
Seroprevalence of Anti-SARS-CoV-2 IgG and IgM among Adults over 65 Years Old in the South of Italy

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results and Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Faculty Opinions recommendation of Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. Fac. Opin. Post-Publ. Peer Rev. Biomed. Lit. 2020, 382, 1199–1207. [Google Scholar] [CrossRef]
- ISTAT-ISS. Rapporto Sulla Mortalità Della Popolazione Residente a Cura di ISS e ISTAT. 2020. Available online: https://www.istat.it/it/files//2020/07/Rapp_Istat_Iss_9luglio.pdf (accessed on 3 March 2021).
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. 2020. Available online: https://covid19.who.int/ (accessed on 3 March 2021).
- WHO. Population-Based Age-Stratified Seroepidemiological Investigation Protocol for COVID-19 Virus Infection. 2020. Available online: https://apps.who.int/iris/handle/10665/331656 (accessed on 3 March 2021).
- Salje, H.; Tran Kiem, C.; Lefrancq, N.; Courtejoie, N.; Bosetti, P.; Paireau, J.; Andronico, A.; Hozé, N.; Richet, J.; Dubost, C.L.; et al. Estimating the burden of SARS-CoV-2 in France. Science 2020, 369, 208–211. [Google Scholar] [CrossRef] [PubMed]
- Kalish, H.; Klumpp-Thomas, C.; Hunsberger, S.; Baus, H.A.; Fay, M.P.; Siripong, N.; Wang, J.; Hicks, J.; Mehalko, J.; Travers, J.; et al. Mapping a Pandemic: SARS-CoV-2 Seropositivity in the United States. medRxiv 2021. [CrossRef]
- Vena, A.; Berruti, M.; Adessi, A.; Blumetti, P.; Brignole, M.; Colognato, R.; Gaggioli, G.; Giacobbe, D.R.; Bracci-Laudiero, L.; Magnasco, L.; et al. Prevalence of Antibodies to SARS-CoV-2 in Italian Adults and Associated Risk Factors. J. Clin. Med. 2020, 9, 2780. [Google Scholar] [CrossRef] [PubMed]
- Lastrucci, V.; Lorini, C.; Del Riccio, M.; Gori, E.; Chiesi, F.; Sartor, G.; Zanella, B.; Boccalini, S.; Bechini, A.; Puggelli, F.; et al. SARS-CoV-2 Seroprevalence Survey in People Involved in Different Essential Activities during the General Lock-Down Phase in the Province of Prato (Tuscany, Italy). Vaccines 2020, 8, 778. [Google Scholar] [CrossRef] [PubMed]
- Pagani, G.; Conti, F.; Giacomelli, A.; Bernacchia, D.; Rondanin, R.; Prina, A.; Scolari, V.; Gandolfi, C.E.; Castaldi, S.; Marano, G.; et al. Seroprevalence of SARS-CoV-2 significantly varies with age: Preliminary results from a mass population screening. J. Infect. 2020, 81, e10–e12. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Valentini, P.; De Rose, C.; Pata, D.; Sinatti, D.; Speziale, D.; Ricci, R.; Carfì, A.; Landi, F.; Ferrari, V.; et al. Gemelli Against COVID-19 Post-Acute Care Study Group. Seroprevalence of anti-SARS-CoV-2 IgG antibodies in children with household exposure to adults with COVID-19: Preliminary findings. Pediatr. Pulmonol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Polvere, I.; Voccola, S.; Cardinale, G.; Fumi, M.; Aquila, F.; Parrella, A.; Madera, J.R.; Stilo, R.; Vito, P.j.; Zotti, T. A peptide-based assay discriminates individual antibody response to SARS-CoV-2. Genes Dis. 2021. [CrossRef]
- ISTAT-ISS. Primi Risultati Dell’Indagine di Siero Prevalenza Sul SARS-CoV-2. 2020. Available online: https://www.istat.it/it/files/2020/08/ReportPrimiRisultatiIndagineSiero.pdf (accessed on 3 March 2021).
