
Evaluating the Practice of Preventive Behaviors and the Fear of COVID-19 among Dentists in Oradea Metropolitan Area after the First Wave of Pandemic; a Cross-Sectional Study





Abstract
:1. Introduction
2. Materials and Methods
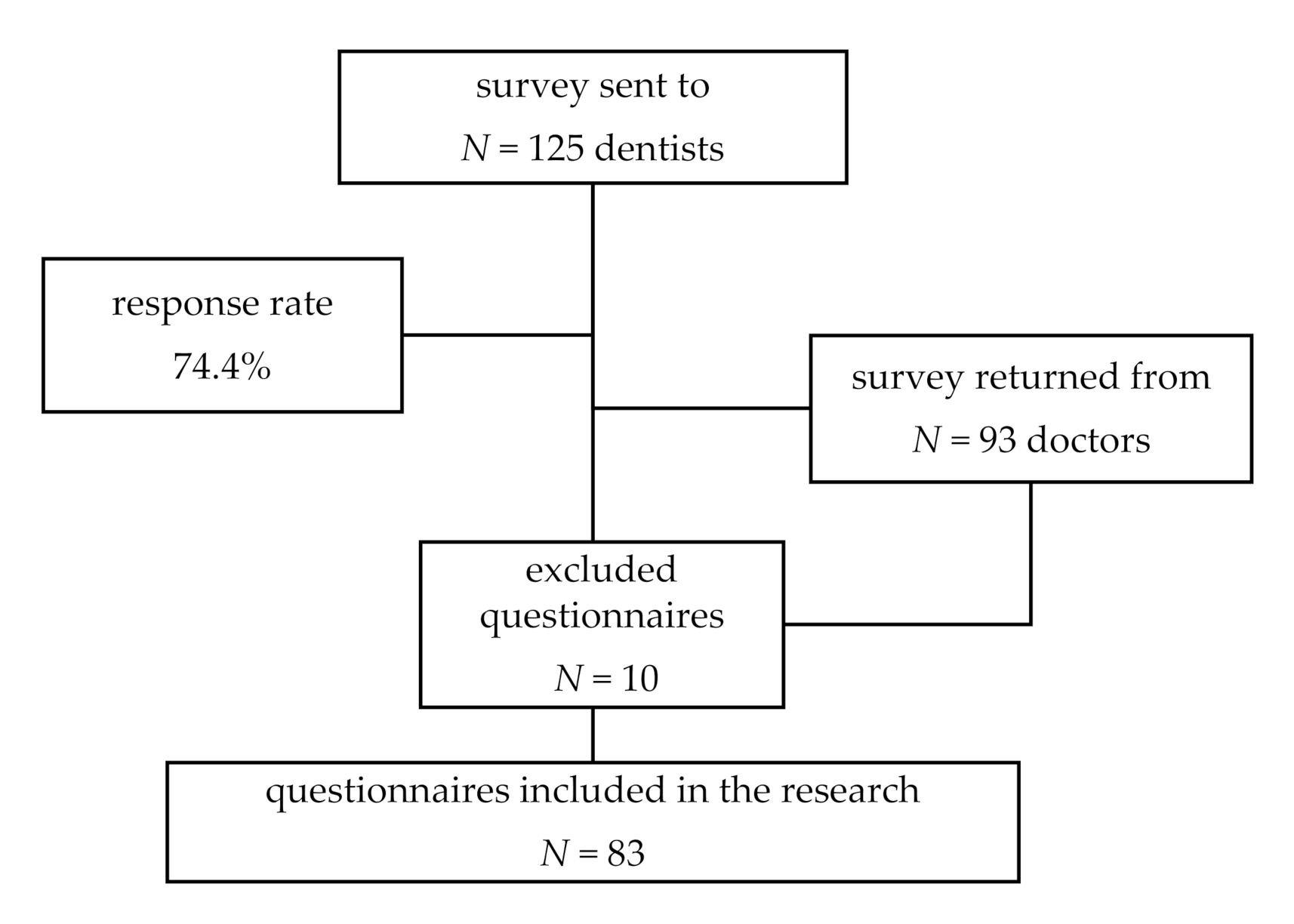
2.1. Participants
2.2. Data Collection
- -
- Sociodemographic data (age, gender, length of employment, number of children, marital status, length of employment, environment, type of institutions, category of patients, level of specialization,) and medical-related data (chronic disease, previously infected with COVID 19).
