Consensus on the Application of Lung Ultrasound in Pneumonia and Bronchiolitis in Children

 ,
, 
 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Expert Panel Selection
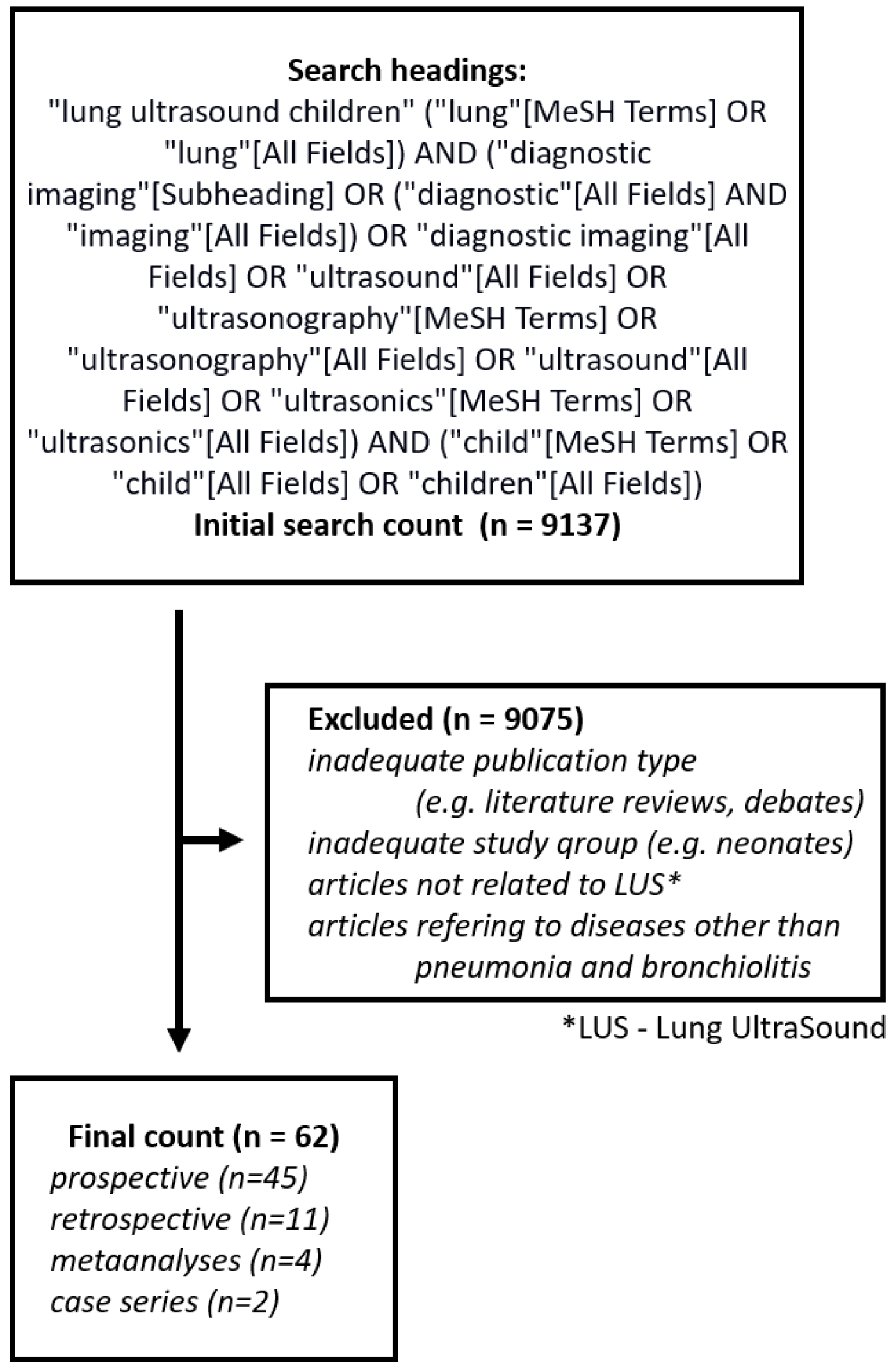
2.2. Literature Search
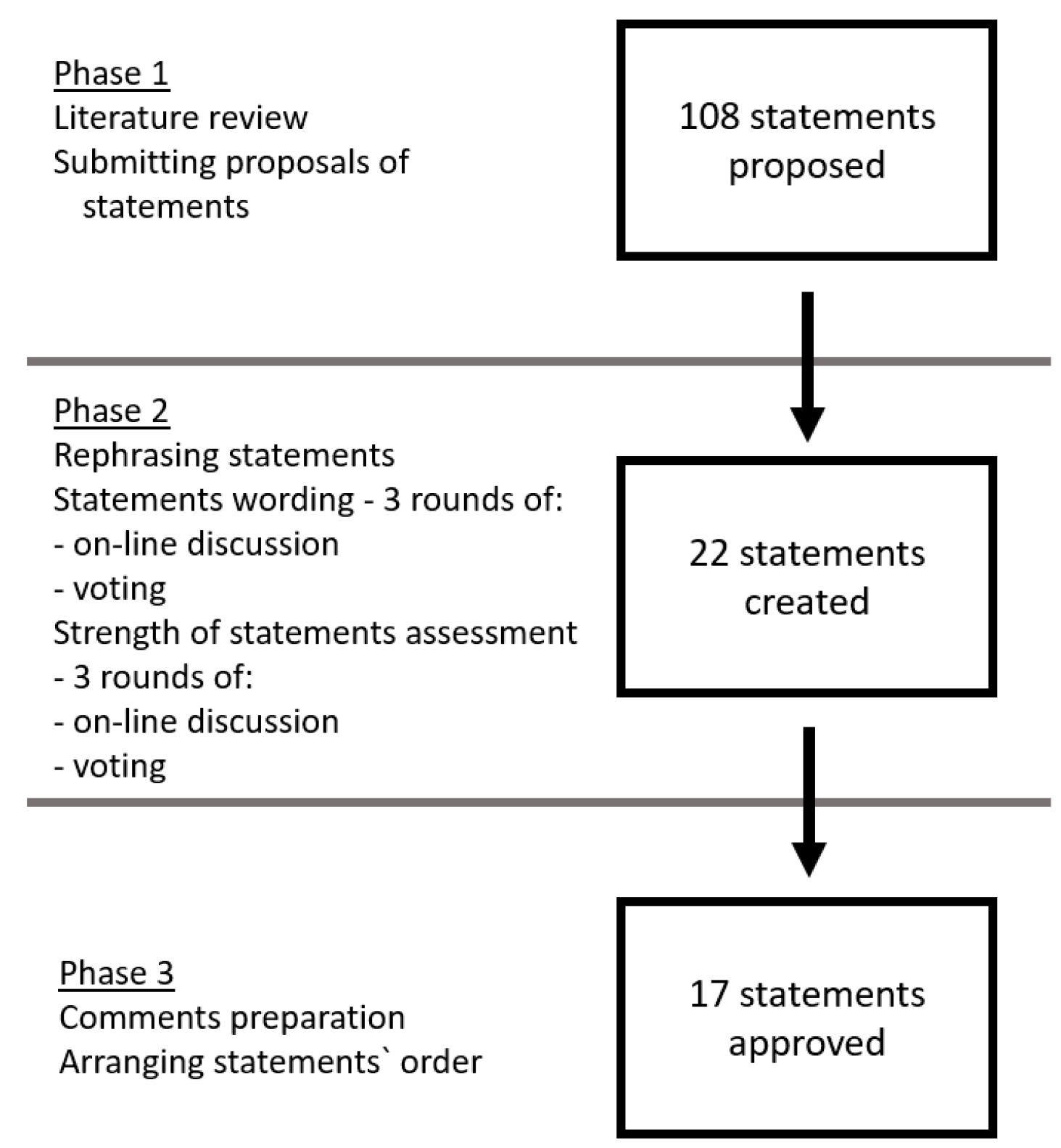
2.3. Statement Development
2.4. Strength of Statements
2.5. Comments
2.6. Statements
3. General Statements
- 1.
- A linear transducer is the most commonly used transducer for LUS examination of a suspected lower respiratory tract infection (LRTI) in children (A1) [29,30,31,32,33,34].Comments:
- a.
- b.
- The appropriate transducer must balance acquiring the best possible image quality with the maintenance of adequate ultrasound wave penetration. The examining conditions may be affected by:
- Lesion size—in case of abnormalities involving a large area of the lung parenchyma (e.g., large consolidations) or massive pleural effusion, transducers with a wide field of view;
- Deeper penetration may prove necessary [33].
- c.
- Differentiation between B-lines and other vertical artefacts (I- and Z-lines) may require the use of a convex or microconvex transducer.
- 2.
- The entire available lung surface should be examined in children with suspected LRTI (A1) [31,35,42,43,44,45,46,47].Comments:
- a.
- The recommended examination technique includes the assessment of the entire available lung surface, i.e., anterior, lateral and posterior surface of both lungs [6,16,19,23,25,28,34,42,43,44,45,48,49,50,51,52,53,54,55]. The examined area may be limited to anterior and lateral surfaces in the case of patients who are:
- Hospitalised in the intensive care unit due to the risk posed by changing their position;
- In life-threatening conditions, examined following quick-assessment protocols, such as EFAST, BLUE, PEA, RADIUS.
