Current Challenges in Providing Good Leukapheresis Products for Manufacturing of CAR-T Cells for Patients with Relapsed/Refractory NHL or ALL

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Healthy Donors
2.2. Leukapheresis Procedures
2.3. Leukapheresis Product
2.4. CAR-T Cell Products
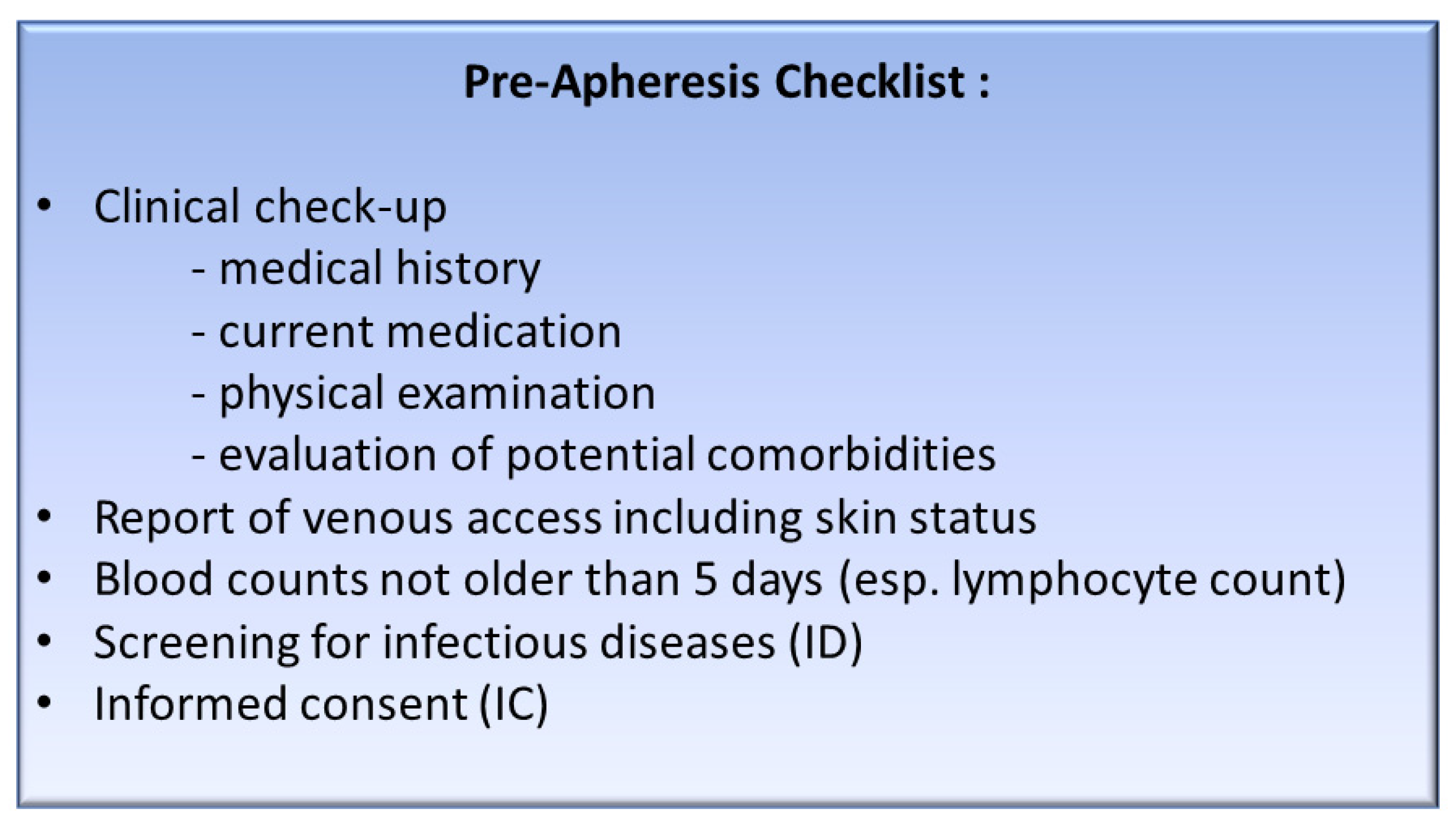
2.5. Clinical Evaluation
2.6. Data Analysis
3. Results
3.1. Patients Characteristics
3.2. Baseline Analysis
3.3. Apheresis Conditions
3.4. Apheresis Concentrate Characteristics
3.5. CAR-T Cell Manufacturing
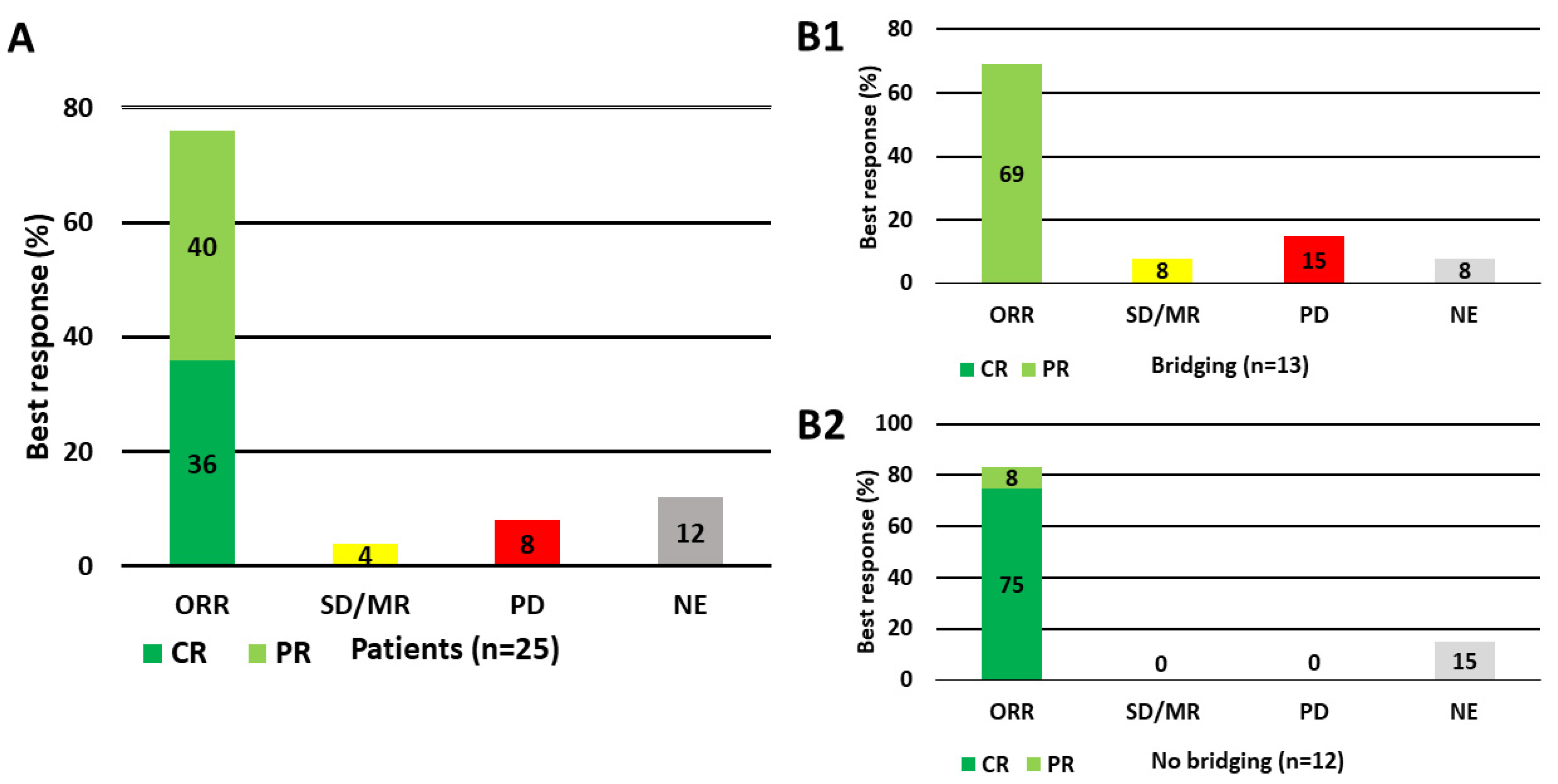
3.6. Remission Status Obtained in the Patient
3.7. Pre-Apheresis Lymphocyte Count and CD3+ Cell Yield by Response
3.8. Comparison of Leukapheresis Products from Patients by Remission Status and Healthy Donors
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Schuster, S.J.; Bishop, M.R.; Tam, C.S.; Waller, E.K.; Borchmann, P.; McGuirk, J.P.; Jager, U.; Jaglowski, S.; Andreadis, C.; Westin, J.R.; et al. Tisagenlecleucel in adult relapsed or refractory diffuse large B-cell lymphoma. N. Engl. J. Med. 2019, 380, 45–56. [Google Scholar] [CrossRef]
- Neelapu, S.S.; Locke, F.L.; Bartlett, N.L.; Lekakis, L.J.; Miklos, D.B.; Jacobson, C.A.; Braunschweig, I.; Oluwole, O.O.; Siddiqi, T.; Lin, Y.; et al. Axicabtagene ciloleucel car t-cell therapy in refractory large B-cell lymphoma. N. Engl. J. Med. 2017, 377, 2531–2544. [Google Scholar] [CrossRef]
- Chavez, J.C.; Bachmeier, C.; Kharfan-Dabaja, M.A. Car T-cell therapy for B-cell lymphomas: Clinical trial results of available products. Ther. Adv. Hematol. 2019, 10, 2040620719841581. [Google Scholar] [CrossRef] [Green Version]
- Schubert, M.L.; Huckelhoven, A.; Hoffmann, J.M.; Schmitt, A.; Wuchter, P.; Sellner, L.; Hofmann, S.; Ho, A.D.; Dreger, P.; Schmitt, M. Chimeric antigen receptor T cell therapy targeting cd19-positive leukemia and lymphoma in the context of stem cell transplantation. Hum. Gene Ther. 2016, 27, 758–771. [Google Scholar] [CrossRef]
- Schubert, M.L.; Hoffmann, J.M.; Dreger, P.; Muller-Tidow, C.; Schmitt, M. Chimeric antigen receptor transduced T cells: Tuning up for the next generation. Int. J. Cancer 2018, 142, 1738–1747. [Google Scholar] [CrossRef] [Green Version]
