
Analyzing the Effectiveness of COVID-19 Lockdown Policies Using the Time-Dependent Reproduction Number and the Regression Discontinuity Framework: Comparison between Countries †

Abstract
:1. Introduction
2. Data and Methods
2.1. Data Sources
2.2. Epidemics and Regression Discontinuity in Time (RDiT) Model
3. Results
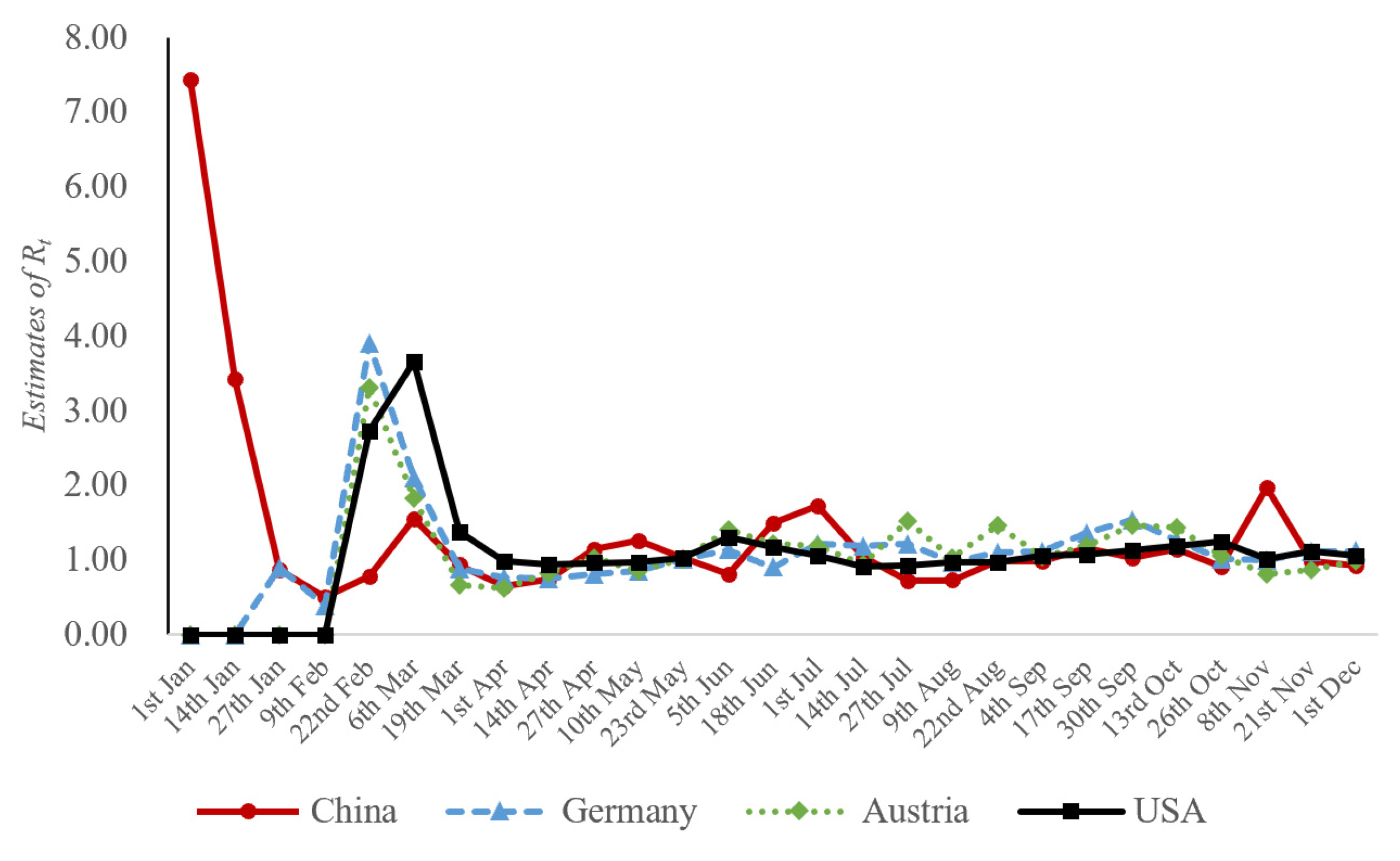
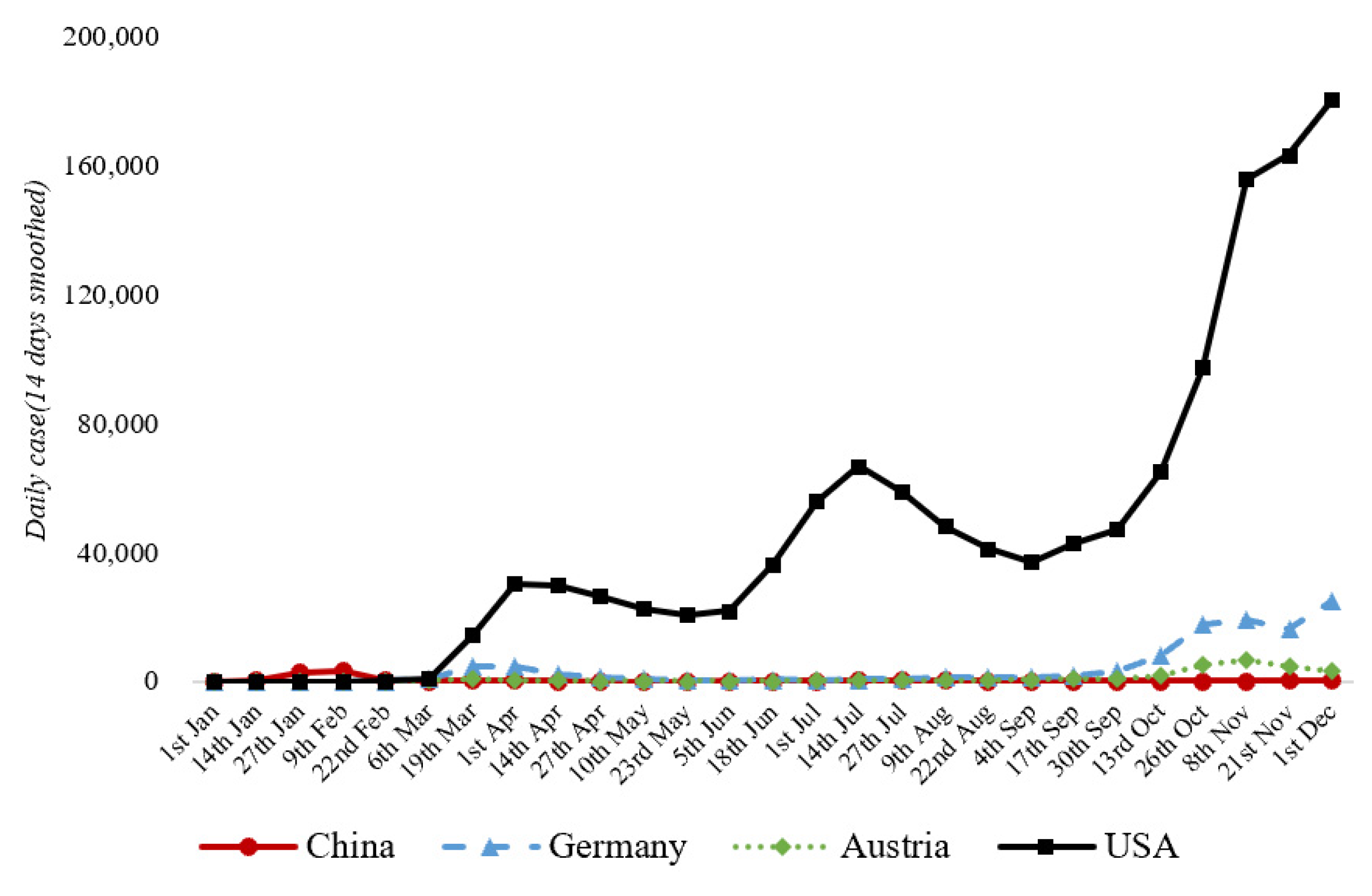
3.1. Estimates of Rt
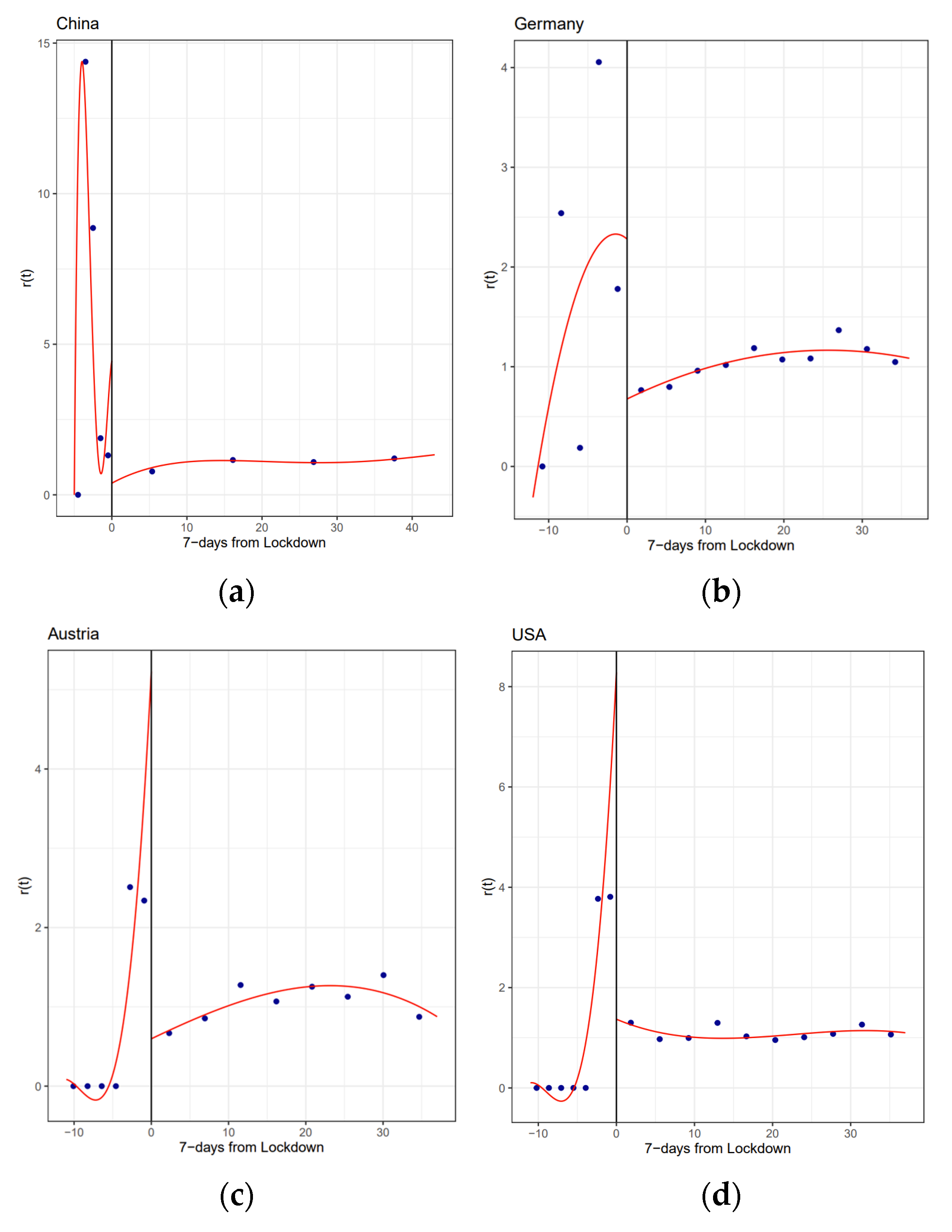
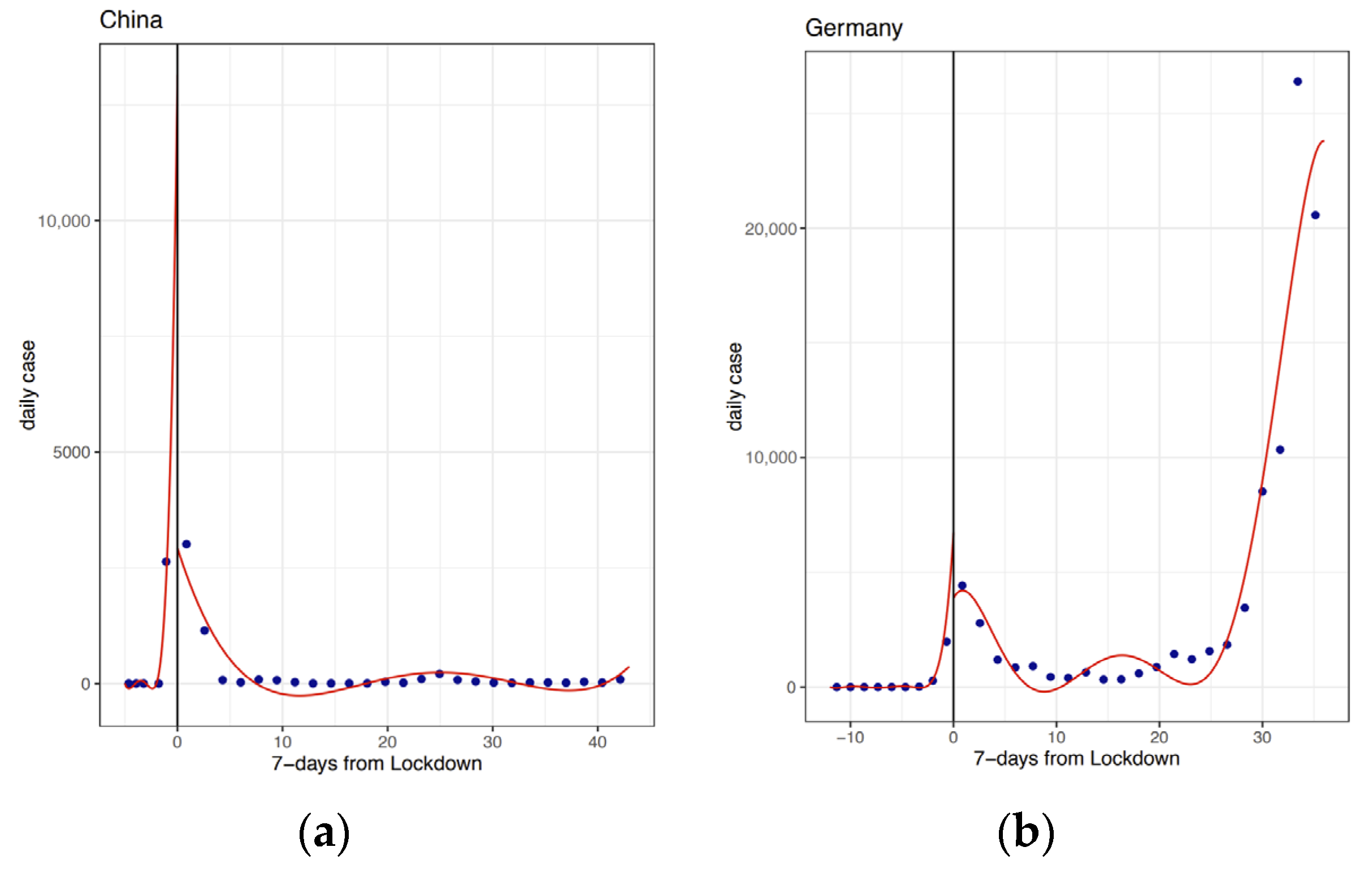
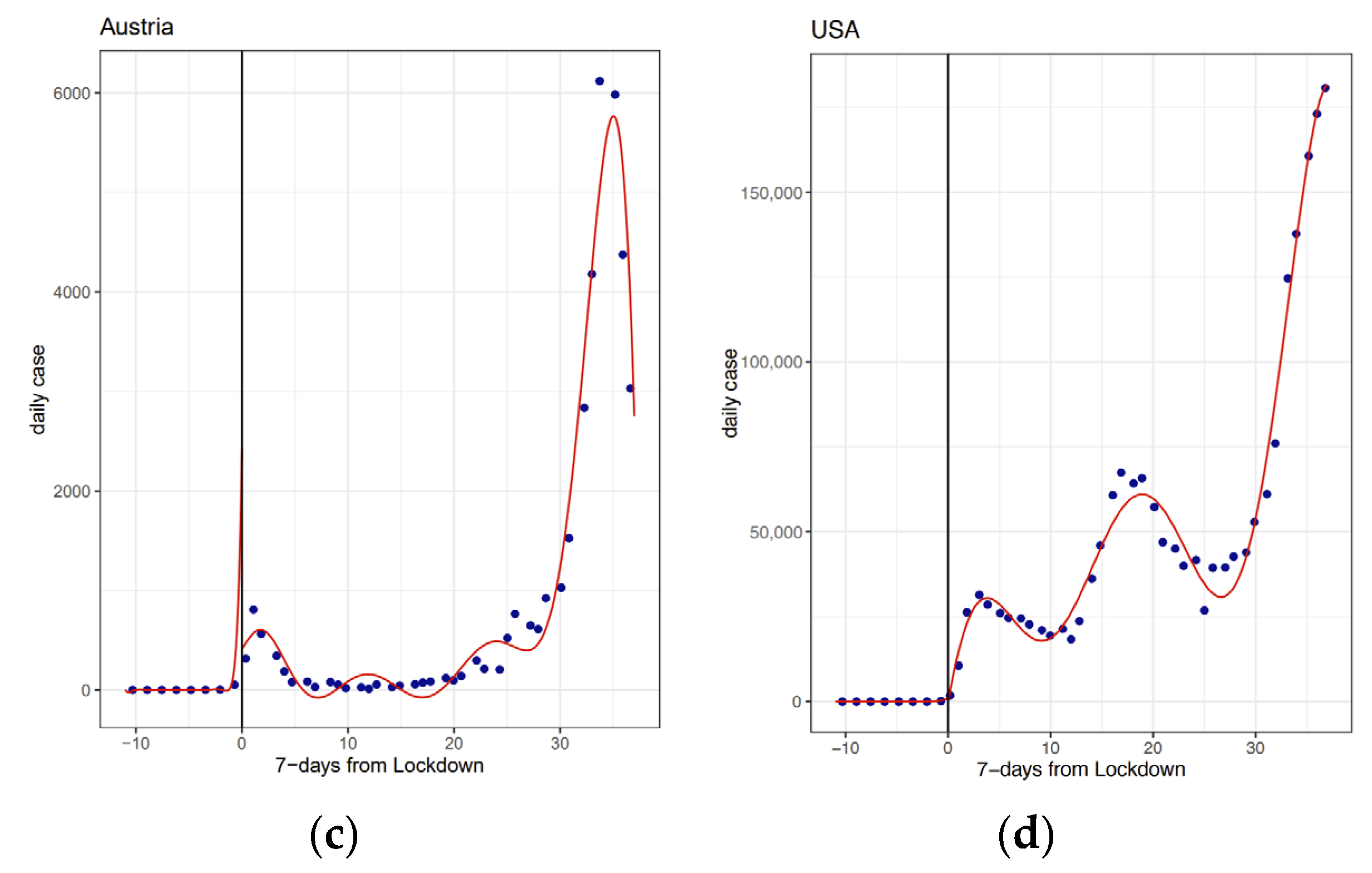
3.2. Overall Impact of Lockdown Interventions
3.3. Comparative Effectiveness of First and second Lockdown
4. Discussion
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
References
- Hui, D.S.; Azhar, E.I.; Memish, Z.A.; Zumla, A. Human Coronavirus Infections—Severe Acute Respiratory Syndrome (SARS), Middle East Respiratory Syndrome (MERS), and SARS-CoV-2. In Reference Module in Biomedical Sciences; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Pincombe, M.; Reese, V.; Dolan, C.B. The effectiveness of national-level containment and closure policies across income levels during the COVID-19 pandemic: An analysis of 113 countries. Health Policy Plan. 2021. [Google Scholar] [CrossRef]
- Chen, S.X.; Lam, B.C.; Liu, J.H.; Choi, H.S.; Kashima, E.; Bernardo, A.B. Effects of containment and closure policies on controlling the COVID-19 pandemic in East Asia. Asian J. Soc. Psychol. 