocon, L.; Diaz, O.; Carreras, M.; Dollet, S.; Guironnet-Paquet, A.; André, P.; Lotteau, V. High-density lipoprotein phospholipids interfere with dendritic cell Th1 functional maturation. Immunobiology 2012, 217, 91–99. [Google Scholar] [CrossRef]
- Tiniakou, I.; Drakos, E.; Sinatkas, V.; Van Eck, M.; Zannis, V.I.; Boumpas, D.; Verginis, P.; Kardassis, D. High-density lipoprotein attenuates Th1 and th17 autoimmune responses by modulating dendritic cell maturation and function. J. Immunol. 2015, 194, 4676–4687. [Google Scholar] [CrossRef] [Green Version]
- Perrin-Cocon, L.; Coutant, F.; Agaugué, S.; Deforges, S.; André, P.; Lotteau, V. Oxidized low-density lipoprotein promotes mature dendritic cell transition from differentiating monocyte. J. Immunol. 2001, 167, 3785–3791. [Google Scholar] [CrossRef] [Green Version]
- Coutant, F.; Agaugué, S.; Perrin-Cocon, L.; André, P.; Lotteau, V. Sensing environmental lipids by dendritic cell modulates its function. J. Immunol. 2004, 172, 54–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coutant, F.; Miossec, P. Altered dendritic cell functions in autoimmune diseases: Distinct and overlapping profiles. Nat. Rev. Rheumatol. 2016, 12, 703–715. [Google Scholar] [CrossRef] [PubMed]
- Robinson, G.A.; Waddington, K.E.; Pineda-Torra, I.; Jury, E.C. Transcriptional Regulation of T-Cell Lipid Metabolism: Implications for Plasma Membrane Lipid Rafts and T-Cell Function. Front. Immunol. 2017, 8, 1636. [Google Scholar] [CrossRef] [Green Version]
- Mailer, R.K.W.; Gisterå, A.; Polyzos, K.A.; Ketelhuth, D.F.J.; Hansson, G.K. Hypercholesterolemia Enhances T Cell Receptor Signaling and Increases the Regulatory T Cell Population. Sci. Rep. 2017, 7, 15655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aguilar-Ballester, M.; Herrero-Cervera, A.; Vinué, Á.; Martínez-Hervás, S.; González-Navarro, H. Impact of Cholesterol Metabolism in Immune Cell Function and Atherosclerosis. Nutrients 2020, 12, 2021. [Google Scholar]
- Jury, E.C.; Flores-Borja, F.; Kabouridis, P.S. Lipid rafts in T cell signalling and disease. Semin. Cell. Dev. Biol. 2007, 18, 608–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, B.J.; Ong, K.L.; Shrestha, S.; Chen, K.; Tabet, F.; Barter, P.J.; Rye, K.-A. Inhibition of arthritis in the Lewis rat by apolipoprotein A-I and reconstituted high-density lipoproteins. Arter. Thromb. Vasc. Biol. 2014, 34, 543–551. [Google Scholar] [CrossRef] [Green Version]
- Tavori, H.; Su, Y.R.; Yancey, P.G.; Giunzioni, I.; Wilhelm, A.J.; Blakemore, J.L.; Zabalawi, M.; Linton, M.F.; Sorci-Thomas, M.G.; Fazio, S. Macrophage apoAI protects against dyslipidemia-induced dermatitis and atherosclerosis without affecting HDL. J. Lipid. Res. 2015, 56, 635–643. [Google Scholar] [CrossRef] [Green Version]
- Ait-Oufella, H.; Salomon, B.L.; Potteaux, S.; Robertson, A.-K.L.; Gourdy, P.; Zoll, J.; Merval, R.; Esposito, B.; Cohen, J.L.; Fisson, S.; et al. Natural regulatory T cells control the development of atherosclerosis in mice. Nat. Med. 2006, 12, 178–180. [Google Scholar] [CrossRef]
- Klingenberg, R.; Gerdes, N.; Badeau, R.M.; Gisterå, A.; Strodthoff, D.; Ketelhuth, D.F.J.; Lundberg, A.M.; Rudling, M.; Nilsson, S.K.; Olivecrona, G.; et al. Depletion of FOXP3+ regulatory T cells promotes hypercholesterolemia and atherosclerosis. J. Clin. Invest. 2013, 123, 1323–1334. [Google Scholar] [CrossRef]