- Baccini, M.; Mattei, A.; Rocco, E.; Vannucci, G.; Mealli, F. Evaluating a SARS-CoV-2 screening strategy based on serological tests. Epidemiol. Prev. 2020, 44, 193–199. [Google Scholar] [PubMed]
- Wajnberg, A.; Amanat, F.; Firpo, A.; Altman, D.R.; Bailey, M.J.; Mansour, M.; McMahon, M.; Meade, P.; Mendu, D.R.; Muellers, K.; et al. Robust neutralizing antibodies to SARS-CoV-2 infection persist for months. Science 2020, 370, 1227–1230. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Du, L. SARS-CoV-2 spike protein: A key target for eliciting persistent neutralizing antibodies. Signal Transduct. Target. Ther. 2021, 6, 95. [Google Scholar] [CrossRef] [PubMed]
- Shrotri, M.; van Schalkwyk, M.C.I.; Post, N.; Eddy, D.; Huntley, C.; Leeman, D.; Rigby, S.; Williams, S.V.; Bermingham, W.H.; Kellam, P.; et al. T cell response to SARS-CoV-2 infection in humans: A systematic review. PLoS ONE 2021, 16, e0245532. [Google Scholar] [CrossRef] [PubMed]
- Poland, G.A.; Ovsyannikova, I.G.; Kennedy, R.B. SARS-CoV-2 immunity: Review and applications to phase 3 vaccine candidates. Lancet 2020, 396, 1595–1606. [Google Scholar] [CrossRef]
- Gallais, F.; Velay, A.; Nazon, C.; Wendling, M.J.; Partisani, M.; Sibilia, J.; Candon, S.; Fafi-Kremer, S. Intrafamilial Exposure to SARS-CoV-2 Associated with Cellular Immune Response without Seroconversion, France. Emerg. Infect. Dis. 2021, 27, 113–121. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| n = 1383 | (%) | ||
|---|---|---|---|
| Age Groups | |||
| Females | |||
| 65–69 | 120 | 18.8 | |
| 70–74 | 269 | 42.0 | |
| 75–79 | 155 | 24.2 | |
| 80-84 | 73 | 11.4 | |
| 85 and over | 23 | 3.6 | |
| Total: | 640 | ||
| Males | |||
| 65–69 | 100 | 13.5 | |
| 70–74 | 324 | 43.6 | |