2021, 24, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, R.; Dranitsaris, G.; Mubashir, T.; Bartoszko, J.; Riazi, S. A country level analysis measuring the impact of government actions, country preparedness and socioeconomic factors on COVID-19 mortality and related health outcomes. EClinicalMedicine 2020, 25, 100464. [Google Scholar] [CrossRef]
- Thu, T.P.B.; Ngoc, P.N.H.; Hai, N.M. Effect of the social distancing measures on the spread of COVID-19 in 10 highly infected countries. Sci. Total Environ. 2020, 742, 140430. [Google Scholar] [CrossRef]
- You, J. Lessons From South Korea’s Covid-19 Policy Response. Am. Rev. Public Adm. 2020, 50, 801–808. [Google Scholar] [CrossRef]
- Bargain, O.; Aminjonov, U. Trust and Compliance to Public Health Policies in Times of Covid-19. J. Public Econ. 2020, 192, 104316. [Google Scholar] [CrossRef]
- Trump, B.D.; Keenan, J.M.; Linkov, I. Multi-Disciplinary Perspectives on Systemic Risk and Resilience in the Time of COVID-19. In COVID-19: Systemic Risk and Resilience; Springer: Berlin/Heidelberg, Germany, 2021. [Google Scholar]
- Post, L.; Culler, K.; Moss, C.B.; Murphy, R.L.; Achenbach, C.J.; Ison, M.G.; Resnick, D.; Singh, L.N.; White, J.; Boctor, M.J.; et al. Surveillance of the Second Wave of COVID-19 in Europe: Longitudinal Trend Analyses. JMIR Public Health Surveill. 2021, 7, e25695. [Google Scholar] [CrossRef] [PubMed]
- Lancet, T. Sustaining containment of COVID-19 in China. Lancet 2020, 395, 1230. [Google Scholar] [CrossRef]