- Cheng, H.-Y.; Gaddis, D.E.; Wu, R.; McSkimming, C.; Haynes, L.D.; Taylor, A.M.; McNamara, C.A.; Sorci-Thomas, M.; Hedrick, C.C. Loss of ABCG1 influences regulatory T cell differentiation and atherosclerosis. J. Clin. Invest. 2016, 126, 3236–3246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilhelm, A.J.; Zabalawi, M.; Owen, J.S.; Shah, D.; Grayson, J.M.; Major, A.S.; Bhat, S.; Gibbs, D.P., Jr.; Thomas, M.J.; Sorci-Thomas, M.G. Apolipoprotein A-I modulates regulatory T cells in autoimmune LDLr-/-, ApoA-I-/- mice. J. Biol. Chem. 2010, 285, 36158–36169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaddis, D.E.; Padgett, L.E.; Wu, R.; McSkimming, C.; Romines, V.; Taylor, A.M.; McNamara, C.A.; Kronenberg, M.; Crotty, S.; Thomas, M.J.; et al. Apolipoprotein AI prevents regulatory to follicular helper T cell switching during atherosclerosis. Nat. Commun. 2018, 9, 1095. [Google Scholar] [CrossRef]
- Rueda, C.M.; Rodríguez-Perea, A.L.; Moreno-Fernandez, M.; Jackson, C.M.; Melchior, J.T.; Davidson, W.S.; Chougnet, C.A. High density lipoproteins selectively promote the survival of human regulatory T cells. J. Lipid Res. 2017, 58, 1514–1523. [Google Scholar] [CrossRef] [Green Version]
- Rosenson, R.S.; Jr, H.B.B.; Barter, P.J.; Björkegren, J.L.M.; Chapman, M.J.; Gaudet, D.; Kim, D.S.; Niesor, E.; Rye, K.-A.; Sacks, F.M.; et al. HDL and atherosclerotic cardiovascular disease: Genetic insights into complex biology. Nat. Rev. Cardiol. 2018, 15, 9–19. [Google Scholar] [CrossRef]
- Bochem, A.E.; Van Der Valk, F.M.; Tolani, S.; Stroes, E.S.; Westerterp, M.; Tall, A.R. Increased systemic and plaque inflammation in ABCA1 mutation carriers with attenuation by statins. Arter. Thromb. Vasc. Biol. 2015, 35, 1663–1669. [Google Scholar] [CrossRef] [Green Version]
- Westerterp, M.; Fotakis, P.; Ouimet, M.; Bochem, A.E.; Zhang, H.; Molusky, M.M.; Wang, W.; Abramowicz, S.; Gemert, S.L.B.-V.; Wang, N.; et al. Cholesterol Efflux Pathways Suppress Inflammasome Activation, NETosis, and Atherogenesis. Circulation 2018, 138, 898–912. [Google Scholar] [CrossRef] [Green Version]
- Voight, B.F.; Peloso, G.M.; Orho-Melander, M.; Frikke-Schmidt, R.; Barbalic, M.; Jensen, M.K.; Hindy, G.; Hólm, H.; Ding, E.L.; Johnson, T.; et al. Plasma HDL cholesterol and risk of myocardial infarction: A mendelian randomisation study. Lancet 2012, 380, 572–580. [Google Scholar] [CrossRef] [Green Version]
- Harslof, M.; Pedersen, K.M.; Nordestgaard, B.G.; Afzal, S. Low HDL (High-Density Lipoprotein) Cholesterol and High White Blood Cell Counts: A Mendelian Randomization Study. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 976–987. [Google Scholar] [CrossRef] [PubMed]
- Trinder, M.; Walley, K.R.; Boyd, J.H.; Brunham, L.R. Causal Inference for Genetically Determined Levels of High-Density Lipoprotein Cholesterol and Risk of Infectious Disease. Arter. Thromb. Vasc. Biol. 2020, 40, 267–278. [Google Scholar] [CrossRef] [PubMed]
- Genga, K.R.; Trinder, M.; Kong, H.J.; Li, X.; Leung, A.K.K.; Shimada, T.; Walley, K.R.; Russell, J.A.; Francis, G.A.; Brunham, L.R.; et al. CETP genetic variant rs1800777 (allele A) is associated with abnormally low HDL-C levels and increased risk of AKI during sepsis. Sci. Rep. 2018, 8, 16764. [Google Scholar] [CrossRef] [Green Version]
- Blauw, L.L.; Wang, Y.; van Dijk, K.W.; Rensen, P.C. A novel role for CETP as immunological gatekeeper: Raising HDL to cure sepsis? Trends Endocrinol. Metab. Tem 2020, 31, 334–343. [Google Scholar] [CrossRef]
- Petropoulou, P.-I.; Berbée, J.F.; Theodoropoulos, V.; Hatziri, A.; Stamou, P.; Karavia, E.A.; Spyridonidis, A.; Karagiannides, I.; Kypreos, K.E. Lack of LCAT reduces the LPS-neutralizing capacity of HDL and enhances LPS-induced inflammation in mice. Biochim. Biophys. Acta 2015, 1852, 2106–2115. [Google Scholar] [CrossRef] [Green Version]