- -
- Job-related data in the first seven months of lockdown (number of working hours per week, number of free days, period of not working due to government restrictions, supplementary measures taken to diminish the risk of being infected with COVD-19, providing medical services only to dental emergency, etc.).
- -
- Preventive behaviors adopted in the first seven months of confinement in the professional and private life (living separately from family members, medical suppliers, disinfection, schedule, pre-trial of patients, medical suits, etc.). Also, items investigated the institutional rules that changed to limit the spread of infections during dental procedures. Self-rated items collected answers using a Likert like scale with 5 points from 1 (never) to 5 (always).
- -
- Self-rated item regarding the fear of being infected with COVID-19 and its consequences on health status. These statements were associated with a 5-point Likert scale from 1 (never) to 5 (always).
- -
- Fear of COVID-19 developed by Ahorsu et al, in 2020 [21]. The tool included 7 items and respondents had to indicate their level of agreement with the statements using a five-item Likert-type scale. Answers included “strongly disagree”, “disagree”, “neither agree nor disagree”, “agree”, and “strongly agree”. The minimum score possible for each question is 1, and the maximum is 5. A total score is calculated by adding up each item score (ranging from 7 to 35). The higher the score, the greater the fear of COVID-19. This is an instrument that was frequently used in many scientific papers and proved to have a good reliability.
2.3. Statistical Analysis
2.4. Ethical Approval
3. Results
3.1. Sociodemographic Data
3.2. Financial Problems and Family-Related Data
3.3. Fear of COVID-19
3.3.1. Self-Rated Items
3.3.2. Fear of COVID-19 Scale
3.4. Patient’s Safety, Triage, and New Protective Measures
3.5. Institutional Preventive Rules
4. Discussion
4.1. Strengths and Limitations of the Study
4.2. Reflections and Planning
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Timeline–COVID-19. Available online: https://www.who.int/news-room/detail/27-04-2020-who-timeline---covid-19 (accessed on 20 December 2020).
- Military Ordinance. Available online: https://www.mai.gov.ro/wp-content/uploads/2020%9Ba-militar%C4%83-nr.-1-2020-m%C4%83suri-de-prima-urgen%C8%9B%C4%83-Decret.pdf (accessed on 3 December 2020).
- National Executive Office of the Romanian College of Dentists. Recommendations for Preventing the Spread of COVID-19 in Emergency Dental Activity. Available online: https://cmdr.ro/download-zone-preview/0/1585254764/3114/7c1a06790c87eb490b59e77515bababd (accessed on 8 December 2020).