- Emeto, T.I.; Alele, F.O.; Ilesanmi, O.S. Evaluation of the effect of border closure on COVID-19 incidence rates across nine African countries: An interrupted time series study. Trans. R. Soc. Trop. Med. Hyg. 2021. [Google Scholar] [CrossRef]
- Bakolis, I.; Stewart, R.; Baldwin, D.; Beenstock, J.; Bibby, P.; Broadbent, M.; Cardinal, R.; Chen, S.; Chinnasamy, K.; Cipriani, A.; et al. Changes in daily mental health service use and mortality at the commencement and lifting of COVID-19 ‘lockdown’ policy in 10 UK sites: A regression discontinuity in time design. BMJ Open 2021, 11, e049721. [Google Scholar] [CrossRef]
- Song, Y.; Li, Z.; Liu, J.; Yang, T.; Zhang, M.; Pang, J. The effect of environmental regulation on air quality in China: A natural experiment during the COVID-19 pandemic. Atmos. Pollut. Res. 2021, 12, 21–30. [Google Scholar] [CrossRef]
- Dang, H.A.H.; Trinh, T.A. Does the COVID-19 lockdown improve global air quality? New cross-national evidence on its unintended consequences. J. Environ. Econ. Manag. 2021, 105, 25. [Google Scholar] [CrossRef]
- Hale, T.; Angrist, N.; Goldszmidt, R.; Kira, B.; Petherick, A.; Phillips, T.; Webster, S.; Cameron-Blake, E.; Hallas, L.; Majumdar, S.; et al. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat. Hum. Behav. 2021, 5, 529–538. [Google Scholar] [CrossRef]
- Hale, T.; Webster, S. Oxford COVID-19 Government Response Tracker; Blavatnik School of Government: Oxford, UK, 2020. [Google Scholar]
- Hasell, J.; Mathieu, E.; Beltekian, D.; Macdonald, B.; Giattino, C.; Ortiz-Ospina, E.; Roser, M.; Ritchie, H. A cross-country database of COVID-19 testing. Sci. Data 2020, 7, 345. [Google Scholar] [CrossRef]