Should examining the entire available lung surface prove impossible (due to patients’ anxiety), such information must be included in the examination result.- b.
- c.
- d.
- Some patients may benefit from extending the examination by:
- 3.
- Diagnostic value of LUS in children with suspected LRTI to a limited extent depends on the sonographer’s experience (B1) [16,27,28,47,56,57].Comments:
- Sonographers, who are novices in diagnosing CAP, can acquire high concordance with experienced sonographers relatively quickly [56].
- 4.
- LUS has high diagnostic value in assessing the presence of fluid in pleural cavities (A1) [16,18,24,26,32,35,36,38,40,44,48,60,63,64].Comments:
- In case of small-volume fluid detection with LUS, it is crucial to evaluate the fluid’s clinical significance.
- LUS enables visualization of small-volume pleural fluid directly adjacent to the area of consolidation.
- To standardise the model result of LUS in case of pleural effusion, we suggest including the following information: the patient’s position during the examination, the precise location (including the maximal height of the fluid, its maximal depth with determining the intercostal space and body line) as well as the characteristics of the fluid.
3.1. Pneumonia
- 5.
- LUS is useful for diagnosing CAP in children (A1) [6,16,19,20,22,24,25,26,27,29,30,33,35,36,37,38,39,40,41,43,44,45,48,49,51,55,57,58,60,65,66,67,68].Comments:
- 6.
- LUS has at least equal diagnostic value to CXR in detecting CAP in children (A1) [6,16,19,26,30,35,37,39,41,44,45,48,51,55,58,60].Comments:
- Some patients will benefit from having both CXR and LUS performed, as these two imaging methods should be regarded as complementary [40].