- Gurzawska-Comis, K.; Becker, K.; Brunello, G.; Gurzawska, A.; Schwarz, F. Recommendations for Dental Care during COVID-19 Pandemic. J. Clin. Med. 2020, 9, 1833. [Google Scholar] [CrossRef]
- Villani, F.A.; Aiuto, R.; Paglia, L.; Re, D. COVID-19 and Dentistry: Prevention in Dental Practice, a Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 4609. [Google Scholar] [CrossRef] [PubMed]
- Peditto, M.; Scapellato, S.; Marcianò, A.; Costa, P.; Oteri, G. Dentistry during the COVID-19 Epidemic: An Italian Workflow for the Management of Dental Practice. Int. J. Environ. Res. Public Health 2020, 17, 3325. [Google Scholar] [CrossRef] [PubMed]
- Lucaciu, O.; Tarczali, D.; Petrescu, N. Oral healthcare during the COVID-19 pandemic. J. Dent. Sci. 2020. [CrossRef]
- Fallahi, H.R.; Keyhan, S.O.; Zandian, D.; Kim, S.G.; Cheshmi, B. Being a front-line dentist during the Covid-19 pandemic: A literature review. Maxillofac. Plast. Reconstr. Surg. 2020, 42, 1–9. [Google Scholar] [CrossRef]
- Passarelli, P.C.; Rella, E.; Manicone, P.F.; Garcia-Godoy, F.; D’Addona, A. The impact of the COVID-19 infection in dentistry. Exp. Biol. Med. 2020, 245, 940–944. [Google Scholar] [CrossRef]
- Amato, A.; Caggiano, M.; Amato, M.; Moccia, G.; Capunzo, M.; De Caro, F. Infection Control in Dental Practice During the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 4769. [Google Scholar] [CrossRef]
- Vergara-Buenaventura, A.; Chavez-Tuñon, M.; Castro-Ruiz, C. The mental health consequences of coronavirus disease 2019 pandemic in dentistry. Disaster Med. Public Health Prep. 2020, 1–4. [Google Scholar] [CrossRef]
- Shacham, M.; Hamama-Raz, Y.; Kolerman, R.; Mijiritsky, O.; Ben-Ezra, M.; Mijiritsky, E. COVID-19 Factors and Psychological Factors Associated with Elevated Psychological Distress among Dentists and Dental Hygienists in Israel. Int. J. Environ. Res. Public Health 2020, 17, 2900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collin, V.; Whitehead, P. Psychological distress and the perceived impact of the COVID-19 pandemic on UK dentists during a national lockdown. Br. Dent. J. 2021, 22, 1–8. [Google Scholar] [CrossRef]
- Ahmed, M.A.; Jouhar, R.; Ahmed, N.; Adnan, S.; Aftab, M.; Zafar, M.S.; Khurshid, Z. Fear and Practice Modifications among Dentists to Combat Novel Coronavirus Disease (COVID-19) Outbreak. Int. J. Environ. Res. Public Health 2020, 17, 2821. [Google Scholar] [CrossRef] [PubMed]
- Casillas Santana, M.Á.; Martínez Zumarán, A.; Patiño Marín, N.; Castillo Silva, B.E.; Sámano Valencia, C.; Salas Orozco, M.F. How Dentists Face the COVID-19 in Mexico: A Nationwide Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 1750. [Google Scholar] [CrossRef]
- Tysiąc-Miśta, M.; Dziedzic, A. The Attitudes and Professional Approaches of Dental Practitioners during the COVID-19 Outbreak in Poland: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2020, 17, 4703. [Google Scholar] [CrossRef]
- Consolo, U.; Bellini, P.; Bencivenni, D.; Iani, C.; Checchi, V. Epidemiological Aspects and Psychological Reactions to COVID-19 of Dental Practitioners in the Northern Italy Districts of Modena and Reggio Emilia. Int. J. Environ. Res. Public Health 2020, 17, 3459. [Google Scholar] [CrossRef]
- Chamorro-Petronacci, C.; Martin Carreras-Presas, C.; Sanz-Marchena, A.; Rodríguez-Fernández, M.A.; María Suárez-Quintanilla, J.; Rivas-Mundiña, B.; Suárez-Quintanilla, J.; Pérez-Sayáns, M. Assessment of the Economic and Health-Care Impact of COVID-19 (SARS-CoV-2) on Public and Private Dental Surgeries in Spain: A Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 5139. [Google Scholar] [CrossRef]