- Valanti, E.K.; Dalakoura-Karagkouni, K.; Sanoudou, D. Current and Emerging Reconstituted HDL-apoA-I and HDL-apoE Approaches to Treat Atherosclerosis. J. Pers. Med. 2018, 8, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilmore, S.F.; Carpenter, T.S.; Ingólfsson, H.I.; Peters, S.K.G.; Henderson, P.T.; Blanchette, C.D.; Fischer, N.O. Lipid composition dictates serum stability of reconstituted high-density lipoproteins: Implications for in vivo applications. Nanoscale 2018, 10, 7420–7430. [Google Scholar] [CrossRef]
- Van Linthout, S.; Frias, M.; Singh, N.; De Geest, B. Therapeutic potential of HDL in cardioprotection and tissue repair. Handb Exp. Pharm. 2015, 224, 527–565. [Google Scholar]
- Nieuwdorp, M.; Vergeer, M.; Bisoendial, R.J.; Roodt, J.O.‘T.; Levels, H.; Birjmohun, R.S.; Kuivenhoven, J.A.; Basser, R.; Rabelink, T.J.; Kastelein, J.J.P.; et al. Reconstituted HDL infusion restores endothelial function in patients with type 2 diabetes mellitus. Diabetologia 2008, 51, 1081–1084. [Google Scholar] [CrossRef] [Green Version]
- Patel, S.; Drew, B.G.; Nakhla, S.; Duffy, S.J.; Murphy, A.J.; Barter, P.J.; Rye, K.-A.; Chin-Dusting, J.; Hoang, A.; Sviridov, D.; et al. Reconstituted high-density lipoprotein increases plasma high-density lipoprotein anti-inflammatory properties and cholesterol efflux capacity in patients with type 2 diabetes. J. Am. Coll. Cardiol. 2009, 53, 962–971. [Google Scholar] [CrossRef] [Green Version]
- Shaw, J.A.; Bobik, A.; Murphy, A.; Kanellakis, P.; Blombery, P.; Mukhamedova, N.; Woollard, K.; Lyon, S.; Sviridov, D.; Dart, A.M. Infusion of reconstituted high-density lipoprotein leads to acute changes in human atherosclerotic plaque. Circ. Res. 2008, 103, 1084–1091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nissen, S.E.; Tsunoda, T.; Tuzcu, E.M.; Schoenhagen, P.; Cooper, C.J.; Yasin, M.; Eaton, G.M.; Lauer, M.A.; Sheldon, W.S.; Grines, C.L. Effect of recombinant ApoA-I Milano on coronary atherosclerosis in patients with acute coronary syndromes: A randomized controlled trial. JAMA 2003, 290, 2292–2300. [Google Scholar] [CrossRef] [PubMed]
- Tardif, J.-C.; Grégoire, J.; L’Allier, P.L.; Ibrahim, R.; Lespérance, J.; Heinonen, T.M.; Kouz, S.; Berry, C.; Basser, R.; Lavoie, M.-A.; et al. Effects of reconstituted high-density lipoprotein infusions on coronary atherosclerosis: A randomized controlled trial. JAMA 2007, 297, 1675–1682. [Google Scholar] [CrossRef] [Green Version]
- Trinder, M.; Wang, Y.; Madsen, C.M.; Ponomarev, T.; Bohunek, L.; Daisely, B.A.; Kong, H.J.; Blauw, L.L.; Nordestgaard, B.G.; Tybjærg-Hansen, A.; et al. Inhibition of Cholesteryl Ester Transfer Protein Preserves High-Density Lipoprotein Cholesterol and Improves Survival in Sepsis. Circulation 2021, 143, 921–934. [Google Scholar] [CrossRef]
- Trinder, M.; Genga, K.R.; Kong, H.J.; Blauw, L.L.; Lo, C.; Li, X.; Cirstea, M.; Wang, Y.; Rensen, P.C.N.; Russell, J.A.; et al. Cholesteryl Ester Transfer Protein Influences High-Density Lipoprotein Levels and Survival in Sepsis. Am. J. Respir. Crit. Care Med. 2019, 199, 854–862. [Google Scholar] [CrossRef]
- Ossoli, A.; Simonelli, S.; Varrenti, M.; Morici, N.; Oliva, F.; Stucchi, M.; Gomaraschi, M.; Strazzella, A.; Arnaboldi, L.; Thomas, M.J.; et al. Recombinant LCAT (Lecithin:Cholesterol Acyltransferase) Rescues Defective HDL (High-Density Lipoprotein)-Mediated Endothelial Protection in Acute Coronary Syndrome. Arter. Thromb. Vasc. Biol. 2019, 39, 915–924. [Google Scholar] [CrossRef] [PubMed]