- Hausman, C.; Rapson, D. Regression Discontinuity in Time: Considerations for Empirical Applications. Annu. Rev. Resour. Econ. 2018, 10, 533–552. [Google Scholar] [CrossRef] [Green Version]
- Cori, A.; Ferguson, N.M.; Fraser, C.; Cauchemez, S. A New Framework and Software to Estimate Time-Varying Reproduction Numbers During Epidemics. Am. J. Epidemiol. 2013, 178, 1505–1512. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.; Lau, E.H.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus–Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef]
- Dehkordi, A.H.; Alizadeh, M.; Derakhshan, P.; Babazadeh, P.; Jahandideh, A. Understanding epidemic data and statistics: A case study of COVID-19. J. Med. Virol. 2020, 92, 868–882. [Google Scholar] [CrossRef] [Green Version]
- Desson, Z.; Lambertz, L.; Peters, J.W.; Falkenbach, M.; Kauer, L. Europe’s Covid-19 Outliers: German, Austrian and Swiss policy responses during the early stages of the 2020 pandemic. Health Policy Technol. 2020, 9, 405–418. [Google Scholar] [CrossRef] [PubMed]
- Coughlin, S.S.; Yiǧiter, A.; Xu, H.; Berman, A.E.; Chen, J. Early detection of change patterns in COVID-19 incidence and the implementation of public health policies: A multi-national study. Public Health Pract. 2020, 2, 100064. [Google Scholar] [CrossRef] [PubMed]
- Fouda, A.; Mahmoudi, N.; Moy, N.; Paolucci, F. Comparing the COVID-19 Pandemic in Greece, Iceland, New Zealand, and Singapore. Icel. N. Z. Singap. 2020. [Google Scholar] [CrossRef]