- 7.
- Normal LUS results in children with suspected LRTI significantly reduce the probability of diagnosing CAP (A1) [16,24,25,26,33,41,49,51,55,60,67].Comments:
- Despite high sensitivity of LUS in diagnosing pneumonia, some lesions remain undetectable (false-negative result) if the lesion:
- 8.
- Consolidation is the most commonly reported LUS finding in children with pneumonia (A1) [6,20,22,24,26,29,30,32,33,35,37,39,41,42,46,51,58,60,67,69].Comments:
- Should a consolidation be detected, it is crucial to measure it in at least two, optimally three, dimensions [67].
- 9.
- Comments:
- 10.
- Assessment of the vascular pattern of the consolidation may improve the diagnostic value of LUS in children with suspected LRTI (C1) [31,36,38].Comments:
- An abnormal vascular pattern may be indicative of other aetiology of the lesions (tuberucolous, fungal or non-infectious).
- Vascular pattern assessment may be hindered in cases of examining an anxious child, small consolidations or lesions located in the pericardiac area (due to cardiac pulse).
- 11.
- Comments:
- Like other imaging techniques, LUS cannot indicate the aetiologic factor. However, regarding pathophysiology and the whole clinical picture, LUS findings can be suggestive of certain groups of pathogens. Features suggestive of viral or atypical aetiology include bilateral consolidations, which are usually smaller compared to the ones observed in bacterial pneumonia, as well as more frequent presence of B-lines forming interstitial syndromes [16,27,58].
- 12.
- Comments:
- In patients with pneumonia, LUS monitoring enables early detection of complications [38].
- It is worth performing an additional control LUS examination 1-2 months after the treatment has been completed. The knowledge of residual findings can facilitate correct interpretation of LUS, should the patient be suspected of a next episode of LRTI [21].
- 13.
- Comments:
- LUS accuracy of lung abscess detection depends mainly on localisation of the lesion.
- LUS seems to be useful in diagnosing pneumothorax in children, though it does not allow air volume assessment, and it cannot aid in the choice of the treatment method.
3.2. Bronchiolitis
- 14.
- Comments:
- 15.
- Comments:
- We suggest LUS as the first-choice method in patients with bronchiolitis who require diagnostic imaging.
- 16.
- Comments:
- 17.
- Comments:
4. Discussion and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Harris, M.; Clark, J.; Coote, N.; Fletcher, P.; Harnden, A.; McKean, M.; Thomson, A.; British Thoracic Society Standards of Care Committee. British Thoracic Society guidelines for the management of community acquired pneumonia in children: update 2011. Thorax 2011, 66 (Suppl 2), ii1–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, G.J.; Macaskill, P.; Kerr, M.; Fitzgerald, D.A.; Isaacs, D.; Codarini, M.; McCaskill, M.; Prelog, K.; Craig, J.C. Variability and accuracy in interpretation of consolidation on chest radiography for diagnosing pneumonia in children under 5 years of age. Pediatr. Pulmonol. 2013, 48, 1195–1200. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D.J.; Hall, E.J. Computed tomography—An increasing source of radiation exposure. N. Engl. J. Med. 2007, 357, 2277–2284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zar, H.J.; Andronikou, S.; Nicol, M.P. Advances in the diagnosis of pneumonia in children. BMJ 2017, 358, j2739. [Google Scholar] [CrossRef] [PubMed]
- Stadler, J.A.M.; Andronikou, S.; Zar, H.J. Lung ultrasound for the diagnosis of community-acquired pneumonia in children. Pediatr. Radiol. 2017, 47, 1412–1419. [Google Scholar] [CrossRef] [Green Version]
- Caiulo, V.A.; Gargani, L.; Caiulo, S.; Fisicaro, A.; Moramarco, F.; Latini, G.; Picano, E.; Mele, G. Lung ultrasound characteristics of community-acquired pneumonia in hospitalized children. Pediatr. Pulmonol. 2013, 48, 280–287. [Google Scholar] [CrossRef]
- Lichtenstein, D.A.; Mezière, G.A. Relevance of lung ultrasound in the diagnosis of acute respiratory failure: The BLUE protocol. Chest 2008, 134, 117–125. [Google Scholar] [CrossRef] [Green Version]
- Kirkpatrick, A.W.; Sirois, M.; Laupland, K.B.; Liu, D.; Rowan, K.; Ball, C.G.; Hameed, S.M.; Brown, R.; Simons, R.; Dulchavsky, S.A.; et al. Hand-held thoracic sonography for detecting post-traumatic pneumothoraces: The Extended Focused Assessment with Sonography for Trauma (EFAST). J. Trauma 2004, 57, 288–295. [Google Scholar] [CrossRef]