- Fesnak, A.; Lin, C.; Siegel, D.L.; Maus, M.V. Car-T cell therapies from the transfusion medicine perspective. Transfus. Med. Rev. 2016, 30, 139–145. [Google Scholar] [CrossRef] [Green Version]
- Dwivedy Nasta, S.; Hughes, M.E.; Namoglu, E.C.; Landsburg, D.J.; Chong, E.A.; Barta, S.K.; Frey, N.V.; Gerson, J.N.; Maity, A.; Plastaras, J.; et al. A characterization of bridging therapies leading up to commercial car T-cell therapy. Blood 2019, 134, 4108. [Google Scholar] [CrossRef]
- Schubert, M.L.; Schmitt, A.; Sellner, L.; Neuber, B.; Kunz, J.; Wuchter, P.; Kunz, A.; Gern, U.; Michels, B.; Hofmann, S.; et al. Treatment of patients with relapsed or refractory cd19+ lymphoid disease with T lymphocytes transduced by rv-sfg.Cd19.Cd28.4-1bbzeta retroviral vector: A unicentre phase i/ii clinical trial protocol. BMJ Open 2019, 9, e026644. [Google Scholar] [CrossRef] [Green Version]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: The Lugano classification. J. Clin. Oncol. 2014, 32, 3059–3068. [Google Scholar] [CrossRef]
- Berry, D.A.; Zhou, S.; Higley, H.; Mukundan, L.; Fu, S.; Reaman, G.H.; Wood, B.L.; Kelloff, G.J.; Jessup, J.M.; Radich, J.P. Association of minimal residual disease with clinical outcome in pediatric and adult acute lymphoblastic leukemia: A meta-analysis. JAMA Oncol. 2017, 3, e170580. [Google Scholar] [CrossRef]
- Horvat, M.; Zadnik, V.; Juznic Setina, T.; Boltezar, L.; Pahole Golicnik, J.; Novakovic, S.; Jezersek Novakovic, B. Diffuse large B-cell lymphoma: 10 years’ real-world clinical experience with rituximab plus cyclophosphamide, doxorubicin, vincristine and prednisolone. Oncol. Lett. 2018, 15, 3602–3609. [Google Scholar] [CrossRef] [PubMed]
- Savage, K.J.; Al-Rajhi, N.; Voss, N.; Paltiel, C.; Klasa, R.; Gascoyne, R.D.; Connors, J.M. Favorable outcome of primary mediastinal large B-cell lymphoma in a single institution: The British Columbia experience. Ann. Oncol. 2006, 17, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Schulz, M.; Bialleck, H.; Thorausch, K.; Bug, G.; Dunzinger, U.; Seifried, E.; Bonig, H. Unstimulated leukapheresis in patients and donors: Comparison of two apheresis systems. Transfusion 2014, 54, 1622–1629. [Google Scholar] [CrossRef] [PubMed]