- Giamberardino, P.D.; Iacoviello, D. Evaluation of the effect of different policies in the containment of epidemic spreads for the COVID-19 case. Biomed. Signal Process. Control 2021, 65, 102325. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y. Government Policies, National Culture and Social Distancing during the First Wave of the COVID-19 Pandemic: International Evidence. Saf. Sci. 2020, 135, 105138. [Google Scholar] [CrossRef]
- Haug, N.; Geyrhofer, L.; Londei, A.; Dervic, E.; Desvars-Larrive, A.; Loreto, V.; Pinior, B.; Thurner, S.; Klimek, P. Ranking the effectiveness of worldwide COVID-19 government interventions. Nat. Hum. Behav. 2020, 4, 1303–1312. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Lockdowns | Date | Rt | COVID-19 Cases | Policy Stringency Index |
|---|---|---|---|---|---|
| China | 1st | 1 February | 1.27 | 2089 | 77.31 |
| 2nd | 10 May | 0.93 | 20 | 81.94 | |
| Germany | 1st | 21 March | 1.09 | 2365 | 68.06 |
| 2nd | 22 October | 1.11 | 5952 | 60.65 | |
| Austria | 1st | 16 March | 0.92 | 158 | 81.48 |
| 2nd | 17 October | 1.49 | 1747 | 58.8 | |
| USA | 1st | 15 March | 1.63 | 234 | 41.2 |
| 2nd | 13 October | 1.22 | 52879 | 66.2 |
| Dependent Variable: Rt | ||||||||
|---|---|---|---|---|---|---|---|---|
| China | Germany | Austria | USA | |||||
| (1) | (2) | (1) | (2) | (1) | (2) | (1) | (2) | |
| X | −0.988 * | 0.007 | 0.240 *** | 0.108 *** | 0.289 *** | 1.201 *** | 0.447 *** | 1.879 *** |
| I(X_2) | 0.0001 | −0.003 ** | 0.076 *** | 0.119 *** | ||||