- Sorokin, A.V.; Karathanasis, S.K.; Yang, Z.; Freeman, L.; Kotani, K.; Remaley, A.T. COVID-19-Associated dyslipidemia: Implications for mechanism of impaired resolution and novel therapeutic approaches. FASEB J. 2020, 34, 9843–9853. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Zhang, Q.; Zhao, X.; Dong, H.; Wu, C.; Wu, F.; Yu, B.; Lv, J.; Zhang, S.; Wu, G.; et al. Low high-density lipoprotein level is correlated with the severity of COVID-19 patients: An observational study. Lipids Health Dis. 2020, 19, 204. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Chen, D.; Wu, L.; He, G.; Ye, W. Declined serum high density lipoprotein cholesterol is associated with the severity of COVID-19 infection. Clin. Chim. Acta 2020, 510, 105–110. [Google Scholar] [CrossRef]
- Wei, X.; Zeng, W.; Su, J.; Wan, H.; Yu, X.; Cao, X.; Tan, W.; Wang, H. Hypolipidemia is associated with the severity of COVID-19. J. Clin. Lipidol. 2020, 14, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Begue, F.; Tanaka, S.; Mouktadi, Z.; Rondeau, P.; Veeren, B.; Diotel, N.; Tran-Dinh, A.; Robert, T.; Vélia, E.; Mavingui, P.; et al. Altered high-density lipoprotein composition and functions during severe COVID-19. Sci. Rep. 2021, 11, 2291. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Role of cholesterol efflux in innate immune cell activation. (A) TLR4, which is expressed in innate immune cells including monocytes, macrophages and dendritic cells, is activated by lipopolysaccharide (LPS). These cells express also high amounts of CD14, which facilitates the activation of TLR4 by LPS. LPS induces a transient TLR4 trafficking to lipid rafts; following dimerization, a process required for the initiation of signaling during innate immune response, TLR4 triggers the MyD88-dependent signaling pathway, leading to the production of pro-inflammatory cytokines and cell activation. ApoA-I and HDL, as well as apoE, may dampen inflammation by selectively reducing the free cholesterol content in lipid rafts and the consequent chance of an MyD88-dependent TLR trafficking to lipid rafts in cells exposed to LPS. PL: phospholipids. (B) In resting T-cells, TCR is localized in non-raft domains of plasma membrane in monomeric form. Cholesterol is imported into the cell LDL; when TCRs become antigen stimulated, they associate with lipid rafts, thus resulting in the activation of downstream signaling pathways and consequent T cell proliferation. ApoA-I and HDL, by removing cholesterol from cell membrane, may modulate the abundance of lipid rafts and their content of cholesterol, thus controlling T cell immune response.
Figure 1.
Role of cholesterol efflux in innate immune cell activation. (A) TLR4, which is expressed in innate immune cells including monocytes, macrophages and dendritic cells, is activated by lipopolysaccharide (LPS). These cells express also high amounts of CD14, which facilitates the activation of TLR4 by LPS. LPS induces a transient TLR4 trafficking to lipid rafts; following dimerization, a process required for the initiation of signaling during innate immune response, TLR4 triggers the MyD88-dependent signaling pathway, leading to the production of pro-inflammatory cytokines and cell activation. ApoA-I and HDL, as well as apoE, may dampen inflammation by selectively reducing the free cholesterol content in lipid rafts and the consequent chance of an MyD88-dependent TLR trafficking to lipid rafts in cells exposed to LPS. PL: phospholipids. (B) In resting T-cells, TCR is localized in non-raft domains of plasma membrane in monomeric form. Cholesterol is imported into the cell LDL; when TCRs become antigen stimulated, they associate with lipid rafts, thus resulting in the activation of downstream signaling pathways and consequent T cell proliferation. ApoA-I and HDL, by removing cholesterol from cell membrane, may modulate the abundance of lipid rafts and their content of cholesterol, thus controlling T cell immune response.