- Kondo, N.; Takahashi, A.; Ono, K.; Ohnishi, T. DNA damage induced by alkylating agents and repair pathways. J. Nucleic Acids 2010, 2010, 543531. [Google Scholar] [CrossRef] [Green Version]
- Fei, F.; Yu, Y.; Schmitt, A.; Rojewski, M.T.; Chen, B.; Gotz, M.; Guillaume, P.; Bunjes, D.; Schmitt, M. The inhibitory effect of cyclosporine a and prednisolone on both cytotoxic cd8+ T cells and cd4+cd25+ regulatory T cells. Curr. Signal Transduct. Ther. 2009, 4, 222–233. [Google Scholar] [CrossRef]
- Czock, D.; Keller, F.; Rasche, F.M.; Häussler, U. Pharmacokinetics and pharmacodynamics of systemically administered glucocorticoids. Clin. Pharmacokinet. 2005, 44, 61–98. [Google Scholar] [CrossRef]
- Davis, T.E.; Kis-Toth, K.; Szanto, A.; Tsokos, G.C. Glucocorticoids suppress T cell function by up-regulating microrna-98. Arthritis Rheum. 2013, 65, 1882–1890. [Google Scholar] [CrossRef] [Green Version]
- Fan, P.T.; Yu, D.T.; Clements, P.J.; Fowlston, S.; Eisman, J.; Bluestone, R. Effect of corticosteroids on the human immune response: Comparison of one and three daily 1 gm intravenous pulses of methylprednisolone. J. Lab. Clin. Med. 1978, 91, 625–634. [Google Scholar]
- Olnes, M.J.; Kotliarov, Y.; Biancotto, A.; Cheung, F.; Chen, J.; Shi, R.; Zhou, H.; Wang, E.; Tsang, J.S.; Nussenblatt, R.; et al. Effects of systemically administered hydrocortisone on the human immunome. Sci. Rep. 2016, 6, 23002. [Google Scholar] [CrossRef] [Green Version]
- Mitsui, K.; Ide, K.; Takahashi, T.; Kosai, K.I. Viral vector-based innovative approaches to directly abolishing tumorigenic pluripotent stem cells for safer regenerative medicine. Mol. Ther. Methods Clin. Dev. 2017, 5, 51–58. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, J.; Mielcarek, M.; Torok-Storb, B. Impaired induction of the cd28-responsive complex in granulocyte colony-stimulating factor mobilized cd4 T cells. Blood 1998, 91, 347–352. [Google Scholar] [CrossRef]