- Buda, N.; Kosiak, W.; Radzikowska, E.; Olszewski, R.; Jassem, E.; Grabczak, E.M.; Pomiecko, A.; Piotrkowski, J.; Piskunowicz, M.; Soltysiak, M.; et al. Polish recommendations for lung ultrasound in internal medicine (POLLUS-IM). J. Ultrason. 2018, 18, 198–206. [Google Scholar] [CrossRef]
- Buda, N.; Kosiak, W.; Wełnicki, M.; Skoczylas, A.; Olszewski, R.; Piotrkowski, J.; Skoczyński, S.; Radzikowska, E.; Jassem, E.; Grabczak, E.M.; et al. Recommendations for Lung Ultrasound in Internal Medicine. Diagnostics 2020, 10, 597. [Google Scholar] [CrossRef]
- Volpicelli, G.; Elbarbary, M.; Blaivas, M.; Lichtenstein, D.A.; Mathis, G.; Kirkpatrick, A.W.; Melniker, L.; Gargani, L.; Noble, V.E.; Via, G.; et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012, 38, 577–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boulkedid, R.; Abdoul, H.; Loustau, M.; Sibony, O.; Alberti, C. Using and reporting the Delphi method for selecting healthcare quality indicators: A systematic review. PLoS ONE 2011, 6, e20476. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Schünemann, H.J.; Tugwell, P.; Knottnerus, A. GRADE guidelines: A new series of articles in the Journal of Clinical Epidemiology. J. Clin. Epidemiol. 2011, 64, 380–382. [Google Scholar] [CrossRef] [PubMed]
- Willis, B.H.; Quigley, M. Uptake of newer methodological developments and the deployment of meta-analysis in diagnostic test research: A systematic review. BMC Med. Res. Methodol. 2011, 11, 27. [Google Scholar] [CrossRef] [Green Version]
- Lichtenstein, D. Novel approaches to ultrasonography of the lung and pleural space: Where are we now? Breathe (Sheff) 2017, 13, 100–111. [Google Scholar] [CrossRef] [Green Version]
- Shah, V.P.; Tunik, M.G.; Tsung, J.W. Prospective evaluation of point-of-care ultrasonography for the diagnosis of pneumonia in children and young adults. JAMA Pediatr. 2013, 167, 119–125. [Google Scholar] [CrossRef] [Green Version]
- Tripathi, S.; Ganatra, H.; Martinez, E.; Mannaa, M.; Peters, J. Accuracy and reliability of bedside thoracic ultrasound in detecting pulmonary pathology in a heterogeneous pediatric intensive care unit population. J. Clin. Ultrasound 2019, 47, 63–70. [Google Scholar] [CrossRef]
- de Souza, T.H.; Nadal, J.A.H.; Peixoto, A.O.; Pereira, R.M.; Giatti, M.P.; Soub, A.C.S.; Brandão, M.B. Lung ultrasound in children with pneumonia: interoperator agreement on specific thoracic regions. Eur. J. Pediatr. 2019, 178, 1369–1377. [Google Scholar] [CrossRef]
- Yilmaz, H.L.; Özkaya, A.K.; Sarı Gökay, S.; Tolu Kendir, Ö.; Şenol, H. Point-of-care lung ultrasound in children with community acquired pneumonia. Am. J. Emerg. Med. 2017, 35, 964–969. [Google Scholar] [CrossRef] [PubMed]
- Özkaya, A.K.; Başkan Vuralkan, F.; Ardıç, Ş. Point-of-care lung ultrasound in children with non-cardiac respiratory distress or tachypnea. Am. J. Emerg. Med. 2019, 37, 2102–2106. [Google Scholar] [CrossRef]
- Wojsyk-Banaszak, I.; Krenke, K.; Jończyk-Potoczna, K.; Ksepko, K.; Wielebska, A.; Mikoś, M.; Bręborowicz, A. Long-term sequelae after lung abscess in children—Two tertiary centers’ experience. J. Infect. Chemother. 2018, 24, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Ellington, L.E.; Gilman, R.H.; Chavez, M.A.; Pervaiz, F.; Marin-Concha, J.; Compen-Chang, P.; Riedel, S.; Rodriguez, S.J.; Gaydos, C.; Hardick, J.; et al. Lung ultrasound as a diagnostic tool for radiographically-confirmed pneumonia in low resource settings. Respir. Med. 2017, 128, 57–64. [Google Scholar] [CrossRef] [Green Version]
- Özkaya, A.K.; Yilmaz, H.L.; Kendir, Ö.; Gökay, S.S.; Eyüboğlu, İ. Lung Ultrasound Findings and Bronchiolitis Ultrasound Score for Predicting Hospital Admission in Children With Acute Bronchiolitis. Pediatr. Emerg. Care 2020, 36, e135–e142. [Google Scholar] [CrossRef]
- Man, S.C.; Fufezan, O.; Sas, V.; Schnell, C. Performance of lung ultrasonography for the diagnosis of communityacquired pneumonia in hospitalized children. Med. Ultrason. 2017, 19, 276–281. [Google Scholar] [CrossRef] [Green Version]
- Lissaman, C.; Kanjanauptom, P.; Ong, C.; Tessaro, M.; Long, E.; O’Brien, A. Prospective observational study of point-of-care ultrasound for diagnosing pneumonia. Arch. Dis. Child. 2019, 104, 12–18. [Google Scholar] [CrossRef]
- Reali, F.; Sferrazza Papa, G.F.; Carlucci, P.; Fracasso, P.; Di Marco, F.; Mandelli, M.; Soldi, S.; Riva, E.; Centanni, S. Can lung ultrasound replace chest radiography for the diagnosis of pneumonia in hospitalized children? Respiration 2014, 88, 112–115. [Google Scholar] [CrossRef]