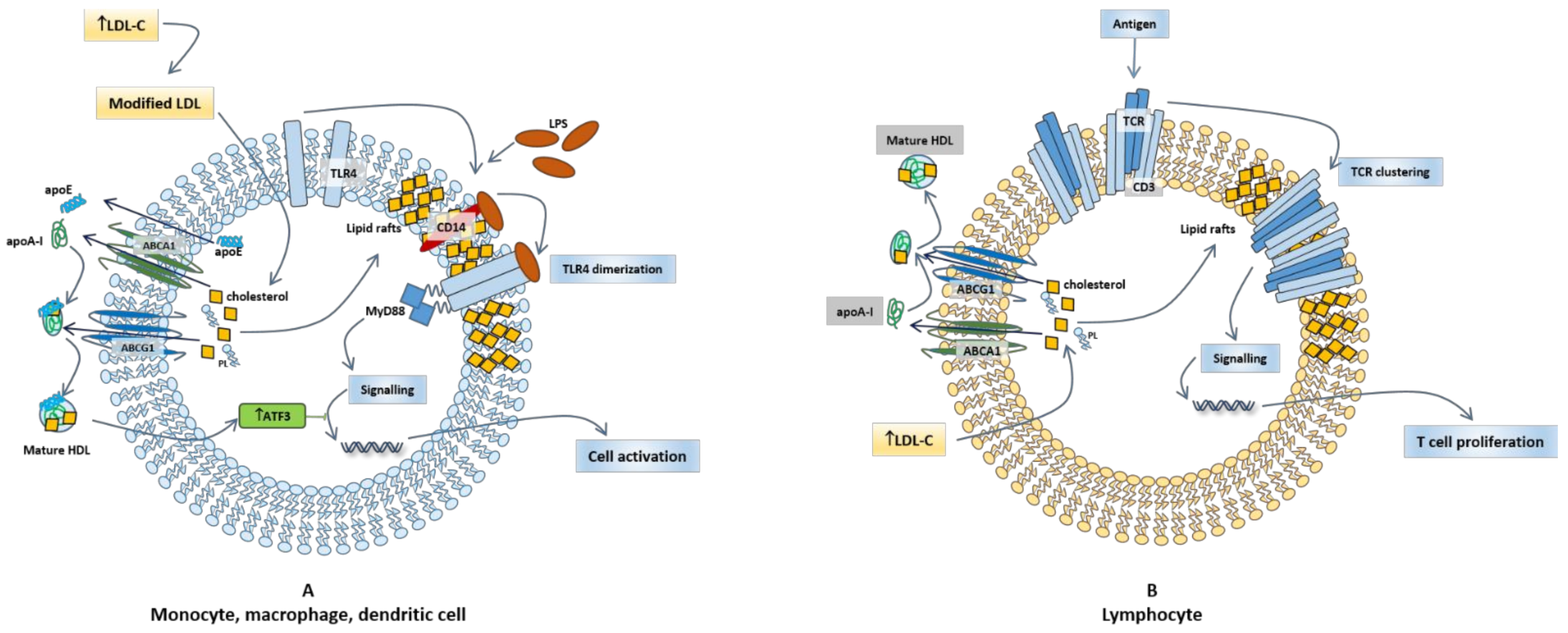{kind=link}
Table 1.
Major HDL alterations in selected autoimmune diseases.