- Shank, B.R.; Do, B.; Sevin, A.; Chen, S.E.; Neelapu, S.S.; Horowitz, S.B. Chimeric antigen receptor T cells in hematologic malignancies. Pharmacotherapy 2017, 37, 334–345. [Google Scholar] [CrossRef]
- Rubin, L.G.; Levin, M.J.; Ljungman, P.; Davies, E.G.; Avery, R.; Tomblyn, M.; Bousvaros, A.; Dhanireddy, S.; Sung, L.; Keyserling, H.; et al. 2013 IDSA clinical practice guideline for vaccination of the immunocompromised host. Clin. Infect. Dis. 2013, 58, e44–e100. [Google Scholar] [CrossRef] [Green Version]
- Perica, K.; Curran, K.J.; Park, J.H. Chapter 4—Peri-car T-cell management. In Chimeric Antigen Receptor T-Cell Therapies for Cancer; Lee, D.W., Shah, N.N., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 29–44. [Google Scholar]
- Duell, J.; Lammers, P.E.; Djuretic, I.; Chunyk, A.G.; Alekar, S.; Jacobs, I.; Gill, S. Bispecific antibodies in the treatment of hematologic malignancies. Clin. Pharmacol. Ther. 2019, 106, 781–791. [Google Scholar] [CrossRef] [Green Version]
- Hedrich, W.D.; Fandy, T.E.; Ashour, H.M.; Wang, H.; Hassan, H.E. Antibody-drug conjugates: Pharmacokinetic/pharmacodynamic modeling, preclinical characterization, clinical studies, and lessons learned. Clin. Pharmacokinet. 2018, 57, 687–703. [Google Scholar] [CrossRef]
- Betts, A.M.; Haddish-Berhane, N.; Tolsma, J.; Jasper, P.; King, L.E.; Sun, Y.; Chakrapani, S.; Shor, B.; Boni, J.; Johnson, T.R. Preclinical to clinical translation of antibody-drug conjugates using pk/pd modeling: A retrospective analysis of inotuzumab ozogamicin. AAPS J. 2016, 18, 1101–1116. [Google Scholar]
- Klinger, M.; Brandl, C.; Zugmaier, G.; Hijazi, Y.; Bargou, R.C.; Topp, M.S.; Gokbuget, N.; Neumann, S.; Goebeler, M.; Viardot, A.; et al. Immunopharmacologic response of patients with b-lineage acute lymphoblastic leukemia to continuous infusion of T cell-engaging cd19/cd3-bispecific bite antibody blinatumomab. Blood 2012, 119, 6226–6233. [Google Scholar] [CrossRef]
- Fraietta, J.A.; Beckwith, K.A.; Patel, P.R.; Ruella, M.; Zheng, Z.; Barrett, D.M.; Lacey, S.F.; Melenhorst, J.J.; McGettigan, S.E.; Cook, D.R.; et al. Ibrutinib enhances chimeric antigen receptor T-cell engraftment and efficacy in leukemia. Blood 2016, 127, 1117–1127. [Google Scholar] [CrossRef] [Green Version]