- Tsung, J.W.; Kessler, D.O.; Shah, V.P. Prospective application of clinician-performed lung ultrasonography during the 2009 H1N1 influenza A pandemic: Distinguishing viral from bacterial pneumonia. Crit. Ultrasound. J. 2012, 4, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biagi, C.; Pierantoni, L.; Baldazzi, M.; Greco, L.; Dormi, A.; Dondi, A.; Faldella, G.; Lanari, M. Lung ultrasound for the diagnosis of pneumonia in children with acute bronchiolitis. BMC Pulm. Med. 2018, 18, 191. [Google Scholar] [CrossRef] [Green Version]
- Pereda, M.A.; Chavez, M.A.; Hooper-Miele, C.C.; Gilman, R.H.; Steinhoff, M.C.; Ellington, L.E.; Gross, M.; Price, C.; Tielsch, J.M.; Checkley, W. Lung ultrasound for the diagnosis of pneumonia in children: A meta-analysis. Pediatrics 2015, 135, 714–722. [Google Scholar] [CrossRef] [Green Version]
- Balk, D.S.; Lee, C.; Schafer, J.; Welwarth, J.; Hardin, J.; Novack, V.; Yarza, S.; Hoffmann, B. Lung ultrasound compared to chest X-ray for diagnosis of pediatric pneumonia: A meta-analysis. Pediatr. Pulmonol. 2018, 53, 1130–1139. [Google Scholar] [CrossRef]
- Lai, S.H.; Wong, K.S.; Liao, S.L. Value of Lung Ultrasonography in the Diagnosis and Outcome Prediction of Pediatric Community-Acquired Pneumonia with Necrotizing Change. PLoS ONE 2015, 10, e0130082. [Google Scholar] [CrossRef]
- Guerra, M.; Crichiutti, G.; Pecile, P.; Romanello, C.; Busolini, E.; Valent, F.; Rosolen, A. Ultrasound detection of pneumonia in febrile children with respiratory distress: A prospective study. Eur J. Pediatr. 2016, 175, 163–170. [Google Scholar] [CrossRef]
- Claes, A.S.; Clapuyt, P.; Menten, R.; Michoux, N.; Dumitriu, D. Performance of chest ultrasound in pediatric pneumonia. Eur. J. Radiol. 2017, 88, 82–87. [Google Scholar] [CrossRef] [Green Version]
- Varshney, T.; Mok, E.; Shapiro, A.J.; Li, P.; Dubrovsky, A.S. Point-of-care lung ultrasound in young children with respiratory tract infections and wheeze. Emerg. Med. J. 2016, 33, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Iuri, D.; De Candia, A.; Bazzocchi, M. Evaluation of the lung in children with suspected pneumonia: Usefulness of ultrasonography. Radiol. Med. 2009, 114, 321–330. [Google Scholar] [CrossRef]
- Kurian, J.; Levin, T.L.; Han, B.K.; Taragin, B.H.; Weinstein, S. Comparison of ultrasound and CT in the evaluation of pneumonia complicated by parapneumonic effusion in children. Am. J. Roentgenol. 2009, 193, 1648–1654. [Google Scholar] [CrossRef] [Green Version]
- Ho, M.C.; Ker, C.R.; Hsu, J.H.; Wu, J.R.; Dai, Z.K.; Chen, I.C. Usefulness of lung ultrasound in the diagnosis of community-acquired pneumonia in children. Pediatr. Neonatol. 2015, 56, 40–45. [Google Scholar] [CrossRef] [Green Version]
- Ianniello, S.; Piccolo, C.L.; Buquicchio, G.L.; Trinci, M.; Miele, V. First-line diagnosis of paediatric pneumonia in emergency: Lung ultrasound (LUS) in addition to chest-X-ray (CXR) and its role in follow-up. Br. J. Radiol. 2016, 89, 20150998. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Song, W.; Wang, Y.; Han, J.; Lv, K. Lung ultrasonography versus chest radiography for the diagnosis of pediatric community acquired pneumonia in emergency department: A meta-analysis. J. Thorac. Dis. 2019, 11, 5107–5114. [Google Scholar] [CrossRef] [PubMed]
- Hajalioghli, P.; Nemati, M.; Dinparast Saleh, L.; Fouladi, D.F. Can Chest Computed Tomography Be Replaced by Lung Ultrasonography With or Without Plain Chest Radiography in Pediatric Pneumonia? J. Thorac. Imaging 2016, 31, 247–252. [Google Scholar] [CrossRef]
- Boursiani, C.; Tsolia, M.; Koumanidou, C.; Malagari, A.; Vakaki, M.; Karapostolakis, G.; Mazioti, A.; Alexopoulou, E. Lung Ultrasound as First-Line Examination for the Diagnosis of Community-Acquired Pneumonia in Children. Pediatr. Emerg. Care 2017, 33, 62–66. [Google Scholar] [CrossRef]
- Berce, V.; Tomazin, M.; Gorenjak, M.; Berce, T.; Lovrenčič, B. The Usefulness of Lung Ultrasound for the Aetiological Diagnosis of Community-Acquired Pneumonia in Children. Sci. Rep. 2019, 9, 17957. [Google Scholar] [CrossRef]
- Milliner, B.H.A.; Tsung, J.W. Lung Consolidation Locations for Optimal Lung Ultrasound Scanning in Diagnosing Pediatric Pneumonia. J. Ultrasound Med. 2017, 36, 2325–2328. [Google Scholar] [CrossRef] [Green Version]
- Iorio, G.; Capasso, M.; Prisco, S.; De Luca, G.; Mancusi, C.; Laganà, B.; Piscopo, M.A.; Comune, V. Lung Ultrasound Findings Undetectable by Chest Radiography in Children with Community-Acquired Pneumonia. Ultrasound. Med. Biol. 2018, 44, 1687–1693. [Google Scholar] [CrossRef]
- Copetti, R.; Cattarossi, L. Ultrasound diagnosis of pneumonia in children. Radiol. Med. 2008, 113, 190–198. [Google Scholar] [CrossRef]