| treatment | −4.457 *** | −4.432 *** | −2.167 *** | −2.059 *** | −1.534 *** | −3.831 *** | −2.605 *** | −5.566 *** |
| X_treatment | 0.999 * | 14.458 *** | −0.228 *** | 0.107 | −0.279 *** | −1.137 *** | −0.448 *** | −1.904 *** |
| I(X_2):treatment | 2.240 *** | 0.023 | −0.077 *** | −0.119 *** | ||||
| Constant | 2.322 | −13.358 *** | 3.000 *** | 2.280 ** | 2.403 *** | 4.379 *** | 3.716 *** | 6.819 *** |
| Adjusted R2 | 0.329 | 0.619 | 0.178 | 0.164 | 0.319 | 0.504 | 0.319 | 0.565 |
| F Statistic | 8.842 *** | 16.567 *** | 4.463 *** | 2.880 ** | 8.493 *** | 10.750 *** | 8.499 *** | 11.171 *** |
| Dependent Variable: Daily Cases | ||||||||
|---|---|---|---|---|---|---|---|---|
| China | Germany | Austria | USA | |||||
| (1) | (2) | (1) | (2) | (1) | (2) | (1) | (2) | |
| X | 526.400 * | 2782.400 *** | 402.040 *** | 550.004 *** | 95.700 *** | 13.405 | 2930.453 *** | 50.155 |
| I(X_2) | 376.000 ** | 27.681 *** | 0.910 | 121.134 *** | ||||
| treatment | −1362.27 * | −3274.50 *** | 5537.66 ** | 7162.482 ** | 1388.330 ** | 1473.104 ** | 18,375.940 | 37,561.110 ** |
| X_treatment | −550.325 ** | −2909.15 *** | 326.664 | 1701.041 | 95.463 | 237.527 | 2846.793 | |
| I(X_2):treatment | −373.61 ** | 16.871 | 7.794 | 153.278 | ||||
| Constant | 2105.600 *** | 4737.600 *** | 2805.675 * | 1631.250 | 19.982 | 43.648 | 74.382 | 163.018 |
| Adjusted R2 | 0.216 | 0.475 | 0.382 | 0.781 | 0.447 | 0.768 | 0.677 | 0.789 |
| F Statistic | 5.41 *** | 9.676 *** | 10.901 *** | 35.251 *** | 13.946 *** | 32.729 *** | 31.495 *** | 32.115 *** |
| Dependent Variable: Rt | ||||||||