- Iurcov, R.; Todor, L.; Iorga, M.; Ioan, B.G. COVID 19 Pandemic and the Impact on Dentistry Practice. Opinion of University Teachers. Rom. J. Oral Rehabil. 2020, 12, 26–35. [Google Scholar]
- Petrescu, N.B.; Aghiorghiesei, O.; Mesaros, A.S.; Lucaciu, O.P.; Dinu, C.M.; Campian, R.S.; Negucioiu, M. Impact of COVID-19 on Dental Emergency Services in Cluj-Napoca Metropolitan Area: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 7716. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The fear of COVID-19 scale: Development and initial validation. Int. J. Ment. Health Addict. 2020, 27, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Gross, C.P.; Essien, U.R.; Pasha, S.; Gross, J.R.; Wang, S.Y.; Nunez-Smith, M. Racial and ethnic disparities in population-level Covid-19 mortality. J. Gen. Intern. Med. 2020, 35, 3097–3099. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.A.; David, M.E. The Pandemic within a Pandemic: Testing a Sequential Mediation Model to Better Understand Racial/Ethnic Disparities in COVID-19 Preventive Behavior. Healthcare 2021, 9, 230. [Google Scholar] [CrossRef] [PubMed]
- Attia, S.; Howaldt, H.-P. Impact of COVID-19 on the Dental Community: Part I before Vaccine (BV). J. Clin. Med. 2021, 10, 288. [Google Scholar] [CrossRef]
- Soraci, P.; Ferrari, A.; Abbiati, F.A.; Del Fante, E.; De Pace, R.; Urso, A.; Griffiths, M.D. Validation and psychometric evaluation of the Italian version of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 1–10. [Google Scholar] [CrossRef]
- Alyami, M.; Henning, M.; Krägeloh, C.U.; Alyami, H. Psychometric evaluation of the Arabic version of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 1–14. [Google Scholar] [CrossRef]
- Bitan, D.T.; Grossman-Giron, A.; Bloch, Y.; Mayer, Y.; Shiffman, N.; Mendlovic, S. Fear of COVID-19 scale: Psychometric characteristics, reliability and validity in the Israeli population. Psychiatry Res. 2020, 289, 113100. [Google Scholar] [CrossRef]
- Haktanir, A.; Seki, T.; Dilmaç, B. Adaptation, and evaluation of Turkish version of the fear of COVID-19 scale. Death Stud. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Perz, C.A.; Lang, B.A.; Harrington, R. Validation of the Fear of COVID-19 Scale in a US College Sample. Int. J. Ment. Health Addict. 2020, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Lorca, M.; Martínez-Lorca, A.; Criado-Álvarez, J.J.; Armesilla, M.D.C. The fear of COVID-19 scale: Validation in Spanish university students. Psychiatry Res. 2020, 293, 113350. [Google Scholar] [CrossRef]
- Chi, X.; Chen, S.; Chen, Y.; Chen, D.; Yu, Q.; Guo, T.; Cao, Q.; Zheng, X.; Huang, S.; Hossain, M.M.; et al. Psychometric evaluation of the fear of COVID-19 scale among Chinese population. Int. J. Ment. Health Addict. 2021, 1–16. [Google Scholar] [CrossRef]
- Masuyama, A.; Shinkawa, H.; Kubo, T. Validation and psychometric properties of the Japanese version of the fear of COVID-19 scale among adolescents. Int. J. Ment. Health Addict. 2020, 1–11. [Google Scholar] [CrossRef]
- Cassiani-Miranda, C.A.; Tirado-Otálvaro, A.F.; Campo-Arias, A. Adaptation and psychometric evaluation of the Fear of COVID-19 Scale in the general Colombian population. Death Stud. 2021, 1–8. [Google Scholar] [CrossRef]
- Iversen, M.M.; Norekvål, T.M.; Oterhals, K.; Fadnes, L.T.; Mæland, S.; Pakpour, A.H.; Breivik, K. Psychometric properties of the Norwegian version of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2021, 1–19. [Google Scholar] [CrossRef]
- Caycho-Rodríguez, T.; Vilca, L.W.; Cervigni, M.; Gallegos, M.; Martino, P.; Portillo, N.; Barés, I.; Calandra, M.; Burgos Videla, C. Fear of COVID-19 scale: Validity, reliability and factorial invariance in Argentina’s general population. Death Stud. 2020, 1–10. [Google Scholar] [CrossRef]