- Lovrenski, J.; Petrović, S.; Balj-Barbir, S.; Jokić, R.; Vilotijević-Dautović, G. Stethoscope vs. ultrasound probe—Which is more reliable in children with suspected pneumonia? Acta Med. Acad. 2016, 45, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Heuvelings, C.C.; Belard, S.; Andronikou, S.; Jamieson-Luff, N.; Grobusch, M.P.; Zar, H.J. Chest ultrasound findings in children with suspected pulmonary tuberculosis. Pediatr. Pulmonol. 2019, 54, 463–470. [Google Scholar] [CrossRef]
- Esposito, S.; Papa, S.S.; Borzani, I.; Pinzani, R.; Giannitto, C.; Consonni, D.; Principi, N. Performance of lung ultrasonography in children with community-acquired pneumonia. Ital. J. Pediatr 2014, 40, 37. [Google Scholar] [CrossRef] [Green Version]
- Samson, F.; Gorostiza, I.; González, A.; Landa, M.; Ruiz, L.; Grau, M. Prospective evaluation of clinical lung ultrasonography in the diagnosis of community-acquired pneumonia in a pediatric emergency department. Eur J. Emerg. Med. 2018, 25, 65–70. [Google Scholar] [CrossRef]
- Zhan, C.; Grundtvig, N.; Klug, B.H. Performance of Bedside Lung Ultrasound by a Pediatric Resident: A Useful Diagnostic Tool in Children With Suspected Pneumonia. Pediatr. Emerg. Care 2018, 34, 618–622. [Google Scholar] [CrossRef]
- Omran, A.; Eesai, S.; Ibrahim, M.; El-Sharkawy, S. Lung ultrasound in diagnosis and follow up of community acquired pneumonia in infants younger than 1-year old. Clin. Respir. J. 2018, 12, 2204–2211. [Google Scholar] [CrossRef]
- Supino, M.C.; Buonsenso, D.; Scateni, S.; Scialanga, B.; Mesturino, M.A.; Bock, C.; Chiaretti, A.; Giglioni, E.; Reale, A.; Musolino, A.M. Point-of-care lung ultrasound in infants with bronchiolitis in the pediatric emergency department: A prospective study. Eur. J. Pediatr. 2019, 178, 623–632. [Google Scholar] [CrossRef]
- Bueno-Campaña, M.; Sainz, T.; Alba, M.; Del Rosal, T.; Mendez-Echevarría, A.; Echevarria, R.; Tagarro, A.; Ruperez-Lucas, M.; Herrreros, M.L.; Latorre, L.; et al. Lung ultrasound for prediction of respiratory support in infants with acute bronchiolitis: A cohort study. Pediatr. Pulmonol. 2019, 54, 873–880. [Google Scholar] [CrossRef]
- Basile, V.; Di Mauro, A.; Scalini, E.; Comes, P.; Lofù, I.; Mostert, M.; Tafuri, S.; Manzionna, M.M. Lung ultrasound: A useful tool in diagnosis and management of bronchiolitis. BMC Pediatr. 2015, 15, 63. [Google Scholar] [CrossRef] [Green Version]
- Iorio, G.; Capasso, M.; De Luca, G.; Prisco, S.; Mancusi, C.; Laganà, B.; Comune, V. Lung ultrasound in the diagnosis of pneumonia in children: Proposal for a new diagnostic algorithm. PeerJ 2015, 3, e1374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pervaiz, F.; Hossen, S.; Chavez, M.A.; Miele, C.H.; Moulton, L.H.; McCollum, E.D.; Roy, A.D.; Chowdhury, N.H.; Ahmed, S.; Begum, N.; et al. Training and standardization of general practitioners in the use of lung ultrasound for the diagnosis of pediatric pneumonia. Pediatr. Pulmonol. 2019, 54, 1753–1759. [Google Scholar] [CrossRef] [Green Version]
- Musolino, A.M.; Tomà, P.; Supino, M.C.; Scialanga, B.; Mesturino, A.; Scateni, S.; Battaglia, M.; Pirozzi, N.; Bock, C.; Buonsenso, D. Lung ultrasound features of children with complicated and noncomplicated community acquired pneumonia: A prospective study. Pediatr. Pulmonol. 2019, 54, 1479–1486. [Google Scholar] [CrossRef]
- Jones, B.P.; Tay, E.T.; Elikashvili, I.; Sanders, J.E.; Paul, A.Z.; Nelson, B.P.; Spina, L.A.; Tsung, J.W. Feasibility and Safety of Substituting Lung Ultrasonography for Chest Radiography When Diagnosing Pneumonia in Children: A Randomized Controlled Trial. Chest 2016, 150, 131–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chavez, M.A.; Naithani, N.; Gilman, R.H.; Tielsch, J.M.; Khatry, S.; Ellington, L.E.; Miranda, J.J.; Gurung, G.; Rodriguez, S.; Checkley, W. Agreement Between the World Health Organization Algorithm and Lung Consolidation Identified Using Point-of-Care Ultrasound for the Diagnosis of Childhood Pneumonia by General Practitioners. Lung 2015, 193, 531–538. [Google Scholar] [CrossRef]
- Yadav, K.K.; Awasthi, S.; Parihar, A. Lung Ultrasound is Comparable with Chest Roentgenogram for Diagnosis of Community-Acquired Pneumonia in Hospitalised Children. Indian J. Pediatr. 2017, 84, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Nadimpalli, A.; Tsung, J.W.; Sanchez, R.; Shah, S.; Zelikova, E.; Umphrey, L.; Hurtado, N.; Gonzalez, A.; Teicher, C. Feasibility of Training Clinical Officers in Point-of-Care Ultrasound for Pediatric Respiratory Diseases in Aweil, South Sudan. Am. J. Trop. Med. Hyg. 2019, 101, 689–695. [Google Scholar] [CrossRef]