|---|---|---|---|---|---|---|---|---|
| China | Germany | Austria | USA | |||||
| 1st | 2nd | 1st | 2nd | 1st | 2nd | 1st | 2nd | |
| X | 0.371 *** | −0.117 *** | −0.282 *** | −0.065 *** | −0.359 *** | 0.002 | −0.874 *** | −2.352 *** |
| I(X_2) | 0.033 *** | −0.005 *** | −0.005 ** | −0.002 *** | −0.006 | −0.001 * | −0.041 *** | −0.180 *** |
| treatment | −1.556 *** | 0.585 * | 0.827 * | 0.112 *** | 0.564 | −0.128 ** | 1.334 | 4.750 *** |
| X_treatment | −0.359 *** | 0.141 ** | 0.272 *** | 0.046 *** | 0.336 *** | −0.037 *** | 0.752 *** | 2.282 *** |
| I(X_2):treatment | −0.034 *** | 0.004 * | 0.005 * | 0.003 *** | 0.007 | 0.001 | 0.044 *** | 0.178 *** |
| Constant | 1.986 *** | 0.529 ** | 0.027 | 1.014 *** | 0.174 | 1.566 *** | 0.771 | −2.742 ** |
| Adjusted R2 | 0.986 | 0.173 | 0.854 | 0.964 | 0.910 | 0.903 | 0.649 | 0.752 |
| F Statistic | 685.674 *** | 3.098 ** | 59.560 *** | 272.104 *** | 91.812 *** | 94.318 *** | 19.486 *** | 22.653 *** |
| Dependent Variable: Daily Cases | ||||||||
|---|---|---|---|---|---|---|---|---|
| China | Germany | Austria | USA | |||||
| 1st | 2nd | 1st | 2nd | 1st | 2nd | 1st | 2nd | |
| X | 353.007 *** | 7.889 *** | 426.831 *** | 646.062 *** | 36.538 ** | 67.566 * | 735.098 *** | 735.098 *** |
| I(X_2) | 9.801 ** | 0.423 *** | 10.875 *** | 12.018 | 1.191 * | 4.351 *** | 24.305 *** | 24.305 *** |
| treatment | −762.321 | −24.508 ** | −865.244 * | 4811.651 *** | −108.633 * | −254.206 | −2058.490 ** | 2100.234 *** |