| Autoimmune Disease | HDL Alterations (Level/Function) | Reference |
|---|---|---|
| Systemic lupus erythematosus | Reduced levels of HDL-C | de Carvalho JF et al., 2008 [31]; Hahn BH et al., 2008 [32]; Toloza SMA et al., 2004 [33]; Gamal SM et al., 2017 [34] |
| No difference in HDL-C levels | ||
| “Lupus dyslipoproteinemia” | Yuan J et al., 2016 [35] | |
| Reduced PON1 activity | Kiss E et al., 2007 [36]; Gaal K et al., 2011 [37] | |
| Pro-inflammatory HDL (piHDL) with increased SAA content, decreased apoA-I levels | McMahon M et al., 2011 [38]; G HB et al., 2011 [39]; Van Lenten BJ et al., 2001 [40] | |
| Oxidized HDL | Smith CK et al., 2014 [41] | |
| Reduced HDL particles/size distribution | Chung CP et al., 2008 [42]; Hua X et al., 2009 [43]; Juarez-Rojas J et al., 2008 [44] | |
| Reduced CEC | Smith CK et al., 2014 [41]; Skaggs BJ et al., 2010 [45] | |
| Reduced anti-inflammatory potential | Smith CK et al., 2016 [46] | |
| Rheumatoid arthritis | Reduced levels of HDL-C | Jae-Yong Kim et al., 2016 [47]; Myasoedova E et al., 2011 [48] |
| No difference in HDL-C | Chung CP et al., 2005 [49]; Liao KP et al., 2013 [50] | |
| Pro-inflammatory HDL (piHDL) | Hahn BH et al., 2008 [32]; Charles-Schoeman C et al., 2009 [51]; Watanabe J et al., 2012 [52] | |
| Oxidized HDL | Vivekanandan-Giri A et al., 2013 [53] | |
| Reduced anti-oxidative activity | Gomez Rosso L et al., 2014 (in patients with active disease) [54] | |
| Reduced CEC | Beatriz Tejera-Segura et al., 2017 (in patients with low or moderate disease activity compared to patients in remission) [55]; Charles-Schoeman C et al., 2012 [56]; Ronda N et al., 2014 [57] | |
| Psoriasis | Increased HDL-C levels | Tam LS et al., 2008 [58]; Mallbris L et al., 2006 [59]; Borska L et al., 2017 [60]; Nakhawa YC et al., 2014 [61] |
| Decreased HDL-C levels | Pietrzak A et al., 2019 [62]; Pietrzak A et al., 2017 [63]; Akkara Veetil BM et al., 2012 [64] | |
| Unchanged HDL-C levels | Uyanik BS et al., 2002 [65]; Asha K et al., 2017 [66]; Miller IM et al., 2013 [67] | |
| Change in HDL particle size | Yu Y et al., 2012 [68]; Tom WL et al., 2016 [69]; Wolk R et al., 2017 [70] | |
| Pro-inflammatory HDL (piHDL) | He L et al., 2014 [71]; Staniak HL et al., 2014 [72] | |
| Reduced CEC | Holzer M et al., 2012 [24]; Tom WL et al., 2016 [69]; Holzer M et al., 2014 [73]; Mehta NN et al., 2012 [74] | |
| Chron’s disease | Decreased HDL-C levels and biochemical changes in HDL particles | Romanato G et al., 2009 [10] |
| Allergic asthma | Lower HDL levels (only children) | Peng J et al., 2017 [75] |
| Inverse correlation between HDL-C levels and circulating eosinophils and monocytes | Barochia AV et al., 2017 [76]; Rastogi D et al., 2015 [77] | |
| Positive correlation of serum apoA-I levels with less severe airflow obstruction in asthmatic individuals | Cirillo DJ et al., 2002 [78] | |
| ApoA-I levels decreased in bronchoalveolar lavage fluid of patients with moderate to severe asthma | Park SW et al., 2013 [79] | |
| Atopic dermatitis | Increased HDL-C levels in patients | Schäfer T et al., 2003 [80] |
| No difference in a paediatric population | Agón-Banzo PJ et al., 2020 [81] | |
| HDL enrichment in apoA-II, SAA, and phosphatidylinositol and significant reduction in the content of apoC-III, apoE, cholesteryl ester, free cholesterol, lysophosphatidylcholine, and phosphatidylethanolamine | Trieb et al., 2019 [82] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Bonacina, F.; Pirillo, A.; Catapano, A.L.; Norata, G.D. HDL in Immune-Inflammatory Responses: Implications beyond Cardiovascular Diseases. Cells 2021, 10, 1061. https://doi.org/10.3390/cells10051061
AMA Style
Bonacina F, Pirillo A, Catapano AL, Norata GD. HDL in Immune-Inflammatory Responses: Implications beyond Cardiovascular Diseases. Cells. 2021; 10(5):1061. https://doi.org/10.3390/cells10051061
Chicago/Turabian StyleBonacina, Fabrizia, Angela Pirillo, Alberico L. Catapano, and Giuseppe D. Norata. 2021. "HDL in Immune-Inflammatory Responses: Implications beyond Cardiovascular Diseases" Cells 10, no. 5: 1061. https://doi.org/10.3390/cells10051061
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.