- Gravel, C.A.; Monuteaux, M.C.; Levy, J.A.; Miller, A.F.; Vieira, R.L.; Bachur, R.G. Interrater reliability of pediatric point-of-care lung ultrasound findings. Am. J. Emerg. Med. 2020, 38, 1–6. [Google Scholar] [CrossRef]
- Jaszczołt, S.; Polewczyk, T.; Dołęga-Kozierowska, M.; Woźniak, M.; Doniec, Z. Comparison of lung ultrasound and chest X-ray findings in children with bronchiolitis. J. Ultrason. 2018, 18, 193–197. [Google Scholar] [CrossRef]
- Caiulo, V.A.; Gargani, L.; Caiulo, S.; Fisicaro, A.; Moramarco, F.; Latini, G.; Picano, E. Lung ultrasound in bronchiolitis: Comparison with chest X-ray. Eur. J. Pediatr. 2011, 170, 1427–1433. [Google Scholar] [CrossRef] [PubMed]
- Ambroggio, L.; Sucharew, H.; Rattan, M.S.; O’Hara, S.M.; Babcock, D.S.; Clohessy, C.; Steinhoff, M.C.; Macaluso, M.; Shah, S.S.; Coley, B.D. Lung Ultrasonography: A Viable Alternative to Chest Radiography in Children with Suspected Pneumonia? J. Pediatr. 2016, 176, 93–98.e97. [Google Scholar] [CrossRef]
- Harel-Sterling, M.; Diallo, M.; Santhirakumaran, S.; Maxim, T.; Tessaro, M. Emergency Department Resource Use in Pediatric Pneumonia: Point-of-Care Lung Ultrasonography versus Chest Radiography. J. Ultrasound Med. 2019, 38, 407–414. [Google Scholar] [CrossRef] [Green Version]
- Urbankowska, E.; Krenke, K.; Drobczyński, Ł.; Korczyński, P.; Urbankowski, T.; Krawiec, M.; Kraj, G.; Brzewski, M.; Kulus, M. Lung ultrasound in the diagnosis and monitoring of community acquired pneumonia in children. Respir. Med. 2015, 109, 1207–1212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenahan, J.L.; Volpicelli, G.; Lamorte, A.; Jehan, F.; Bassat, Q.; Ginsburg, A.S. Multicentre pilot study evaluation of lung ultrasound for the management of paediatric pneumonia in low-resource settings: A study protocol. BMJ Open Respir. Res. 2018, 5, e000340. [Google Scholar] [CrossRef] [Green Version]
- Orso, D.; Ban, A.; Guglielmo, N. Lung ultrasound in diagnosing pneumonia in childhood: A systematic review and meta-analysis. J. Ultrasound 2018, 21, 183–195. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Musolino, A.M.; Gatto, A.; Lazzareschi, I.; Curatola, A.; Valentini, P. Lung ultrasound in infants with bronchiolitis. BMC Pulm. Med. 2019, 19, 159. [Google Scholar] [CrossRef]
- Buonsenso, D.; Brancato, F.; Valentini, P.; Curatola, A.; Supino, M.; Musolino, A.M. The Use of Lung Ultrasound to Monitor the Antibiotic Response of Community-Acquired Pneumonia in Children: A Preliminary Hypothesis. J. Ultrasound Med. 2020, 39, 817–826. [Google Scholar] [CrossRef]
- Ricci, V.; Delgado Nunes, V.; Murphy, M.S.; Cunningham, S.; The Guideline Development Group and Technical Team. Bronchiolitis in children: Summary of NICE guidance. BMJ 2015, 350, h2305. [Google Scholar] [CrossRef]
- Silver, A.H.; Nazif, J.M. Bronchiolitis. Pediatr. Rev. 2019, 40, 568–576. [Google Scholar] [CrossRef]
- Cohen, J.S.; Hughes, N.; Tat, S.; Chamberlain, J.M.; Teach, S.J.; Boniface, K. The Utility of Bedside Lung Ultrasound Findings in Bronchiolitis. Pediatr. Emerg. Care 2017, 33, 97–100. [Google Scholar] [CrossRef]
- Correa, M.; Zimic, M.; Barrientos, F.; Barrientos, R.; Román-Gonzalez, A.; Pajuelo, M.J.; Anticona, C.; Mayta, H.; Alva, A.; Solis-Vasquez, L.; et al. Automatic classification of pediatric pneumonia based on lung ultrasound pattern recognition. PLoS ONE 2018, 13, e0206410. [Google Scholar] [CrossRef]
- Cisneros-Velarde, P.; Correa, M.; Mayta, H.; Anticona, C.; Pajuelo, M.; Oberhelman, R.; Checkley, W.; Gilman, R.H.; Figueroa, D.; Zimic, M.; et al. Automatic pneumonia detection based on ultrasound video analysis. Conf Proc. IEEE Eng. Med. Biol Soc. 2016, 2016, 4117–4120. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Experts’ Opinion | % Positive Votes |
|---|---|
| Agreed for—1 | ≥80% |
| Agreed against—2 | ≤50% |
| Indeterminate—rejected | 51–79% |
| Level of Evidence | Criteria for Quality of Evidence |
|---|---|
| A (high) | Data come from many meta-analyses, and/or it is unlikely that further research will change the credibility of effectiveness or accuracy of the method. |
| B (moderate) | Data come from individual large non-randomized trials (meta-analysis, prospective cohort study), and/or further testing may have a significant impact on the credibility of effectiveness or accuracy of the method. |
| C (low or very low) | Agreed expert opinion and/or data from small studies, retrospective studies, registers, case series, or case reports, and/or it is very likely that further testing will have an important impact on the credibility of effectiveness or accuracy of the method. Very low in case any estimation of the effects or accuracy of the method is very uncertain. |