| X_treatment | −243.693 | −8.009 *** | −192.626 ** | 441.737 | 110.960 *** | 208.117 *** | 2100.234 ** | −35.416 *** |
| I(X_2):treatment | −20.954 *** | −0.416 *** | −24.520 *** | −46.101 *** | −17.168 *** | −1.549 | −35.416 *** | 986.184 |
| Constant | 2981.537 *** | 31.207 *** | 4104.298 *** | 9243.376 *** | 303.808 *** | 1558.123 *** | 938.363 | 938.363 |
| Adjusted R2 | 0.699 | 0.768 | 0.942 | 0.879 | 0.972 | 0.981 | 0.991 | 0.991 |
| F Statistic | 24.255 *** | 34.156 *** | 162.698 *** | 122.417 *** | 226.549 *** | 521.901 *** | 1091.190 *** | 1091.190 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, S.; Ermolieva, T.; Cao, G.; Chen, G.; Zheng, X. Analyzing the Effectiveness of COVID-19 Lockdown Policies Using the Time-Dependent Reproduction Number and the Regression Discontinuity Framework: Comparison between Countries. Eng. Proc. 2021, 5, 8. https://doi.org/10.3390/engproc2021005008
Liu S, Ermolieva T, Cao G, Chen G, Zheng X. Analyzing the Effectiveness of COVID-19 Lockdown Policies Using the Time-Dependent Reproduction Number and the Regression Discontinuity Framework: Comparison between Countries. Engineering Proceedings. 2021; 5(1):8. https://doi.org/10.3390/engproc2021005008
Chicago/Turabian StyleLiu, Shangjun, Tatiana Ermolieva, Guiying Cao, Gong Chen, and Xiaoying Zheng. 2021. "Analyzing the Effectiveness of COVID-19 Lockdown Policies Using the Time-Dependent Reproduction Number and the Regression Discontinuity Framework: Comparison between Countries" Engineering Proceedings 5, no. 1: 8. https://doi.org/10.3390/engproc2021005008