- Cavalheiro, F.R.S.; Sticca, M.G. Adaptation and Validation of the Brazilian Version of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 1–9. [Google Scholar] [CrossRef]
- Tsipropoulou, V.; Nikopoulou, V.A.; Holeva, V.; Nasika, Z.; Diakogiannis, I.; Sakka, S.; Kostikidou, S.; Varvara, C.; Spyridopoulou, E.; Parlapani, E. Psychometric properties of the Greek version of FCV-19S. Int. J. Ment. Health Addict. 2020. [CrossRef]
- Gasparro, R.; Scandurra, C.; Maldonato, N.M.; Dolce, P.; Bochicchio, V.; Valletta, A.; Sammartino, G.; Sammartino, P.; Mariniello, M.; di Lauro, A.E.; et al. Perceived Job Insecurity and Depressive Symptoms among Italian Dentists: The Moderating Role of Fear of COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 5338. [Google Scholar] [CrossRef]
- Mekhemar, M.; Attia, S.; Dörfer, C.; Conrad, J. The Psychological Impact of the COVID-19 Pandemic on Dentists in Germany. J. Clin. Med. 2021, 10, 1008. [Google Scholar] [CrossRef]
- Ammar, N.; Aly, N.M.; Folayan, M.O.; Khader, Y.; Virtanen, J.I.; Al-Batayneh, O.B.; Mohebbi, S.Z.; Attia, S.; Howaldt, H.P.; Boettger, S.; et al. Behavior change due to COVID-19 among dental academics—The theory of planned behavior: Stresses, worries, training, and pandemic severity. PLoS ONE 2020, 15, e0239961. [Google Scholar] [CrossRef]
- Farronato, M.; Tadakamadla, S.K.; Ali Quadri, M.F.; Acharya, S.; Tadakamadla, J.; Love, R.M.; Jamal, M.; Mulder, R.; Maspero, C.; Farronato, D.; et al. A Call for Action to Safely Deliver Oral Health Care during and Post COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6704. [Google Scholar] [CrossRef]
- Farronato, M.; Boccalari, E.; Del Rosso, E.; Lanteri, V.; Mulder, R.; Maspero, C. A Scoping Review of Respirator Literature and a Survey among Dental Professionals. Int. J. Environ. Res. Public Health 2020, 17, 5968. [Google Scholar] [CrossRef]
- Local Authority of Ministry of Health. Available online: http://www.dspbihor.gov.ro/2020/03/Informatii%20publice/Comunicate%20de%20presa/Comunicat%20de%20presa%2014032020_3_Detalii%20privind%20primul%20caz%20din%20judetul%20Bihor%20confirmat%20COVID-19.pdf (accessed on 20 January 2020).


{kind=link}
| Sociodemographic and Medical Characteristics | N (%)/M ± SD 1 |
|---|---|
| Age | 37.81 ± 8.45 |
| Length of employment (years) | 11.87 ± 8.62 |
| Gender | |
| Male | 29 (34.94) |
| Female | 53 (63.86) |
| I prefer not to say | 1 (1.20) |
| Marital status | |
| Single | 11 (13.25) |
| In relationship | 72 (86.75) |
| Having children | |
| yes | 46 (55.42) |
| no | 37 (44.58) |
| Level of specialization | |
| Dentists | 38 (45.78) |
| Male | 17 (20.48) |
| Female | 21 (25.30) |
| Residents | 16 (19.28) |
| Male | 1 (1.20) |
| Female | 15 (10.64) |
| Specialists | 10 (12.05) |
| Male | 6 (7.23) |
| Female | 4 (4.82) |
| Consultants | 19 (22.89) |
| Male | 5 (6.02) |
| Female | 13 (15.66) |
| I prefer not to say | 1 (1.20) |
| Teaching activity | |
| yes | 23 (27.71) |
| no | 60 (72.29) |
| Type of institution | |
| only public sector | 3 (3.61) |
| only private sector | 50 (60.24) |
| both private and public sectors | 30 (36.14) |
| Providing medical assistance to | |
| only children | 0 |
| only adults | 5 (6.02) |
| both children and adults | 78 (93.98) |
| Working environment | |
| urban | 77 (92.77) |
| rural | 6 (7.23) |
| Items | M ± SD 1 |
|---|---|
| I fear that wearing the protective suit against COVID-19 does not protect me enough | 2.55 ± 1.41 |
| I fear that patients do not tell the truth about their health | 3.47 ± 1.40 |
| I fear that I can get infected when I take off my protective suit | 2.51 ± 1.43 |
| I fear that I might get infected from co-workers | 2.54 ± 1.30 |