- Ruella, M.; Kenderian, S.S.; Shestova, O.; Fraietta, J.A.; Qayyum, S.; Zhang, Q.; Maus, M.V.; Liu, X.; Nunez-Cruz, S.; Klichinsky, M.; et al. The addition of the BTK inhibitor ibrutinib to anti-cd19 chimeric antigen receptor T cells (CART19) improves responses against mantle cell lymphoma. Clin. Cancer Res. 2016, 22, 2684–2696. [Google Scholar] [CrossRef] [Green Version]
- Gill, S.; Frey, N.V.; Hexner, E.O.; Lacey, S.F.; Melenhorst, J.J.; Byrd, J.C.; Metzger, S.; Marcus, T.; Gladney, W.; Marcucci, K.; et al. Cd19 car-T cells combined with ibrutinib to induce complete remission in CLL. J. Clin. Oncol. 2017, 35, 7509. [Google Scholar] [CrossRef]
- Silberstein, L.; Anastasi, J. Chapter T cell therapy of hematological diseases. In Hematology: Basic Principles and Practice, 7th ed.; Hoffman, R.B., Heslop, H., Weitz, J., Eds.; Elsevier: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Allen, E.S.; Stroncek, D.F.; Ren, J.; Eder, A.F.; West, K.A.; Fry, T.J.; Lee, D.W.; Mackall, C.L.; Conry-Cantilena, C. Autologous lymphapheresis for the production of chimeric antigen receptor T cells. Transfusion 2017, 57, 1133–1141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceppi, F.; Rivers, J.; Annesley, C.; Pinto, N.; Park, J.R.; Lindgren, C.; Mgebroff, S.; Linn, N.; Delaney, M.; Gardner, R.A. Lymphocyte apheresis for chimeric antigen receptor T-cell manufacturing in children and young adults with leukemia and neuroblastoma. Transfusion 2018, 58, 1414–1420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruella, M.; Xu, J.; Barrett, D.M.; Fraietta, J.A.; Reich, T.J.; Ambrose, D.E.; Klichinsky, M.; Shestova, O.; Patel, P.R.; Kulikovskaya, I.; et al. Induction of resistance to chimeric antigen receptor T cell therapy by transduction of a single leukemic B cell. Nat. Med. 2018, 10, 1499–1503. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Therapeutic Framework/Indication | Apheresis Procedure | Leukapheresis Product | Application | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Commercial Product (C)/Clinical Trial Product (T) | Indication | HK (%) | Anticoagulant | TNC × 108 | CD3+ × 108 | CD3+ of TNC (%) | Lympho-Depleting Chemotherapy | CAR-T Cell Dose | Time Thawing—Transfusion | |