| Expert’s Opinion | Level of Evidence | Strength of Statement | Strength of Statement—Practical Implications |
|---|---|---|---|
| 1 | A | A1 | Strong statement; the given statement should be widely followed, as long as there are no major obstacles. |
| 1 | B | B1 | Strong statement, but with less degree of certainty; probably right in most individual cases. |
| 1 | C | C1 | The average (moderate) strength of statement; the statement may change after obtaining more reliable data; probably right. |
| 2 | A | A2 | The average (moderate) strength of statement; the decision on its adoption is a matter of choice and may depend on local and individual conditions; intervention does not have to be used. |
| 2 | B | B2 | Weak statement; alternative conduct can be just as good or better. |
| 2 | C | C2 | Weak statement; alternative conduct is probably equally acceptable. |
| LUS Finding | Definition |
|---|---|
| A-lines (A-line artefacts) | Repetition of the pleural line at a standardized distance equal to the skin–pleural line distance. |
| B-lines (B-line artefacts) | Comet-tail artefacts that arise from the pleural line and move simultaneously with the breathing cycle. The other optional 4 criteria are: screen-long, well-defined, erasing A-lines, and hyperechoic. |
| Consolidation | Hypoechoic, subpleural tissue-like area, caused by fluid displacing alveolar air. In case of a large consolidation, the appearance is characteristically liver-like. Usually, a consolidation has blurred margins and the following associated features:
|
| I-lines, Z-lines (I- and Z-line artefacts) | Short vertical hyperechoic artefacts arising from the pleural line, not reaching the distal edge of the screen. |
| Interstitial syndrome | ≥3 B-lines visible in the longitudinal plane between two ribs. |
| Strength of Statement * | Statement | |
|---|---|---|
| A1 | 1. | A linear transducer is the most commonly used transducer for LUS examination of a suspected lower respiratory tract infection (LRTI) in children. |
| 2. | The entire available lung surface should be examined in children with suspected LRTI. | |
| 4. | LUS has high diagnostic value in assessing the presence of fluid in pleural cavities. | |
| 5. | LUS is useful for diagnosing community-acquired pneumonia (CAP) in children. | |
| 6. | LUS has at least equal diagnostic value to chest X-ray (CXR) in detecting CAP in children. | |
| 7. | Normal LUS results in children with suspected LRTI significantly reduce the probability of diagnosing CAP. | |
| 8. | Consolidation is the most commonly reported LUS finding in children with pneumonia. | |
| 9. | LUS is more sensitive in detecting consolidations than CXR. | |
| B1 | 3. | Diagnostic value of LUS in children with suspected LRTI to a limited extent depends on the sonographer’s experience. |
| 12. | LUS is useful in monitoring the course of pneumonia in children. | |
| 13. | LUS is useful in diagnosing complications of pneumonia in children. | |
| 14. | LUS is useful in bronchiolitis diagnosis. | |
| 16. | LUS is useful in assessing the severity of bronchiolitis. | |
| C1 | 10. | Assessment of the vascular pattern of the consolidation may improve the diagnostic value of LUS in children with suspected LRTI. |
| 11. | LUS does not determine the aetiology of CAP in children. | |
| 15. | LUS has a diagnostic value equal or greater than CXR in bronchiolitis diagnosis. | |
| 17. | LUS is useful in monitoring patients with bronchiolitis. | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jaworska, J.; Komorowska-Piotrowska, A.; Pomiećko, A.; Wiśniewski, J.; Woźniak, M.; Littwin, B.; Kryger, M.; Kwaśniewicz, P.; Szczyrski, J.; Kulińska-Szukalska, K.; et al. Consensus on the Application of Lung Ultrasound in Pneumonia and Bronchiolitis in Children. Diagnostics 2020, 10, 935. https://doi.org/10.3390/diagnostics10110935
Jaworska J, Komorowska-Piotrowska A, Pomiećko A, Wiśniewski J, Woźniak M, Littwin B, Kryger M, Kwaśniewicz P, Szczyrski J, Kulińska-Szukalska K, et al. Consensus on the Application of Lung Ultrasound in Pneumonia and Bronchiolitis in Children. Diagnostics. 2020; 10(11):935. https://doi.org/10.3390/diagnostics10110935
Chicago/Turabian StyleJaworska, Joanna, Anna Komorowska-Piotrowska, Andrzej Pomiećko, Jakub Wiśniewski, Mariusz Woźniak, Błażej Littwin, Magdalena Kryger, Piotr Kwaśniewicz, Józef Szczyrski, Katarzyna Kulińska-Szukalska, and et al. 2020. "Consensus on the Application of Lung Ultrasound in Pneumonia and Bronchiolitis in Children" Diagnostics 10, no. 11: 935. https://doi.org/10.3390/diagnostics10110935