| 75–79 | 188 | 25.3 | |
| 80–84 | 95 | 12.8 | |
| 85 and over | 36 | 4.8 | |
| Total: | 743 | ||
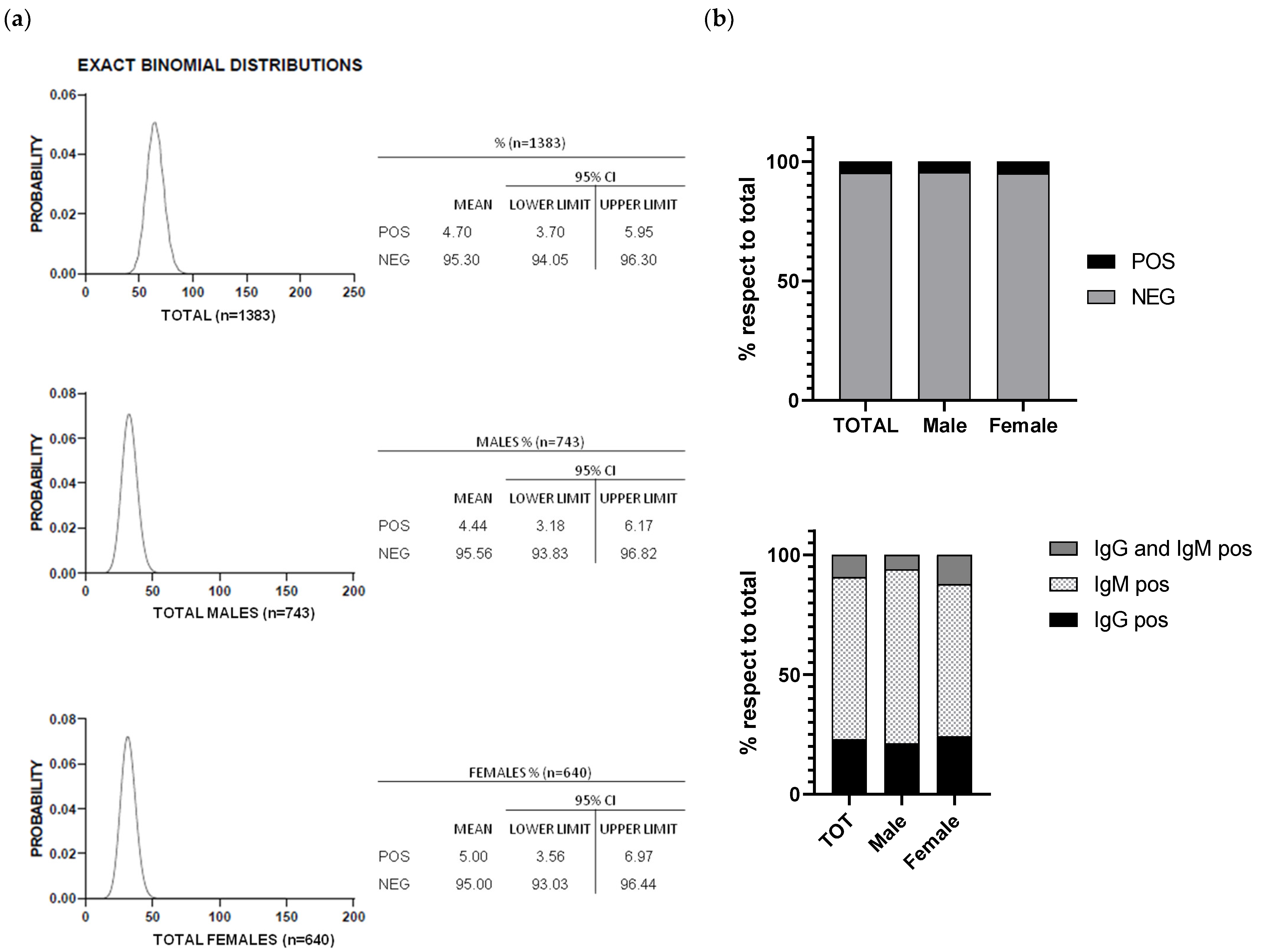
| TOTAL | MALES | FEMALES | |||||||
|---|---|---|---|---|---|---|---|---|---|
| AGE GROUPS | POS | NEG | % POS/AGE GROUP | POS | NEG | % POS/AGE GROUP | POS | NEG | % POS/AGE GROUP |
| 65–69 | 10 | 210 | 4.55 | 7 | 93 | 7.00 | 3 | 117 | 2.50 |
| 70–74 | 25 | 568 | 4.22 | 12 | 312 | 3.70 | 13 | 256 | 4.83 |
| 75–79 | 19 | 324 | 5.54 | 8 | 180 | 4.26 | 11 | 144 | 7.10 |
| 80–84 | 9 | 159 | 5.36 | 5 | 90 | 5.26 | 4 | 69 | 5.48 |
| ≥85 | 2 | 57 | 3.39 | 1 | 35 | 2.78 | 1 | 22 | 4.35 |
| TOTAL | 65 | 1318 | 4.70 | 33 | 710 | 4.44 | 32 | 608 | 5.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polvere, I.; Parrella, A.; Casamassa, G.; D’Andrea, S.; Tizzano, A.; Cardinale, G.; Voccola, S.; Porcaro, P.; Stilo, R.; Vito, P.; et al. Seroprevalence of Anti-SARS-CoV-2 IgG and IgM among Adults over 65 Years Old in the South of Italy. Diagnostics 2021, 11, 483. https://doi.org/10.3390/diagnostics11030483
Polvere I, Parrella A, Casamassa G, D’Andrea S, Tizzano A, Cardinale G, Voccola S, Porcaro P, Stilo R, Vito P, et al. Seroprevalence of Anti-SARS-CoV-2 IgG and IgM among Adults over 65 Years Old in the South of Italy. Diagnostics. 2021; 11(3):483. https://doi.org/10.3390/diagnostics11030483
Chicago/Turabian StylePolvere, Immacolata, Alfredina Parrella, Giovanna Casamassa, Silvia D’Andrea, Annamaria Tizzano, Gaetano Cardinale, Serena Voccola, Piercarmine Porcaro, Romania Stilo, Pasquale Vito, and et al. 2021. "Seroprevalence of Anti-SARS-CoV-2 IgG and IgM among Adults over 65 Years Old in the South of Italy" Diagnostics 11, no. 3: 483. https://doi.org/10.3390/diagnostics11030483