| C | Axicabtagen Ciloleucel | r/r DLBCL, PMBCL | nr | nr | nr | nr | nr | F 30 mg/m2 | 0.4 - 2 × 108 | 3 h |
| (Kite) | C 250 mg/m2 | |||||||||
| Tisagen-lecleucel | ALL < 26 yo, r/r DLBCL | 4 | ACD-A or ACD-A plus Heparin | ≥20 | ≥10 | ≥3 | F 25 mg/m2 | ALL: 2.5 × 108 | 30 min | |
| (Novartis) | C 250 mg/m2 | DLBCL: 0.6 - 6 × 108 | ||||||||
| T | HD-CAR-1 (Heidelberg) | r/r ALL, NHL, ped r/r ALL | nr | nr | nr | nr | nr | F 30 mg/m2 | Dose I: 1 × 106/m2 Dose II: 5 × 106/m2 Dose III: 20 × 106/m2 | 2 h |
| C 500 mg/m2 | ||||||||||
| Characteristics of All Patients | All Patients | Male | Female |
|---|---|---|---|
| n = 41 | n = 29 | n = 12 | |
| Age (years), median (range) | 56 (20–72) | 56 (20–70) | 56 (20–72) |
| Weight (kilogram), median (range) | 79 (47–147) | 82 (53–147) | 60 (47–85) |
| Height (centimeters), median (range) | 176 (150–197) | 180 (163–197) | 164 (150–171) |
| Total blood volume (L), median (range) | 5.1 (3.2–7.6) | 5.4 (3.9–7.6) | 3.6 (3.2–4.6) |
| Characteristics (Yescarta® group) | 25 Patients receiving leukapheresis | ||
| Patient gender | Male n = 19 (76%), Female n = 6 (24%) | ||
| Age (years), median (range) | 54 (20–68) | ||
| Disease | DLBCL n = 24 (96%), PMBCL n = 1 (4%) | ||
| Prior therapy lines median (range) | 5 (2–8) | ||
| Best response | CR (36%), PR (40%), SD/MR (4%), PD (8%), NE (12%) | ||
| Characteristics | Healthy Donors | Lymphoma | CLL | ALL |
|---|---|---|---|---|
| n = 30 | n = 32 | n = 2 | n = 6 | |
| Leukapheresis duration | n.a. | 239 (120–300) | 213 (180–245) | 271 (185–300) |
| (minutes), median (range) | ||||
| Processed blood volume | 10.5 (5.8–15.0) | 12.0 (5.8–15.0) | 9.5 (9.0–10.0) | 9.0 (6.4–15.0) |
| (L), median (range) | ||||
| Times TBV processed | 2.1 (1.7–3.1) | 2.5 (1.2*–3.9) | 1.6 (1.5–1.7) | 2.3 (1.3–2.7) |
| median (range) | ||||
| Neutrophil count prior | 4.0 (2.8–5.7) | 4.1 (2.1–18.7) | 3.0 (2.9–3.1) | 2.9 (1.4–3.9) |
| /nL, median (range) | ||||
| Lymphocytes count prior | 1.3 (0.7–1.6) | 0.7 (0.2–3.4) | 1.0 (0.4–1.6) | 0.4 (0.1–1.5) |