| I believe that dentists have a very high risk of COVID-19 infection by their patients | 3.52 ± 1.51 |
| Dental procedures can be a source of infection and spread of COVID-19 | 2.81 ± 1.26 |
| The fact that patients cannot wear a mask during medical treatment causes me to fear infection | 2.48 ± 1.35 |
| I fear I can get infected by my patients | 2.78 ± 1.38 |
| I think my patients are afraid of getting infected with COVID-19 after dental procedures | 3.01 ± 1.37 |
| I have noticed that patients avoid coming to routine dental check-ups | 3.49 ± 1.31 |
| Items | M ± SD 1 |
|---|---|
| As an additional measure, I no longer receive family members in the medical room | 4.09 ± 1.29 |
| I ask patients to get a COVID test before giving them medical care | 1.51 ± 0.84 |
| As an additional measure, I measure the patients’ temperature before providing them with medical care | 4.54 ± 1.15 |
| As an additional measure, patients disinfect their hands when entering the office | 4.81 ± 0.49 |
| As an additional measure, patients wear a surgical mask while in the waiting room | 4.85 ± 0.56 |
| As an additional measure, I offer patients protective equipment (disposable gown, cap and shoe protection) | 4.18 ± 1.23 |
| As an additional measure, patients should rinse their mouth with disinfectants for the oral cavity | 4.14 ± 1.36 |
| To avoid contact with blood or saliva I use modern isolation systems | 3.60 ± 1.25 |
| As an additional preventive measure, I schedule consultations | 4.79 ± 0.71 |
| As an additional measure, I perform telephone epidemiological triage | 4.07 ± 1.26 |
| As an additional measure, I perform the epidemiological triage by filling in a triage form by the patient | 4.63 ± 0.82 |
| Patients are scheduled according to the severity of the condition | 3.84 ± 1.40 |
| I try to shorten the duration of dental interventions for fear of not staying too long in contact with patients | 2.75 ± 1.51 |
| I change my protective suit after each patient | 3.61 ± 1.35 |
| Items | M ± SD 1 |
|---|---|
| At my workplace, the additional protection measures against COVID-19 infection are effective | 4.51 ± 0.78 |
| My workplace provides me with the protection equipment against COVID-19 infection | 4.14 ± 1.53 |
| Since the onset of the pandemic, we have provided medical care to patients online or by telephone | 3.32 ± 1.26 |
| I had difficulty in purchasing myself a protective suit/mask/visor | 2.61 ± 1.59 |
| I respect the time interval for performing the disinfection | 4.65 ± 0.63 |
| I keep the social distance from the auxiliary staff | 4.12 ± 1.17 |
| I fully comply with the hygienic-sanitary measures to prevent COVID-19 infection imposed by the competent authorities | 3.81 ± 1.40 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iurcov, R.; Pop, L.M.; Ciavoi, G.; Iorga, M. Evaluating the Practice of Preventive Behaviors and the Fear of COVID-19 among Dentists in Oradea Metropolitan Area after the First Wave of Pandemic; a Cross-Sectional Study. Healthcare 2021, 9, 443. https://doi.org/10.3390/healthcare9040443
Iurcov R, Pop LM, Ciavoi G, Iorga M. Evaluating the Practice of Preventive Behaviors and the Fear of COVID-19 among Dentists in Oradea Metropolitan Area after the First Wave of Pandemic; a Cross-Sectional Study. Healthcare. 2021; 9(4):443. https://doi.org/10.3390/healthcare9040443
Chicago/Turabian StyleIurcov, Raluca, Lavinia Maria Pop, Gabriela Ciavoi, and Magdalena Iorga. 2021. "Evaluating the Practice of Preventive Behaviors and the Fear of COVID-19 among Dentists in Oradea Metropolitan Area after the First Wave of Pandemic; a Cross-Sectional Study" Healthcare 9, no. 4: 443. https://doi.org/10.3390/healthcare9040443