| /nL, median (range) |
| Characteristics | Healthy Donors | Lymphoma | CLL | ALL |
|---|---|---|---|---|
| n = 30 | n = 32 | n = 2 | n = 6 | |
| Total nucleated cells | 149.0 (66.4–392.7) | 100.4 (9.3–340.5) | 79.6 (78.3–80.8) | 62.5 (19.7–156.0) |
| (×108), median (range) | ||||
| Total CD3+ cell count | 72.0 (4.1–185.9) | 41.0 (4.2–231.8) | 36.7 (23.5–49.8) | 26.0 (4.0–68.0) |
| (×108), median (range) | ||||
| Volume | 176.6 (106.0–268.7) | 238.0 (136.0–310.0) | 223.0 (190.0–255.0) | 235.5 (188.0–289.0) |
| (mL), median (range) | ||||
| Hematocrit | 3.9 (1.8–7.4) | 2.6 (1.3–7.4) | 2.2 (2.1–2.2) | 2.5 (1.1–3.3) |
| (%), median (range) | ||||
| Monocytes | n.a. | 24.7 (8.1–53.8) | 27.3 (6.9–47.8) | 14.7 (6.2–33.0) |
| (%), median (range) | ||||
| Platelets | 987.0 (418.0–7551.0) | 1088.0 (147.0–3120.0) | 1004.5 (966.0–1043.0) | 615.5 (170.0–1310.0) |
| (×108), median (range) | ||||
| Viability | 99.8 (99.6–100) | 99.9 (99.6–100) | 99.8 (99.8–99.8) | 99.8 (99.6–99.9) |
| (%), median (range) |
| Number of Patients | Sex | Age | Diagnosis | Pretreatments | Disease Status before Leuka-Pheresis | Last Treatment (<12 Weeks before Leukapheresis) | Pre-Apheresis TNC in Peripheral Blood | Pre-Apheresis Lymphocyte Count | Apheresis Concentrate TNC Count | Bridging Therapy Prior CAR-T Cell Therapy | Response to CAR-T Cell Therapy |
|---|---|---|---|---|---|---|---|---|---|---|---|
| (male/female) | median (range) | median (range) | (percentage; weeks prior leukapheresis) | median (range), /nL | median (range), ×108 | median (range), ×108 | w/w/o (%) | ||||
| 25 patients (with 23 patients receiving axicabtagen ciloleucel) *,° | 76%/24% | 54 (20–68) | DLBCL (96%) PMBCL (4%) | 5 (2–8) | PR (4%), SD/MR (8%), PD (84%), NE (4%) | Ibr (4%), Rituximab (20%), R-DHAO/P (12%), R-ICE (8%), R-B (4%), Len (4%), GDP (4%), GemOx (8%), Dexa (4%), Ino (4%), Brent (8%), Pola (4%), st (4%), NT (12%) | 4.3 (2.2–18.7) | 0.6 (0.2–3.4) | 100 (9–341) | 57%/43% | CR (36%) PR (40%) SD/MR (4%) PD (8%) NE (12%) |
| Four patients receiving second apheresis * | 100%/0% | 51 (27–63) | DLBCL (100%) | 4 (2–5): R-CHOP (100%), R-DHAO/P (50%), (R-) ICE (50%), R-Pola (25%), allogeneic SCT (25%), Nivolumab (25%) | PD (100%) | First leukapheresis: P1: R-DHAP (5 wks) P2: R-DHAP (8 wks) P3: Rituximab (1 wk) P4: NT | First leukaph.: 5.8 (4.1–8.6) | First leukaph.: 0.5 (0.4–0.7) | First leukaph.: 128 (75–341) | 67%/33% bridging therapy: Ibr, R-B, Pola-BR | PR (33%) PD (33%) NE (33%) |
| Second leukapheresis: P1: R-DHAP (8 wks) P2: Dexa (2 wks) P3: Rituximab (3 wks) P4: NT | Second leukaph.: 4.3 (3.5–5.4) | Second leukaph.: 0.6 (0.4–0.9) | Second leukaph.: 104 (68–169) | ||||||||
| One patient CAR-T cell production failed * | male | 63 | DLBCL | 3: R-CHOP, R-DHAP, R-B | PD | R-DHAP (8 wks prior first leukapheresis) | First leukaph.: 8.6 | First leukaph.: 0.4 | First leukaph.: 75 | - | - |
| Dexa (2 wks prior second leukapheresis) | Second leukaph.: 4.3 | Second leukaph.: 0.9 | Second leukaph.: 86 | ||||||||
| One patient deceased prior to infusion ° | male | 52 | DLBCL | 3: R-CHOP, R-DHAP, R-ICE | PD | R-ICE (9 wks prior) | 18.7 | 2.2 | 317 | - | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korell, F.; Laier, S.; Sauer, S.; Veelken, K.; Hennemann, H.; Schubert, M.-L.; Sauer, T.; Pavel, P.; Mueller-Tidow, C.; Dreger, P.; et al. Current Challenges in Providing Good Leukapheresis Products for Manufacturing of CAR-T Cells for Patients with Relapsed/Refractory NHL or ALL. Cells 2020, 9, 1225. https://doi.org/10.3390/cells9051225
Korell F, Laier S, Sauer S, Veelken K, Hennemann H, Schubert M-L, Sauer T, Pavel P, Mueller-Tidow C, Dreger P, et al. Current Challenges in Providing Good Leukapheresis Products for Manufacturing of CAR-T Cells for Patients with Relapsed/Refractory NHL or ALL. Cells. 2020; 9(5):1225. https://doi.org/10.3390/cells9051225
Chicago/Turabian StyleKorell, Felix, Sascha Laier, Sandra Sauer, Kaya Veelken, Hannah Hennemann, Maria-Luisa Schubert, Tim Sauer, Petra Pavel, Carsten Mueller-Tidow, Peter Dreger, and et al. 2020. "Current Challenges in Providing Good Leukapheresis Products for Manufacturing of CAR-T Cells for Patients with Relapsed/Refractory NHL or ALL" Cells 9, no. 5: 1225. https://doi.org/10.3390/cells9051225